
Abstract
Objective
We previously found that administering a pre-screening lifestyle questionnaire lowered the subsequent attendance proportion in the first-ever colorectal cancer screening. We sought to determine whether the effect continued in subsequent screening rounds.
Methods
The eligible survey cohort (n = 10,375) received a follow-up questionnaire in 2012, and in 2013, they were invited for colorectal cancer screening for the second time. For the third screening round, in 2015, no questionnaires were sent in the previous year. Screening attendance in 2013 and in 2015 was examined in relation to survey mailings.
Results
The colorectal cancer screening attendance rate in 2013 was 58.4% in the survey population, and 63.9% in those not surveyed (P < 0.001). In 2015, the screening attendance rate was 61.7% among those who had been sent the questionnaires in 2010 and in 2012, and 66.2% in those not surveyed (P < 0.001). The reduction in screening attendance was greater at the second (2013) round than at the first (2011).
Conclusion
The effect of the initial survey seemed to continue even when no questionnaires were being sent. Attendance among those who had been sent questionnaires earlier did not reach the level of the group that was never surveyed.
Organized screening programmes provide appealing settings for epidemiological surveys, but such additional investigations may reduce willingness of the target population to participate in screening. A population-based colorectal cancer (CRC) screening programme using biennial fecal occult blood testing (FOBt) for 60–69 year olds has been running in Finland since 2004. 1 The ‘Psychosocial effects of colorectal cancer screening study’ was incorporated into the CRC screening programme in 2010–2012. Lifestyle and quality of life were assessed through a self-administered postal questionnaire at baseline one year before the first screening invitation, and again after two years.2,3 We previously reported that participation after the first screening invitation was lower among those surveyed (56.6% vs. 60.2%). 2 A similar baseline phenomenon has been reported from England, where CRC screening uptake was significantly lower in those who received a questionnaire with their FOBt kit than in those who did not (48.6% vs. 53.5%). 4 The purpose of this study was to examine CRC screening behaviour after subsequent invitations, to determine if the effect of surveys on screening attendance is long term.
The study population consisted of individuals born in 1951, residing in municipalities involved in the CRC screening programme and, therefore, eligible to be invited to CRC screening in 2011 (n = 31,951). In 2010 (i.e. in advance of screening), we sent a random sample of every sixth subject (n = 5312) a 7-paged lifestyle questionnaire, and to another random sample of every sixth subject (n = 5336) a 10-paged lifestyle and quality of life questionnaire (Figure 1). In 2011, 31,484 individuals of the original cohort (467 had moved to a non-screening municipality, or died) were independently randomized (1:1) to be invited for CRC screening (n = 15,748) or to the control group (n = 15,736), according to the invitation schema of Finnish CRC screening programme.
1
In 2012, the survey cohort (n = 10,375; 273 had either died, refused 2010, or had unknown address) received a follow-up questionnaire with the same contents as in 2010. In 2013, 15,041 individuals were invited to CRC screening for the second time, following the original screening randomization, irrespective of their attendance at the previous screening round. The third screening round was in 2015 (14,096 individuals invited), with no questionnaires sent the previous year.
Flow chart of study population of ‘Psychosocial effects of colorectal cancer screening’ study.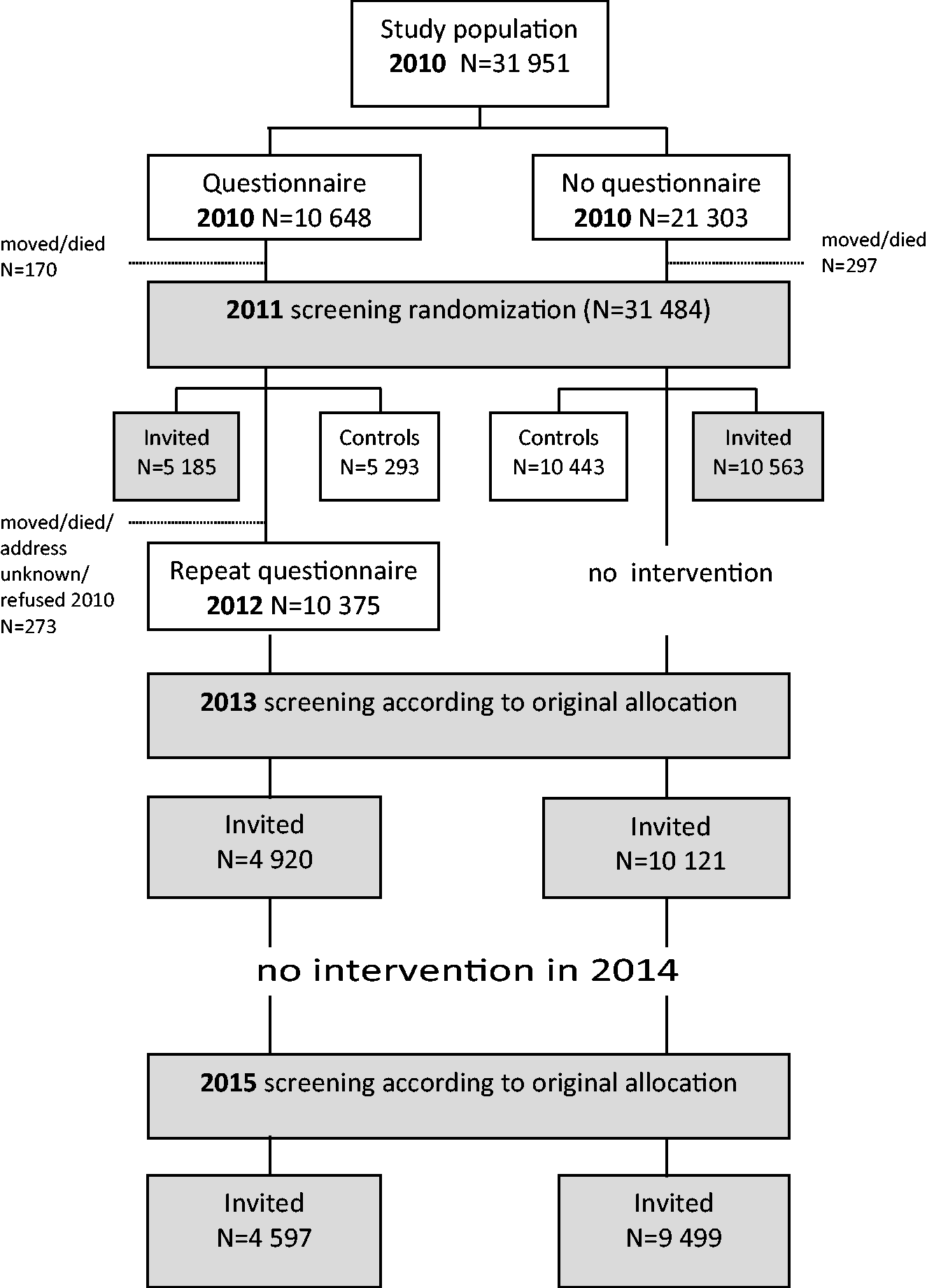
To assess the association between CRC screening attendance and inclusion in the survey study, two-way tables were used. Screening attendance proportions were compared between those who were and were not sent the questionnaires, using a two sample test of proportions (z-test) with a 5% significance level. Attendance was also compared by sex, marital status, urbanization level of residential area and geographical area of residence. The study received ethical approval from the Helsinki and Uusimaa Hospital District Ethics Committee (15 December 2009, 420/13/03/00/2009).
Colorectal cancer screening attendance 2013 and 2015 in those sent and not sent study questionnaires 2010 and 2012.
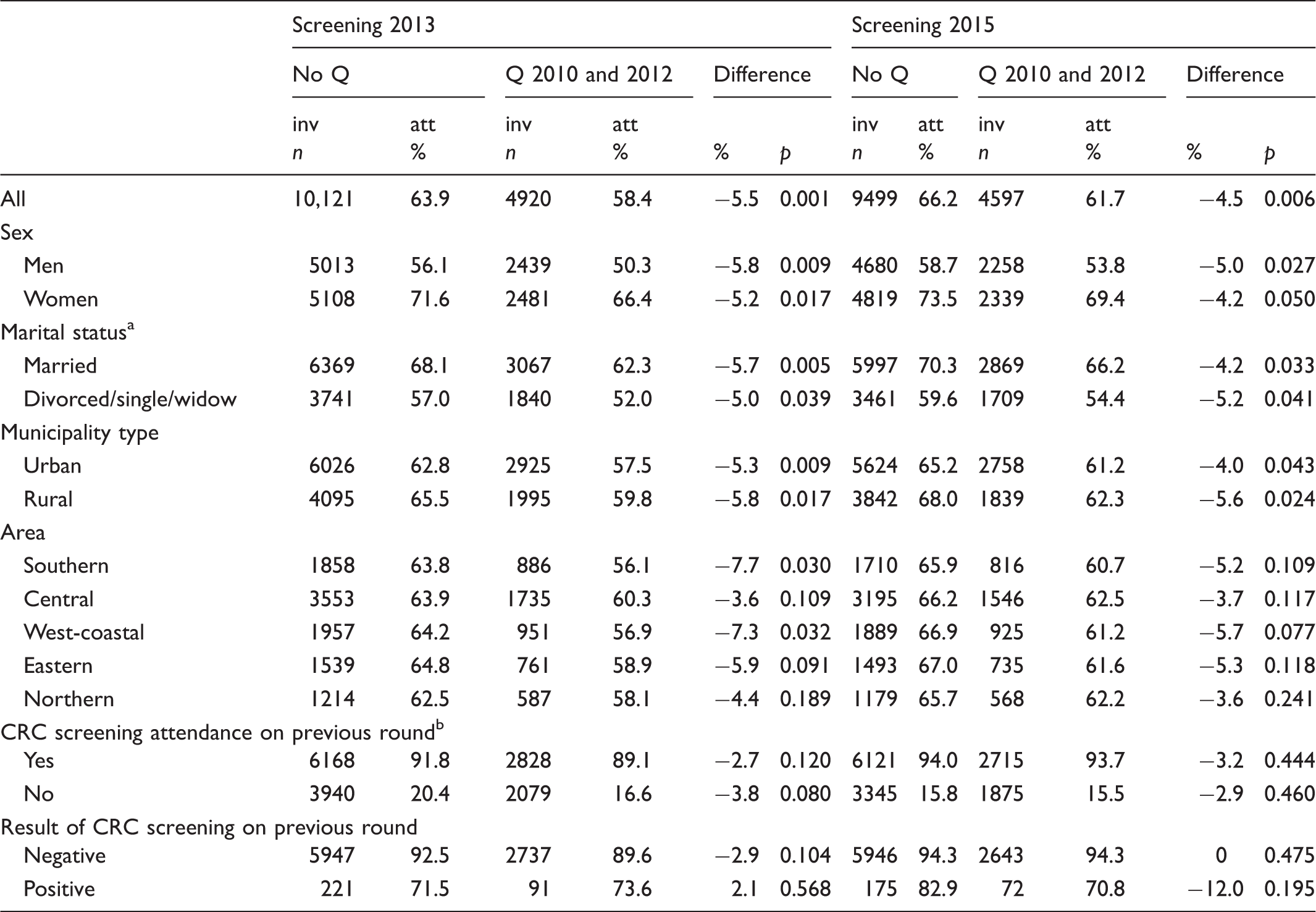
Q: study questionnaire; inv: invited; att: attended; CRC: colorectal cancer.
Marital status was missing in Population Register Centre data for 24 persons in 2013 and in 20 persons in 2015.
Twenty-six persons in 2013 were not invited in 2011, and 40 persons in 2015 were not invited in 2013.
In 2015, screening attendance was still significantly lower in those who had received the questionnaires in 2010 and 2012 than among those who had not. Attendance was 61.7% (62.0% for short and 61.4% for long questionnaire) and 66.2%, respectively (p = 0.006).
Being subjected to a questionnaire study before screening invitation resulted in reduction in CRC screening attendance. We found that the detrimental effect of questionnaires on screening attendance was long term. The effect augmented with repeated surveys; the reduction in screening attendance in those subjected to questionnaires was greater in the second (2013) than in the first screening round (2011). The effect seemed to continue so that in the subsequent third screening round with no questionnaires the previous year, the attendance still did not reach the level of the group never exposed to questionnaires. Results were similar for men and women, by marital status, and by area. Unlike in 2011, the length of the questionnaire did not have an effect on screening attendance, except in Northern Finland, where screening attendance was decreased only among the long (10-paged) questionnaire recipients.
Screening attendance for CRC screening in the survey study population remained low in 2015, even though one could imagine that the detrimental effect of burdensome questionnaires would dilute after not receiving the questionnaires anymore. We believe that the long-term effect is partly due to attendance pattern, i.e. previous screening behaviour (especially participation in the first invitation round) is a predictor of subsequent participation. This has been observed previously in the context of breast cancer screening5–7 and CRC screening.8–10 Those disturbed by the original study questionnaires in 2010 established a pattern of non-participation, which did not abate with time.
Jäntti et al. 3 examined, in this same population, whether screening allocation in 2011 had any impact on follow-up survey response. Among CRC screening invitees in 2011 response to the survey increased in 2012 compared with that in 2010, whereas among controls (not invited for screening) the response to the survey decreased slightly. These results support the idea that it is the nature of the contact, not just the contact, which is essential. The screening invitation can be perceived as a service or offer, which could make the attitude towards the subsequent survey more positive. Rather laborious surveys, instead, can be seen as a burden, and the rejection of this burden also affects future screening.
Adequate attendance is fundamental for successful population screening, and careful monitoring and optimization of attendance must be ensured in any screening programme. Surveys are necessary to obtain information that health care or other registers cannot provide. When embedding surveys in cancer screening, questionnaire design should aim to include only relevant issues, in a compact form, and to present the questionnaire as advantageous for the recipient. There is an ethical issue in employing a research intervention endangering engagement; the benefit gained should outweigh the harm caused by reduced attendance.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.