
Abstract
Objective
In 2017, the Australian National Cervical Screening Program changed from two-yearly Pap smears between ages 18 and 69, to five-yearly human papillomavirus screening between ages 25 and 74 (the “Renewal”). This study investigated attitudes towards the changes, among individuals previously affected by cervical abnormalities/cervical cancer, personally or through a friend/relative.
Methods
We conducted a thematic analysis of comments expressing personal history or a family/friend history of cervical abnormalities/cervical cancer as a reason for opposing changes to the cervical screening program. The comments were taken from a 20% random sample of 19,633 comments posted on the “Change.org” petition “Stop May 1st Changes to Pap Smears – Save Women's Lives” in February–March 2017.
Results
There were 831 (20.8%) commenters who reported that they were concerned about a change in screening due to: feelings of increased personal vulnerability to cervical cancer due to their own personal history of cervical abnormalities; comparison of extended screening intervals and later age of first screening to their own experiences; and a perception of increased personal risk due to family history.
Conclusion
Women previously affected by cervical abnormalities or cervical cancer, personally or through a friend/relative, expressed concern about changes to cervical screening due to perceived increased risk and feeling vulnerable due to personal history.
Introduction
In December 2017, the Australian National Cervical Screening Program (NCSP) changed from cytology (Pap testing) to human papillomavirus (HPV) testing, increased the age of first invitation to screen, and extended the screening interval. These changes were known as the “Renewal”. When the changes were announced, a “Change.org” online petition: “Stop May 1st Changes to Pap Smears – Save Women’s Lives”, attracted 70,000 signatures in just a few weeks, one of the biggest petitions on that site that year. Many of those who expressed opposition to the changes referred to a history of cervical abnormalities or cancer. 1 This study aimed to examine their views in more detail. While some previous studies have linked cervical abnormalities and family history with perceptions of vulnerability and increased risk perception of cervical cancer, other studies have failed to detect a relationship between the perception of cervical cancer risk and screening behaviour. A review concluded that quantitative measures do not sufficiently capture an individual’s complex feelings and perceptions of cervical cancer risk. 2 As the lifetime chance of an abnormal Pap smear in cervical screening programs is high (26%), a large number of women potentially fall into this category. 3 This study aimed to analyse reactions to the renewal of the NCSP among those reporting a history of cervical abnormalities or cervical cancer themselves, or in a person close to them (friend or family).
Methods
Through February and March 2017, 19,633 comments were posted to the “Change.org” petition. A random sample of 2000 of these comments, in response to the prompt, “I am signing this petition because …” has been analysed in our previous publications.1,4 Our previous publications demonstrated, through content analysis, that the main concerns for commenters were about missing cases of cervical cancer, due to increased screening interval, and later age of invitation to screen. In addition, 22% of the 2000 comments analysed cited a history of cervical abnormalities or cervical cancer, themselves or in a person close to them (friend or family), as the reason for their opposition to screening changes. 1 We analysed an additional random sample of 2000 comments (total 4000 comments), looking only for comments referring to a history of cervical abnormalities or cervical cancer in the commenter themselves, or in a person close to them (friend or family). These comments were analysed using thematic analysis to understand in-depth the attitudes and perspectives of commenters with a history of cervical abnormalities or cervical cancer themselves or in a person close to them (friend or family). Thematic analysis is a research method used to report patterns or themes within a dataset, by organising, describing and interpreting the content. 5 This method was used in this study by identifying comments related to a history of cervical abnormalities or cervical cancer themselves or in a person close to them (friend or family), and searching for and describing themes within this dataset. This analysis presents results which were more prevalent or concentrated in this group of comments.
Results
From the randomly selected 4000 comments, 831 (20.8%) independent commenters expressed opposition to the renewal of the NCSP due to a history of cervical abnormalities or cervical cancer themselves or in a person close to them (friend or family). Of these, 559 (67.3%) comments discussed a personal history of cervical cancer or cervical abnormalities or cervical cancer, and 292 (35.1%) discussed a personal history of cervical abnormalities or cervical cancer in a person close to them (friend or family) as their reason for opposing the changes. In 20 comments (2.4%), the commenters described both a history of cervical abnormalities or cervical cancer in themselves and also in a person close to them (friend or family). The present analysis identified three themes of key importance to this sub-sample describing personal experience, presented with representative quotes in Table 1.
Main themes and example quotes extracted from comments posted to the “Change.org” petition expressing personal or family/friend history of cervical cancer or cervical abnormalities.
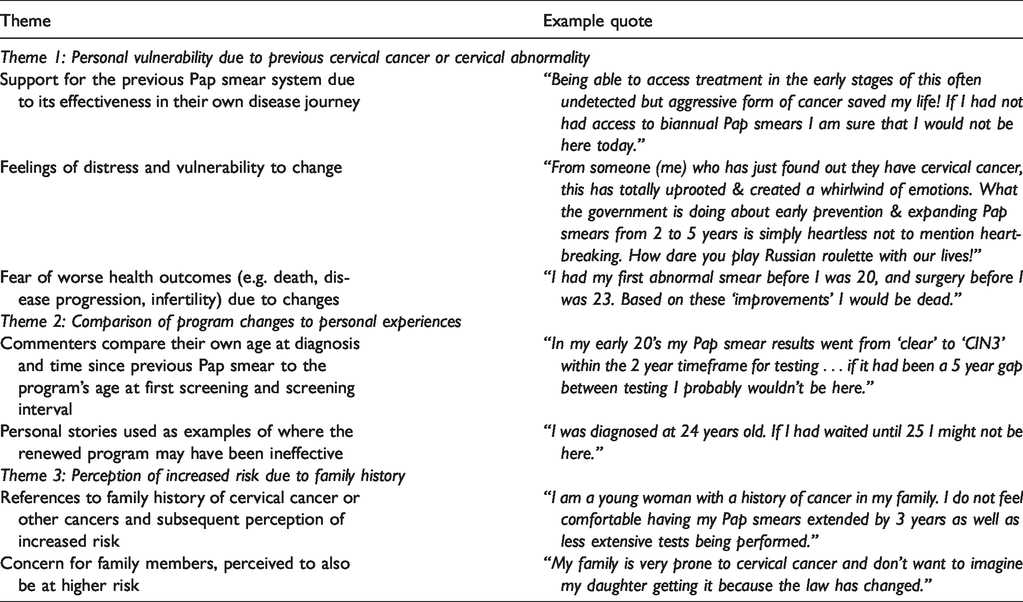
Among the one in five commenters who were opposed to the changes due to personal experience, in-depth analysis found that these women felt particularly vulnerable to the changes due to their confidence in the previous screening program, and perceived potential negative consequences of a change, such as later diagnosis, progression of disease and death. They compared their own stories with what they may have experienced under the renewed screening program, and used their personal experiences as evidence of the potential dangers when changing the invitation age or interval of screening. Commenters also identified family history as a major concern, and argued for more frequent and earlier screening on this basis. For this sub-sample, the previous Pap smear screening program was seen to have prevented their death, or that of a friend/family member, from cervical cancer, and they perceived it as an injustice by the healthcare system that a life-saving test should be taken away from them.
Discussion
The feelings of personal vulnerability demonstrated by this group indicate that additional reassurance and education about the changes may be required in this program, but may also apply in other cancer screening programs that are modified. Previous work has described risk adjusted approaches to screening, with high-risk women invited by their GP, rather than the overarching screening program, allowing greater personalization. 6 Another study demonstrated that particularly those women with previous cervical abnormalities wanted to be actively involved in the decision-making surrounding their cervical cancer screening. 7 A more personalised approach, in combination with more informative education about the reasons for changes to screening age and interval, may need to be considered by public health authorities, given the feelings of personal vulnerability evident from the findings of this study.
Comments to this petition indicate that a diagnosis of cervical cancer or cervical abnormalities has a long-lasting effect on perception of personal risk, and that women see themselves as cancer survivors, even if their diagnosis was of a pre-cancerous cervical abnormality. 8 While HPV screening does not apply to those with current or recent diagnoses of cervical abnormalities or cervical cancer, under the renewed NCSP, those women treated for cervical abnormalities resume the normal five-yearly screening after two negative co-tests (cytology plus HPV), 12 months apart. 9 This separate pathway may not yet be well known or understood, and the difference between screening and testing in those with previous abnormalities was not mentioned in any of the comments analysed. While we cannot identify the exact sources of misinformation and risk perception for the commenters to the petition, the two-year interval between treatment for abnormalities and resumption of normal population-level screening may not be perceived as long enough for women who feel they are at increased personal risk due to a recent diagnosis of cervical abnormality and need more reassurance. This may need to be taken into consideration when communicating to women about the post-treatment surveillance interval.
Previous literature has shown inconsistent results about the effects of a prior abnormal cancer screening test experience on attitudes towards future screening. 2 The inconsistency may be explained by the difference in the source of fear; while fear of screening itself may lead to avoidance, greater cancer worry can predict increased screening and intention to screen in order to reduce the threat of cancer. 10 A retrospective register-based cohort study demonstrated that those with a history of cervical abnormalities or any cancers had increased rates of adherence to screening. 11 Furthermore, two recent studies surveying patients about barriers to screening participation and willingness to extend screening intervals found that those with a history of abnormal Pap smears were less likely to accept less frequent screening.12,13 Our study is consistent with the literature in this area and suggests that those with a personal or family/friend history of cervical cancer/cervical abnormalities may be reluctant to support less regular screening, even more so than the general population.
We examined reasons for opposition to the renewal of the NCSP by women with a history of cervical cancer or cervical abnormalities, and give an understanding of particular concerns that may need to be addressed by screening services. As this petition was one of the largest Australian petitions on “Change.org” in 2016 and 2017, high public interest is apparent. 14 Given ethical constraints regarding the use of commenter’s data, we were unable to verify whether comments were from those with a genuine medical history of cervical cancer or cervical abnormalities or not. However, two previous studies have shown that women with no medical record history of cervical abnormalities do not tend to self-report cervical abnormalities.15,16 As these comments are taken from a petition opposing the changes, they may represent a vocal minority who feel passionately about the changes.
Conclusion
These findings could inform further research to identify and address concerns in this cohort of women, and more generally to develop strategies for more tailored education about screening changes in the future for those who have a history of an abnormality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.