
Abstract
Objectives
Quantitative faecal immunochemical tests (FIT) for faecal haemoglobin (f-Hb) in colorectal cancer (CRC) screening pose challenges when colonoscopy is limited. For low positivity rates, high f-Hb concentration cut-offs are required, but little is known about interval cancer (IC) proportions using FIT. We assessed IC proportions using an 80 µg Hb/g cut-off.
Methods
In two NHS Boards in the Scottish Bowel Screening Programme, f-Hb was estimated for 30,893 participants aged 50–75, of whom 753 participants with f-Hb ≥ 80 µg Hb/g were referred for colonoscopy. ICs, defined as CRC within two years of a negative result, were identified from the Scottish Cancer Registry.
Results
There were 31 ICs and 30 screen-detected (SD) CRCs, an IC proportion of 50.8% (48.4% for men, 53.3% for women). CRC site distribution was similar between ICs and SD, but ICs were later stage (46.7% and 33.3%, Dukes’ stages C and D, respectively). Of 31 ICs, 23 had f-Hb < 10 µg Hb/g, including six with undetectable f-Hb. A f-Hb cut-off of 10 µg Hb/g would have raised the positivity rate from 2.4% to 9.4%, increased colonoscopy requirement from 753 to 2147, and reduced the IC proportion to 38.3%.
Conclusions
The IC proportion was similar to that seen with guaiac-based FOBT. The later stage distribution of ICs highlights the benefits of lower f-Hb cut-offs, but with 19.4% of ICs having undetectable f-Hb, some cancers would have been missed, even with drastic reduction in the f-Hb cut-off.
Keywords
Introduction
Interval cancers (ICs), defined by the World Endoscopy Organization as “cancer diagnosed after a screening test or examination in which no cancer is detected and before the date of the next recommended examination”, 1 are a significant issue in colorectal cancer (CRC) screening programmes. Minimizing the number of undetected CRCs is crucial to the primary goal of these programmes, to reduce CRC mortality through early detection.
Although guaiac faecal occult blood test (gFOBT) screening reduces CRC mortality, 2 high proportions of all CRC diagnosed in screened populations are ICs (IC proportion). In England 3 and Denmark, 4 IC proportions of 51.3% and 55.2% have been found, and a large non-randomized trial in Burgundy reported an IC proportion of 59.3%. 5 Studies from Denmark, 6 Scotland, 7 and France 8 also show that ICs consistently account for more than half of CRC detected in populations screened biennially with gFOBT. Some characteristics are more associated with IC than gFOBT screen-detected (SD) CRC. Higher proportions of IC compared with SD CRC are found in women,7,9,10 and in the right colon.7,9–15 Rectal cancers are more common amongst IC than SD CRC,6–8 perhaps because rectal cancer tumour growth is faster, 16 or because the erythrocytes in blood originating in the rectum have not been haemolysed and do not yield positive gFOBT or faecal immunochemical tests (FIT) for haemoglobin. ICs have a worse prognosis than SD CRC, with larger, later stage tumours more frequently reported.6–8
In view of their many advantages, 17 FIT are now replacing gFOBT in CRC screening programmes. FIT are more sensitive than gFOBT, particularly for advanced adenoma detection, 18 and are likely to have the potential to reduce IC proportions. Quantitative FIT allow the selection of a faecal haemoglobin concentration (f-Hb) cut-off most appropriate for a programme, but this poses challenges when colonoscopy capacity is limited. To secure low positivity rates that match colonoscopy capacity, high f-Hb cut-offs are required, negating the improved sensitivity of FIT over gFOBT. In an evaluation of quantitative FIT in Scotland, at a cut-off f-Hb of 80 µg Hb/g faeces, the positive predictive values (PPV) for advanced neoplasia were no better than with gFOBT. 19
Data on IC proportions in population screening with FIT might provide insights into how quantitative FIT can be utilized when colonoscopy capacity is limited, to minimize IC proportions and address the sex inequalities that exist with gFOBT screening. To establish the IC proportions associated with the use of FIT at a cut-off equivalent to gFOBT and whether characteristics such as female sex and location in the proximal colon also show positive associations with IC, we assessed the consequences of FIT using a f-Hb cut-off of 80 µg Hb/g faeces (set to give around 2% positivity) in terms of IC within an established CRC screening programme.
Methods
FIT as a first-line test evaluation has been described previously. 19 From 1 July 2010 to 12 January 2011, all eligible participants in the Scottish Bowel Screening Programme aged 50–74 and resident in NHS Tayside and NHS Ayrshire & Arran were sent a FIT kit pack containing an invitation letter, a booklet on bowel cancer, a thin card wallet with written and pictorial instructions for sample collection which contained a single faecal specimen collection device (Eiken Chemical Co. Ltd., Tokyo, Japan), a small zip-lock plastic bag with integral absorbent material, and a foil mailing pouch for device return. Both NHS Boards had offered screening previously, using a gFOBT/qualitative FIT two-tier reflex screening algorithm, 20 but this was the first time that any participant had taken part in a quantitative FIT-based CRC screening programme. Those who returned an untestable FIT were sent another FIT kit pack.
The characteristics of all returned samples were documented. Samples were analysed for f-Hb using OC-Sensor Diana automated immunoturbidimetric analysers (Eiken) in the Scottish Bowel Screening Centre Laboratory, by trained staff whose major function is to perform faecal test analyses. The Laboratory had comprehensive quality management and was accredited to ISO15189 based standards by Clinical Pathology Accreditation (UK) Ltd.
Participants with negative test results (f-Hb < 80 µg Hb/g faeces) were informed by letter. Those with positive results (f-Hb ≥ 80 µg Hb/g faeces) were contacted by letter, their general practitioner was notified, and they were referred to their NHS Board for colonoscopy. The f-Hb cut-off was chosen to give around 2% positivity, to mimic the positivity rate of the existing Screening Programme and match the available colonoscopy resource. Data for colonoscopy outcomes and any subsequent pathology were downloaded from the NHS clinical IT systems and details on colonoscopy findings including number, size, Dukes’ stage, and localization of colorectal cancers and adenomas were collected. Right-sided location of neoplasia was defined as cancer detected in the region of the colon up to and including the splenic flexure, left-sided as the region thereafter up to the recto-sigmoid junction, and rectal neoplasia as lesions located both in the recto-sigmoid junction and the rectum.
Linkage with the Scottish Cancer Registry was performed to identify IC from the cohort of negative participants and to allow comparison of factors including f-Hb and gender distribution of CRC between the IC and SD CRC groups. IC data were available for diagnoses to 31 December 2012, so the analysis included only negative participants with a result date up to 31 December 2010. Participants with later result dates were excluded from the analysis. The linkage was completed using IBM SPSS version 21. CRCs arising after a negative colonoscopy were referred to as “missed” cancers, and not IC in our cohort.
Population weighted Scottish Index of Multiple Deprivation (SIMD) 2012 quintiles were used for analysis by deprivation. 21
We used MedCalc (MedCalc Software, Mariakerke, Belgium) statistical software for all calculations and Mann–Whitney U test for comparison of median f-Hb between groups. Probability of p < 0.05 was considered significant. Logistic regression analysis was performed to calculate odds ratios (OR) for IC amongst different demographic groups, adjusted for confounding variables.
Results
Characteristics of interval cancers and screen-detected colorectal cancer.
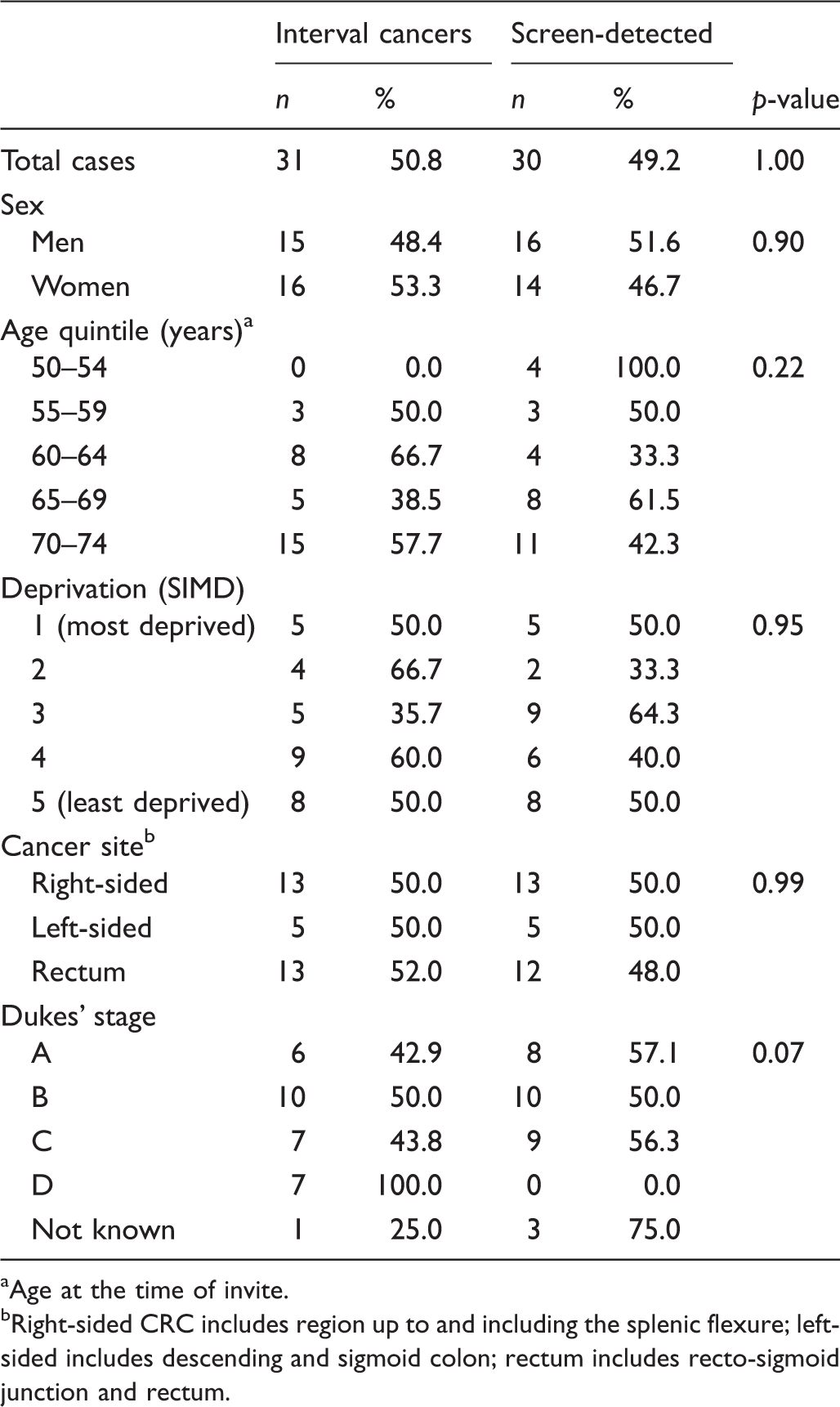
Age at the time of invite.
Right-sided CRC includes region up to and including the splenic flexure; left-sided includes descending and sigmoid colon; rectum includes recto-sigmoid junction and rectum.
IC proportions were 48.4% in men, and 50.3% in women. Median age in those with an IC was 68 (interquartile range [IQR]: 63–72) compared with 67 (IQR: 61–72) for SD CRC. ICs were diagnosed at a more advanced stage, 46.7% being late stage (Dukes’ stage C or D) compared with 33.3% of SD CRC.
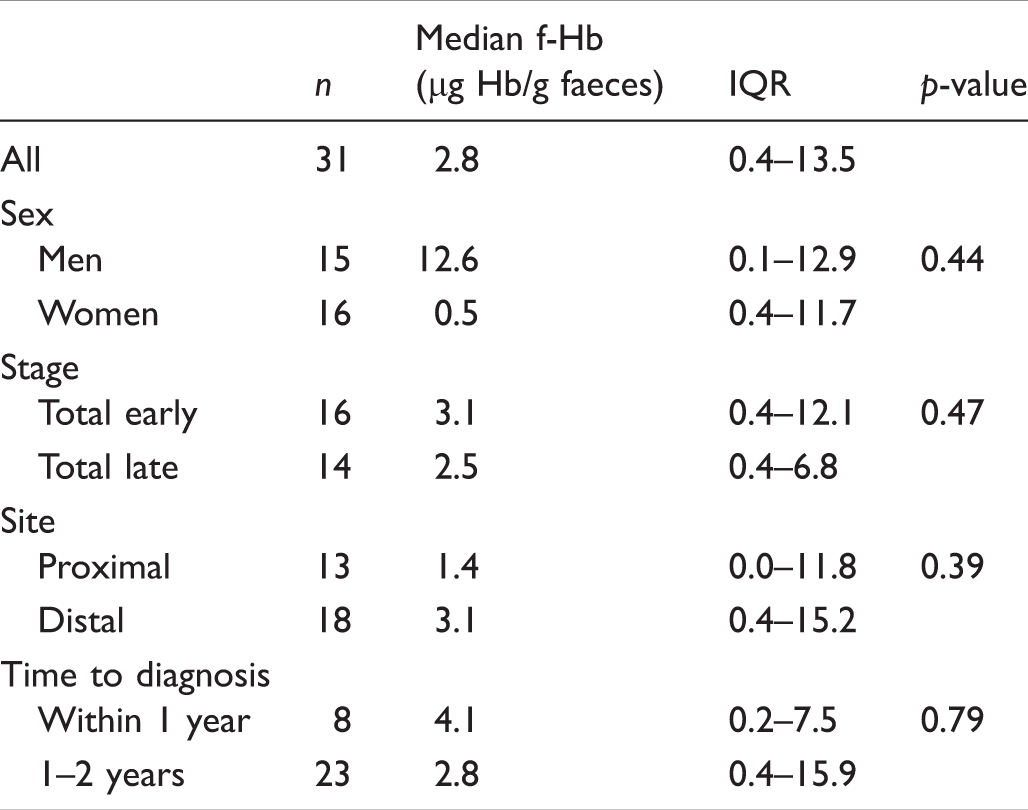
Median f-Hb and interquartile range at time of negative screening test in those who had interval cancer.
The effect on positivity rate and IC proportion of lowering the f-Hb cut-off to various concentrations was assessed. Between cut-off concentrations of 80 and 10 µg Hb/g faeces, positivity rate would have increased steadily from 2.4% to 9.4%, before escalating to 24.7% at 2 µg Hb/g faeces, and 49.5% using any detectable blood as a cut-off. Figure 1 shows the number of colonoscopies required for different f-Hb cut-offs, alongside the associated proportions of IC and SD CRC.
Effect of lowering the faecal haemoglobin (f-Hb) cut-off on proportions of interval cancer and screen-detected colorectal cancers (CRC) and number of colonoscopies required.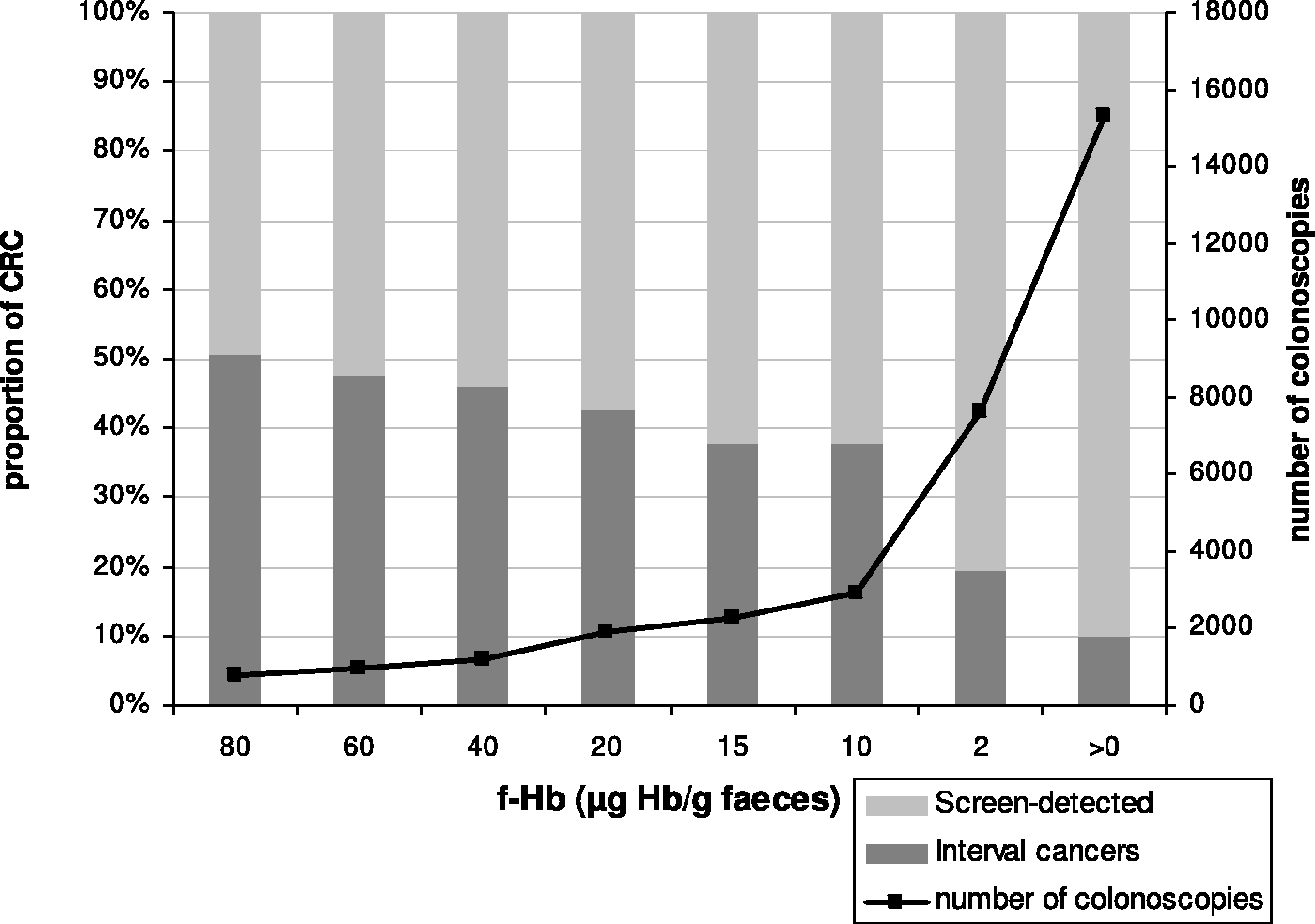
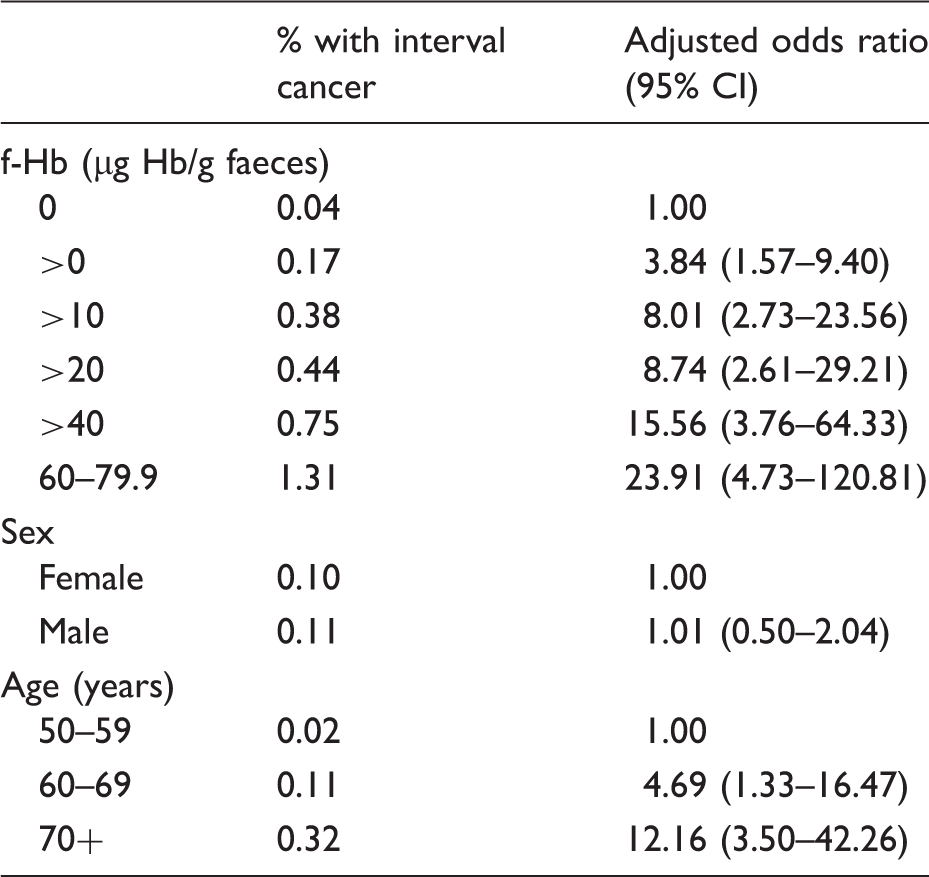
Proportion of interval cancers by faecal haemoglobin (f-Hb), gender and age with adjusted odds ratios.
Discussion
Our results provide unique insights into IC proportions, using FIT with a high f-Hb cut-off (80 µg Hb/g faeces) in an established screening programme with limited colonoscopy capacity, and how these proportions could be influenced by varying the f-Hb cut-off. Our IC proportion was no different from the circa 50% found using traditional gFOBT.
A major strength of this study is that a large cohort of over 30,000 completed FIT screening in the context of a fully rolled out operational screening programme, so the IC proportions we observed, using FIT at a high f-Hb cut-off concentration, are those that could be expected in nationwide screening. Our results show that FIT-based CRC screening programmes would benefit from using low f-Hb cut-offs to gain lower IC proportions as well as higher sensitivity and detection of earlier stage disease, but at the cost of increased colonoscopy demand. 22 This study also has limitations. The relatively small numbers of IC and SD CRC mean that statistical significance was not reached for differences between CRC categories for Dukes’ stage. In addition, because the distributions of f-Hb are country specific, 23 our findings may not be internationally transferable. Also, our calculation of the yield of SD CRC at different f-Hb cut-offs is likely to be an underestimation. The lower f-Hb cut-off may also have led to detection of CRC that would arise as SD CRC in the subsequent screening round, as well as a small proportion of over-diagnosed cancers, so the IC proportions would be lower than we have reported, although this is difficult to quantify.
Our IC proportion of 50.8% at a cut-off concentration of 80 µg Hb/g was much higher than the 14.4% found in Italy using a much lower f-Hb cut-off of 20 µg Hb/g faeces, 24 confirming that the use of a high f-Hb cut-off negates the improved sensitivity for significant neoplasia offered by FIT over gFOBT, and consequently increases the IC proportion. 19 Previous findings that women have a higher IC proportion than men when a high f-Hb cut-off is used are supported to some extent. In contrast to the results of previous studies, an association with location in the proximal colon for IC in women was lacking, with just a quarter of cases in women located from the caecum up to and including the splenic flexure, whereas most IC in men were right-sided. However, the relatively small numbers of IC and SD CRC detected in this study make this lack of association unreliable; the relationships between IC proportions and sex and age did not reach statistical significance, although the trends were as expected.
The more advanced stage distribution of IC highlights the need to improve CRC detection with screening. Lowering the f-Hb cut-off would increase colonoscopy demand, which may not be sustainable with available resources. In our cohort, halving the f-Hb cut-off to 40 µg Hb/g faeces would reduce the IC proportion from 50.8% to 45.9%, but with a significant 58.6% increase in the number of colonoscopies required. Small gains in sensitivity come at the cost of significant losses in specificity and PPV. This could be counteracted by screening at a low f-Hb cut-off, but with a longer interval than two years between screening rounds. This is an important area for future research. In addition, given the important effects of age and gender on IC proportions seen in previous studies and supported here, exploring stratified f-Hb cut-offs based on these variables is warranted.
Although participants with undetectable f-Hb accounted for over half of the screened population, the proportion of IC in this group was over 30 times lower than the proportion in those with f-Hb in the range of 60.0–79.9 µg Hb/g faeces, who constituted just 0.5% of the cohort. Adjusted OR demonstrated increasing risk of IC with increasing f-Hb, and perhaps suggests that participants with elevated f-Hb should be offered more regular screening. Men and women have different f-Hb, as do older compared with younger participants.22,25 Our results support the inclusion of numerical data for f-Hb in risk-scoring models for population CRC screening, as recently advocated. 26 As IC has a worse prognosis, women and older participants may be disadvantaged by the use of a single f-Hb cut-off for all, and better individualized use of FIT in CRC screening is required. Further work is required to determine specific performance characteristics of FIT in subgroups at different f-Hb cut-off concentrations. IC proportion alone is not sufficient to address inequalities. As CRC incidence rates are lower among women than men, the residual risk of IC diagnosis following a negative screening result will also be lower in women than in men. The selection of the appropriate f-Hb cut-off concentration is complex, and other factors such as PPV are important considerations in a setting limited by endoscopic resources.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CGF undertook consultancy with Immunostics Inc., Ocean, NJ, USA, Mode Diagnostics, Glasgow, Scotland, and Kyowa-Medex, Tokyo, Japan. All other authors had no conflicting interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Scottish Government Health Directorates.
Research Ethics
Approval from the NHS National Services Scotland. Privacy Advisory Committee was also secured for the data linkage required in this analysis.