
Abstract
Introduction
Renal cancer incidence has increased markedly in the United States in recent decades, largely due to incidentally detected tumours from computed tomography imaging. Here, we analyze the potential for low-dose computed tomography lung cancer screening to detect renal cancer.
Methods
The National Lung Screening Trial randomized subjects to three annual screens with either low-dose computed tomography or chest X-ray. Eligibility criteria included 30 + pack-years, current smoking or quit within 15 years, and age 55–74. Subjects were followed for seven years. Low-dose computed tomography screening forms collected information on lung cancer and non-lung cancer abnormalities, including abnormalities below the diaphragm. A reader study was performed on a sample of National Lung Screening Trial low-dose computed tomography images assessing presence of abnormalities below the diaphragms and abnormalities suspicious for renal cancer.
Results
There were 26,722 and 26,732 subjects enrolled in the low-dose computed tomography and chest X-ray arms, respectively, and there were 104 and 85 renal cancer cases diagnosed, respectively (relative risk = 1.22, 95% CI: 0.9–1.5). From 75,126 low-dose computed tomography screens, there were 46 renal cancer diagnoses within one year. Abnormalities below the diaphragm rates were 39.1% in screens with renal cancer versus 4.1% in screens without (P < 0.001). Cases with abnormalities below the diaphragms had shorter median time to diagnosis than those without (71 vs. 160 days, P = 0.004). In the reader study, 64% of renal cancer cases versus 13% of non-cases had abnormalities below the diaphragms; 55% of cases and 0.8% of non-cases had a finding suspicious for renal cancer (P < 0.001).
Conclusion
Low-dose computed tomography screens can potentially detect renal cancers. The benefits to harms tradeoff of incidental detection of renal tumours on low-dose computed tomography is unknown.
Introduction
As a result of the demonstrated reduction in lung cancer mortality using low-dose computed tomography (LDCT) in high-risk smokers in the National Lung Screening Trial (NLST), the United States Preventive Services Task Force (USPSTF) has recommended LDCT lung cancer screening for high risk smokers, 1 and the Center for Medicaid and Medicare Services has approved coverage for such screening in Medicare-eligible high-risk smokers. 2 As a result an increase in LDCT screening is expected over the next several years, with an associated increase in cardiovascular-related abnormalities, non-cancer related lung findings, and abdominal findings, in particular, renal lesions suggestive of cancer.
The approximately two-fold increase in renal cancer incidence in the United States in recent decades3,4 is generally acknowledged to be largely due to the growing use of imaging, especially computed tomography (CT) scans, with renal tumours increasingly being detected incidentally.4–6 Most of the increased incidence has been in localized disease and smaller tumours (<4 cm), and renal cancer mortality rates have remained essentially unchanged.3,4 Thus, it is likely that many renal cancers are being overdiagnosed, with potential harms due to treatment but little potential for a mortality benefit of earlier detection.
To address these issues, we assessed the incidence of renal cancer in the LDCT versus the chest X-ray (CXR) arms of the NLST trial and examined the rate of LDCT-detected renal abnormalities in subjects with and without a subsequent renal cancer diagnosis. We further performed a reader study to assess the extent to which the kidneys could be visualized on LDCT and to further characterize renal lesions seen on LDCT.
Methods
NLST design
The NLST randomized participants aged 55–74 to LDCT or CXR screening.7,8 Eligibility criteria included 30+ pack-years of cigarette smoking, and being a current smoker or having quit within the past 15 years. Participants enrolled at 33 screening centers across the United States during 2002–2004 received either LDCT or CXR screens at baseline (year 0) and annually for two more years (year 1, year 2). LDCT acquisition parameters were KVp of 120–140, mAs of 40–80 depending on body habitus, and reconstruction interval of 1.0–2.5 mm. A positive LDCT screen was defined as a non-calcified nodule ≥4 mm in greatest transverse diameter, 5 or other abnormalities such as mediastinal or hilar adenopathy and pleural effusion. The screening form included check-boxes for non-lung cancer LDCT findings of significant cardiac abnormalities, other significant abnormalities above the diaphragm, and other significant abnormalities at or below the diaphragm. For these, in addition to checking the box, radiologists provided a free-text written description of the abnormality on the screening form. Screens were classified overall as positive, negative without abnormalities, negative with minor abnormalities, or negative with clinically significant abnormalities, where “positive” and “negative” refer to suspicion of lung cancer and “abnormalities” refer to non-lung cancer-related findings. By protocol, radiologists determined whether an abnormality was clinically significant. Subjects and their physicians were notified of the results of the screen, including incidental (non-lung cancer related) findings. Diagnostic follow-up was carried out by subjects’ personal physicians.
Positive screens were tracked for diagnostic procedures and cancer diagnoses. Additionally, participants were followed with annual surveys to ascertain incident cancers (non-lung as well as lung). All reported cancers, including non-lung cancers, were verified with medical records. Deaths were tracked with the annual surveys and supplemented by National Death Index searches. For renal and other non-lung cancers, ICDO-3 codes and date of diagnosis were recorded, but not stage, tumour size, or treatment. Subjects were followed until 31 December 2009, death, or study withdrawal, whichever came first. The NLST was approved by the institutional review board at each screening center. All participants provided informed consent. Consent forms varied across screening centers; some included specific language concerning incidental findings and the fact that these could lead to unnecessary testing, whereas others did not.
Analysis
Person years of follow-up for renal cancer were computed from randomization date to the end of follow-up, or the date of renal cancer diagnosis, whichever came first, with renal cancer defined as ICDO-3 topography code 64.9. Renal cancer incidence rates were calculated as number of cases divided by person years. The Kaplan-Meier procedure was used to estimate cause-specific survival of renal cancer. We defined renal cancer as being present at the LDCT screen if there was a renal cancer diagnosis within one year and before the next screen (if any). We examined the relationship between renal cancer and LDCT screen findings, which included screen positivity and abnormalities at or below the diaphragm (ABD), using both univariate and multivariate analyses. The GENMOD procedure (SAS Version 12.2) was used to estimate multivariable odds ratios, using a logit link and compound symmetry to model within-subject correlations due to repeated screens; covariates included age, sex, smoking status, pack-years, ABD, and screen positivity. The screening form free-text written descriptions of non-lung cancer abnormalities, including ABDs, were available as electronic text fields, which were searched for keywords and patterns of responses to define broad anatomic categories of ABDs, including renal, hepatic, adrenal, gallbladder, and pancreas. Kidney-related abnormalities were further refined into the following hierarchical categories: mass or probable/possible mass, lesion, nodule, cyst, and stones/calcifications.
Reader study
A reader study was performed on all screens with renal cancer (diagnosed within one year) and a sample without renal cancer; for the latter, screens with ABDs on the original NLST report were oversampled. All images had personal identifiers removed before being sent to readers. Each screen was reviewed using a standardized form by two independent readers, blinded to renal cancer status and the original NLST read results; DG and RM were assigned one half of the screens (Group 1) and HN and LB the other half (Group 2). The reader study form included questions on (1) the presence of any ABDs, (2) the presence specifically of a lesion suspicious for a renal tumour, along with characteristics thereof, and (3) upper and lower slice numbers corresponding to the visible portion of the kidneys. Disagreements between readers on the presence of ABDs or of suspicious renal lesions were resolved through consensus. From the slice numbers, the visible portion of each kidney (as a percentage of the whole) was estimated by taking the difference between the upper and lower slice numbers, multiplying by the slice interval, and dividing by 10.5 cm (average length of the human kidney). The estimate for each reader of the portion of (both) kidneys visible was obtained by averaging the estimates across the two kidneys; the final estimate for analysis of the visible portion of the kidneys in each scan was derived as the average of the two reader estimates. Rates from the reader study were computed using the inverse sampling weights. The degree of reader agreement, before consensus, on the presence of an ABD was assessed using the Kappa statistic. Agreement between readers on proportion of kidneys visualized was assessed using correlation coefficients. The reader study was approved by the Institutional Review Board of the lead reading center.
Results
Of 26,722 and 26,732 participants enrolled in the LDCT and CXR arms, 99% (LDCT) and 98% (CXR) received at least one scheduled screen. Participants were 59% male, median (25th/75th) age was 60 (57/65), 48% were current smokers, and median pack-years was 48. Median follow-up was 6.5 years in each arm. There were 104 and 85 cases of renal cancer diagnosed in the LDCT and CXR arm, respectively (Figure 1), with incidence rates (per 10,000 person years) of 6.2 and 5.1, giving a relative risk (RR) of 1.22 (95% CI: 0.92–1.6; P = 0.18 for difference). Five-year renal-specific survival was 90.6% in the LDCT arm versus 88.2% in the CXR arm (P = 0.47).
Renal cancer incidence by trial arm.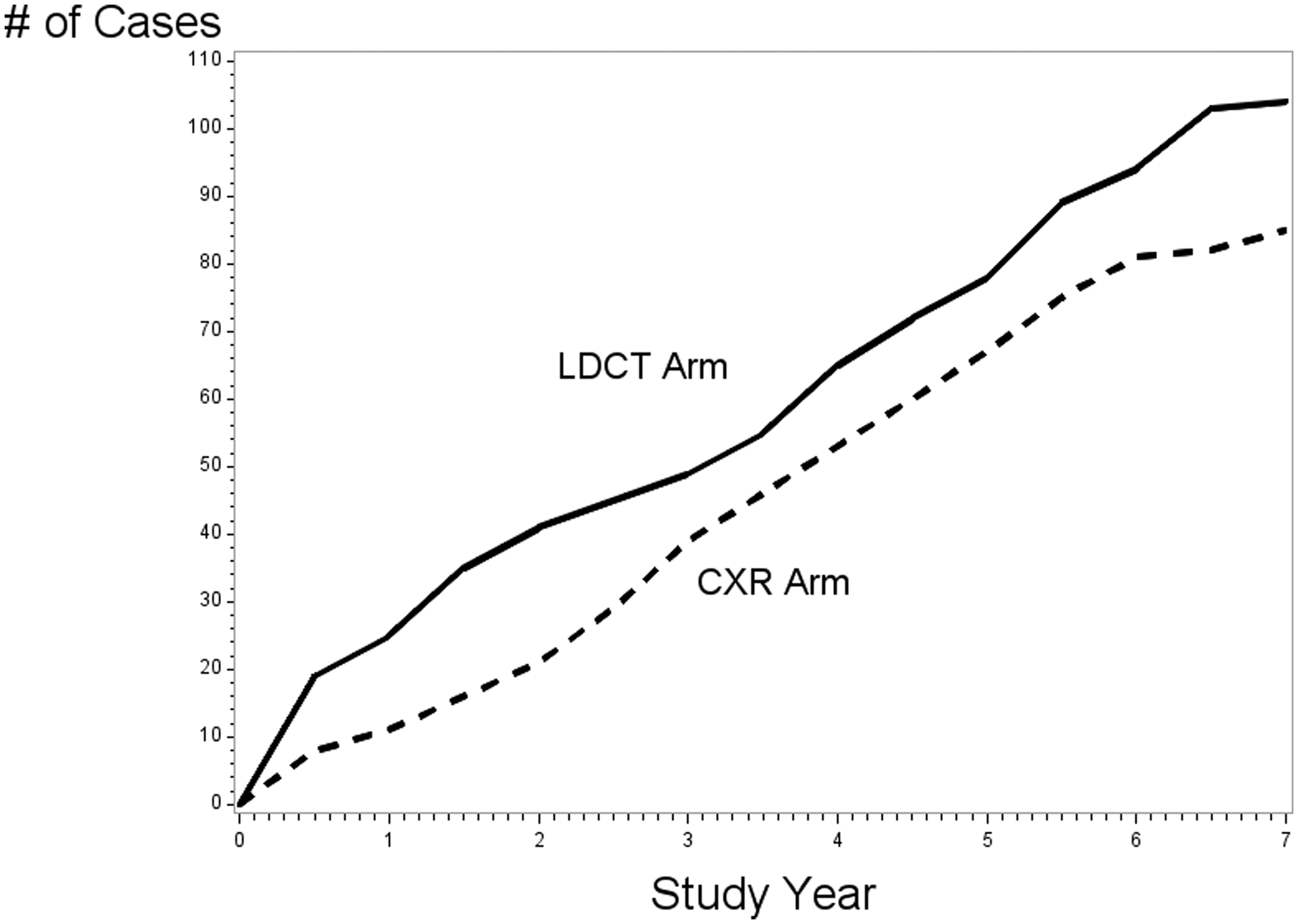
LDCT findings, smoking history, and demographics for screens with and without renal cancer.
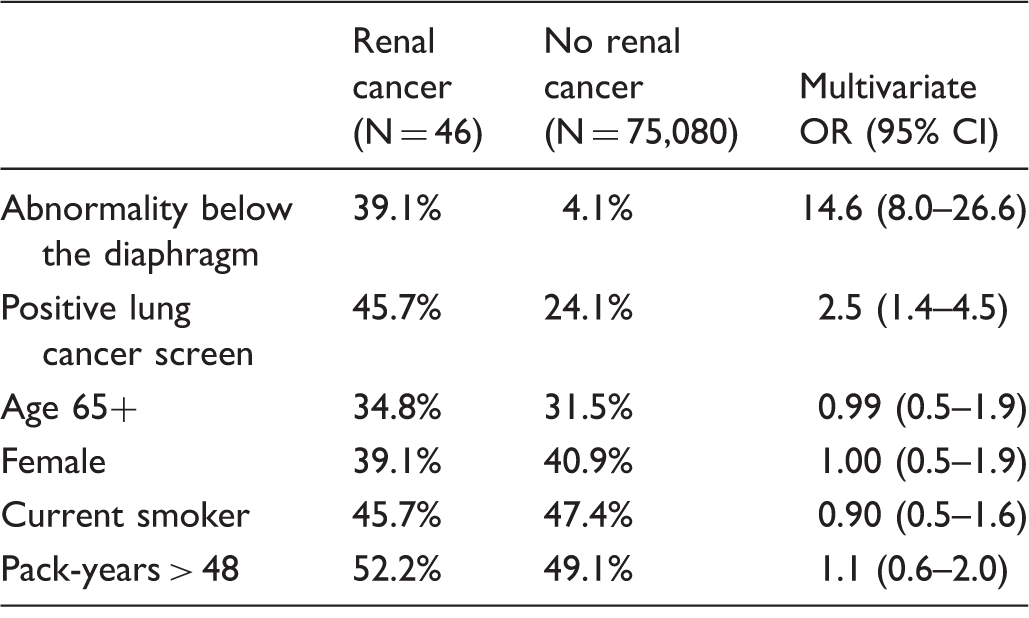
Note: Screens with renal cancer had a diagnosis within 365 days and before a subsequent screen (if any). Multivariate model controlled for all of the displayed factors.
Renal-related abnormalities below the diaphragm on LDCT screens.
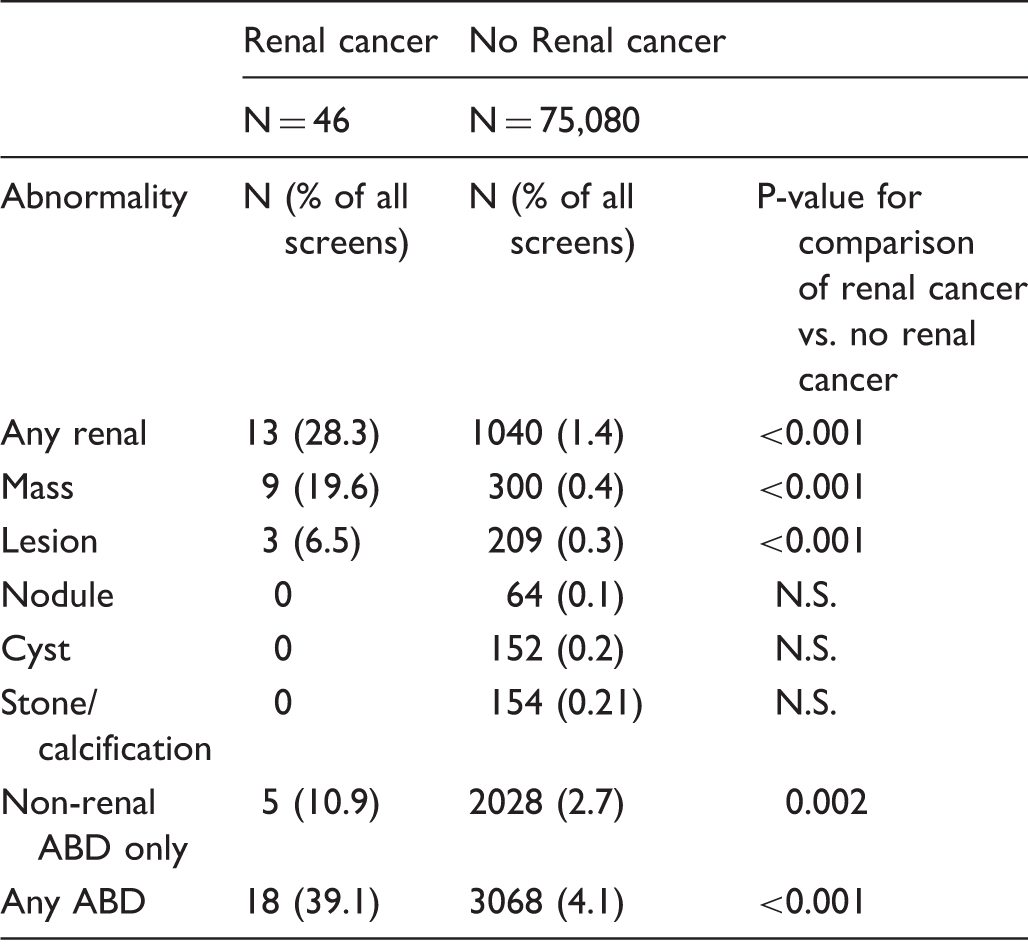
Note: Renal-related categories are hierarchical.
Reader study
Results of reader study.
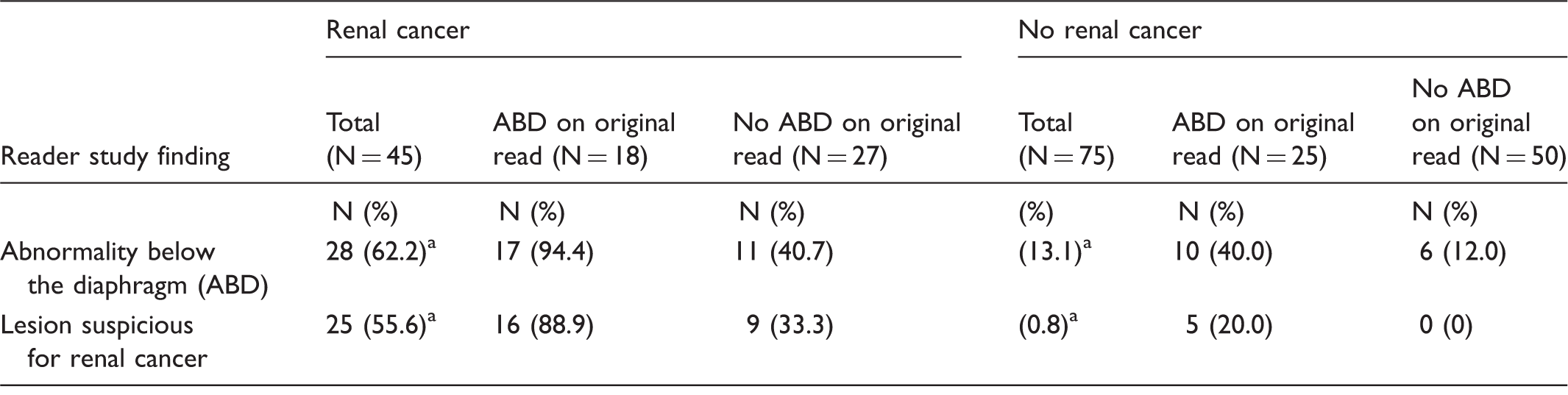
ABD: Abnormality below the diaphragm.
Note: For no renal cancer, images with ABD on original read were oversampled. Percentages for No renal cancer (total) reflect inverse weights of 0.0855 for ABD on original read and 1.0 for No ABD on original read. One renal cancer had no available image for the reader study.
P < 0.001 for comparison of renal cancer (total) vs no renal cancer (total).
Discussion
We found substantial evidence that renal tumours were being detected incidentally on LDCT exams in the NLST. The rate of finding an ABD was markedly higher among those with a renal cancer diagnosis within one year (39%) than among those without (4%). Further, among the renal cancer cases, those with an ABD had a considerably (and statistically significantly) shorter median time to diagnosis (71 days) than those without an ABD (160 days). This suggests that ABDs were noted disproportionately in eventual renal cancer cases, and that the reporting of ABDs had clinical consequences. In a more detailed analysis of ABDs based on radiologists’ written text fields, the rate of specifically renal-related ABDs was again substantially higher in renal cancer cases (28.3%) than in non-cases (1.4%).
Abnormalities other than ABDs may also have led to renal cancer detection. The lung cancer screen positivity rate was higher among renal cancer cases (OR = 2.5 controlling for presence of an ABD, age, sex, and smoking history), suggesting that additional imaging from diagnostic follow-up of positive screens could also have incidentally detected some renal tumours. The data on specific renal abnormalities allow clinicians to assess the a priori likelihood that such an abnormality seen on LDCT in a lung cancer screening population represents a renal tumour. For a renal mass, of 309 total reports, nine (2.9%) were followed by a renal cancer diagnosis within one year; this compares with 3.6% of positive LDCT screens being followed by a lung cancer diagnosis within one year. For the broader category of any ABD, the rate of renal cancer in the next year was substantially lower, 0.6% (18/3086). This retrospective analysis embedded within the NLST does not, however, permit clear distinction between detection of renal tumours with lethal potential and those that are overdiagnosed. Nor does it provide definitive evidence of the balance of benefits versus harms associated with the incidental discovery of other tumours. It does, however, provide radiologists and clinicians with an estimate of how frequently non-contrast LDCT of the chest can lead to non-directed discovery of renal abnormalities.
An ABD was identified in a substantially greater proportion of renal cancer cases in the reader study (62%) than the original NLST (39%), with only a small increase in ABD rate among non-renal cancer cases (13% vs. 4%). With the more specific reader study finding of a lesion suspicious for renal cancer, the rate among renal cancer cases was similar to the ABD rate (56%), while the rate among non-renal cancer cases was 0.8%. There are several possible explanations for the higher ABD rate in renal cancer cases in the reader study than in the original NLST. First, readers here knew they were participating in a study concerning renal cancer, and in a setting where the images were enriched for renal cancers, compared with the NLST where the focus was lung cancer, and renal cancer was expected to be rare. Also, in contract with the NLST setting, the reader study had no clinical impact. The reader study results show that, potentially, over half of renal cancers that would be diagnosed within a year of an LDCT lung cancer screen could be identified on that screen.
In an apparent paradox, only around 30% of the kidneys were visible on LDCT, yet the reader study showed 55% of renal tumours having a visible lesion. If LDCT screening detected renal tumours that were overdiagnosed and never would have become symptomatic, and as such tumours would have to be located in the visible portion of the kidneys, the diagnosed renal tumours would be expected to be disproportionately located in LDCT-visible regions.
Few studies have examined incidental renal tumours on LDCT lung cancer screening. Swensen et al. 9 reported on 1520 high-risk smokers undergoing 4436 LDCT screens over three rounds, with incidental LDCT findings including four renal cancers (0.90 per 1000 screens) and an additional 63 renal masses (14.2 per 1000 screens). Rampinelli et al. 10 examined extrapulmonary potentially significant incidental findings from an Italian study of LDCT screening in high-risk smokers. 10 Over five screening rounds and 23,128 LDCT screens, seven renal cancers were diagnosed following a potentially significant incidental finding (0.30 per 1000 screens). In our study, 18 renal cancers were diagnosed following an ABD over a total of 75,126 LDCT screens, for a rate of 0.24 per 1000 screens; the rate of finding a renal mass (without renal cancer) was 4.0 per 1000 screens (300/75,126).
Incidentally detected cancers raise the question of potential overdiagnosis. Although there were more cases in the LDCT (N = 104) than CXR arm (N = 85), the risk ratio was not statistically significantly elevated. A post-hoc analysis, however, showed only 33% statistical power to detect a true 25% increase in the LDCT versus CXR arm, so the likelihood of detecting a true modest incidence increase was small. Some CXR arm renal cancers could have been detected incidentally as part of the screening process, as CXR arm subjects with positive screens often received CT scans as diagnostic follow-up, but as the CXR positivity rate was only 7%, the potential for incidental detection of renal cancer was limited in this arm.
Whether the benefits of early detection of renal cancer outweigh the harms is an open question. The harms include possible overdiagnosis (and overtreatment) of renal cancer and additional imaging and other work-ups for renal cancer; the possible benefits include reduction in mortality from renal cancer. In this study, renal-cancer specific survival was high, about 90%, and not different by trial arm. As a randomized trial of renal cancer screening would not be feasible due to the low-population mortality rate of the disease, and lack of strong identifiable risk factors to select a high-risk group, it is difficult to assess potential benefits. Surrogate outcome measures such as survival can be analyzed; however, lead-time and overdiagnosis bias must be taken into account, making definitive conclusions unlikely. National trends of steady renal cancer mortality rates in the face of increasing incidence trends, due primarily to increases in incidental detection, argue that any mortality benefit of early detection through CT imaging of renal cancer would probably be modest.
There are several limitations to this study. Because the focus of NLST was lung cancer, the trial did not generally track the diagnostic follow-up of non-lung cancer-related abnormalities, and the diagnostic procedures received by those with reported ABDs are unknown. In addition, these findings come from a randomized trial and it is not clear how they would translate to clinical practice settings.
In conclusion, renal abnormalities are visible on LDCT screens in a substantial fraction of subjects with renal cancer. The harms-benefit tradeoff of incidental detection of renal tumours on LDCT screens is unknown.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.