
Abstract
Objective
To examine the effect of a mass media campaign designed to increase bowel cancer screening participation.
Methods
We assessed weekly participation, from January 2015 to December 2017, in the Australian National Bowel Cancer Screening Program in Victoria, where a seven-week campaign aired in mid-2017, and in the adjacent comparison state of South Australia. Participation, defined as the number of immunochemical faecal occult blood tests returned out of those invited by the Screening Program in the past 16 weeks, was analysed using negative binomial regression.
Results
Compared with non-campaign weeks, there was an increase in the return rate in the campaign state during campaign weeks (adjusted return rates non-campaign weeks = 34.4% vs. campaign weeks = 45.3%, p < 0.01), not observed in the comparison state (38.3% vs. 40.3%, p > 0.05). The increase in the return rate was significantly greater in the campaign state (Rate Ratio of Campaign/Non-Campaign weeks = 1.31, p < 0.01) than the comparison state (1.05, p > 0.05, interaction p < 0.001), and did not differ significantly by age, sex or socio-economic area. The relative increase was greater among never-participants (Rate Ratio of Campaign/Non-Campaign weeks = 1.24) than previous-participants (1.16), interaction p < 0.001).
Conclusions
This mass media campaign increased bowel cancer screening participation, including from never and low participation subgroups. To maximize participation and ensure equitable population benefit, repeated campaigns that reach eligible people about bowel cancer risks and potential life-saving benefits of screening should be standard.
Introduction
Bowel cancer is the third most commonly diagnosed cancer and the second biggest cause of cancer deaths in Australia. In 2019, it is estimated to affect 16,398 people and cause 5597 deaths annually. 1 If detected early, over 90% of bowel cancer cases can be successfully treated. 2 In 2006, the Australian Government commenced the National Bowel Cancer Screening Program, with immunochemical faecal occult blood tests (FIT) kits sent directly to people aged 50–74 years, as recommended by the Australian National Health and Medical Research Council. 3 Less than half (41%) of those who were sent a kit in 2015–2016 participated. 4 To increase participation, a non-government organization (Cancer Council Victoria) conducted a television-led mass media campaign in mid-2017 in the state of Victoria. Figure 1 shows key images and messages (see also https://youtu.be/9DEffgTZwyY for the 30-s message). To evaluate the effectiveness of the campaign, we examined Screening Program kit completion and return rates before, during and after the campaign, compared with those in a state where the campaign did not air.
Images from the campaign advertisements shown on television and on digital and outdoor advertising featuring several bereaved relatives reflecting on loved ones lost to bowel cancer, emphasizing the importance of early detection to save lives.
Cancers in the large bowel tend to produce low-grade bleeding,5,6 which the FIT uses globin antibodies to detect. Unlike the guaiac test (which detects chemical activity in haem), FIT does not rely on the user avoiding red meat and vitamin C supplements for several days before use.7,8 With the Screening Program collecting two FIT samples, the positive predictive value and negative predictive value for bowel cancer were 3.6% and 99.9%, respectively, showing high sensitivity (85%) and specificity (92%) for cancer detection, 9 supporting other work that indicates high validity of this method.10–12 Among participants who had a follow-up colonoscopy after a positive screening result in 2016, 3.8% had bowel cancer, 6% had an advanced adenoma and 6% a non-advanced adenoma. 9 Participants with bowel cancer detected through the Screening Program have been found to be more likely to be diagnosed at a less advanced stage than non-participants (44% vs. 24%), and had lower estimated risk of bowel cancer mortality (per 100,000) over a year, than those diagnosed outside the Screening Program (9.6% vs. 23.8%). 13
The Screening Program has had a gradual introduction, with full implementation using biennial invitations to be complete by the end of 2019. A biennial participation rate of 40% would prevent 92,200 cancer cases and 59,000 deaths between 2015 and 2040, and if the participation rate could be boosted to 60%, an additional 37,300 cancer cases and 24,800 bowel cancer deaths could be prevented. 14
Among eligible people, those who are younger, male or living in lower socioeconomic (SES) areas were less likely to participate. 4 A trial in New South Wales, Australia, found that people with the lowest education levels had greater difficulties making a choice about participation, and concluded that further information and support would facilitate their participation. 15 In the French colorectal screening program, participation rates were lowest among unskilled workers and people with lower health care access (i.e. fewer visits to medical practitioners).16,17 A 2014 Australian survey of people aged 50 and over found that believing ‘screening was only necessary for those experiencing symptoms’ was associated with lower rates of participation. This belief was higher among non-English speaking migrants and those aged 65 and over, suggesting that bowel cancer screening beliefs should be targeted to correct these misperceptions. 18 Studies of barriers to screening by SES and education have indicated that worry about cancer and lower health literacy may be greater in these groups.19,20 Other known screening barriers include perceiving at-home tests as less important than screening in formal health settings and cultural taboos related to sampling faeces and storing faecal samples. 21
In Australia, the rate of participation in subsequent rounds of invited biennial screening after first-round participation is 77%. 4 This is consistent with colorectal screening programs elsewhere, 22 suggesting that reducing barriers to initial participation is a key target for interventions to maximize future participation. Mass media campaigns are likely to be particularly effective for correcting misperceptions, encouraging initial participation and conveying the urgency of completing the test, 23 as they have the advantage of communicating with a broad cross-section of the population. Well-funded paid public health campaigns can reach different SES groups at least equally, 24 while health communication formats with lower reach, or that are limited to certain opt-in media (such as social media, brochures or digital video), may increase disparities.25,26
Previous bowel cancer campaigns that have focused on increasing awareness about early symptoms have effectively increased awareness and showed some increases in referrals,27,28 but this has not translated into changes in the tumour stage at presentation, nor into increased short-term patient survival, partly due to the proportion of individuals who first present with well-advanced disease. In contrast to campaigns about early symptoms, media campaigns encouraging cancer screening have the potential to greatly increase early detection and survival at a population level. 4 The few studies that have examined the effectiveness of mass media bowel cancer screening campaigns provide evidence that they can increase participation.29,30 Effects tend to be small but, similar to mass media campaigns for other health behaviours,23,24 they increase with message repetition. 31 With the broad reach of mass media campaigns, small repeated effects can have a substantial impact on population behaviour change.32,33
In this study, we evaluated whether Screening Program kit completion and return rates in Victoria increased from before to during and after a mass media campaign designed to increase participation, compared with the state of South Australia, where campaign activity was limited. We also examined whether campaign-associated increases in participation were observed similarly across subgroups known to have lower screening rates.
Methods
The Screening Program was introduced incrementally, with full implementation (a two-yearly invitation program for those aged 50–74 years) to be complete by the end of 2019. Two samples are collected and returned. FIT is a non-invasive test that can detect microscopic amounts of blood in a bowel motion, which might indicate a bowel abnormality, such as a polyp, an adenoma or cancer. Participants complete the received kit and return it in a post-paid envelope for analysis by the Screening Program pathology service within 14 d of completion. Results are sent to the participant, their nominated primary health-care practitioner and to the Screening Program Register. Those with a positive test result are advised to consult their primary health care practitioner to discuss further diagnostic assessment (colonoscopy in most cases). 34
We compared kit return rates from the campaign state (Victoria) with those from South Australia, where the campaign was not run, as South Australia was the largest Australian state that did not have concurrent bowel screening campaign activity planned. Anonymized weekly Victorian and South Australian FIT ‘kit return’ data were obtained from the Screening Program, and we calculated return rates from the invited populations in each state. The ‘kit return’ datasets included the number of Screening Program invitations sent, and kits returned and analysed per week. Separate datasets were provided for breakdowns of age group by gender, SES area and prior screening status, to enable comparison of kit return rates from specific sub-groups. Kit return data were from weeks before (January 2015 to June 2017), during (30th July to 16th September 2017) and after the end of the campaign (September to December 2017). Baseline data (January 2015 to June 2017) provided the comparison point from which to judge campaign-related increases and enabled seasonal kit return patterns to be controlled. Ethics approval was obtained from the Cancer Council Victoria’s Institutional Research Review Committee (QA1702).
The mass media campaign consisted of seven weeks of paid 30-s advertisements shown on television, digital video and in health centre waiting rooms; advertorial segments aired within light entertainment television programs; radio advertisements; social media posts; and online native website advertising. The campaign achieved 792 Target Audience Television Rating Points (TARPs) in metropolitan areas and 802 TARPs in regional Victorian areas. TARPs are a standard advertising industry measure of campaign reach and frequency in a target audience. For example, 1000 TARPs per quarter equates to, on average, 100% of those within a region exposed to 10 advertisements, or 50% exposed to 20 advertisements and so on. The leading campaign advertisements featured several bereaved relatives reflecting on loved ones lost to bowel cancer, emphasizing the importance of early detection to save lives (see Figure 1; https://youtu.be/9DEffgTZwyY). Key messages included that ‘Bowel cancer kills 80 Australians each week; If found early, 90% of bowel cancers can be successfully treated; Are you 50 or over? Do the free test when it’s sent to your home’. Five ‘advertorials’ were aired only in the campaign state; however, 13 advertorials were aired nationally (including in the comparison state where broadcasts were provided as unpaid bonus or as standard from the television networks). Television advertisements were also shown half-hourly in 395 general medical practices in the campaign state.
In the campaign state, televised elements were supported by 734 radio advertisements on four metropolitan Victorian radio stations with a mix of 30-s recorded and live reads. One radio station provided a 15-min segment, including an interview and talkback. Geo-targeted digital advertising was also used, with over 500,000 digital video views, almost 21,000 website visits from content marketing posts and around 14,000 from Facebook posts. Participating general medical practices also displayed campaign brochures and posters.
In a controlled cohort telephone survey of 1700 Screening Program eligible individuals aged 50–74 years, 80% of participants in the campaign state and 24% in the comparison state were aware of at least one aspect of the campaign. 35 In the campaign state, 53% recalled the campaign from television, 46% from medical practices, 24% from radio, 7% from advertorials, 6% from social media, 5% from websites, 3% via an online video and 22% had heard about it from someone else. Of those exposed, 40% discussed the message with someone else (e.g. friends, family or colleagues). Of those who recalled the main campaign message, a large majority found it believable (97%) and relevant (87%), with 87% reporting that the message made them feel they had more control over their future health, and 69% that it made them think about how their family and friends would feel if they got bowel cancer.
In the kit return datasets, cells with fewer than six counts per week were suppressed, to ensure participant anonymity (The Australian Institute of Health and Welfare cleans and supplies data on behalf of the Screening Program). For cells with missing data, we imputed weekly invitation counts (We used the random number generator from Excel (=INT(RAND()*5)) to return any random integer between zero and five). Imputation created a small difference between overall and sub-group datasets in the number of total invitations. In the 157 weeks of 2015–2017, 14–15 weeks had suppressed data (8.9–9.6% of weeks) depending on the sub-group dataset. Low-count weeks tended to cluster around mid-late December and early January, coinciding with seasonal holidays and high temperatures (kits can be adversely affected by high temperatures). Preliminary seasonality analyses revealed fewer invitations issued each December, and correspondingly lower kit returns each January, compared with other months. As previous research has shown behaviour change campaigns can persist for up to three months after broadcast,30,36,37 we examined the effects of the mass media campaign during the weeks on air and in each two-week period after broadcast up to 15 weeks post-broadcast.
Similar to the results of prior research examining the effects of mass media campaigns on cervical cancer screening rates, 38 the kit return data was over-dispersed (mean = 2392; variance = 2,182,641), and so negative binomial regression was used. The primary outcome variable was the kit return rate, measured as weekly kit returns out of people invited in the current and past 15 weeks (invitation count included as the offset term). The main predictor variables were the effective campaign period (during and outside) and state (campaign and comparison).
To establish the effective campaign period, we examined the wear-in and wear-out of the campaign using a preliminary set of negative binomial regressions, which examined kit return rates during the campaign and post-campaign weeks in both states compared with the rates in the two-and-a-half years prior to the campaign broadcast. We then tested for the overall impact of the campaign on kit return rates by comparing rates during and outside of the effective campaign period and evaluating the differences in this effect by state (i.e. the effective campaign period × state interaction term). To explore campaign impact on population sub-groups, we examined the three-way interactions between the effective campaign period × state × each age (50-59 vs. 60-74 years), gender, SES 39 (Socio-Economic Index For Areas -Disadvantage: Lower SES areas from quintiles 1-2 vs Higher SES areas from quintiles 3-5) and prior screen sub-group split separately. Models were adjusted for seasonality (using calendar month), year (as new eligible age-groups were added incrementally to the Screening Program each year) and other nationally broadcast promotions of the Screening Program (i.e. national Screening Program promotions 12–26 April 2015, and the national Jodi Lee campaign aired 26 April to 10 May 2015 (https://www.youtube.com/watch?v=UdBeacvJQkY&list=UUJFjxzHR9qf7Hzvfj-HP3qw) in both campaign and comparison states.
Results
Compared with the average weekly FIT return rate in the two-and-a half year pre-campaign period, FIT kit return rates in the campaign state increased in the first two weeks of the campaign, rose further after four weeks on air and peaked during the final three weeks on air, maintaining elevated return rates post-campaign in the first two weeks and up to four weeks after broadcast ended. Figure 2 provides the change in FIT kit return rates compared with the baseline return rates in Rate Ratios, adjusted for seasonality and covariates, with 95% confidence intervals. The return rate in the campaign state reverted to pre-campaign levels from five weeks after the broadcast ended. No such increases were observed in the comparison state (for Rate Ratios and 95% CIs, see Figure 2).
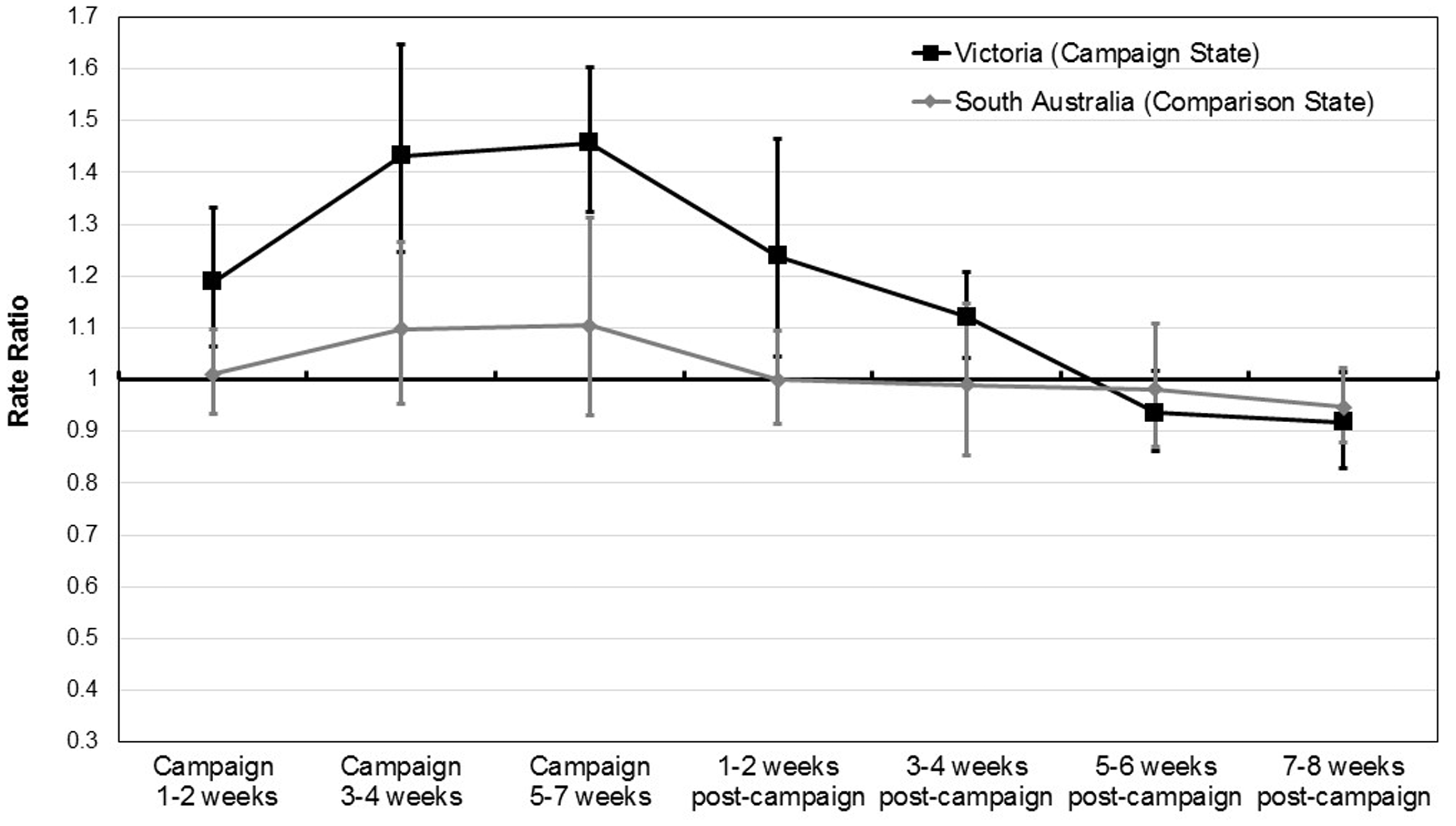
Changes in FIT kit return rates compared with the return rates in the two-and-a-half year baseline period (Rate Ratios, adjusted for covariates), during campaign and early post-campaign weeks in Victoria (campaign state) and South Australia (comparison state).
Overall, comparing the effective campaign weeks (first campaign weeks through to four weeks post-campaign) with the non-campaign weeks outside of this period, we found a significant increase in the rate of kits returned for analysis in the campaign state (Rate Ratio of Campaign/Non-Campaign weeks =1.31, p < 0.01), with no significant increase in the comparison campaign state (Rate Ratio of Campaign/Non-Campaign weeks =1.05, p > 0.05, campaign × state interaction F = 17.54, p < 0.001, see Table 1 for unadjusted and adjusted return rates and differences in states’ Rate Ratios). There were no significant differences in the impact of the campaign between age groups (Campaign × State × Age interaction F = 0.55, p = 0.457), sex (Campaign × State × Sex interaction F = 0.14, p = 0.711) or SES areas (Campaign × State × SES interaction F = 0.23, p = 0.632, see online Supplemental tables); however, there was a significantly greater increase in the kit return rate from never-screeners (Rate Ratio of Campaign/Non-Campaign weeks =1.24, p < 0.001) than from those who had previously completed a Screening Program kit (Ratio of Campaign/Non-Campaign weeks adjusted return rates = 1.16, p < 0.001, interaction F = 11.28, p < 0.001, see Table 2 for unadjusted and adjusted return rates and differences in states’ Rate Ratios).
Weekly FIT kit return rates, and Rate Ratios associated with the Bowel Cancer Screening campaign, in the comparison and campaign states.
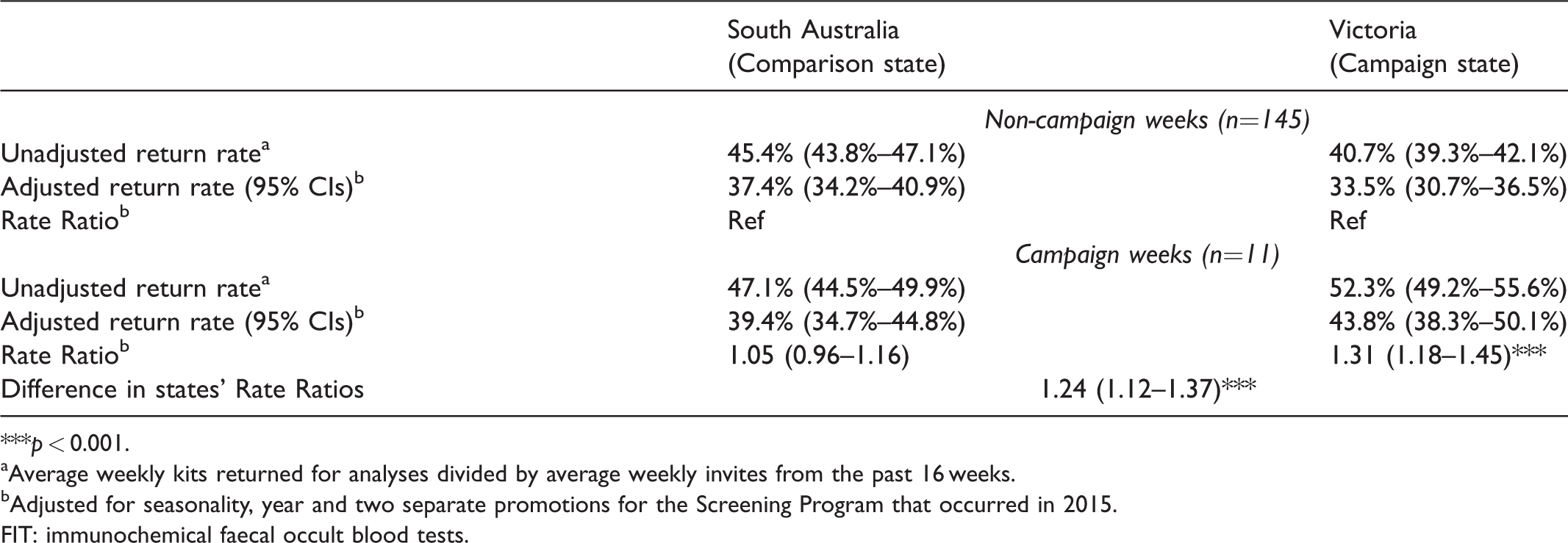
***p < 0.001.
aAverage weekly kits returned for analyses divided by average weekly invites from the past 16 weeks.
bAdjusted for seasonality, year and two separate promotions for the Screening Program that occurred in 2015.
FIT: immunochemical faecal occult blood tests.
Unadjusted and adjusted estimates of weekly FIT kit return rates, and Rate Ratios associated with the Bowel Cancer Screening campaign separately for those who had never participated versus those who had previously participated, in the comparison and campaign states from January 2015 to December 2017.
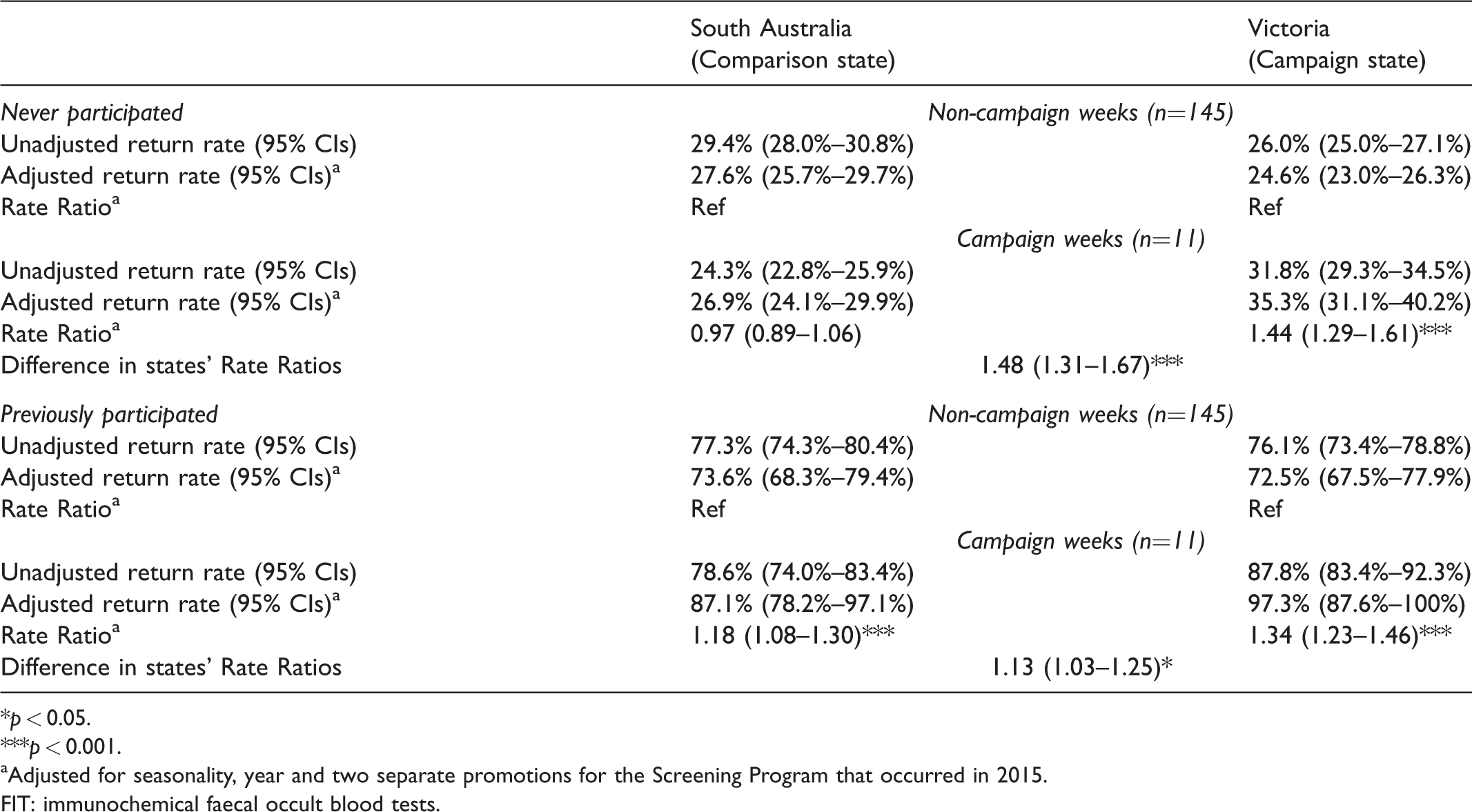
*p < 0.05.
***p < 0.001.
aAdjusted for seasonality, year and two separate promotions for the Screening Program that occurred in 2015.
FIT: immunochemical faecal occult blood tests.
Discussion
The seven-week multi-media campaign increased the numbers of recently invited age-eligible individuals who underwent screening from the start of the campaign until four weeks after broadcast, compared with non-campaign weeks. Increased kit return rates were observed only in the state where the campaign was broadcast. In the state where no campaign aired (but where a limited number of nationally syndicated daytime television advertorials were broadcast), there was no significant increases in kit return rates during or soon after the campaign. The effects of the campaign were proportionally greater among never screeners (i.e. first-time invitees and previous non-participants) than those who had previously participated. This result is particularly promising, as first-time invitees have the greatest early detection benefit of all eligible invitees, 4 and the campaign motivated kit returns among those who had not participated in previous biennial rounds. Given that kit return rates among previous participants is around 77%, 4 this campaign may provide an extra boost to the screening rates over the long-term life of the Screening Program, if those activated by this campaign also screen at higher rates in future invitation rounds.
We found no differences in the relative increase in screening rates between SES groups, consistent with previous analyses of campaign effects for cervical cancer screening campaigns, 38 and other research showing that well-funded campaigns can achieve broad population reach across socioeconomic areas. 24 Equivalent effects are less likely to result from smaller campaigns that rely on donated media or channels that offer only opt-in exposure, such as brochures and some social and digital media.26,40 We also found no sex or age group differences, with increased kit return rates observed as strongly among groups with lower participation as among those with higher participation.
Our findings are consistent with previous research indicating that bowel cancer campaigns can increase bowel cancer screening participation.29,30 These results illustrate the potentially substantial impact of a well-funded campaigns broadcast using high reach media, such as paid television and radio advertising, along with supportive narrow-casting in GP practices and on digital and social media. Importantly, campaign effects diminished after 5–6 weeks, similar to other public health behaviour change campaigns. 23 Therefore, regular investment in repeated bowel cancer screening campaigns is probably needed to motivate invitees throughout the year and to promote equitable participation.
A limitation of this study is that we could not examine campaign effects on kit return rates among culturally and linguistically diverse subgroups due to the unavailability of data on the number of weekly invitations issued to each population subgroup. 4 Other methods of estimating subgroup participation (e.g. by geographic regions known to contain many people from these subgroups) should be investigated in future research. It is also possible that Victorians may have been more receptive to the campaign messages, given the lower baseline screening rates in Victoria compared with South Australia. Future research across a range of jurisdictions with higher and lower screening rates is required to examine the influence of baseline rates on screening propensity. Another limitation was that we only examined campaign effects among those invited by the Screening Program in the past 16 weeks. As a minority of invitees keep the uncompleted kit for longer than this before participating, and some eligible people access kits or other screening (e.g. colonoscopy) outside of the program, we may have underestimated campaign impact. 35
A strength of this study was the use of an objective behavioural outcome rare in public health campaign evaluations, 23 and models were adjusted for seasonality, year and the potential influence of other promotions and campaigns. We also tested for the duration of campaign effects, providing greater confidence that the observed findings are due to the campaign rather than other factors.
Conclusion
This study suggests that broad population-level media campaigns can increase participation rates in organized bowel cancer screening programs. Mass-reach campaigns could potentially contribute to saving many lives, not only by detecting bowel cancer early, but also by identifying other pre-cancerous conditions (e.g. adenomas) that might lead to bowel cancer over time. If bowel cancer screening programs are to maximize participation and ensure equitable population benefit, repeated mass media campaigns that reach and inform eligible people about both bowel cancer risks and the potential life-saving benefits of timely screening should be standard.
Footnotes
Acknowledgements
We thank the Australian National Bowel Cancer Screening Program and the Australian Institute of Health and Welfare for providing access to cleaned FIT data and the Screening Program for reviewing the results of these analyses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Cancer Council Victoria. Melanie Wakefield is supported by an Australian National Health and Medical Research Council Principal Research Fellowship (#1109720).
Supplemental material
Supplemental material is available for this article online.