
Abstract
Objective
To explore the association between disability and participation in breast, cervical, and colorectal cancer screening in Flanders (Belgium).
Methods
Data from the Centre for Cancer Detection were linked to data of the Flemish Agency for disabled persons by the Crossroads Bank for Social Security, using National Social Security Numbers.
Results
The study population consisted of 92,334 invited individuals registered as disabled in 2013–2015. For breast cancer screening (including both opportunistic screening and participation in the screening program), 51.7% of disabled women had undergone mammography in the last two years, compared with the Flemish uptake of 61.8%. In cervical screening, 45% of the women with a disability had undergone a PAP smear in the last three years (overall Flemish uptake was 60.7%). For colorectal cancer screening, 40.7% of individuals with a disability had undergone a fecal immunochemical test in the last two years (overall Flemish uptake was 51.5%). Participation in breast and colorectal cancer screening among persons with a disability was 10% points less than the Flemish average during the same period. In the cervical cancer screening program, the difference between the participation of disabled women and the Flemish average was 10% points. Persons with any type of disability had a lower uptake of cancer screening than the Flemish average, except for individuals with a hearing impairment.
Conclusions
Participation disparities in the Flemish cancer screening programs between persons with and without disabilities require specific efforts to increase cancer screening among people with a disability.
Introduction
In Flanders (Belgium), three population-based cancer screening programs exist. 1 Breast cancer screening started in 2001. Eligible women aged 50–69 are invited to attend a biennial two-view mammogram, which is double read. Some women also undergo opportunistic screening. Cervical cancer screening was primarily opportunistic until 2013, when organized screening promoting one cervical smear every three years for women aged 25–64 was introduced. In the colorectal cancer screening program, operative since 2013, a fecal immunochemical test (FIT) is mailed biennially to the homes of individuals aged 56 (reducing to 50 in 2020) to 74. In all three programs, invitations and accompanying information leaflets are sent by mail. Only in the colorectal screening program are reminders sent. More detailed information can be found on the website or by dialling a toll-free phone number. Participation in the breast and colorectal screening programs is free of charge, but the cost of further examinations or treatment following an abnormal test result falls under the regulation of the Belgian health care system. This applies also for participating in the cervical cancer screening program. Patients generally pay costs upfront and are partially reimbursed by their health insurance fund.
Although the United Nations Convention on the Rights of Persons with Disabilities and its Optional Protocol, ratified by Belgium in 2009, 2 states that persons with disabilities should be provided with “the same range, quality and standard of free or affordable healthcare and programmes as provided to other persons, including population-based public health programmes,” some literature suggests that participation in routine cancer screening programs may be reduced in people with disabilities. Although their cancer risk equals that of the general population.3,4 The objective of this study was to explore the association between different disabilities and participation in cancer screening in Flanders.
Methods
The Flemish Agency for Disabled Persons aims to promote participation, integration, and equal opportunities for individuals with a disability in all life areas, whether they are living in or outside an institution. Disability is defined as any long-term and significant participation problem experienced by a person, which is attributable to a combination of functional disorders of a learning, psychic, physical or sensory nature, limitations in the performance of activities, and personal and external factors. The definition has a clear link with international definitions such as that published by the World Health Organization. For the definition (severity and long-term) and for the classification of mental disorders (including behavioural and emotional disorders), the Flemish Agency for Disabled Persons relies on the Diagnostic and Statistical Manual of Mental Disorders. For the determination of a mental handicap, the Flemish Agency for Disabled Persons focuses on the definition of the American Association on Intellectual and Developmental Disabilities.
The Centre for Cancer Detection coordinates screening programs in Flanders, using a centralized invitation procedure. The target populations are identified from the central population registry. Non-eligible persons (e.g. people with an invasive tumour or those who have had the respective organ removed) and those who actively opt out are included on an exclusion list compiled by the Belgian Cancer Registry. Unique 11-digit National Social Security Numbers are used to cross-link the population registry with the Belgian Cancer Registry data.
The study population consisted of women aged 25–74 and men aged 56–74 registered in the database of the Flemish Agency for Disabled Persons in 2015. The studied periods were 2014–2015 for breast and colorectal screening, and 2013–2015 for cervical screening. Participation was defined as having undergone mammography in the last two years (either through organized or opportunistic screening), having had a PAP smear taken in the last three years, and having a FIT analysed during the last two years.
Data from both organizations were merged by the Crossroads Bank for Social Security using National Social Security Numbers, and the data were returned in aggregated tables, ensuring anonymity. The study was approved by the Belgian privacy commission. Frequency distributions were generated to describe screening uptake, stratified by disability type. All statistical analyses were performed with SPSS version 24.
Results
Of the disabled women, 51.7% had undergone mammography in the last two years, (compared with the Flemish uptake of 61.8%), and 45% had undergone a PAP smear in the last three years (Flemish uptake was 60.7%). Among men and women with a disability, 40.7% had undergone a FIT in the last two years (Flemish uptake was 51.5%). Participation in the breast and colorectal cancer screening programs among persons with a disability was 10% points less than the Flemish average during the same time period. For the cervical cancer screening program, the uptake difference between women with a disability and the Flemish average was 15% points during the same time period. Persons with any type of disability participated less in all three cancer screening programs than the Flemish average, except for individuals with a hearing impairment (Table 1). Individuals with mild, moderate, and severe learning disability (whether or not in combination with another handicap) and/or with a cognitive disability had the lowest screening uptake.
Participation in cancer screening programs according to disability type.
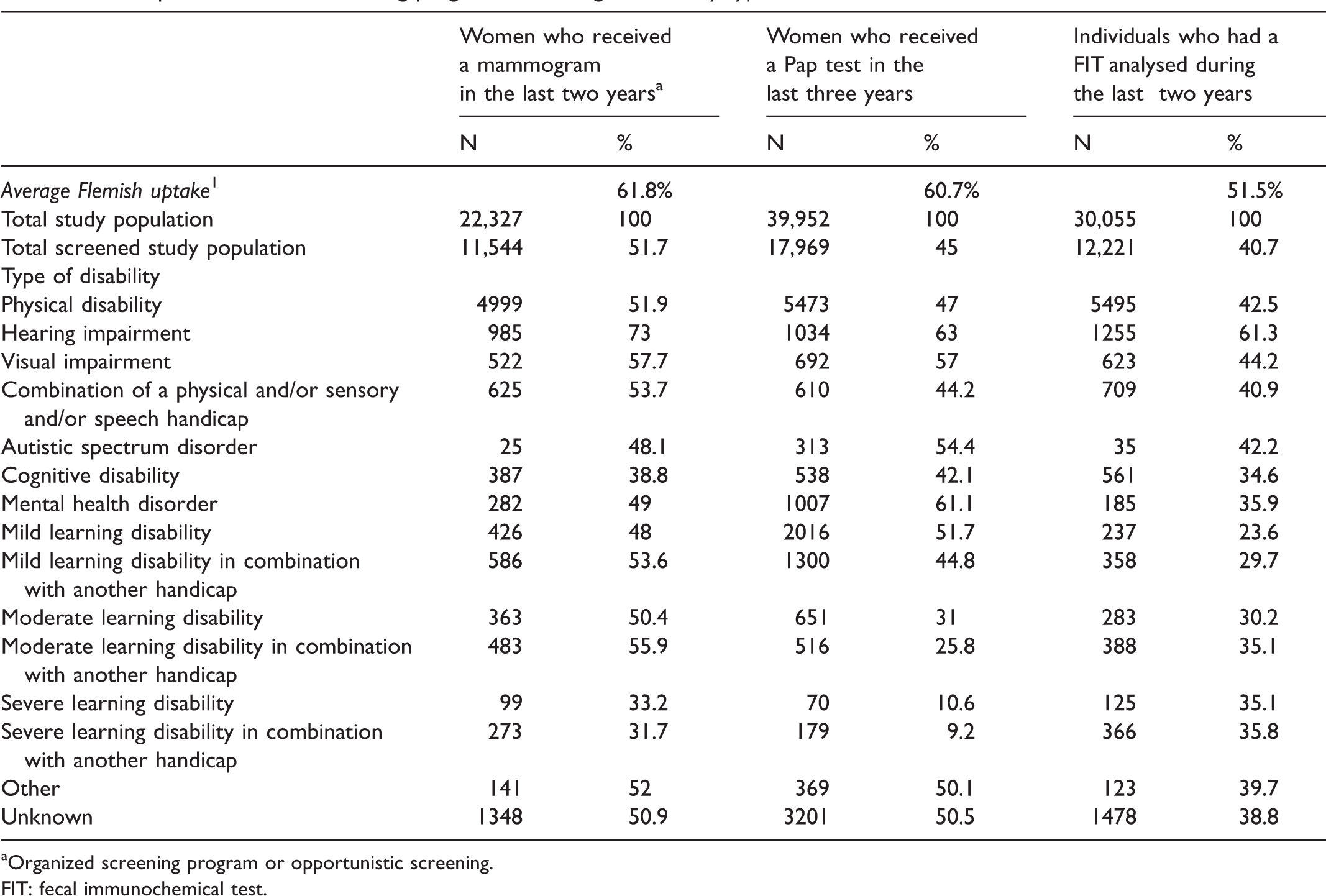
Organized screening program or opportunistic screening.
FIT: fecal immunochemical test.
Discussion
Persons with any type of disability had a lower uptake of all cancer screening programs than the Flemish average during the same time period, except for individuals with a hearing impairment, who were better screened than the Flemish average. The lowest screening uptake was seen amongst individuals with a mild, moderate, and severe learning disability (at least 65% of whom are not adequately screened for breast, cervical and colorectal cancer), and among individuals with a cognitive disability.
Previous studies have examined the question of uptake of cancer screening among persons with disabilities. A systematic review of five publications found modest evidence for disparity in breast and cervical cancer screening with increasing disability levels, and among women with the most severe disability. The review also drew attention to varied definitions of disability and severity in the publications, and of differences in indicators of screening guidelines. 5 A US paper found, similarly to our own findings, that people with vision or cognitive limitations were less likely to have been screened for colorectal cancer than those with hearing impairment. 6 A Canadian study demonstrated a low uptake of cancer screening among adults with intellectual and development disabilities.7,8 One report from France on women with an intellectual disability living in institutions found participation in breast cancer screening to be slightly higher than among the general population (64.4% vs. 62% respectively), 3 but another found a low cervical cancer screening rate amongst women living in institutions in France. 9 A review on colorectal cancer in people with intellectual disabilities concluded that, although this group has a risk of colorectal cancer comparable with the general population, their uptake of screening is lower. 4
A centrally organized screening program is unable to identify which individuals of the target population have a disability. Future research should explore why the uptake of cancer screening among Flemish disabled persons is lower than the Flemish average. Large media campaigns with images of persons without a disability may not appeal to individuals with a physical disability. Using written material may hamper uptake by persons with a visual or learning disability. The attitude and knowledge of their legal guardians may play a pivotal role in enhancing screening uptake among persons with a learning disability. It is also possible that general practitioners do not sufficiently direct persons with a disability towards preventive health care. 5 Tailored interventions to promote cancer screening among men and women with different disability types need to be developed. A qualitative study among mammography technologists and radiologists reported that the participants were uncertain about respectful and appropriate communication with disabled women; screening disabled women may require additional time and accommodations. 10
A published review has identified the barriers to breast and cervical cancer screening that are encountered by women with physical disability. Many healthcare workers ignore the importance of screening to women with a disability, and physical barriers (transport, accessibility of mammography screening machines and examination tables) hamper attendance. 11 Another review identified additional individual barriers to screening, including intellectual ability, anxiety, and interpersonal factors such as spousal or other support systems, and stressed the need for additional training for health care providers to discuss cancer screening with their patients who have disabilities. 12
Linkage of the screening database with the database of the Flemish Agency for Disabled Persons, using National Social Security Numbers, made it possible to conduct a study with high quality information. Not relying on self-report data on screening status and disabilities minimized selection and information bias, and enhanced validity and generalizability. Another strength of the study is the large sample size. The study did have some weaknesses. The small sample size for some disability types may limit the generalizability for those types. Because the database of the Flemish Agency for Disabled Persons was considered the data source, and we received the joined data in aggregated tables from the Crossroads Bank for Social Security, we were not able to statistically compare people with and without a disability. In addition, the population used to calculate the average Flemish uptake did not exclude persons with a disability, however, if this introduced bias we believe it is limited, as the number of people with a disability is small compared with the number of those without.
Conclusion
This study demonstrates that disparities exist in the Flemish cancer screening programs between persons with and without disabilities. Future research is required to explore why the uptake of Flemish disabled persons in cancer screening programmes is lower than the Flemish average.
Footnotes
Acknowledgements
We thank the members of the Breast, Cervical, and Colorectal Cancer Screening Working Groups of the Flemish government, and the members of the research group of the Centre for Cancer Detection, for their valuable comments on the progress of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the Flemish government.