
Abstract
Objectives
Flexible sigmoidoscopy screening at around age 60 can reduce colorectal cancer incidence. Insufficient evidence exists on flexible sigmoidoscopy at age 60 in a population being offered biennial faecal occult blood test screening from age 50. This randomized controlled trial assessed if flexible sigmoidoscopy would be an effective adjunct to faecal occult blood test.
Methods
In the Scottish Bowel Screening Programme between June 2014 and December 2015, 51,769 individuals were randomized to be offered flexible sigmoidoscopy instead of faecal occult blood test at age 60 or to continue faecal occult blood test. Those not accepting flexible sigmoidoscopy and those with normal flexible sigmoidoscopy were offered faecal occult blood test. All with flexible sigmoidoscopy-detected neoplasia or a positive faecal occult blood test result were offered colonoscopy.
Results
Overall flexible sigmoidoscopy uptake was 17.8%, higher in men than women, and decreased with increasing deprivation (25.7% in the least to 9.2% in the most deprived quintile). In those who underwent flexible sigmoidoscopy, detection rate for colorectal cancer was 0.13%, for adenoma 7.27%, and for total neoplasia 7.40%. In those who underwent colonoscopy after a positive flexible sigmoidoscopy, detection rate for colorectal cancer was 0.28%, adenoma 8.66%, and total neoplasia 8.83%. On an intention to screen basis, there was no difference in colorectal cancer detection rate between the study and control groups. Adenoma and total neoplasia detection rate were significantly higher in the study group, with odds ratios of 5.95 (95%CI: 4.69–7.56) and 5.10 (95%CI: 4.09–6.35), respectively.
Conclusions
In a single screening round at age 60, there was low uptake and neoplasia detection rate. Flexible sigmoidoscopy detected significantly more neoplasia than faecal occult blood test alone.
Keywords
Introduction
Three randomized controlled trials (RCTs) have demonstrated that a single flexible sigmoidoscopy (FS) between ages 55 and 64 results in statistically significant and clinically substantial reductions in both mortality and incidence of colorectal cancer (CRC).1–3 While some of the mortality reduction may be due to early detection of invasive cancer, the main effect, certainly on incidence, results from the identification and removal of precursor lesions (adenomatous polyps). 4 The United Kingdom (UK) National Screening Committee in 2011 recommended the addition of FS at age 55 to the NHS Bowel Cancer Screening Programme in England, 5 which was based on biennial guaiac faecal occult blood testing (gFOBT) offered between ages 60 and 74.
The Scottish Bowel Screening Programme (SBoSP) was introduced following three pilot screening rounds from 2000 to 2007 and was fully rolled out across every NHS Board in Scotland by the end of 2009. It used biennial gFOBT offered between ages 50 and 74, with a qualitative faecal immunochemical test for haemoglobin (FIT) for those with a weak positive gFOBT result. This two-tier reflex algorithm (described elsewhere 6 ) is referred to here as faecal occult blood test (FOBT). In November 2017, FOBT was replaced by quantitative FIT. 7 When FS was introduced in England it was decided not to do the same in Scotland, as FOBT was being offered from age 50, rather than 60 as in the other UK nations, and because no evidence existed regarding the effectiveness of FS in a population that was already being offered biennial FOBT. However, given the clear effectiveness of FS in a screening naïve population, a randomized evaluation of a single FS at age 60 (the mean age of participants in the previous RCTs) as an adjunct to the existing FOBT programme was performed. One rationale for this was the absence of an effect of FOBT on the incidence of CRC. 8
Methods
The study tested the primary hypothesis that offering a FS at age 60 in addition to FOBT would result in a significant additional yield of colorectal neoplasia. Other end-points were uptake of FS and the effect of offering FS on the overall uptake of screening.
Between 19 June 2014 and 15 December 2015, 51,769 individuals aged 59, 60, or 61 in four NHS Boards (Fife, Grampian, Greater Glasgow and Clyde, and Tayside), and identified by their unique community heath index 9 as eligible for FOBT screening were randomly assigned to study and control groups. Those in the study group (n = 25,851) were offered FS at their scheduled screening invitation. Those in the control group (n = 25,918) continued being invited using the usual screening algorithm. Random allocation to the study group was carried out with a modification to the existing Bowel Screening Scotland IT System. (For details of the study pathway, please see online appendix.)
Individuals allocated to the study group were sent a pre-notification letter, followed two weeks later by a letter inviting them to attend for FS at the scheduled invitation to participate in the SBoSP closest to their 60th birthday. They were also sent a Participant Information Leaflet describing the study procedure, with local contact details. This information was developed by Health Information Scotland using focus groups and extensive user testing. Participants could contact the study team if they had any questions regarding participation and were asked to return a reply slip, using an included stamped addressed return envelope, to indicate that they wished to take part. If no response was received, a reminder letter was sent after 14 days.
Attendance for FS was in the local endoscopy unit within a target of four weeks of the invitation. Potential participants were first given an opportunity to discuss the study and FS with a specialist nurse, who also carried out pre-assessment regarding suitability for FS. Informed consent was then obtained using a FS consent form accompanied by written information about the study and FS. Participants were given an appointment date and an enema to be used at home 4 h before FS. FS was carried out by an NHS endoscopist (medical, surgical, or nursing). Standard operating procedures were used to ensure that the FS was performed across the endoscopy units involved in as uniform a manner as possible. FS was defined as large bowel endoscopy carried out without sedation until solid faeces, pathology, or subject intolerance of the procedure required termination. Although reaching the splenic flexure was regarded as optimal, this was not mandated, to avoid causing discomfort from over-zealous endoscopy.
Those who did not accept the invitation for FS were immediately invited to FOBT screening. Those who did not respond to the invitation for FS were invited to FOBT screening within three months. Those who had a normal FS were immediately issued a FOBT to offer screening for the right colon.
Colonoscopy was offered to all with a positive FOBT result, and to those in whom any adenoma (or serrated epithelial polyp of 10 mm diameter or more) was found on FS, even if it was removed, as this was the usual standard of care to ensure inspection of the entire large bowel. Those who had had polyps removed were offered a FOBT immediately, and if the polyps were found to be non-neoplastic, colonoscopy was only offered if the FOBT result was positive, as non-neoplastic polyps were not considered as an indication for colonoscopy. Individuals found to have invasive CRC at FS were referred immediately for complete colonoscopy, surgical assessment, and staging.
FS was carried out using a standard therapeutic Olympus® colonoscope with a magnetic endoscope guide to allow visualization of the position of the colonoscope within the abdomen. If possible, any small polyps (up to 7 mm) were removed using cold snare. Larger polyps were removed at subsequent colonoscopy. Lesions thought to be CRC were biopsied and the participant referred for surgical assessment and work up, including colonoscopy. Standard data from each FS, including duration of procedure, adequacy of bowel preparation, level of patient discomfort, details of abnormality encountered, any procedures performed, extent of insertion of endoscope as estimated by the guide, and any complications, were recorded on a study database, in addition to that in use at the endoscopy unit. These data were recorded as hard copy and transferred to a secure electronic database held by the Information Services Division of National Services Scotland.
All polyps were sent for histological examination locally, and the findings recorded on the database using the standard SBoSP proforma. The designated study pathologists (one per centre) were experienced in screening pathology and participated in the UK Bowel Screening Pathology External Quality Assurance Programme. Quality of data entry was checked by one of the authors (FAC), who reviewed the pathology of all FS-detected cancers across the study. In addition, the pathology of all FS positives in Tayside was reviewed, as access to the relevant findings was feasible only in that NHS Board.
The population-weighted deprivation quintile of the participants in the study was assessed using the Scottish Index of Multiple Deprivation (SIMD) based on post-code. 10
Results
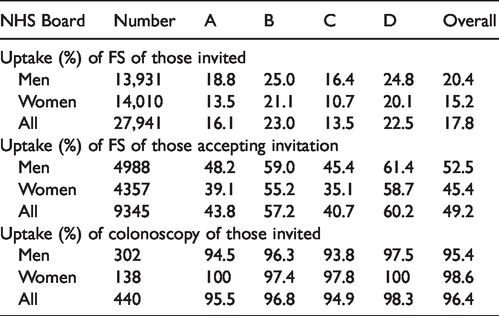
Figure 1 is a flow chart describing numbers invited and uptake in both arms of the trial. Overall uptake, defined as the percentage of those invited (n = 25,851) who underwent FS was 17.8% (n = 4597). The uptake of FS among those who had accepted the invitation (n = 9345, 36.2%) was 49.2%. As shown in Table 1, these varied by NHS Board. Of those with a positive FS (adenoma, serrated lesion ≥10 mm, or CRC), (n = 440), 96.4% went on to have a colonoscopy (Table 1). As shown in Table 2 and Figure 2, uptake of FS was higher in men (20.4%) than women (15.2%), and varied with deprivation index, from 9.2% in the most deprived quintile (SIMD 1) to 25.7% in the least (SIMD 5). The uptake of FOBT in the control group was 46.4% in SIMD 1 and 69.1% in SIMD 5 (Table 3 and Figure 3). The deprivation gradient for uptake of FS was significantly different from that for uptake of FOBT (p = 0.02), with uptake of FOBT having a steeper gradient (5.66 for FOBT compared with 4.09 for FS).
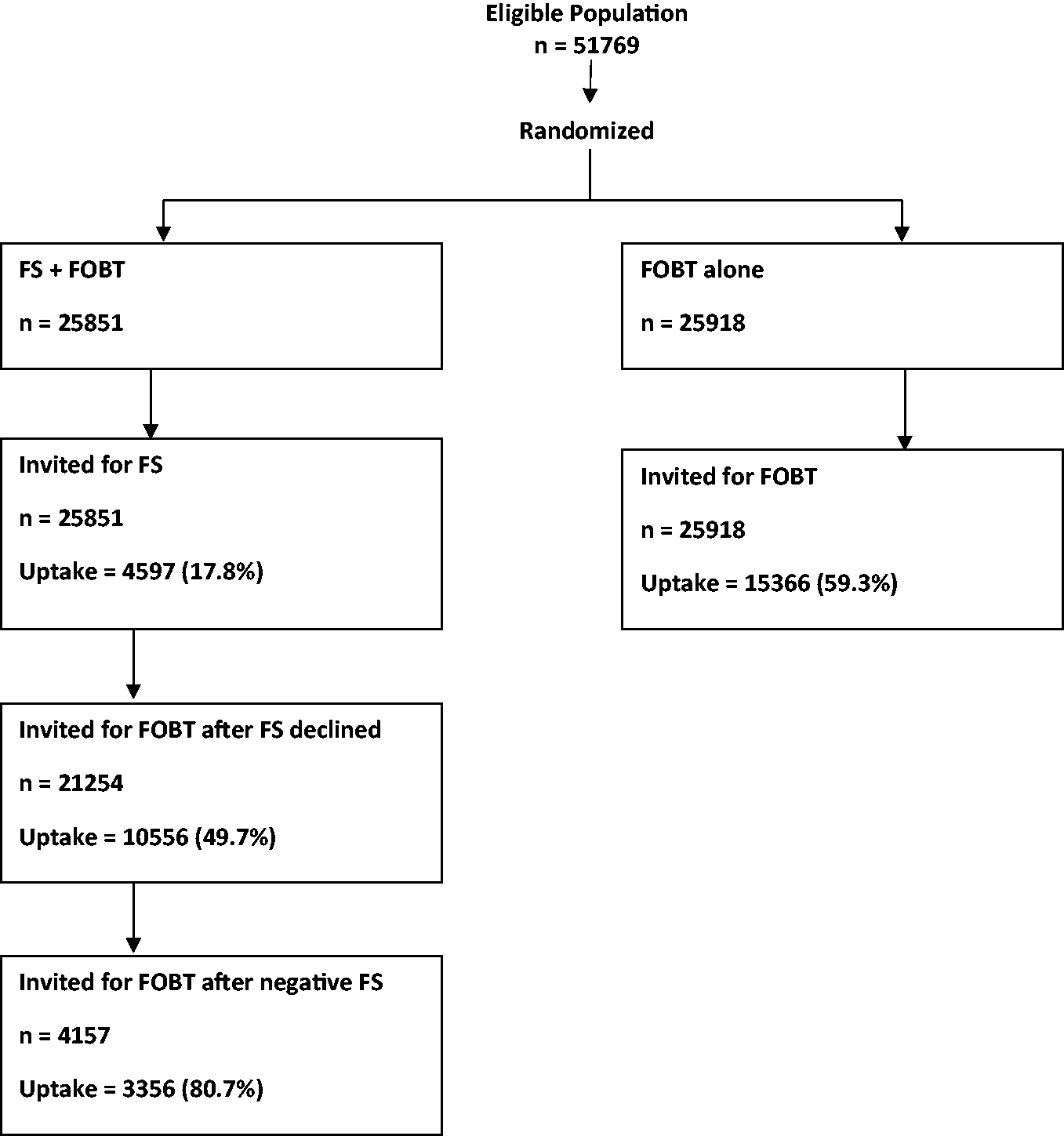
Flow chart documenting numbers invited and uptake in both arms of the RCT.
Uptake (%) of flexible sigmoidoscopy (FS) and subsequent colonoscopy in the study group by NHS Board (A–D) and overall.
Uptake (%) of FS in the study group by sex and Scottish Index of Multiple Deprivation (SIMD).
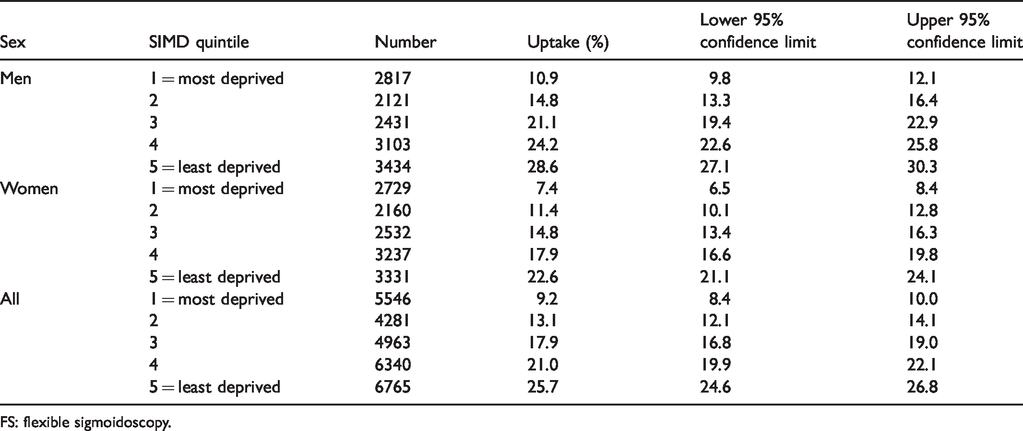
FS: flexible sigmoidoscopy.
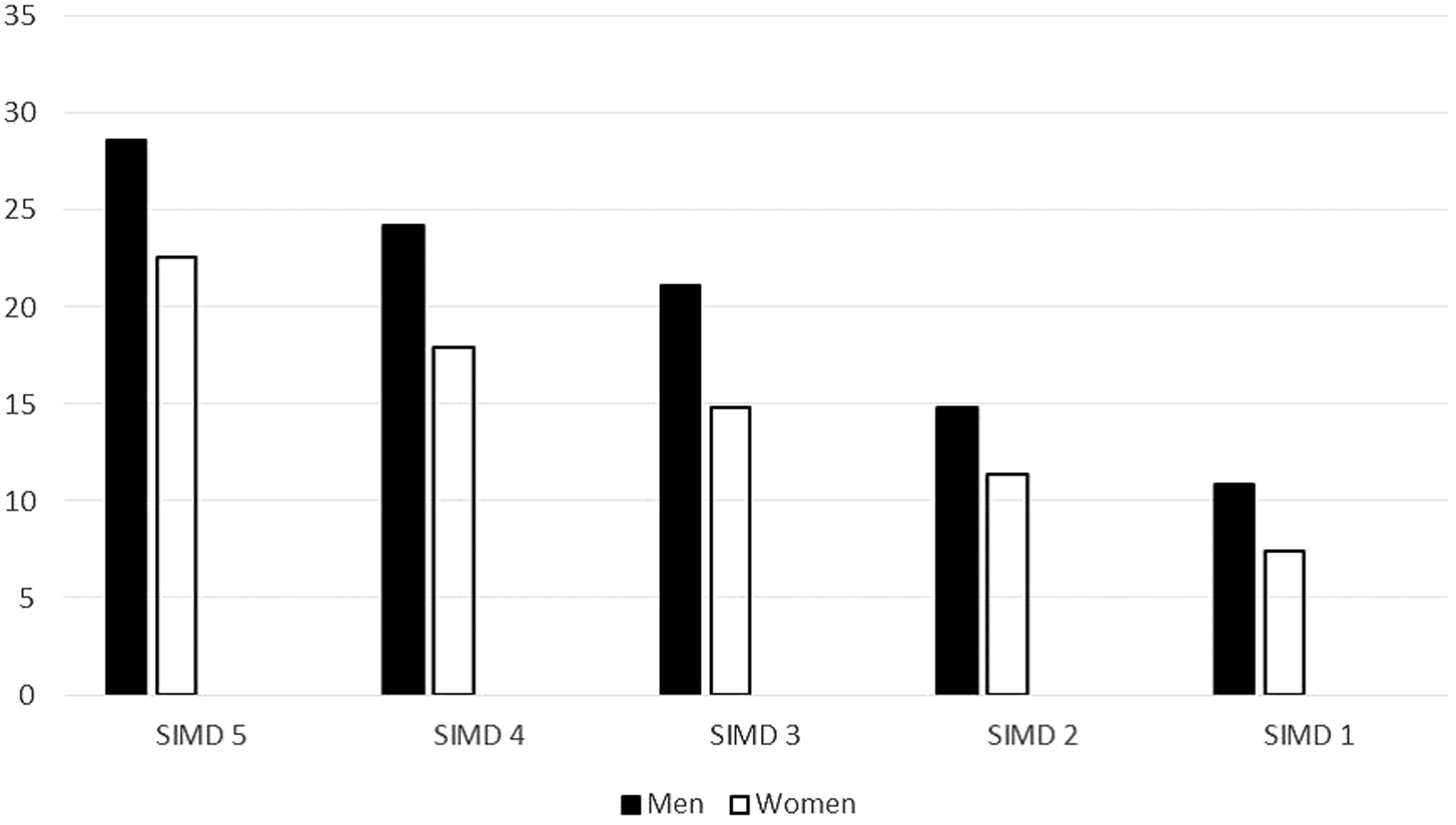
Uptake (%) of FS in males and females by SIMD (SIMD 5: least deprived, SIMD 1: most deprived).
Uptake (%) of FOBT in the control group by sex and Scottish Index of Multiple Deprivation (SIMD).
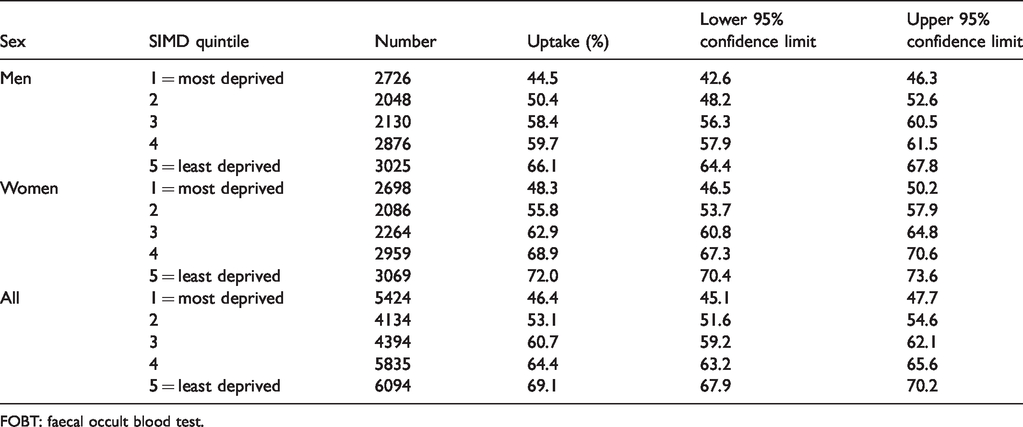
FOBT: faecal occult blood test.
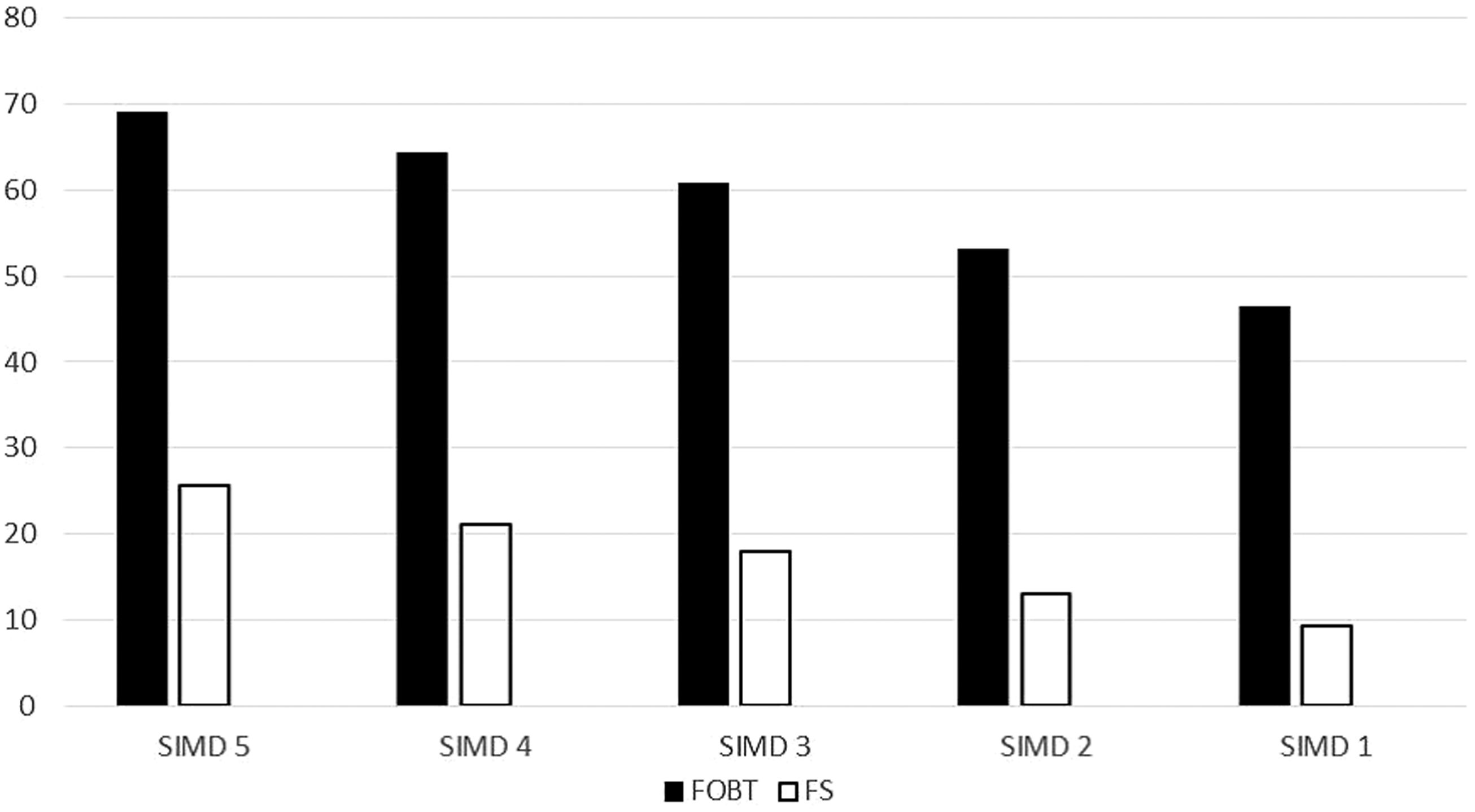
Overall (males and females) uptake (%) of FOBT (control group) and FS (study group) by SIMD. This illustrates an absolute difference between the most and least deprived of 22.7% for FOBT and 16.5% for FS, and the differences between the deprivation gradients for FS and FOBT are statistically significant (p = 0.02 using analysis of covariance to compare two regression lines).
The uptake of FS was examined by screening history; overall, 8.8% of those undergoing FS had declined participation in any previous round of FOBT screening, and 14.1% had not participated in the round immediately prior to that in which FS was offered (Table 4). To determine the effect of offering FS on the overall uptake of screening, the study and control groups were compared with respect to either form of screening (FS or FOBT in the study group and FOBT only in the control group). The uptakes were 58.6 and 59.3% in study and control groups; these were not different (p = 0.121) (Table 5).
History of faecal occult blood test (FOBT) screening participation prior to flexible sigmoidoscopy (FS) invitation in those who subsequently underwent FS by sex and overall.
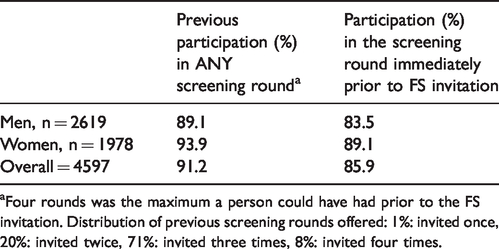
aFour rounds was the maximum a person could have had prior to the FS invitation. Distribution of previous screening rounds offered: 1%: invited once, 20%: invited twice, 71%: invited three times, 8%: invited four times.
Uptake of any screening test in the study and control groups. χ2: 2.403, p = 0.121.
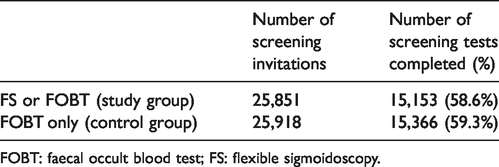
FOBT: faecal occult blood test; FS: flexible sigmoidoscopy.
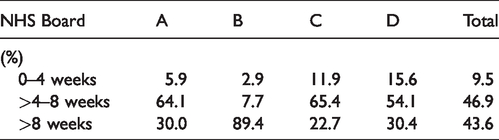
The quality standard of four weeks’ maximum wait between invitation and FS was achieved overall for only 9.5%. Waiting times were between four and eight weeks in 46.9%, and over eight weeks in 43.6%. This varied considerably among the four NHS Boards (Table 6), and one Board (B) withdrew from recruitment to the study in May 2015 owing to workload issues. No complications attributable to FS were reported, and there was only one complication of colonoscopy that resulted in hospitalization (a post-polypectomy bleed that did not require intervention).
Waiting times (%) between invitation and performance of flexible sigmoidoscopy.
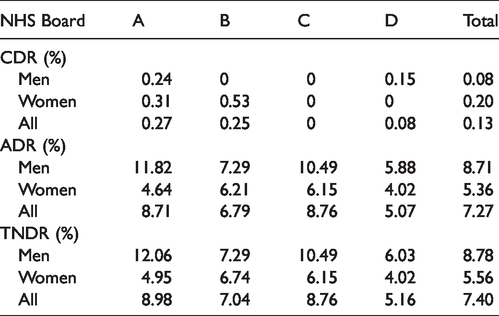
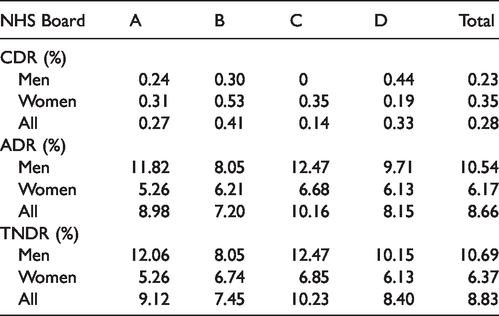
In those who underwent FS, the cancer detection rate (CDR) was 0.13%, the adenoma detection rate (ADR) was 7.27%, and the total neoplasia detection rate (TNDR) was 7.40% (Table 7). In those who underwent FS and colonoscopy in response to a positive FS finding, the CDR was 0.28%, the ADR 8.66%, and the TNDR 8.83% (Table 8). These percentages were different because not all lesions were biopsied at the time of FS, and in such cases, a definitive diagnosis was made only after colonoscopy. Of those who had a negative FS result and, therefore, did not proceed to colonoscopy, uptake of the subsequently offered FOBT was 80.7%, and the positivity was 0.82%. This group comprised 27 individuals, two diagnosed with CRC, and four with adenoma on subsequent colonoscopy. The time between the FS result and issuing the FOBT invitation did not exceed two weeks.
Cancer detection rate (CDR), adenoma detection rate (ADR), and total neoplasia detection rate (TNDR) at flexible sigmoidoscopy by sex.
Cancer detection rate (CDR), adenoma detection rate (ADR), and total neoplasia detection rate (TNDR) at flexible sigmoidoscopy (FS) and subsequent colonoscopy (not all lesions were removed or biopsied at initial FS).
On an intention to screen basis, the CDR was not statistically different in study and control groups. However, both the ADR and TNDR were significantly higher in the study group, with odds ratios of 5.95 (95%CI: 4.69–7.56) and 5.10 (95%CI: 4.09–6.35), respectively (Table 9).
Cancer detection rate (CDR), adenoma detection rate (ADR), and total neoplasia detection rate (TNDR) in the study group and the control group on an intention to screen basis.
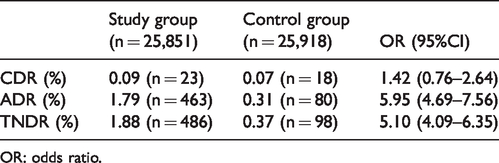
OR: odds ratio.
Discussion
A single FS performed at around age 60 has the potential to be a highly effective population CRC screening modality. Randomized trials in England (the UK Flexible Sigmoidoscopy Screening randomised controlled trial (UKFSST)), 1 Italy (SCORE), 2 and Norway (NORCCAP) 3 have all shown that offering a one-off FS between ages 55 and 64 results in significant and substantial reductions in both mortality from, and incidence of, CRC. In a United States trial, in those aged 55–75, FS offered twice had a similar effect. 11
For FS to have an impact on national CRC mortality and incidence, uptake and yield of neoplasia that approach those of the RCTs must both be achieved. A comparison between the data here and those of the previous RCTs12–15 is given in Table 10. In Scotland, the uptake was well below that of the RCTs, and the ADR was also lower. The reasons for the low uptake in this study are unclear, but there are several possible explanations. Randomization in the UKFSST and SCORE trials was only offered to those who had already expressed an interest in participation and, if those who had expressed an interest did accept an invitation to FS, the uptakes in the RCTs translate to population uptakes considerably lower than those observed. In keeping with this, uptake in the rolled-out FS programme in England has been reported to be about 43%. 16 The very high uptake of 83.5% in the US trial can be explained by the fact that randomization took place after recruitment and consent had been obtained. This makes the population uptake of 63% in the Norwegian trial (NORCAPP) remarkable, and perhaps unachievable elsewhere.
Comparison between previous randomized control trials and study data.
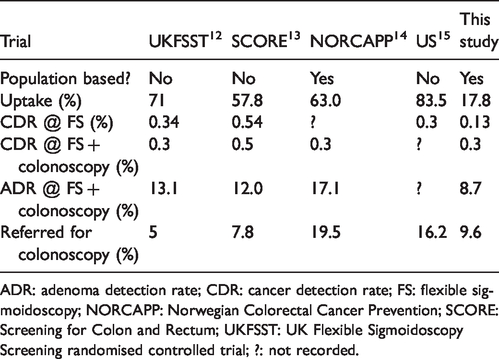
ADR: adenoma detection rate; CDR: cancer detection rate; FS: flexible sigmoidoscopy; NORCAPP: Norwegian Colorectal Cancer Prevention; SCORE: Screening for Colon and Rectum; UKFSST: UK Flexible Sigmoidoscopy Screening randomised controlled trial; ?: not recorded.
However, the fact that randomization was carried out at a population level is unlikely to totally explain the low uptake, especially as an uptake of around 40% has been achieved in the NHS BSCP in England. One possibility is that long waiting times between invitation and performance of the FS may have led to undue attrition, leading to poor eventual uptake. However, although only half of those initially accepting the invitation actually underwent FS, there did not seem to be a link between the uptake in the four NHS Boards (Table 1) and the waiting times (Table 6). This also suggests that many participants did not appreciate the nature of the FS, despite the carefully developed and tested information leaflets provided with the invitations. There may be cultural issues, or other factors, that make FS less acceptable in Scotland than elsewhere. However, in the UKFSST, Glasgow was one of the recruitment centres, then screening naïve, and uptake here among those invited was 62% and, when extrapolated to the whole eligible population, would have been around 24%, 17 well above our observed uptake. Another more likely explanation may be that the established and less onerous FOBT approach may have dissuaded individuals from engaging in what may appeared to be an alternative and more demanding approach.
The reduced yield of neoplastic pathology in this study compared with the RCTs may reflect either the quality of the FS, or the fact that the population undergoing FS had been exposed to FOBT screening for up to four rounds. The ADR varied substantially between NHS Boards (Table 7), suggesting that quality of FS may have been a factor, and, indeed, variation in ADR between endoscopists is well evidenced. 18 It was impossible to assess this objectively in our study as individual endoscopist data were unavailable. Despite the limitations of both uptake and yield of neoplasia, the intention to screen analysis showed a very significant increase in the ADR in the group offered FS, compared with the control group who underwent FOBT screening.
If uptake and ADR could be improved, it is speculated that FS at age 60 superimposed on a FOBT programme (or a programme based on FIT with a faecal haemoglobin concentration cut-off selected to give a similar positivity rate) from age 50 could significantly enhance the effect of screening on CRC mortality and incidence. If FIT were to be employed at a lower cut-off, giving a substantially higher positivity rate than FOBT, this might detract from the added value of FS. This hypothesis would have to be tested by prospective studies. In addition, as FOBT screening is known to be associated with a lower CDR in the proximal colon compared with the distal colon, 19 this also has the potential to dilute the effect of FS.
An important aim of the study was to assess the feasibility of delivering a FS screening programme. From both the waiting times and the inability of one of the NHS Boards to complete the study, introduction of FS into the SBoSP would be a significant challenge. The overall conclusion is that the addition of FS to the SBoSP would be unlikely to have a beneficial effect at a population level, given the observed uptake and current service constraints.
Despite these conclusions, there are messages to take from this study. Offering FS to a population that is already being offered FOBT screening not only increases the yield of adenomas, it also appears to increase choice, as an appreciable proportion (around 9%) who took up the offer of FS had never engaged in FOBT screening. In a study from Italy, offering FIT to non-responders in a FS screening programme increased overall screening uptake. 20 The reverse (offering FS to FOBT non-responders) has not been recorded before, but while this approach appeared favourable, it did not translate into an overall increase in uptake, as the uptake of any form of screening in the control and study groups was so similar, perhaps due to the very small numbers of people accepting the FS invitation.
An additional and germane question would be the effect of FS on the performance of subsequent FOBT screening, which might be considerably diminished by the endoscopic procedure. A recent study in England showed that uptake, positivity, and positive predictive value of gFOBT screening were reduced following prior offer of FS screening. A quarter of FS screened participants receiving a diagnostic examination after positive gFOBT were diagnosed with advanced colorectal neoplasia. 21 As Scotland has now moved to a FIT-based programme, it would be difficult to extrapolate from the former to the current algorithm.
As with all CRC screening studies, we observed variations in uptake by gender and deprivation. It has been widely reported that the uptake of FOBT or FIT screening is consistently higher in women than in men.22,23 In FS screening, however, this gender difference is consistently reversed,1–3,10 and the findings here are in keeping with other studies. A recent qualitative Canadian study suggests that women find bowel screening-associated stress to be a more important barrier than men, 24 and it can be argued that FS is a more stressful procedure than FOBT or FIT. However, a pooled analysis of RCTs demonstrates that FS is less effective in older women than in men, in terms of CRC mortality and incidence reductions. 25 By inference, the data generated in this study support this observation, given the lower uptake and the lower yield of neoplasia in women at age 60 compared with men.
There was a significant deprivation gradient associated with the uptake of FS, entirely consistent with previous studies. When this was compared with the gradient for uptake of FOBT screening in the control group, there was a statistically significant difference, suggesting that the effect of deprivation on the uptake of FOBT screening is greater than for FS screening. This is perhaps surprising, given the more burdensome nature of FS, but it indicates that FS screening does not appear to increase inequalities, at least at low levels of uptake.
The strengths of this study include the ability to deliver FS to a population already engaged in a FOBT screening programme, and the pragmatic study design, which mirrored what would have happened had FS been rolled out in the SBoSP. The weaknesses include the fact that the FOBT algorithm used in this study has been replaced by quantitative FIT, which could be used at a lower faecal haemoglobin concentration cut-off. Indeed, it has been shown recently that multiple rounds of FIT at a low cut-off detect significantly more advanced neoplasia, on a population level, compared with once only FS or colonoscopy screening, and that significantly fewer colonoscopies are required by individuals screened by multiple FIT. 26 In addition, in this study, the effect of adding FS on the yield of pathology was only examined within a single round of FOBT screening, and FOBT is employed as part of a biennial iterative process.
This study underlines the importance of piloting population-based screening programmes. Before national roll-out, FOBT screening was carefully piloted and learning informed the rolled-out programmes across the UK. 27 This did not occur to the same extent for FS screening, and both the uptake and the ability to provide FS fell short of that expected from the results of the RCTs when it was introduced in England. It is possible that FS uptake in the English screening programme is an underestimate of what might be achieved in a fully rolled-out national screening programme. Because FS has not yet been offered to the whole eligible population, there has been little promotional material to encourage uptake. With a fully rolled-out programme, enhanced communication with possible participants and good promotional materials may mean that uptake would significantly increase over time. Because of these uncertainties in both countries, the UK National Screening Committee has recommended a re-appraisal of the role of FS in the UK. 28
Supplemental Material
MSC879955 Supplemetal Material - Supplemental material for Randomized controlled trial: Flexible sigmoidoscopy as an adjunct to faecal occult blood testing in population screening
Supplemental material, MSC879955 Supplemetal Material for Randomized controlled trial: Flexible sigmoidoscopy as an adjunct to faecal occult blood testing in population screening by Robert JC Steele, Francis A Carey, Greig Stanners, Jaroslaw Lang, Jess Brand, Linda A Brownlee, Emilia M Crichton, Jack W Winter, Perminder S Phull, Craig Mowat, Judith A Strachan, Ann-Marie Digan and Callum G Fraser in Journal of Medical Screening
Footnotes
Authors’ note
Further information on the study and additional data may be available through discussion with the corresponding author, Professor RJC Steele.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NHS Tayside, through CGF, had a paid consultancy contract with Immunostics Inc., Ocean, NJ, USA, the suppliers of gFOBT and qualitative FIT. All other authors declare no conflicts of interest.
Ethical approval
The study was approved by the East of Scotland Ethics Service (REC Reference: 14/ES/0021, Protocol No. 2013ON22, IRAS project ID: 146024).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Scottish Government. The views expressed are those of the authors.
Supplemental material
Supplemental material for this article is available online.
Trial registration
The study was registered as a trial at ClincalTrials.gov (ID: NCT02560194).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.