
Abstract
Objective
Despite a growing body of evidence suggesting inequalities in breast cancer screening uptake in the United States for women with disabilities, few attempts have been made to examine whether this association applies to the United Kingdom. We conducted the first population-wide study investigating the impact of disability on uptake of breast cancer screening in Northern Ireland.
Methods
Breast screening records extracted from the National Breast Screening System were linked to the Northern Ireland Longitudinal Study. This identified a cohort of 57,328 women who were followed through one complete three-year screening cycle of the National Health Service Breast Screening Programme in Northern Ireland. The presence of disability was identified from responses to the 2011 Census.
Results
Within this cohort, 35.8% of women reported having at least one chronic disability, and these individuals were 7% less likely to attend compared with those with no disability (odds ratio 0.93; 95% confidence interval 0.89–0.98). Variation in the degree of disparity observed was evident according to the type and number of comorbid disabilities examined.
Conclusion
This is the first population-wide study in Northern Ireland to identify disparities in breast screening uptake for women with chronic disabilities, in particular, those with multimorbidity. This is of particular concern, given the projected rise in the prevalence of disability associated with the ageing population.
Introduction
Breast cancer is now the commonest cancer in the United Kingdom (UK), accounting for 15% of all new cancer cases diagnosed each year. 1 Early diagnosis, through routine screening of the at-risk population, remains the gold-standard method of detecting breast cancer and reducing the mortality associated with the disease. 2 Since the implementation of the National Health Service Breast Screening Programme (NHSBSP) in 1988, there has been some controversy surrounding the potential harms of the programme; however, an independent review concluded that the 20% reduction in breast cancer mortality far outweighs the potential harms associated with routine screening. 2 The efficacy of the programme, and the subsequent gain in terms of mortality benefit, is reliant on maintaining high participation rates. Although there is some regional variation, approximately 74% of eligible women in the UK attend breast screening every year. 3 Whilst this figure exceeds the UK minimum standard (70%), uptake remains below the 80% national target, and this has been identified as a central factor contributing to avoidable cancer deaths. 4
Considerable research exists examining the underlying determinants of participation in breast cancer screening.5–10 Although the vast majority of studies focus on the impact of socio-demographic factors on breast screening uptake, there is evidence implicating poor physical health as a key determinant of screening behaviour, 7 and a growing body of evidence that women with disability are significantly less likely to participate in breast screening.11–16 This is not unexpected given the extensive literature indicating that these individuals experience inequalities in many other aspects of healthcare service utilisation, including preventive cervical cancer screening,17–20 and oral health services.19,21
Many potential mechanisms through which disability may contribute to reduced breast screening participation relate to the additional physical barriers to screening attendance, including difficulty obtaining suitable transport to screening appointments, lack of accessibility at screening centres, and difficulty standing unaided during screening. 22 Increased levels of social deprivation among those with disabilities may also contribute further to uptake inequalities, given that social deprivation has been linked to reduced breast screening uptake.7,8,23,24 Although there are currently no meta-analyses or systematic reviews summarising the evidence between disability and breast cancer screening uptake, the available evidence has been narratively reviewed. 12 In three of the five studies included in this review, attendance at breast screening was significantly lower for women with disability.13,18,25 However, the authors noted that considerable methodological heterogeneity and an inability to universally control for confounding factors, particularly social determinants such as socio-economic status, cause difficulty in making reliable inferences from the results and hinder the generalisability of these studies. Additionally, although there is a growing body of research examining this association in the United States, there is a dearth of studies investigating this relationship in the UK. This research gap is particularly concerning in light of a recent study which showed that women with disability in England were nearly 40% less likely to attend routine breast screening. 11 Although the authors provided robust, population-wide evidence of disparities in breast cancer screening uptake for women with disabilities, this study was limited to previous breast screening attenders. As previous attendance is a significant determinant of future attendance at screening, whether these findings can be generalised to the wider body of individuals who are eligible for breast cancer screening is unclear.26,27
With the prevalence of disability projected to rise with the ageing population, a better understanding of the relationship between disability and breast screening attendance is essential, not only in overcoming the inequalities in screening access, but in the drive to reduce the overall morbidity and mortality associated with breast cancer. 28 This paper aims to describe a more generalisable population-wide study to determine whether chronic disabilities are associated with reduced uptake of routine breast cancer screening in the UK, and more specifically: (i) to examine the overall association between having any disability and participation in breast screening, (ii) to examine the association between different types of disability and multimorbidity on participation in breast screening, and (iii) to investigate whether the effect of disability on screening attendance is modified by social factors such as marital status and car access.
Methods
In the UK, women aged 50–70 are invited to attend breast screening once every three years. Data for all women invited through the Northern Ireland Breast Screening Programme in the three-year screening cycle following the 2011 Census were extracted from the National Breast Screening System. Attendance was recorded as a binary yes/no variable. Individuals who do not attend their original screening appointment are sent a second invitation several weeks later. Women who attended their subsequent appointment were classified as attenders. These were subsequently linked to the Northern Ireland Longitudinal Study (NILS) via encrypted Health and Care numbers to produce a de-identified research dataset.
The NILS is a large-scale data-linkage study containing information on approximately 28% of the population of Northern Ireland (∼508,000 people). NILS members are drawn from the Northern Ireland Health Card Registration System (the centralised system containing information on individuals registered to receive health and social care through the National Health Service) on the basis of birth date. Anyone with one of 104 pre-designated birth days is included in the cohort. Additional information including vital events, such as births, deaths, and marriages, migration data, and data from the 1981, 1991, 2001, and 2011 Census are also linked to the NILS core database. A more detailed overview of the NILS has been presented previously. 29
All individual, household, and area level cohort attributes were drawn from the 2011 Census, within the NILS core database. Variables included in the model were selected based on previous evidence of association with breast screening uptake. Age at the 2011 Census was categorised in five bands: under 50, 50–54, 55–59, 60–64, and 65–70. The under 50 group was included to incorporate women who reached eligibility for breast screening in the three years following the 2011 Census. Marital status was classified as ‘currently married’, ‘separated, widowed or divorced’, or ‘single (never married)’. National-Statistics Socio-Economic Status (NSSEC) combines occupation with employment status to provide an indication of socio-economic position. 30 In the 2011 Census, NSSEC was calculated based on an individual’s most recent period of employment, so that estimates could be made for retired or short-term unemployed individuals. For the purposes of the study, NSSEC was divided into ‘managerial, administrative and professional’, ‘intermediate’, ‘own account’, ‘lower supervisory and technical’, ‘routine and semi-routine’, and ‘never worked, were full-time students, or long term unemployed’. Measures of housing tenure (owner, private renter, or social renter), educational attainment (degree or higher, up to A-Level, up to GCSE, or none), and number of cars or vans in the household (two or more, one, or none) were included as supplementary indicators of social class. Number of cars also provided insight into means of accessing the screening clinic. Finally, an indicator of area of residence was included, in which individuals were classed as living in the Belfast Metropolitan Area, or the rest of Northern Ireland.
Measure of disability in this study was based on the 2011 Census data, in which participants were asked, ‘Do you have any of the following conditions, which have lasted, or are expected to last, at least 12 months?’, Participants were asked to tick all that applied from a list of 12 options: (i) ‘deafness or partial hearing loss’; (ii) ‘blindness or partial sight loss’; (iii) ‘communication difficulty (a difficulty with speaking or making yourself understood)’; (iv) ‘a mobility or dexterity difficulty (a condition that substantially limits one or more basic physical activities such as walking, climbing stairs, lifting or carrying)’; (v) ‘a learning difficulty, an intellectual difficulty, or a social or behavioural difficulty’; (vi) ‘an emotional, psychological or mental health condition (such as depression or schizophrenia)’; (vii) ‘long-term pain or discomfort’; (viii) ‘shortness of breath or difficulty breathing (such as asthma)’; (ix) ‘frequent periods of confusion or memory loss’; (x) ‘a chronic illness (such as cancer, HIV, diabetes, heart disease or epilepsy’; (xi) ‘other condition’; (xii) or ‘no condition’ were all possible responses. ‘Chronic illness’ was excluded from the analyses to avoid crossover in answers, as the first nine responses could be considered ‘symptoms’ of a chronic illness (e.g. someone who has a chronic illness such as arthritis is likely to also respond as having a mobility or dexterity difficulty). Similarly, ‘other condition’ was also excluded, as the lack of additional information prevents classification of the condition as a disability. Although in some cases mental disorders meet the criteria for disability status, there is a well-recognised distinction between physical/neurological disabilities and mental disorders. Responses to ‘an emotional, psychological or mental health condition (such as depression or schizophrenia)’ were therefore excluded as this is beyond the scope of the analysis.
The final cohort consisted of 57,328 women aged between 48 and 70 at the 2011 Census, who were invited for routine breast screening through the Northern Ireland NHSBSP in the three-year screening cycle following the 2011 Census. The study was approved by the Office for Research Ethics Committee Northern Ireland (ORECNI), the local ethics committee in Northern Ireland (ORECNI no: 07/NIR01/90 + 5).
Descriptive statistics were employed to compare the socio-demographic characteristics of women with and without disability. Crude uptake rates were calculated to facilitate inter-group comparison. Uptake was calculated as the percentage of women who attended breast screening out of the total number of women invited for screening during the study period.
Logistic regression was utilised to calculate age-only and fully adjusted odds ratios and 95% confidence intervals (CIs) for attendance at breast screening. Initially, logistic regression was employed to examine the overall impact of having any disability on participation in breast screening, with gradual adjustment for socio-demographic confounders. Any disability refers to the presence of any of the disabilities examined in the study. To assess and compare the impact of specific types of disability on breast screening uptake, odds ratios were calculated for women with a single disability in isolation. For this investigation, a separate logistic regression model was produced for each type of disability included in the study against a common comparator (women with none of the disabilities examined in the study). To disentangle the effect of having multiple disabilities on screening attendance, separate logistic regression models were generated to examine the impact of each type of disability on attendance against the reference group with no disability, with further adjustment for the presence of all other types of disability as binary yes/no variables. Subsequently, an indicator of multimorbidity was employed, to examine the impact of comorbid disabilities on breast screening uptake.
Interaction terms were included in fully adjusted models to determine whether the effect of disability on screening uptake was modified by marital status or car access.
Results
In this sample, 35.8% of women reported at least one disability (see Table 1). Long-term pain or discomfort was the most commonly reported disability (21.2%), followed by mobility or dexterity difficulties (20.4%), and shortness of breath or difficulty breathing (12.2%). Women with a disability were more likely to be older, be un-married, live in rented accommodation, have no access to a car, be unemployed, have no educational qualifications, and live in the Belfast Metropolitan Area (see Supplemental Table 1). In the age-only adjusted logistic regression models, women with a disability were 29% less likely to attend screening compared with their counterparts with no disability (OR 0.71, 95% CI 0.68–0.74). Further adjustment for marital status and socio-economic differences explained the majority of this effect; however, the negative influence of disability remained statistically significant with further adjustment for area of residence (OR 0.93, 95% CI 0.89–0.98). Interaction terms were introduced into the model to determine whether marital status or car access offsets the effect of having any disability on breast screening uptake; however, no statistically significant interactions were observed (where p > 0.05).
The likelihood of attending breast screening by disability status. Data show the odds ratios (ORs) and 95% confidence intervals of attending breast screening with gradual adjustment for socio-demographic characteristics.

Adjusted for social class (NSSEC), housing tenure, number of cars in the household, and educational attainment.
Figures in bold indicate significance at p < 0.05.
Among the 17.3% of women who reported having a single disability in isolation (see Table 2), long-term pain or discomfort was the most commonly reported disability (5.6%). Although initial comparison of the crude uptake rates revealed lower attendance for all types of disability except deafness or partial hearing, the fully adjusted logistic regression models revealed that only mobility or dexterity difficulties were associated with significantly reduced odds of attending screening (OR 0.88, 95% CI 0.80–0.97), although overadjustment for factors such as car access and social class (which may not be applicable covariates for individuals with particular disabilities, e.g. car access in individuals who report blindness or partial sight loss) potentially explains this observation. There was some evidence that women with blindness or partial sight loss who were single were less likely to attend screening than married women (OR 0.28, 95% CI 0.12–0.63, p = 0.002); however, no significant interaction effects were observed for any other types of disability.
Effect of single disabilities on screening attendance: results represent the numbers and proportions of people with single disabilities, uptake rates, and ORs (95% CI) of attending screening, from separate logistic regression models comparing each disability against people with no disability.
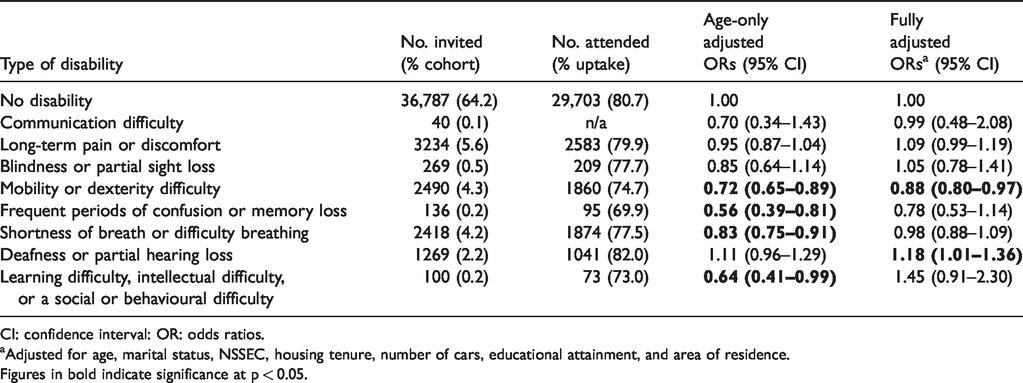
CI: confidence interval: OR: odds ratios.
Adjusted for age, marital status, NSSEC, housing tenure, number of cars, educational attainment, and area of residence.
Figures in bold indicate significance at p < 0.05.
Logistic regression was employed to examine the impact of different types of disability, allowing for the presence of multimorbidity (see Table 3). In the age-only adjusted models, having any of the examined disability types was associated with significantly reduced attendance at breast screening compared with those with no disability. With further adjustment for socio-demographic characteristics, having frequent periods of memory loss or confusion (OR 0.75, 95% CI 0.66–0.85), communication difficulty (OR 0.80, 95% CI 0.67–0.96), a mobility or dexterity difficulty (OR 0.85, 95% CI 0.80–0.89), shortness of breath or difficulty breathing (OR 0.90, 95% CI 0.85–0.96), or long-term pain or discomfort (OR 0.93, 95% CI 0.88–0.98) were associated with significantly reduced attendance at screening compared with those with no disability. However, these associations were attenuated considerably with adjustment for the presence of other disabilities, and only mobility or dexterity difficulties (OR 0.88, 95% CI 0.81–0.95) and frequent periods of confusion or memory loss (OR 0.76, 95% CI 0.58–1.00) remained significant determinants of reduced screening attendance. There was some evidence that participation in screening was lower for those with deafness or partial hearing loss who were single, compared with their married counterparts (OR 0.65, 95% CI 0.47–0.88, p = 0.006); however, there was no evidence that being married or having access to a car modified the effect of any other type of disability on screening uptake.
The association between different types of disability and screening attendance: results represent ORs (95% CIs) of attending screening compared to those with no disability.
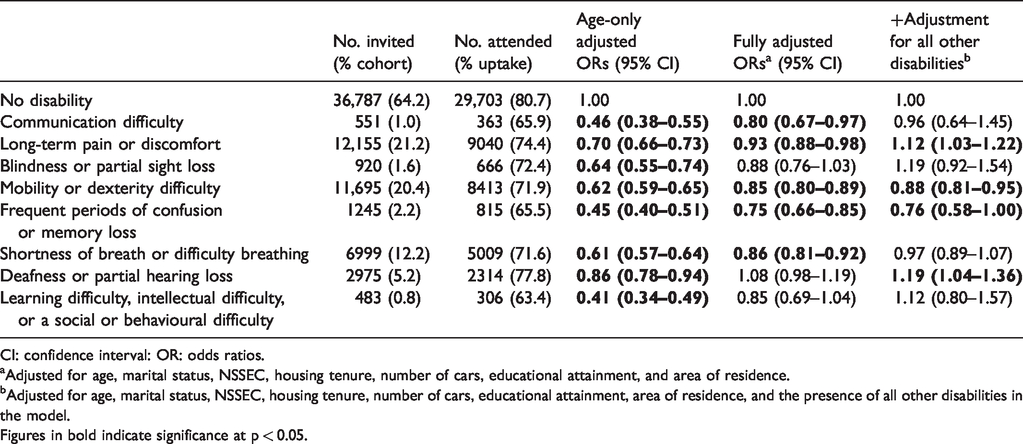
CI: confidence interval: OR: odds ratios.
Adjusted for age, marital status, NSSEC, housing tenure, number of cars, educational attainment, and area of residence.
Adjusted for age, marital status, NSSEC, housing tenure, number of cars, educational attainment, area of residence, and the presence of all other disabilities in the model.
Figures in bold indicate significance at p < 0.05.
Among those who reported disability, multimorbidity was more common than singular disability; 17.4% reported having only one disability whilst 18.5% of individuals in the cohort reported multimorbidity (see Table 4). Although a strong dose–response effect was observed with increasing number of disabilities, the magnitude of the effect was attenuated with adjustment for other socio-demographic factors. After adjustment for these attributes, women with two or three disabilities were, respectively, 9% (OR 0.91, 95% CI 0.85–0.97) and 16% (OR 0.84, 95% CI 0.77–0.91) less likely to attend screening compared with those with no disabilities. Women with four or more disabilities were over 25% less likely to attend (OR 0.76, 95% CI 0.66–0.86). There was no evidence that the effect of multimorbidity on breast screening uptake was modified by car access or marital status (p > 0.05).
The effect of multimorbidity on attendance rates: results represent the numbers and proportions of women with one, two, three, or four+ disabilities; uptake rates; and the odds ratio (OR) and 95% confidence intervals of attending screening.
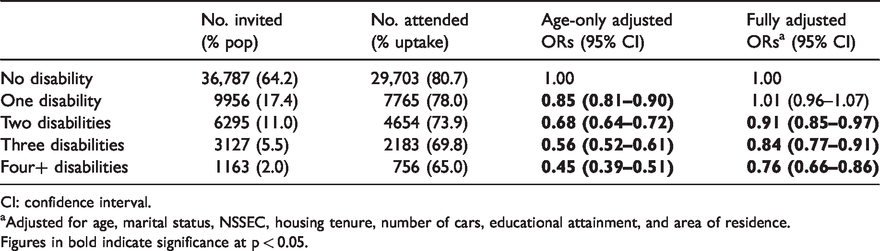
CI: confidence interval.
Adjusted for age, marital status, NSSEC, housing tenure, number of cars, educational attainment, and area of residence.
Figures in bold indicate significance at p < 0.05.
Discussion
The findings of this study provide population-wide evidence of disparities in breast cancer screening uptake for women with disabilities in the UK. Attendance at screening was not only influenced by the presence of a disability, but also by the type of disability and the number of comorbid disabilities.
The results indicate that, overall, women with any disability are 7% less likely to attend screening compared with women with no disability, although the true effect size is probably much greater, given the challenges in appropriately adjusting for confounders across the various types of disability examined. Although there is a severe lack of research on the impact of disabilities on breast screening attendance in the UK, this finding builds on a previous study, 11 which observed a 36% reduction in the odds of attending breast screening in women with any disability. Although a much smaller effect size was observed in our study, this can be explained by the inclusion of a more limited range of disability types, and the ability to apply ‘thresholds’ in the other study, which limited the analysis to more severe forms of disabilities.
Although there was evidence that some types of isolated disabilities had greater impact on a woman’s likelihood of attending screening than others, with the exception of individuals with mobility or dexterity difficulties, the significance of these associations was fully attenuated with adjustment for socio-demographic factors. Given the extensive variation in the socio-demographic characteristics of individuals across the spectrum of disability, and the resulting difficulty in universally controlling for confounders, it is important to consider the role of overadjustment in these findings. For example, adjusting for factors such as educational attainment and socio-economic status in individuals with learning disabilities, given the well-documented inequalities in access to education and employment, probably underestimates the true extent of this association. 23
Further analyses accounting for the presence of comorbid disabilities revealed disparities in uptake by type of disability examined, particularly for women with mobility or dexterity difficulties, frequent periods of confusion or memory loss, or shortness of breath or difficulty breathing. Whilst there is also a dearth of literature examining the impact of specific types of disability on screening attendance, these findings generally corroborate the observations made in the existing literature.11,25
Multimorbidity was also an important determinant of screening uptake. As previously noted by Floud et al. 11 and Chan et al., 17 a dose–response relationship was evident with increasing number of disabilities. Having two or more disabilities was significantly and cumulatively associated with lower breast screening attendance, which can presumably be attributed to the increased degree of activity limitation imposed by having comorbid disabilities.
The findings from this study are reflective of the qualitative literature examining the barriers to obtaining screening for women with disabilities, and together, provide further clarification of the underlying explanation for the disparities in uptake.31–33 In a review of the literature, Ramjan et al. 22 highlighted a lack of accessible features at screening units, healthcare workers attitudes and knowledge about disabilities, and difficulties in standing unaided during screening mammography as key deterrents to attending screening. This probably explains the larger disparities observed for particular types of disability, e.g. mobility or dexterity difficulties, as the limitations of certain disabilities will impose greater obstacles to participation than others.
Further analyses were employed to determine whether the additional social and physical support (i.e. having the support of a partner and having access to a car) modifies the association between having a disability and attendance at screening. Notably, there was no evidence to suggest that car access or marital status modified the overall impact of having any disability on uptake. The findings of the current study contrast with those by Floud et al., 11 who observed that individuals with disability who had no access to a car were significantly less likely to attend compared with similar individuals with car access, although the inclusion of a broader range of disabilities, and an inability to adjust for severity in the current study may have contributed to the ‘dilution’ of the observed disparities. There was some evidence that for those with blindness or partial sight loss, not being married contributed to further reductions in uptake; however, no effect modification was observed for any other specific disability. Although this finding suggests that individuals with disability are universally affected by inequalities in screening access, it is possible that the study lacked statistical power to detect any significant interaction effects in this part of the analyses.
This study had both strengths and limitations. The study design provided a unique opportunity to prospectively examine the association between disability and breast cancer screening at a population-wide level. In contrast to previous research in the UK, the inclusion of previous non-attenders in the current study increases the generalisability of these findings to the wider body of women eligible for breast screening. The use of validated screening records and an indicator of disability reported prior to screening invitation surmounted the issue of recall-bias. The primary limitation of the study is the use of a self-reported measure of disability. As a result, responses were subject to an individual’s perception of their physical health. Furthermore, the lack of information on the severity of disability limited the scope of the analyses, and possibly contributed to an underestimation of the overall impact of disability on screening uptake, through the inclusion of less limiting conditions.
Conclusion
This is one of the few studies examining the impact of disability on breast cancer screening uptake in the UK. Our findings highlight concerning disparities in attendance at breast cancer screening for women with disability, particularly for those with multimorbidity. This evidence must be carefully considered by policy makers, to ensure that targeted interventions can be put in place to ensure equity in accessing preventive screening for all women, especially given the projected rise in disability associated with the ageing population.
Supplemental Material
MSC888553 Supplemetal Material - Supplemental material for Disability as a predictor of breast cancer screening uptake: A population-based study of 57,328 women
Supplemental material, MSC888553 Supplemetal Material for Disability as a predictor of breast cancer screening uptake: A population-based study of 57,328 women by Emma Ross, Aideen Maguire, Michael Donnelly, Adrian Mairs, Clare Hall and Dermot O’Reilly in Journal of Medical Screening
Footnotes
Acknowledgements
The help provided by the staff of the Northern Ireland Longitudinal Study (NILS) and the NILS Research Support Unit is acknowledged. The NILS is funded by the Health and Social Care Research and Development Division of the Public Health Agency (HSC R&D Division) and NISRA. The NILS-RSU is funded by the ESRC and the Northern Ireland Government. The authors alone are responsible for the interpretation of the data and any views or opinions presented are solely those of the author and do not necessarily represent those of NISRA/NILS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ORECNI, the local ethics committee in Northern Ireland (ORECNI no: 07/NIR01/90 + 5).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a studentship from the Department for the Economy (DFE), formerly the Department for Employment and Learning (DEL).
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.