
Abstract
Objective
Screening programmes based on the faecal occult blood test (FOBT) can reduce mortality from colorectal cancer (CRC). However, a significant variation exists in uptake of the test within the UK. Disproportionate uptake risks increasing inequity during staging at diagnosis and survival from CRC. This study aims to evaluate the impact of socioeconomic deprivation on the uptake of CRC screening (FOBT) in London.
Methods
A retrospective review of the “Vanguard RM Informatics” database was performed to identify eligible individuals for CRC screening across all general practices across London over 30 months (2014–2017). The postcodes of the general practices were used to obtain the deprivation data via the “Indices of Deprivation” database. A Spearman’s rho correlation was performed to quantify the impact of the deprivation variables on FOBT uptake.
Results
Overall, 697,402 individuals were eligible for screening across 1359 London general practices, within 5 Clinical Commissioning Groups (CCGs); 48.4% (range: 13%–74%) participated in CRC screening with the lowest participation rates in North West (46%) and North East (47%) London CCGs. All indices of deprivation had a significant correlation with the uptake of FOBT (p < 0.01).
Conclusion
This is the largest study across London to date demonstrating a significant positive correlation between deprivation indices and FOBT uptake, highlighting areas of particular risk. Further studies are imperative to quantify the impact of deprivation on CRC morbidity and mortality, together with focused strategies to reduce socioeconomic inequalities in screening in these high risk areas.
Keywords
Introduction
Colorectal cancer (CRC) is the second highest cause of cancer deaths in the United Kingdom. 1 Globally, CRC accounts for 9% of the cancer incidence. 1 Evidence from randomised controlled trials suggests a reduction in CRC mortality with use of the home-based guaiac faecal occult blood test (FOBT).2,3 In England, the National Health Service (NHS) introduced the Bowel Cancer Screening Programme (BCSP) in 2006, providing biennial FOBT to all men and women aged 60 to 74. 4 Upon a positive FOBT, patients are eligible for a diagnostic test (most commonly colonoscopy). 4 More recently, a single flexible sigmoidoscopy at the age of 55 years has been introduced.
To maintain the quality and effectiveness of CRC screening, it is essential to have a high uptake, adherence and equal access to the screening programme. However, substantial variations in uptake of CRC screening have been highlighted with regard to age, gender, socioeconomic deprivation and ethnicity.5,6 It is crucial to study the impact of socioeconomic deprivation on the uptake of CRC screening as it has been highlighted that the faecal haemoglobin positivity rates increase with greater deprivation. 7 Furthermore, Smith et al. 8 observed that social deprivation was an independent risk factor of postoperative length of stay and associated with higher postoperative mortality following colorectal cancer resection, with other studies also showing a significant increase in cancer morbidity and mortality with greater socioeconomic deprivation.9,10
Previous studies have been based on recall of screening history by patients (self-reporting) compared to data collection via a prospective central register, the former being prone to selection and recall bias.11,12 To date, a majority of the studies have not considered markers of socioeconomic deprivation such as education and income.5,13 As the index of multiple of deprivation (IMDR) encompasses several domains such as income, employment and education, recent studies have chosen to report on IMDR alone where a higher IMDR correlates with a lower level of relative deprivation or a relatively more privileged area. 14 In the UK, this limits the evaluation of the effect of literacy on the uptake of mailed FOBT kits, as printed communication can deter less educated individuals from CRC screening. 15 In addition, the ASCEND trial, whose purpose was to determine if interventions such as reminder letters or general practice endorsement letters would improve uptake in relation to IMDR, showed contrasting results. 16 Our study therefore aimed to evaluate the impact of individual indices of socioeconomic deprivation such as income, employment and education as well as the IMDR on the uptake of the BCSP in an unselected population within London.
Methods
Study population and data collection
The National Cancer Vanguard (NCV) was set up in 2015 as part of NHS England’s New Care Models Programme to improve cancer care. The NCV consists of three Vanguard partners of which RM Partners is one. RM Partners, hosted by the Royal Marsden, works closely with North West and South West London Commissioners. High quality data are collected and stored on the “Vanguard RM Informatics” database. This database contains information regarding total number of patients that are eligible for screening, number of patients screened and the percentage coverage over 30 months per general practice (GP). In addition, it contains basic GP demographics including address, associated Trust and Clinical Commissioning Group (CCG). Special permission was granted to us by RM Partners to access this database.
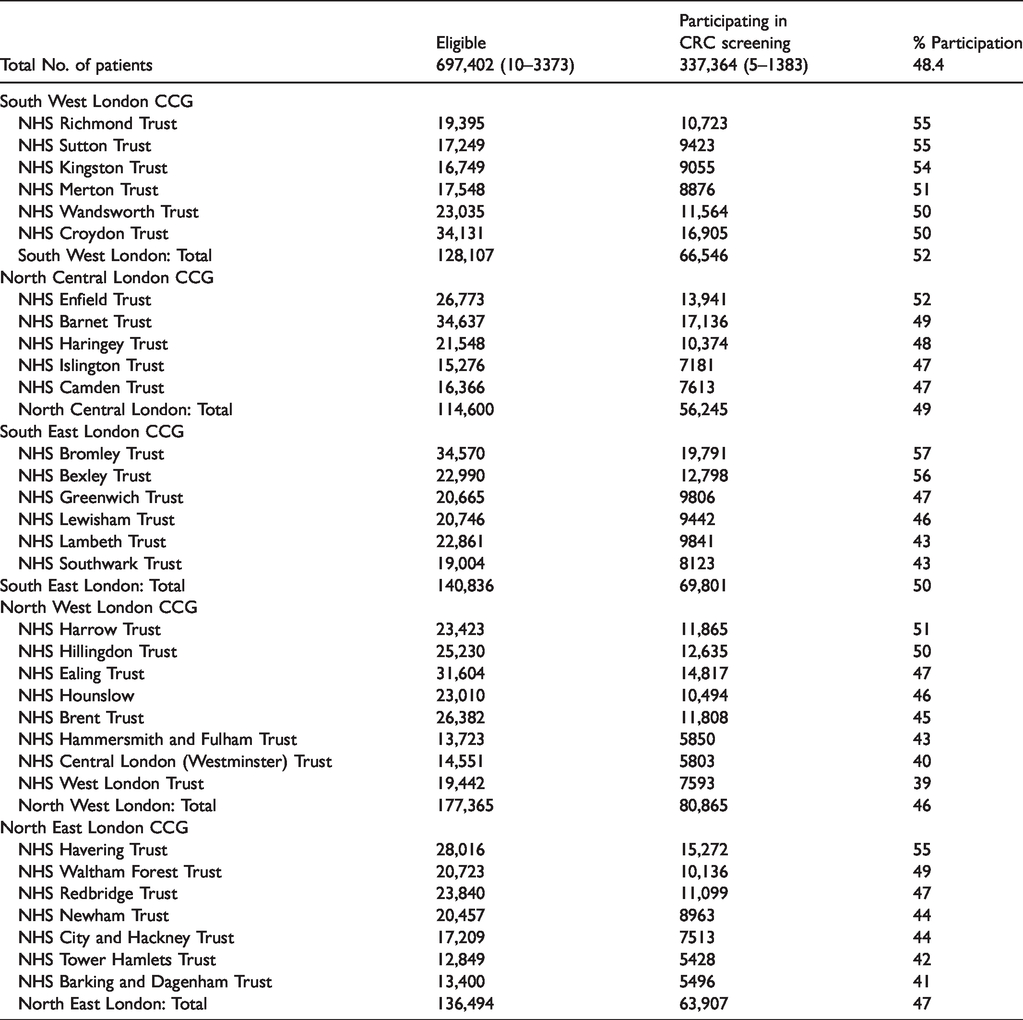
A retrospective review of the database was conducted to identify patients aged 60–69 who were invited to partake in the BCSP across all 1359 GPs within London. The study period extended over 30 months, from December 2014 to May 2017, as per the database. The Trusts and CCGs included in the study are described further in Table 1.
Uptake of CRC screening across London per Trust and CCG.
As part of the BSCP, all participants were mailed a FOBT sampling kit with instructions on collecting samples at home and sending the samples to the laboratory. The proportion of patients participating in the screening programme was noted for each individual GP and its associated Trust and CCG. The postcodes of the GPs were used to obtain the deprivation data such as the index of multiple deprivation rank (IMDR), income rank, employment rank, education and skills rank (ESR), and health and disability rank (HDR), via the “Indices of Deprivation 2015” database. 14
Definitions
Index of multiple deprivation rank (IMDR): this is the quantitative relative measure of deprivation in an area. It is comprised of seven domains: income deprivation, employment deprivation, education, skills and training deprivation, health deprivation and disability, crime, barriers to housing and services, and living environment deprivation. A higher IMDR correlates to a lower level of relative deprivation in a given area. Income rank: this relates to the income deprivation domain. It is the measure of the population whom are out-of-work and have a relatively low income. The higher the rank, the higher the income bracket for that area. Employment rank: this is associated with the employment deprivation domain. Employment rank measures the population unemployed or unable to work due to sickness or disability or caring responsibility. A higher employment rank indicates a greater proportion of employed individuals. Education and skills rank (ESR): this relates to the proportion of population lacking skills. A higher ESR indicates a greater proportion of skilled and educated individuals. Health and disability rank (HDR): this measures the impairment of quality of life due to mental or physical health. A higher HDR indicates a lower proportion of individuals suffering from mental or physical health within the area. Uptake/participation in screening: uptake of CRC screening was defined as individuals participating in the FOBT and returning the samples to the laboratory. Clinical Commissioning Group (CCG): a clinically led organising body responsible for the planning, commissioning and delivery of the healthcare services required in their local population. All GPs will belong to a CCG. Trust: a Trust provides the care that the CCGs commission. They include primary and secondary care services. All GPs will belong to a Trust.
Statistical analysis
The percentage of patients participating in FOBT screening was calculated per Trust, CCG and postcode (Supplementary Material). A Spearman’s rho correlation was performed to quantify the impact of each deprivation variable on FOBT uptake, separately per CCG. Statistical significance was set at a p value of under 0.05. The Kruskal–Wallis test was used to compare the IMD decile across the five CCGs in London. All analyses were carried out using SPSS, version 14.0 (SPSS, Inc., Chicago, IL, USA).
Results
Overall, 697,402 individuals were eligible for screening across 1359 London GPs within the 30-month time period. Of these, 337,364 (median: 48.4%, range: 13%–74%) patients participated in the FOBT screening (Table 1). The median number of individuals per GP practice eligible and participating in the FOBT screening was 421 and 192, respectively. The range of the number of patients eligible and participating was 10–3373 and 5–1383, respectively. Participation across the five CCGs in London ranged from 47% to 52%. North West London had the lowest participation rate with 46%; in contrast, South West London showed a participation rate of 52% (Table 1). Figure 1 represents the participation rates by postcode region. Postcodes ‘W1F’, ‘SW1P’ and ‘CR9’ noted a participation rate of under 30%. Apart from the aforementioned postcodes, ‘W5’, ‘SW5’ and ‘SW1X’ were the only postcodes highlighting a participation rate of less than 35%. A majority of postcodes in the South East of London demonstrated a participation rate of 45%–49.99%. ‘EC3N’, ‘N6’, ‘N20’, ‘N21’ and ‘SW14’ reported a participation rate of over 55%, closer to the national average.
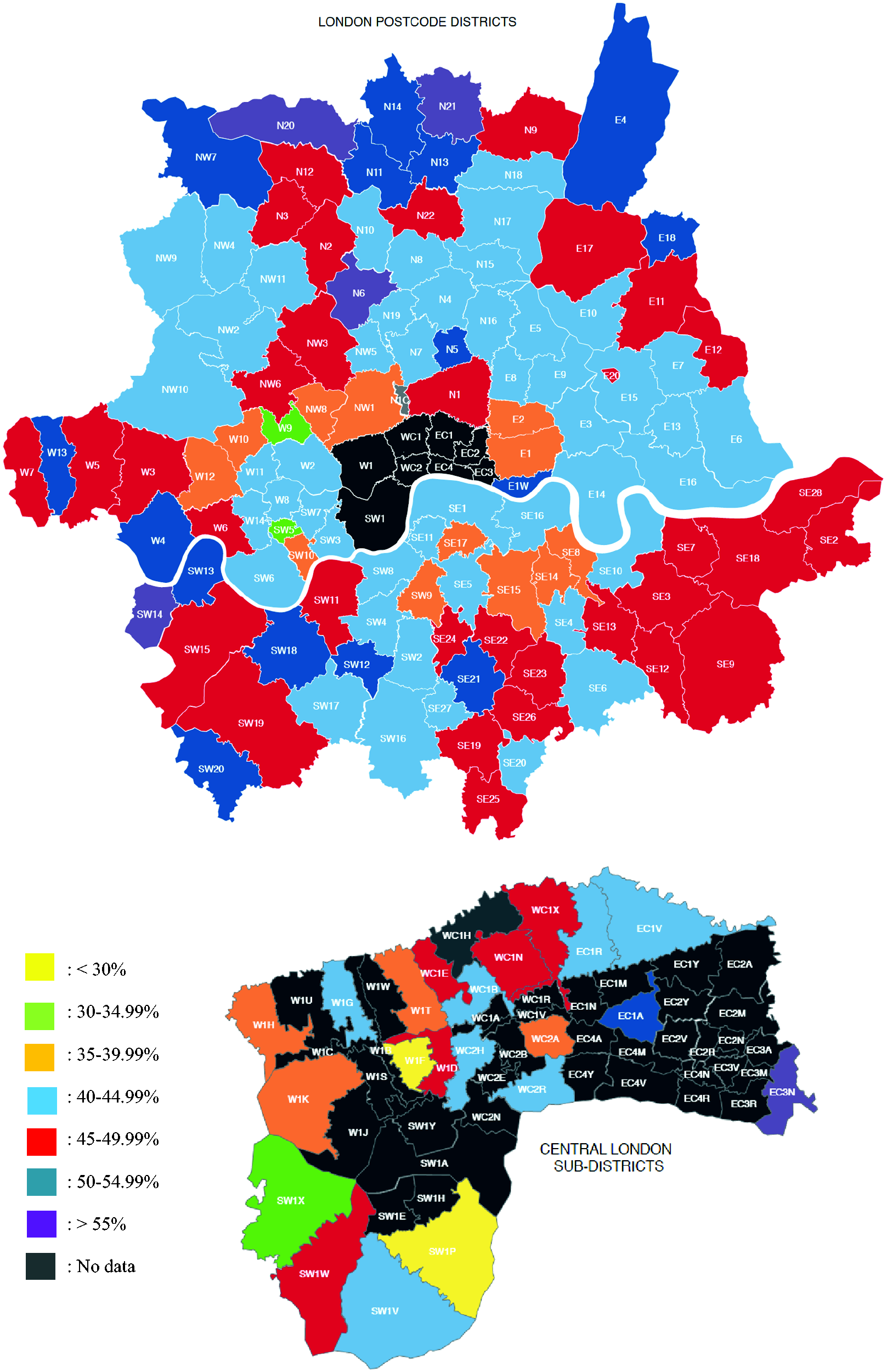
Participation rates across London postcodes.
A significant positive correlation (p < 0.001) was demonstrated between the uptake of screening and IMDR (r = 0.525), income rank (r = 0.457), employment rank (r = 0.426), ESR (r = 0.309) and HDR (r = 0.449) across all five London CCGs (Table 2). This was despite varying levels of deprivation across all areas (Table 3).
Summary of the impact of deprivation on CRC screening uptake at CCG level.
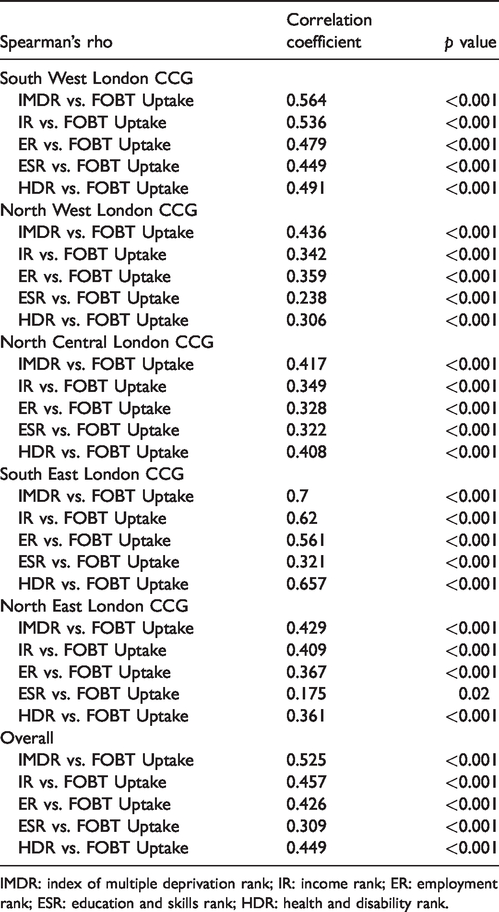
IMDR: index of multiple deprivation rank; IR: income rank; ER: employment rank; ESR: education and skills rank; HDR: health and disability rank.
Median index of multiple deprivation (IMD) decile in the five London CCGs.
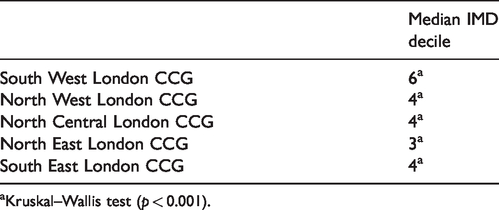
aKruskal–Wallis test (p < 0.001).
Discussion
Our retrospective review of 697,402 patients shows that the uptake rate of CRC screening was 48.4% across London over a period of 30 months. The study was based in London due to its urban, ethnically diverse and large population. Our results are in accordance with other recent studies. Hirst et al. 17 noted a participation rate of 51.68% in the UK from 2010 to 2015; meanwhile, studies in Europe have all reported a similar participation rate.18,19
In addition, our data confirm a significant impact from socioeconomic deprivation (IMDR, income rank, employment rank, ESR and HDR) on the uptake of FOBT (p < 0.01) in our London population. Although the association is not a novel one, it has never been studied in London specifically, nor have particular postcodes (‘W1F’, ‘SW1P’ and ‘CR9’) or CCGs (North West and North East) that require targeting due to particularly low uptake rates been identified. This is important as it allows for further strenuous health promotion in these specific areas.
However, it is imperative to note the varying participation across London. Participation in affluent areas such as ‘Richmond’ was 55% (closer to the national average of 52% 17 ) with other affluent areas (e.g. ‘Westminster’) reaching a rate of only 40%. This highlights the need to understand other factors that may affect uptake of CRC screening. For example, employees in affluent areas being offered screening through workplace programmes may impact on the results. 20
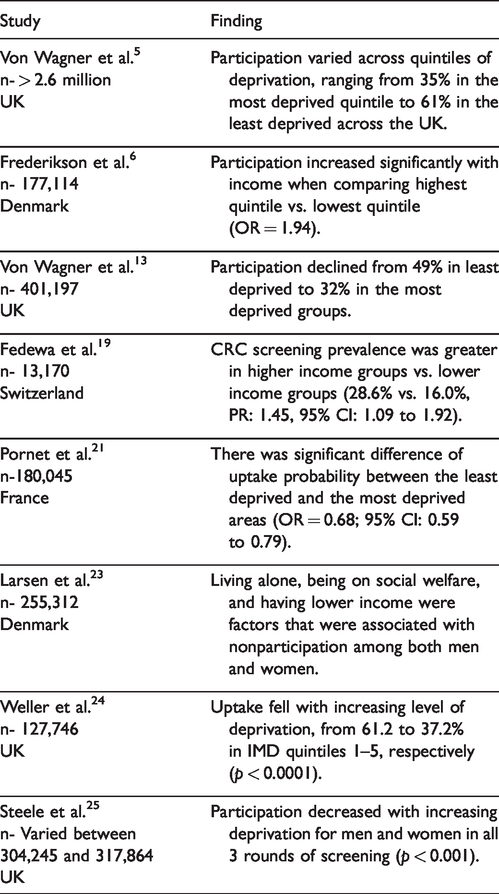
Previous similar studies in the field have been of a substantially smaller sample size18,19,21 (except for Von Wagner et al. 5 who analysed uptake of screening across the UK in over 2.6 million individuals). Some of these studies are summarised in Table 4. With almost 700,000 patients, our study is the largest to evaluate the impact of socioeconomic deprivation on CRC screening in London. The use of the “Vanguard RM Informatics” database, rather than questionnaires, eliminated the risk of classification and information bias. In addition, our study is methodologically superior to self-reported studies, which have a greater risk of recall bias. Previous studies have focused only on the IMDR to assess deprivation. Our study encompassed other related aspects such as income, occupation, education and health. Hence, it provides a more accurate and comprehensive review of overall and individual dimensions of social class with regard to the uptake of CRC screening. 22
Studies evaluating the impact of socioeconomic deprivation on participation in CRC screening.
The decrease in uptake of CRC with an increase in socioeconomic deprivation is aggravated by the increase in prevalence of CRC in deprived areas 26 and worse outcomes. 8 The pathways by which socioeconomic deprivation can affect uptake are complex and poorly understood.27–29 Greater unemployment and lower incomes mean increased life stressors, prioritisation of other activities and fewer coping mechanisms. 27 A lack of education is linked to poorer “health literacy” that is a lack of education around cancer susceptibility, potential serious consequences of cancer, and an awareness of the presence and long-term benefits of screening. 29 It is also linked to poor information seeking behaviour 15 and difficulties in understanding the instructions for FOBT, and therefore decreased participation. 30 In fact, health literacy is associated with a lower probability of screening uptake in univariate and multivariate models, and contributes to nearly 8% of inequality.31,32 In addition, individuals in the lower socio-economic groups display poorer health behaviours 28 and greater fear and fatalism regarding the consequences of being diagnosed with cancer. 27
With the disparities noted in uptake of cancer screening with regard to socioeconomic deprivation, it is imperative to focus future secondary prevention and health promotion on strategies that will address the aforementioned reasons. Some studies have focused on interventions to combat the effect of socioeconomic deprivation. These include the ASCEND trial which showed that reminder letters to individuals who had not responded to the first invitation reduced the socioeconomic deprivation gradient (measured as IMDR) in participation rates. 16 Interestingly, they noted that GP endorsement letters raised the overall participation rates with no significant impact with regard to socioeconomic deprivation. 16 The effect on individual deprivation deciles was not studied.
Other studies have looked into the effect of GP endorsement letters, 33 step-by-step/narrative leaflets33,34 and personally delivered health promotion in the individual’s first language through face-to-face and telephone conversations. 35 Leaflets or ‘gist based’ material along with the invitation improve both the knowledge of patients and attitudes and beliefs towards CRC screening which would enhance their likelihood to take part.33,34 Although there was improvement in uptake, none of these studies33–36 noted a reduction in the socioeconomic gradient, which is in keeping with results from ASCEND. 16 Wardle et al. 16 described this as due to the interventions only affecting the determinants of intention and not the determinants of action.
GPs in London implemented the use of endorsement and reminder letters in June 2016. 37 Unfortunately, our data have not completely captured the impact of this particular intervention. Our findings together with the observed persistent variation in uptake of CRC screening despite this intervention would suggest further scope for individual-based interventions. Promotional interventions will need to vary between subpopulations to ensure equal optimal outcomes as the use of widespread endorsement and reminder letters may not be effective for individuals with poor literacy or language barriers. Therefore, an intervention tailored to the subpopulation in question with a combination of GP endorsement letters in a multi-lingual format, personal telephone or face-to-face promotion and education could prove to be more effective. The ACE programme supported by Cancer Research UK is currently exploring some of these interventions. 38
Others have proposed that the barrier in uptake lies within the screening programme itself. The idea of a ‘one stop’ clinic, similar to breast cancer screening, which would offer multiple screening tests at the same time and location to improve participation amongst patients, has been proposed. 39 Although acceptable to patients, the influence such a clinic would have on enhancing CRC screening participation overall and in terms of socioeconomic deprivation is currently unclear. 40 Even changing the investigation of choice for screening has been looked at as an avenue to improve uptake rates. Pilot studies utilising faecal immunochemical testing (FIT) for CRC screening have shown an improvement in uptake by as much as 11.4% compared to FOBT. 17 This in part may be attributed to easier use; only a single specimen is required and it is more hygienic. However, socioeconomic disparities persist with the use of FIT, 23 and therefore we believe changing from FOBT to FIT will not offer a long-term solution to the impact of socioeconomic deprivation on health equity.
Our study has a few methodological limitations. There were no data reported on age, sex and ethnicity of the patients invited for CRC screening. Therefore, a multivariate analysis combining the aforementioned variables was not possible. Instead of individual-level measures, an area-based measure was used to collate deprivation data. A postcode-dependent IMDR may not be reflective of all individuals, especially in London where the gradient of affluence even in small areas is large. Geodemographic segmentation may be a better method of determining regional inequalities and consideration of its use in the future is prudent. Moreover, only the percentage of patients participating in CRC screening from every GP was available, rather than the participation status of each individual patient. Hence, it is not possible to precisely assess the true extent of the health inequality; the true association between socioeconomic deprivation and uptake of CRC screening may be in either direction due to ecological fallacy. We included patients aged 60 to 69, but in England the BCSP has been recently extended to incorporate patients up to the age of 74. This may in fact exacerbate the health inequality, as studies have highlighted a significant reduction in participation rates in the older population. 5 Therefore, continuing work is imperative to evaluate the impact of socioeconomic deprivation on the age group invited for CRC screening.
Conclusions
This is the largest study to date demonstrating a significant correlation between deprivation indices and compliance with the BCSP in London. In addition to IMDR, our study evaluated the impact of education, income and employment on CRC screening uptake, and identified postcodes with uptake rates below the national average that should catapult respective CCGs into action. We believe that a change to FIT will not address this inequality and that focus should be placed on introducing strategies to reduce attitudinal and educational barriers in the high-risk areas. It is essential to enhance health literacy to relieve patients of any misconceptions about cancer screening; to highlight the importance of screening as a priority inspite of financial and social instability; and to boost their confidence in their ability to undertake screening. Enhancing health literacy may require improved modalities of communication and increased contact with healthcare professionals.
Supplemental Material
MSC916206 Supplemental Material - Supplemental material for The impact of socioeconomic deprivation on the uptake of colorectal cancer screening in London
Supplemental material, MSC916206 Supplemental Material for The impact of socioeconomic deprivation on the uptake of colorectal cancer screening in London by Nikhil Lal, Harpreet KSI Singh, Azeem Majeed and Nikhil Pawa in Journal of Medical Screening
Footnotes
Acknowledgements
We would like to acknowledge RM partners for allowing access to their informatics database and for their review of the manuscript submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.