
Abstract
Objective
To investigate trends in quality of screening colonoscopy (using the Global Rating Score) in the 13 years since introduction of the Bowel Cancer Screening Programme in England.
Setting
An English Bowel Cancer Screening Programme colonoscopy service from 2007 to 2019.
Methods
A retrospective observational study was undertaken using a prospectively collected database in order to analyse trends in screening endoscopies (including patients following positive faecal occult blood test or with high-risk findings on flexible sigmoidoscopy). The Global Rating Score quality indicators for Bowel Cancer Screening Programme colonoscopy were used as outcome measures, and trends over time were analysed. These included caecal intubation rate, adenoma detection rate, colorectal cancer detection rate, proportion of patients with minimal or mild discomfort scores, proportion of patients who required intravenous sedation, and adverse events.
Results
There were 5352 colonoscopies included, performed by 3 endoscopists; 73.8% were index procedures (i.e. first Bowel Cancer Screening Programme colonoscopy) and the remainder were follow-up or surveillance colonoscopies. The mean age of patients was 66 (standard deviation 5) years, and 59.8% were male. Mean age increased over time (R2=0.033; p < 0.001). There were significant trends over time towards higher caecal intubation rate (p = 0.015), higher adenoma detection rate (p < 0.001), lower proportion requiring intravenous sedation (p < 0.001). There were no significant trends in comfort scores (p = 0.606), adverse events (p = 0.503) or colorectal cancer detection (p = 0.089).
Conclusion
There was a consistent improvement in the Global Rating Score for Bowel Cancer Screening Programme colonoscopies since the start of the programme, even when quality was already high at the start. Patients can expect high-quality colonoscopy when participating in the Bowel Cancer Screening Programme.
Introduction
The Bowel Cancer Screening Programme (BCSP) was initiated in the UK’s National Health Service (NHS) in 2006 in order to screen for colorectal cancer (CRC) in asymptomatic patients using faecal occult blood tests (FOBt). As part of this programme, patients with positive FOBt were invited to have a colonoscopy so that CRC and premalignant polyps could be detected earlier than they might have been before the existence of the screening programme. 1 The aim of such a programme is to reduce CRC incidence by removing premalignant polyps before they become malignant, and to reduce overall mortality from CRC by earlier detection. Screening was initially undertaken using guaiac-based FOBt, but more recently a faecal immunochemical test (FIT) has been reported as having higher diagnostic accuracy. 2 FIT replaced FOBt in the English BCSP in 2019.
High quality of screening colonoscopy is important in order to ensure complete examination, and to avoid ‘missed’ cancers, whilst at the same time minimising discomfort for patients. 3 In the UK, the Joint Advisory Group (JAG) is a multi-disciplinary body that determines the standards for training and appraisal of colonoscopy. One of the quality indicators is the self-reported Global Rating Score (GRS). This is used to measure particular markers of colonoscopy quality such as caecal intubation rate (CIR; the percentage of colonoscopies that successfully reach the caecum), adenoma detection rate (ADR; the proportion of patients who have ≥1 adenoma detected during colonoscopy) and use of intravenous (IV) sedation. Screening colonoscopy has been of high quality according to these criteria (with high CIR and ADR in a study of 36,460 screening colonoscopies 4 ). There is some evidence that volume and accreditation are associated with higher quality colonoscopy. 5
It is likely that quality of colonoscopy for an individual screener will improve over time as their experience increases, but this hypothesis has not been widely tested. There is some evidence of improvement over time for screening flexible sigmoidoscopies in the UK Flexible Sigmoidoscopy Screening Trial, 6 which would support such a hypothesis. We aimed to evaluate a group of screeners at our centre in England where the GRS bar is already set high, by investigating the trends in GRS over time since the introduction of the BCSP in the organisation.
Methods
Study design
An observational cohort study was undertaken to investigate trends in self-reported quality indicators (GRS) for BCSP colonoscopy over the 13-year period since its instigation at a single English NHS screening centre (2007–2019). All colonoscopies were performed as part of the BCSP after either positive FOBt or high-risk findings at flexible sigmoidoscopy. The Open Exeter database (as part of the National Health Application and Infrastructure Services) was recorded prospectively, and the current study is a retrospective analysis of the data derived in that manner. This was registered as a local quality assurance exercise (ID 4946). The study period precedes introduction of FIT testing in the BCSP in 2019, so that all patients within the study cohort are included within the same referral criteria period.
Data collection
Prospective data for colonoscopies were entered onto anonymised electronic records by the Specialist Screening Practitioners according to pre-determined domains, and held on an encrypted, password-protected database. This database was interrogated retrospectively in order to derive the demographic data and the quality indicators (GRS) for each year for each individual screening endoscopist.
Quality indicators
The quality indicators (GRS) collated were CIR, ADR, proportion of patients with minimal or mild discomfort scores, proportion of patients who required IV sedation, CRC detection rate and adverse events (including colonic perforation and post-procedural gastrointestinal bleeding).
Screening endoscopists
There were three endoscopists who have been performing screening colonoscopy as part of the English BCSP since 2007 until present day, which allows analysis over the entire period. These included two Consultant colorectal surgeons and one Consultant gastroenterologist. All of the colonoscopists also have non-screening colonoscopy practices. They were all accredited by the Joint Advisory Group (JAG) on Gastrointestinal Endoscopy for the entire study period, 7 which justifies an assumption that they started their screening practice at a high baseline level of quality.
Data analysis
Categorical data are presented as n and %, and continuous data are presented as mean and standard deviation (SD) for normally distributed data, and median and interquartile range for non-normally distributed data. Statistical analysis was performed using GraphPad Prism V8.4.3 (GraphPad Software, LLC). Trends in these variables over time were analysed using Cochran-Armitage tests for categorical data, Spearman’s rank correlation coefficient for non-normal continuous data and linear regression for normal continuous data. Comparison of continuous variables between the three screeners was undertaken using Kruskal-Wallis for non-normally distributed data. A p-value <0.05 was considered significant. No power calculation was undertaken, since the data were taken for the entire 13-year study period to demonstrate the trends over this specific period.
Results
Patient characteristics
There were 5352 colonoscopies included, performed by 3 endoscopists (endoscopist A: n = 1633; endoscopist B: n = 1593 and endoscopist C: n = 2126); 3949/5352 (73.8%) of these were index procedures (i.e. the first colonoscopy that the patient had within the BCSP), and the remainder were follow-up or surveillance colonoscopies as part of the BCSP. The mean age of patients was 66 (SD 5) years, and 59.8% were male. In the first year (2007), the mean age was 66 (SD 3) and in the last year (2019) the mean age was 68 (SD 5). There was a linear increase in age over time for the study period (R2=0.033; p < 0.001) but there was no significant trend in gender over time (Figure 1).
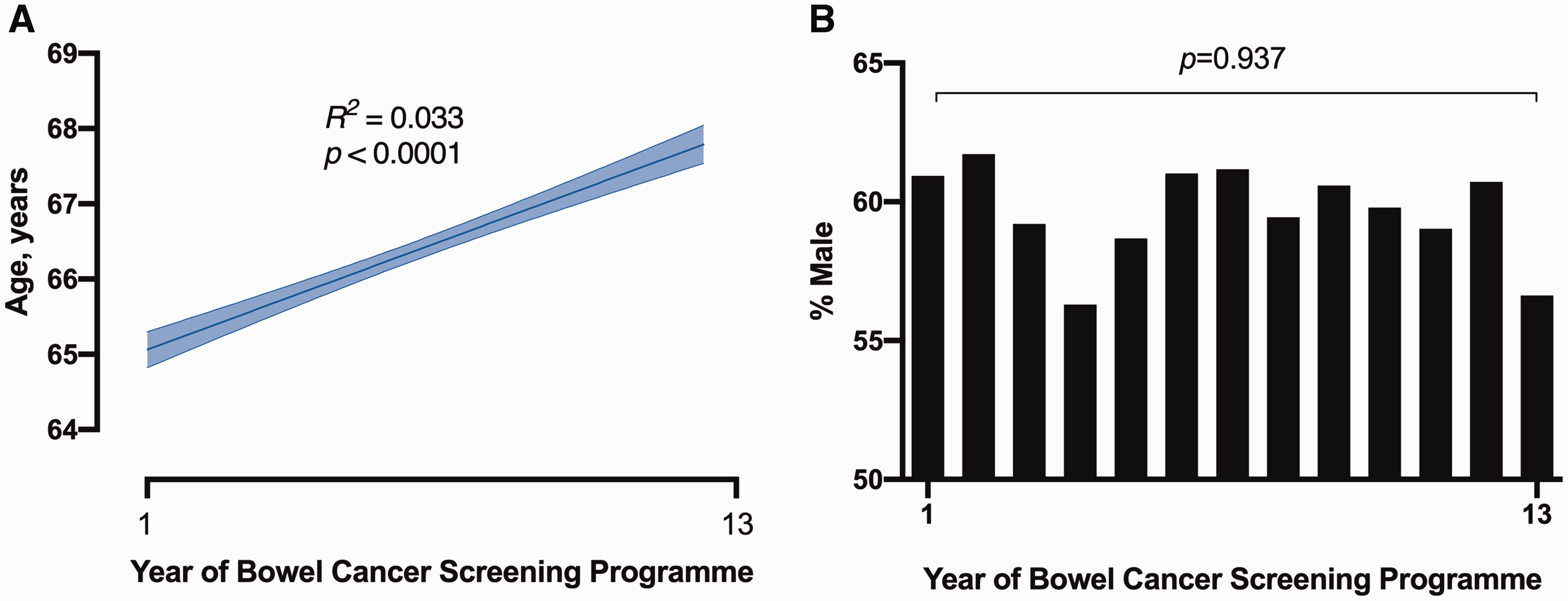
Trends in (a) age and (b) gender over time in the study period.
Volume of practice
The number of colonoscopies performed each year in the study period is summarised in Table 1 and Figure 2. There was an increase in colonoscopies performed over time at the screening centre (p < 0.001). There was no difference in average volume between colonoscopists over the study period (p = 0.293) (Table 1).
Number of screening colonoscopies performed in the study period.
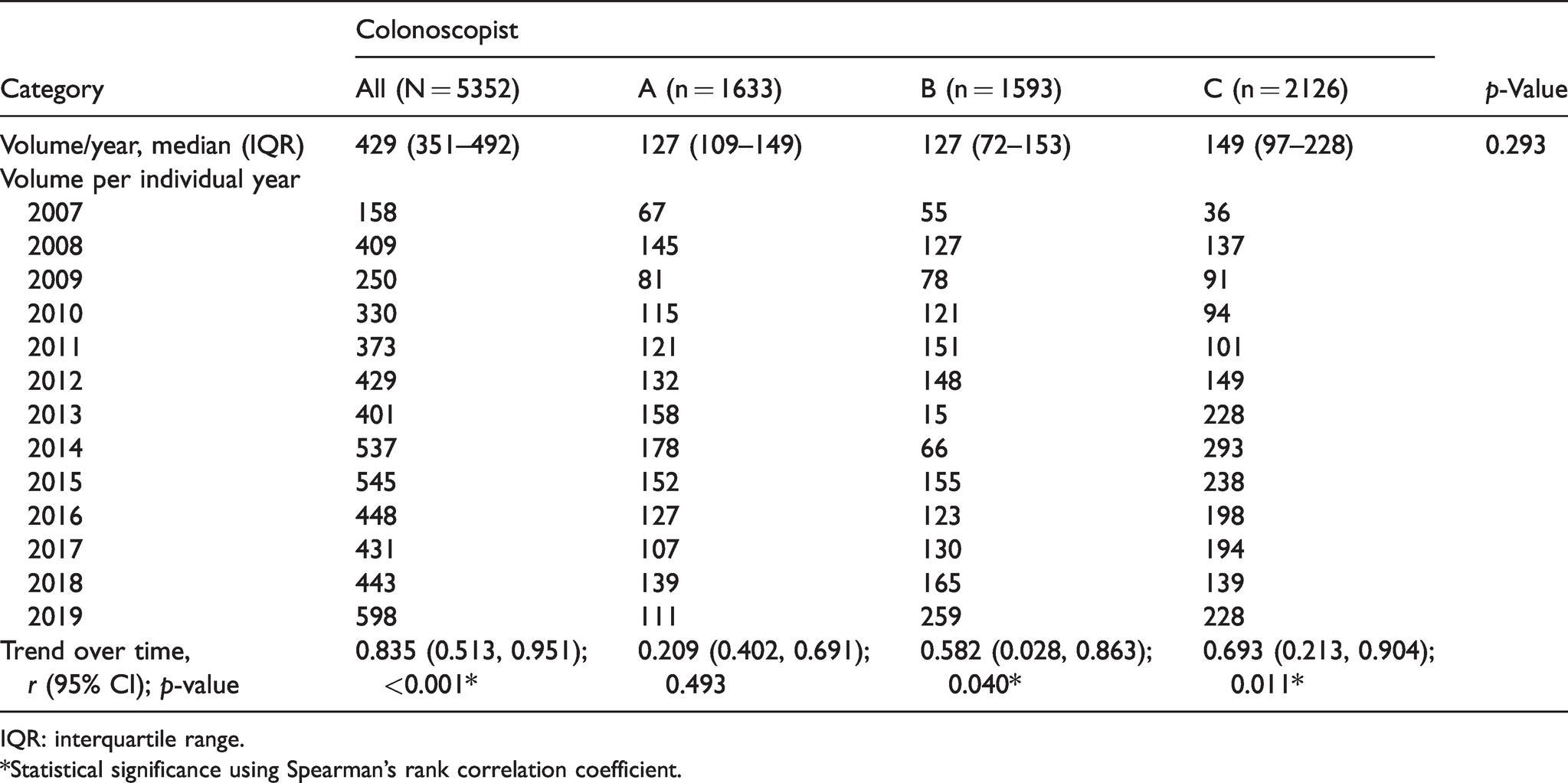
IQR: interquartile range.
*Statistical significance using Spearman’s rank correlation coefficient.
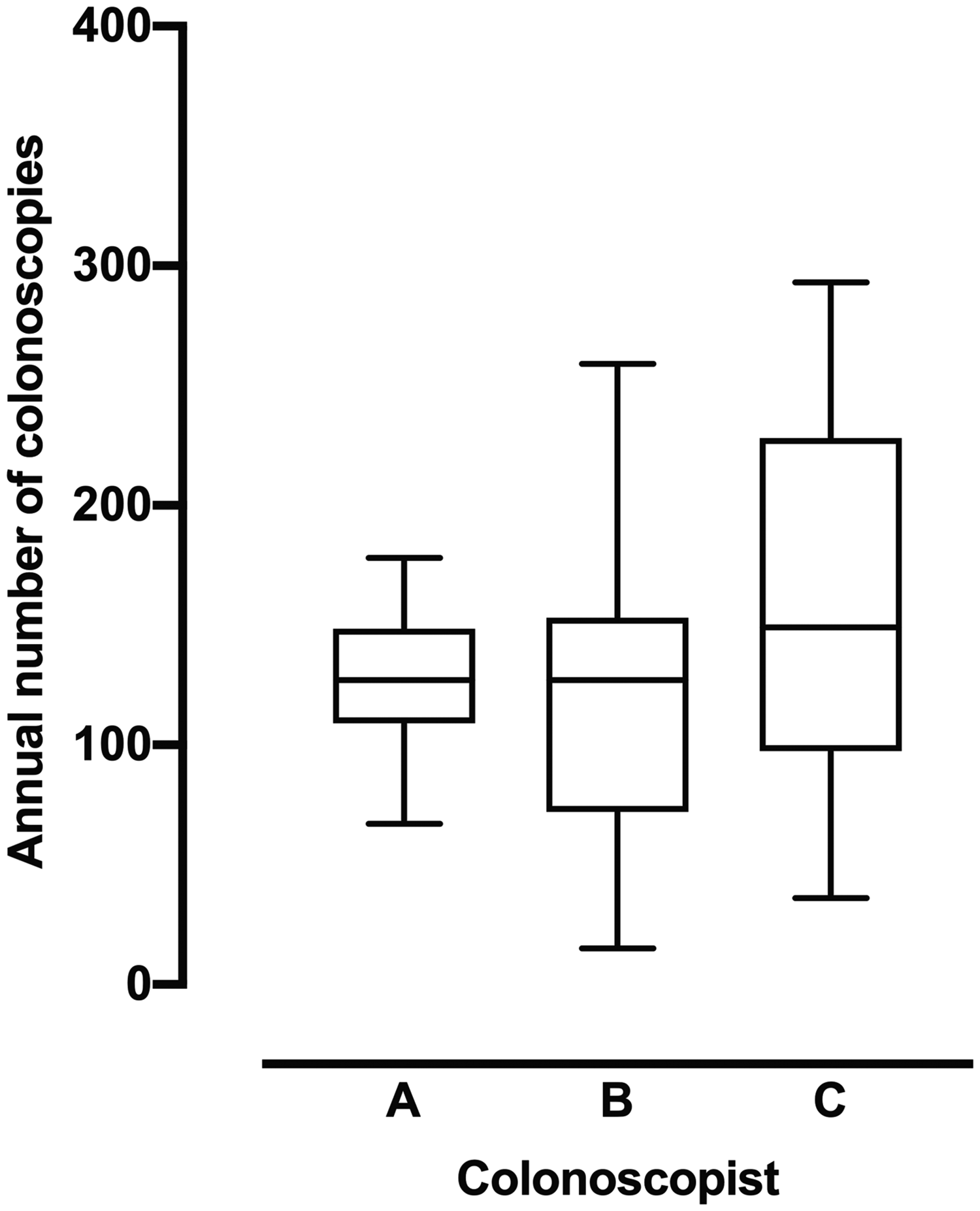
Annual number of colonoscopies performed by colonoscopists A, B and C. The horizontal bar indicates median, the box indicates interquartile range and the whiskers represent the 95% confidence intervals.
Global rating scales
The overall CIR for the study period was 97.3%, and the overall ADR was 47.7%. Overall CRC detection rate was 10.0%. When trends over time in GRS metrics were analysed for all three colonocopists, there were significant trends over time for CIR (p = 0.015) (Figure 3(a)), ADR (p < 0.001) (Figure 3(b)) and proportion requiring IV sedation (p < 0.001) (Figure 3(d)). There were no significant trends in proportion of patients with minimal or mild discomfort scores (p = 0.606) (Figure 3(c)), rate of adverse events (p = 0.503) (Figure 3(e)) or cancer detection rate (p = 0.089) (Figure 3(f)). The GRS values for individual colonoscopists are summarised in Supplementary Tables 1–6.
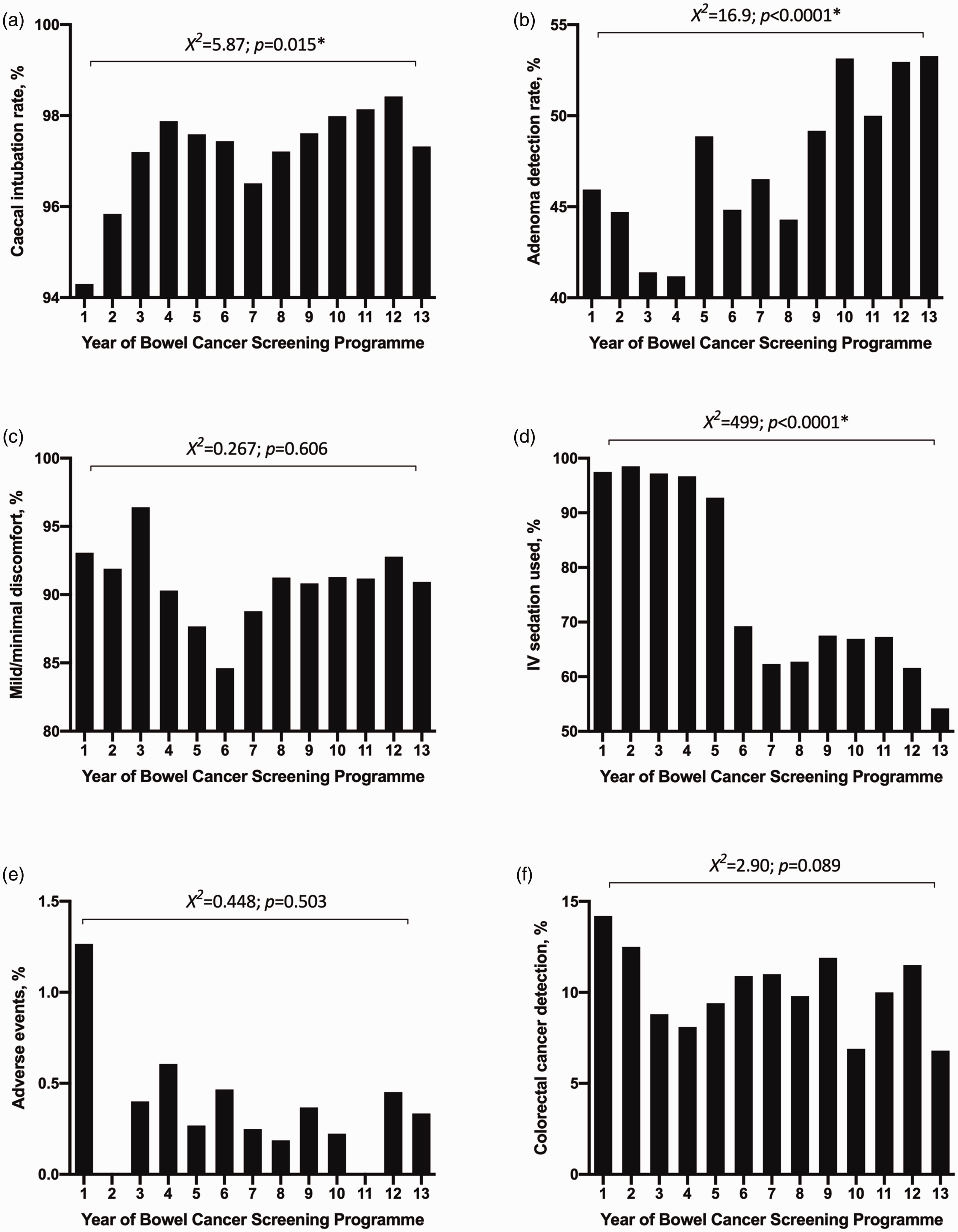
Trends over time since inception of the BCSP for (a) CIR; (b) ADR; (c) discomfort levels (percentage of patients with mild/minimal discomfort); (d) use of IV sedation; (e) adverse events and (f) CRC detection (*indicates statistically significant).
Adverse events
During the study period, there were 2/5352 (0.04%) patients who had a perforated colon, and 15/5352 (0.28%) who had post-procedure gastrointestinal bleeding (Table 2). There were no significant trends over time for adverse events overall (combined post-procedural gastrointestinal bleeding and colonic perforation), or specifically for perforation or post-procedure bleeding (Table 2).
Adverse events following screening colonoscopy during the study period.
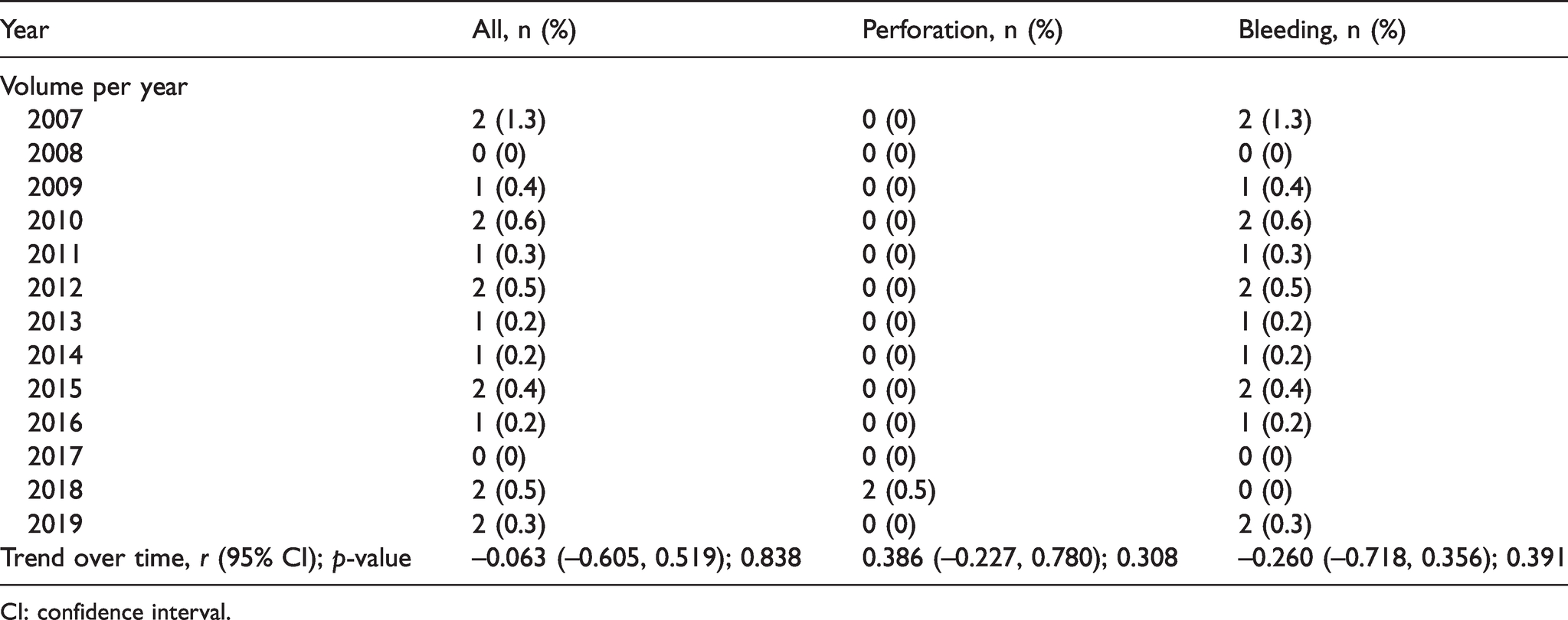
CI: confidence interval.
Discussion
The main finding from our observational study of participants in the BCSP who had a positive FOBt or high-risk findings at flexible sigmoidoscopy over a 13-year study period is that the GRS has consistently improved over time, even with a high baseline threshold set for the screening programme. There is improvement in most domains of the GRS in this study cohort. These findings suggest that even very experienced practitioners may improve the quality of colonoscopy over years of high-volume practice (>120 colonoscopies per year on average). Importantly for patients, it is likely that they can expect high-quality colonoscopy in the English BCSP after being referred with a positive FOBt or high-risk findings at flexible sigmoidoscopy.
Achievement of competency in diagnostic colonoscopy requires a dedicated training pathway for individuals to gain the necessary skills and then maintain these in clinical practice. There are some barriers to effective colonoscopy training within the trainee pathway, such as a reduction in available time, insufficient numbers of dedicated training lists and wrong case-loads for effective training. 8 These must be addressed if the high-quality indicators reported in the current study are to be maintained for future generations of endoscopists. Organisations such as the British Society of Gastroenterology have established programmes to monitor standards, such as the Endoscopy Quality Improvement Programme in order to reduce heterogeneity in training and standards in the UK.9 Our study findings may emphasise the importance of case volume of endoscopic practice, which represents a challenge that must be addressed for the training of future screening endoscopists.
In a previous study of more than 10,000 colonoscopies in England from 2007 to 2010, the authors reported an overall CIR of 90.2%, ADR of 19.2% and perforation rate of 0.06%, and that these markers were superior for those with higher volumes of practice. 5 Others have reported CIR of 95.2% and ADR of 46.5% for more than 34,000 BCSP colonoscopies. 4 The data from the current study demonstrate superior caecal intubation (97.3%) and adenoma detection (47.7%) to these reports, and a very similar rate of perforation (0.04). The three colonoscopists within the current study have high volume practices, which may be one of the factors contributing to the high standards. Other investigators have reported CRC detection during colonoscopy of approximately 1–6%. 10 , 11 The CRC detection rate in the current study was 10%, which is higher than these other reports, and may also reflect the higher volumes of practice.
There is some evidence that screening colonoscopy is performed at a higher standard than non-screening colonoscopy. 12 However, the overall success of a BCSP depends on a series of steps that require attention (rather than simply colonoscopy), such as the invitation and participation of all those eligible for screening, as well as the sensitivity and specificity of initial screening tests. Each of these must be of high quality at the system, provider and individual levels in order to reduce mortality from CRC.13 High-quality endoscopy – such as that reported in the current study – must be taken in the context of an effective screening programme overall. For example, efforts to improve the screening process amongst the population must also be made to ensure maximum uptake. 14 The accepted minimum uptake is currently set at 52%. 15 Some investigators have proposed that utilisation of population segmentation tools might help to identify groups of the population with poorer uptake in order to provide more targeted awareness and participation. 16 It is recommended that concurrent attention is given to patient uptake, quality of colonoscopy and overall quality of patient experience, follow-up and care.
There were a very low number of adverse events within this cohort of patients in the screening programme. However, even though the quality of colonoscopy improved over time, there were no negative trends in adverse events. This may suggest that adverse events (albeit at a low rate) are relatively unavoidable, even with experienced providers with high-volume practices. Comfort scores did not appear to improve over time within this study cohort – a finding that requires some attention if centres seek to improve patient-centred practice. 17 However, there was a dramatic reduction in the use of IV sedation over the same time period. When these data are viewed together, they suggest that patients were not in any further discomfort despite lower levels of IV sedation, which may seem counterintuitive. One interpretation of these data may be that discomfort usually associated with more difficult colonoscopy 18 was reduced over the study period, in keeping with an overall improvement in quality. Alternatively, these findings may suggest that higher rates of IV sedation in the earlier years of the BCSP were unjustified, and that usage was reduced to a more appropriate level over the years without the cost of increasing discomfort. Efforts to improve patient-centred care would require further investigations to determine the optimal levels of IV sedation whilst still reducing the overall discomfort for patients.
Limitations
The current study reports the 13-year data from three endoscopists at a single English BCSP centre, and therefore these data may not necessarily be translatable to other centres, systems and programmes. Furthermore, it is unknown whether there were any changes over the study period in the baseline population risk of polyps or cancer that might have influenced some of the GRS standards. There are differences in access to upgrades in endoscopy technology between sites in the BCSP (including scope guides and better-quality endoscopes). In the 13-year study period, it is possible that equipment has improved to a degree that might have influenced some of the variables that account for differences in GRS, which may have introduced some confounding bias.
Conclusion
Screening colonoscopy was performed at a high standard during the last 13 years of the BCSP at our centre. There were further improvements over time for the three colonoscopists who were undertaking high-volume practice over this time period. Patients who have been referred for colonoscopy following positive FOBt can expect high-quality diagnostic colonoscopy as part of the current screening programme.
Supplemental Material
sj-pdf-1-msc-10.1177_09691413211009562 - Supplemental material for Impact of cumulative experience on the quality of screening colonoscopy: A 13-year observational study
Supplemental material, sj-pdf-1-msc-10.1177_09691413211009562 for Impact of cumulative experience on the quality of screening colonoscopy: A 13-year observational study by David N Naumann, Cheryl Kavanagh, Gaynor Hipkiss, Sarah Potter-Concannon, Misra Budhoo, Monzur Ahmed and Sharad Karandikar in Journal of Medical Screening
Footnotes
Authors’ contribution
SK and DNN planned the study. SK, DNN, CK, GH and SP-C conducted the study and collected the data. SK, MB and MA were the endoscopists participating in the study. DNN analysed and interpreted the data. DNN wrote the first manuscript. SK, MB and MA provided critical appraisal and revisions. All authors approved the final version of the manuscript.
Acknowledgements
The authors thank the endoscopy department for participating in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.