
Abstract
Objective
Current United States recommendations for low-dose computed tomography (LDCT) lung cancer screening limit eligibility to ever-smokers with 30+ pack-years, with former smokers eligible only within 15 years of quitting. The 15 year limit is partly based on perceived decreases in lung cancer risk as years since quitting (YSQ) increase. We examine the relationship between lung cancer risk and YSQ among 30+ pack-year former smokers.
Methods
In the Prostate, Lung, Colorectal, and Ovarian trial, participants aged 55–74 were randomized to screening or usual care; screened subjects received annual chest-radiographs for lung cancer screening. Subjects completed a baseline questionnaire; smoking history included average cigarettes per day and age at starting and stopping smoking. Subjects were followed 13 years. Cox proportional hazards models were utilized to estimate hazard ratios (HRs) associated with YSQ, with YSQ treated as a time-varying covariate. The models adjusted for age and sex.
Results
Of 154899 subjects randomized, 27101 were former smokers with 30+ pack-years, and 69182 were never smokers. HRs relative to never smokers ranged from 30.8 (95% CI:23.4–40.5) for YSQ ≤5 to 6.4 (95% CI:5.1–8.0) for YSQ > 30. For YSQ of >10–15, >15–20, and >20–25, HRs were 14.8 (95% CI:11.9–18.2), 13.5 (95% CI:11.3–16.2), and 9.9 (95% CI: 8.1–12.0), respectively.
Conclusions
Lung cancer risk decreases gradually with YSQ in 30+ pack year former smokers. A range of upper limits on YSQ may be supportable for LDCT screening.
Introduction
The United States Preventive Services Task Force 2014 recommendations for low-dose computed tomography (LDCT) screening for current and former smokers with at least 30 pack years of cigarette smoking limited eligible former smokers to those who had quit smoking within the past 15 years. 1 The 15 year cutoff, as well as the 30 pack year minimum, mirrored the eligibility requirements for the National Lung Screening Trial (NLST), which provided much of the evidence base for the task force decision. 2 Other LDCT screening guidelines, and the 2015 Medicare coverage guidelines, also use the 15 year limit.3,4
The 15 year limit may have been chosen to cover screening in a population similar to that in the NLST (to date the only randomized trial showing LDCT benefit), and to restrict screening to those at sufficiently high lung cancer risk, in whom the evidence that the benefits of screening outweigh the harms is strongest. There may be a perception that lung cancer risk decreases substantially 15+ years since quitting smoking, however, no direct evidence or quantitative risk estimates have been cited to support the 15 year limit.
None of the studies on the relationship between years since quitting smoking (YSQ) and lung cancer risk have been tailored to the LDCT screening scenario, in terms of focusing on those with 30+ pack years and examining the short term risk of incident lung cancer, which is relevant in deciding who should be screened at a given time point. These studies also vary in important aspects, eg: specific intervals of YSQ for which relative risk estimates are presented, study design (case-control versus cohort), endpoints (incidence or mortality), and analytic approach (smoothed estimates using modeling or non-parametric estimates for each YSQ interval).5–8
The Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial randomized trial evaluated chest radiograph for lung cancer screening. 9 Unlike the NLST, it had no smoking history eligibility requirement, so the range of YSQ values through 30+ years can be examined. We examine lung cancer risk by YSQ in the PLCO cohort, among ever smokers meeting the 30+ pack year requirement of the various guidelines.
Methods
In the PLCO trial 10 participants aged 55–74 were randomized from 1993 to 2001 at ten screening centers across the United States. Exclusion criteria included history of a PLCO cancer, current cancer treatment, and removal of one lung. Intervention arm participants were offered annual posterior-anterior chest-radiograph for four years. Chest radiograph screens were considered positive if a nodule, mass, or other abnormality suspicious for lung cancer was noted. Diagnostic evaluation was decided by the patients and their physicians, not by trial protocol. All diagnosed cancers were ascertained, primarily by means of a mailed Annual Study Update (ASU) questionnaire, which asked about type and date of any cancers diagnosed in the prior year. Participants not returning ASUs were contacted by repeat mailing or telephone. Cancers were confirmed by medical records and trained abstractors recorded cancer histology and stage. Deaths were ascertained through the ASUs and other means, with supplementation by National Death Index searches. Participants were followed for up to 13 years, or until 31 December 2009, whichever came first.
At study entry, participants completed a baseline questionnaire on demographics, medical history, smoking history, and past screenings. The smoking-related questions asked if subjects had ever smoked cigarettes regularly for 6 months or longer, if they smoke regularly now, the start and (last) stopping ages of regular smoking, and the number of cigarettes usually smoked per day during periods when the subject smoked, with categories of 1–10, 11–20, 21–30, 31–40, 41–60, 61–80, and 81 or more. A supplemental questionnaire was mailed to PLCO participants at 6–12 (median 9.3) years from enrollment, asking similar questions about smoking, and additional questions concerning smoking craving, passive smoking exposure, and attempts to quit.
Quantitative Methods
YSQ at baseline for former smokers was calculated by subtracting the age at which regular smoking was last stopped from current age. Pack-years were computed as the product of years of smoking and cigarettes per day (CPD) divided by 20, with years of smoking calculated as either current age (for current smokers) or age at which smoking was last stopped (for former smokers) minus age at which smoking started, and CPD was calculated using the high point of each CPD category range (and 100 CPD for the 81 or more category).
To assess lung cancer risk by YSQ in the context of LDCT screening, we are interested in short term risk. The decision to undergo LDCT screening in a given year should be based on the current risk of lung cancer and not, for example, the risk over the next decade. Because YSQ increases over study time in former smokers, to accurately estimate the short term risk associated with a given YSQ level, subjects’ assigned YSQ values should be changing over study time so that lung cancer incidence in a given study year is related to YSQ levels at that same study year. We therefore employed Cox proportional hazards modeling with YSQ included as a time varying covariate, increasing by one year as study time increased by one year. Sex and age (time-varying) were included as covariates; YSQ was grouped into 5 year categories for analysis.
The supplemental questionnaire data for 30+ pack-year former smokers with YSQ ≤5 at baseline (N = 3576) showed that a non-negligible proportion (13%) relapsed to current smoking at the time of the questionnaire. For 30+ pack-year subjects with baseline YSQ > 5 (N = 12466), the relapse rate on the supplemental questionnaire was low, 1.8% overall and under 4% for each 5-year baseline YSQ category. Therefore, subjects with baseline YSQ ≤ 5 were censored at 3 years from baseline, to minimize contamination of that group with (relapsed) current smokers. Subjects with baseline YSQ > 5 were followed for the full study period.
Never smokers were assumed to continue their never smoking status through all study years. Current smokers, however, could have quit after enrollment, which would change their status to former smoker. Of baseline current smokers with 30+ pack-years who responded to the supplemental questionnaire (N = 5970), 35.4% reported on that questionnaire that they were currently former smokers. Therefore, to insure minimal contamination of the current smoker category, this group was also censored at 3 years from baseline.
To examine possible interactions of the YSQ and lung cancer risk relationship by sex and study arm, we restricted the basic model to former smokers at baseline and utilized a continuous measure of YSQ, along with an interaction term of YSQ by sex or YSQ by study arm.
Among incident lung cancers we examined the relationship of YSQ and histology. The Chi-squared test was used to test for the statistical significance of the association of YSQ (≤15 versus > 15) and histology (with categories of adenocarcinoma, squamous cell carcinoma, other NSCLC and small cell). The YSQ level at the time of cancer diagnosis was used for this analysis.
Results
Of 154899 subjects randomized, 149930 (96.8%) completed the smoking section of the baseline questionnaire. There were 69182 (46.1%) never smokers, 16057 (10.7%) current smokers and 64691 (43.2%) former smokers. For current smokers, 15869 (98.8%) had calculable pack years (based on completing the age started smoking and cigarettes per day questions), and of these, 12243 (77.2%) had 30+ pack years. Among former smokers, 63402 (98.0%) completed the age at which smoking stopped question, enabling calculation of YSQ. Of the 63402, 63,000 (99.4%) had calculable pack years, with 27101 (42.7%) of these having 30+ pack years. Mean follow-up time for the analysis cohort was 11.2 years.
Baseline demographics and smoking history of the analysis cohort.
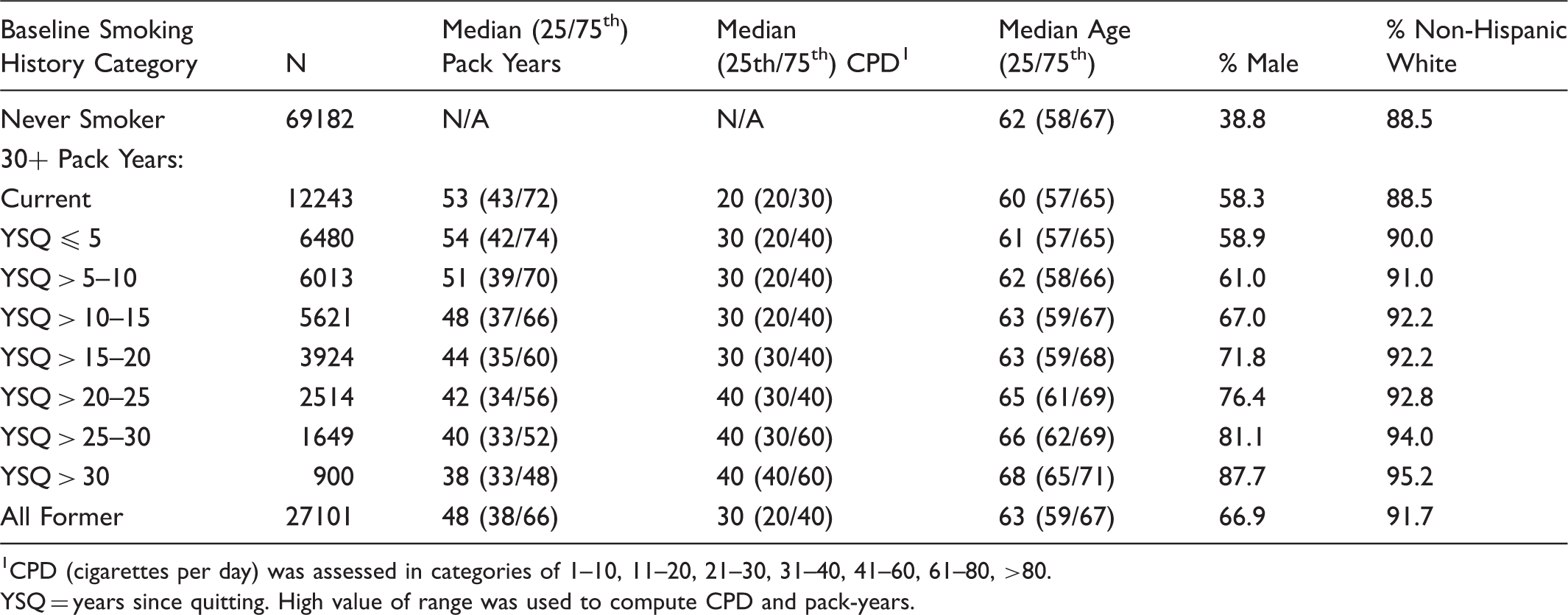
CPD (cigarettes per day) was assessed in categories of 1–10, 11–20, 21–30, 31–40, 41–60, 61–80, >80.
YSQ = years since quitting. High value of range was used to compute CPD and pack-years.
Cox Proportional Hazards Model.
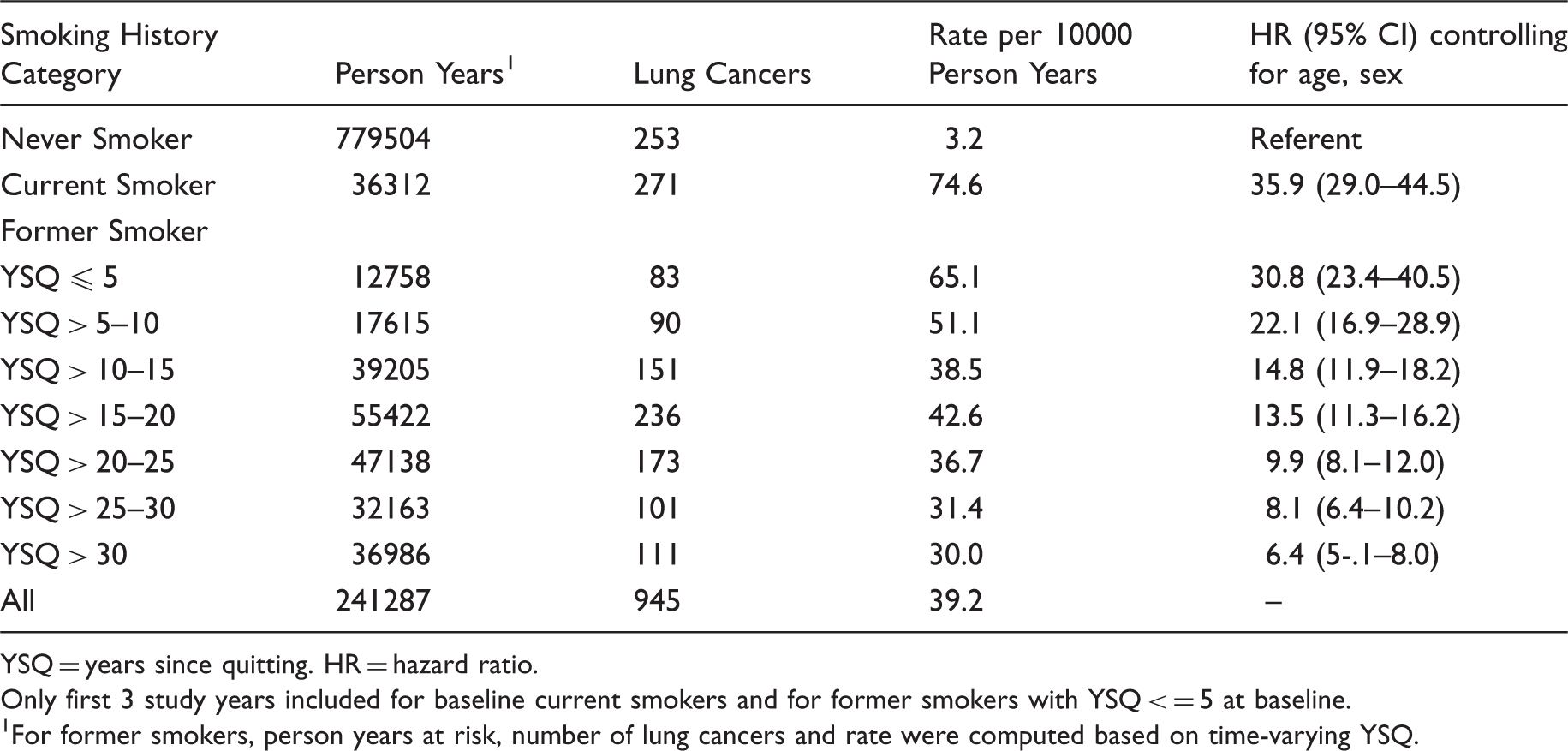
YSQ = years since quitting. HR = hazard ratio.
Only first 3 study years included for baseline current smokers and for former smokers with YSQ < = 5 at baseline.
For former smokers, person years at risk, number of lung cancers and rate were computed based on time-varying YSQ.
Figure 1 displays HRs versus YSQ levels with never smokers as the referent group, as in Table 2, and also with current smokers as the referent group. HRs versus current smokers were 0.41 (95% CI: 0.33–0.51) for YSQ >10–15, 0.38 (95% CI: 0.30–0.47) for YSQ >15–20, 0.27 (95% CI: 0.22–0.35) for YSQ >20–25 and 0.22 (95% CI: 0.17–0.29) for YSQ >25–30.
Hazard ratios of lung cancer risk for various years since quitting (YSQ) levels. Solid and dotted line are for referent group never smokers and current smokers, respectively.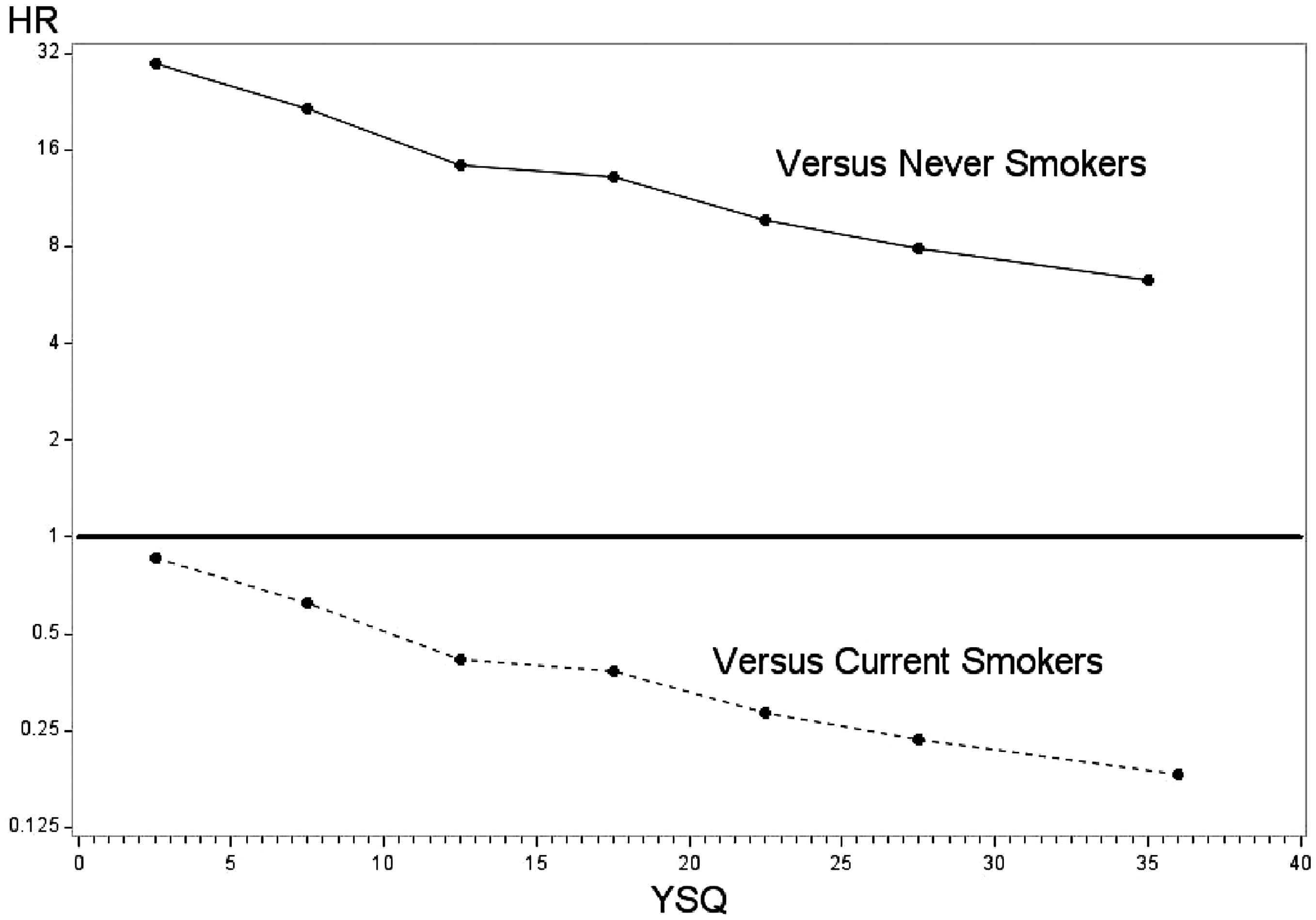
There were no significant interactions of YSQ by sex (p = 0.84) or study arm (p = 0.43).
Lung cancer histology by smoking history.
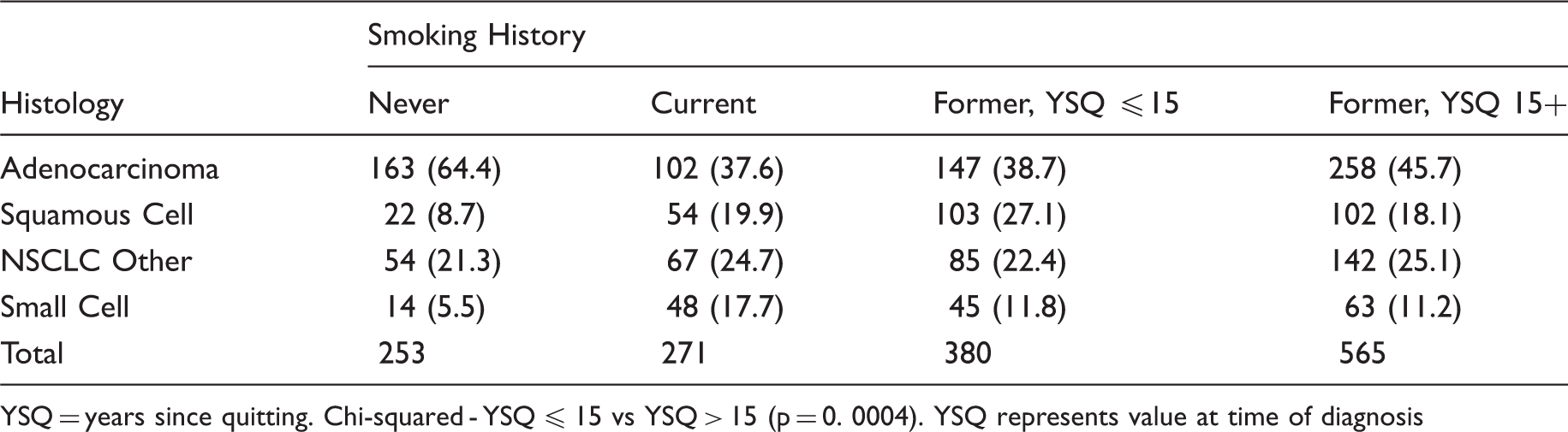
YSQ = years since quitting. Chi-squared - YSQ ≤ 15 vs YSQ > 15 (p = 0. 0004). YSQ represents value at time of diagnosis
Discussion
Our analysis of PLCO trial data in subjects with 30+ pack-years of smoking showed that the decrease in lung cancer risk with YSQ is gradual, with no dramatic drop-off after 15 years since quitting. Even with YSQ > 30, lung cancer risk was still substantially elevated compared with that of never smokers.
Although there is no literature directly addressing the question of risk reduction with YSQ among 30+ pack-year former smokers, several large studies have addressed the more general question of YSQ and lung cancer risk. A 1990 United Kingdom case-control study showed Relative Risks (RRs) for lung cancer incidence compared with current smokers of 0.66, 0.44, and 0.20 for YSQ values of <10, 10–19, and 20–29, respectively in men, and RRs of 0.69 (YSQ < 10) and 0.21 (YSQ 10–19) in women.
5
Halperin et al. used statistical modeling to estimate lung cancer mortality risk for different age and age at quitting groups in the CPS-II cohort.
6
Translating these into YSQ, RRs (for those aged 65) relative to current smokers were 0.56, 0.29, and 0.18 (men) and 0.60, 0.33, and 0.22 (women) for YSQ levels of >5–10, >10–15, and >15–25, respectively. Knoke et al. analyzed CPS-I data and displayed age-standardized lung cancer mortality rates by YSQ among former smokers.
7
Utilizing the group with YSQ < 3 as representing the risk level of current smokers, RRs (age standardized) compared with current smokers were 0.39 (YSQ > 5–10), 0.22 (YSQ > 10–15), 0.15 (YSQ > 15–20), and 0.13 (YSQ > 20–25). To compare these findings with each other, and with those of the current study, RRs (or HRs) for lung cancer risk compared with current smokers are plotted against YSQ (Figure 2). Despite differences in study design, analytic methods, and eligible populations, the studies are generally consistent in how much risk falls off with YSQ.
Relative Risk (RR) or hazard ratio (HR) estimates of lung cancer risk compared with current smokers by YSQ for various studies. Solid line is current (PLCO) study, long- dashed line is Knoke et al study, short-dashed line is Peto et al study, dotted line is Halpern et al. study. For Halperin et al. and Peto et al., the means of the RRs for men and women are plotted. Sizes of dots are proportional to the total number of lung cancer events among former smokers in the study.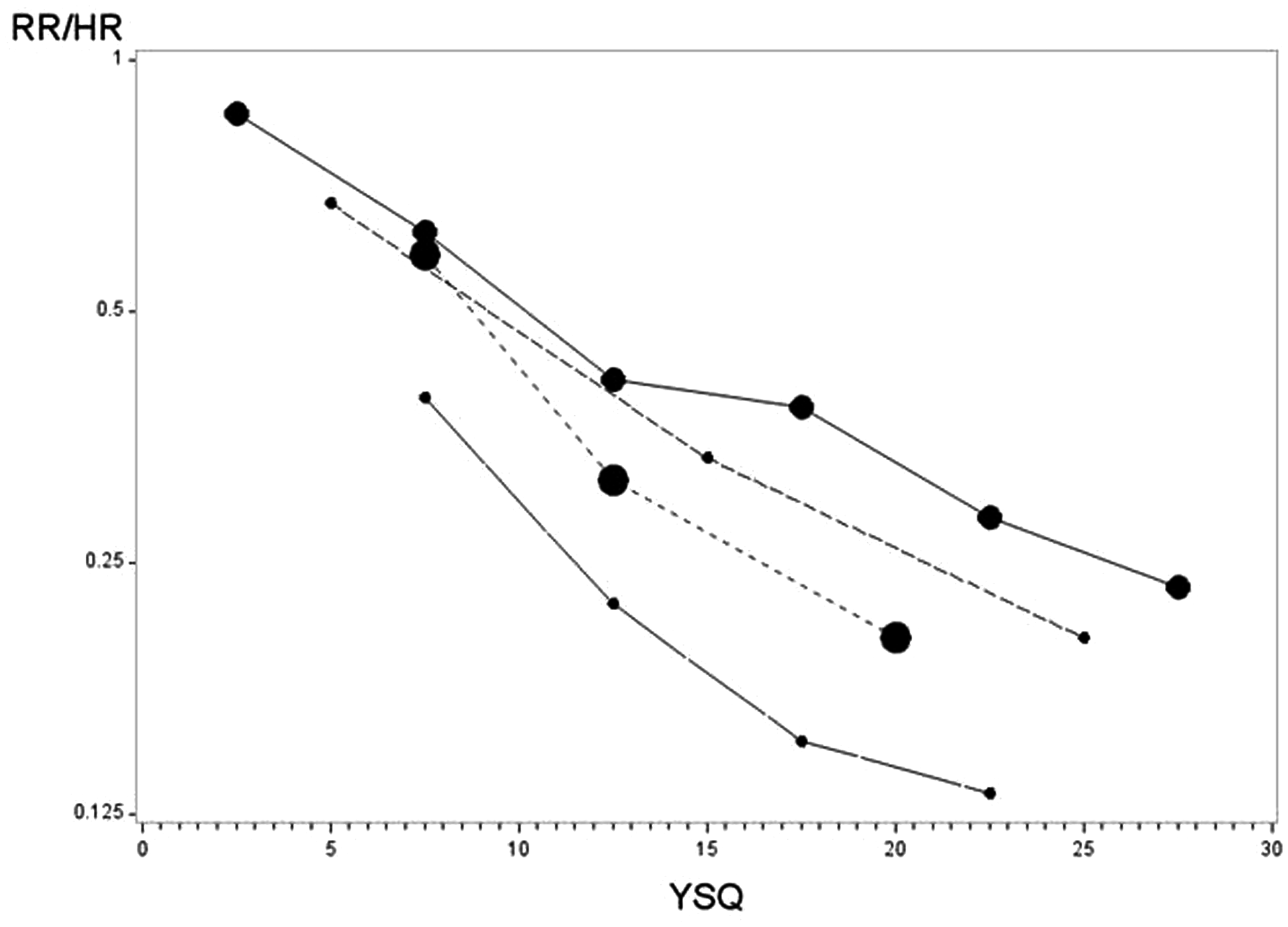
A recent meta-analysis examined 85 studies with data on lung cancer risk in former smokers grouped by YSQ category, as well as in current and never smokers. 8 Using a model in which smoking-related excess lung cancer risk decayed exponentially with YSQ, the authors estimated an average half-life of 9.9 years, which corresponds to an exponential decay parameter of C = 0.07 years–1. Using this value of C, with the observed HR in PLCO of 35.9 for current smokers, and the midpoints of each 5 year YSQ category, the HRs predicted by this model are 15.6, 11.3, 8.2, and 6.1 for YSQ of >10–15, >15–20, >20–25, and >25–30, respectively. This compares with observed HRs of 14.8, 13.5, 9.9, and 8.1, respectively, for these YSQ categories. For YSQ > 15, the decrease in risk is close to that predicted by the model, but slightly less steep.
In our analysis, limited to those with 30+ pack-years, median pack-years were similar for current (53) versus former (48) smokers, and the decrease in median pack-years from current smokers to YSQ > 30 was only 28% (53 versus 38). Cigarettes per day were higher in former smokers (median = 30) than in current smokers (median = 20). In contrast, for all of PLCO, not limited by a minimum pack-years, the differential was much greater, with medians of 46 for current smokers, 24 for former smokers overall, and 7 for former smokers with YSQ > 30 (85% decrease from current smokers); current and former smokers both had a median of 20 cigarettes per day. Therefore, for many of the studies cited above, pack-years were probably substantially lower for long-term former smokers than for current smokers, which would tend to augment the rate of decrease in risk observed with YSQ.
Two primary lines of reasoning underlie the YSQ limit recommendations. The first is that, below a certain level of lung cancer risk, the harms of LDCT screening may outweigh the benefits, and relatedly, that LDCT screening is not cost effective below a certain level of risk. Implied in this reasoning is that for YSQ > 15, lung cancer risk may drop below this required level. None of the analyses of the benefits to harms tradeoff, and of the cost-effectiveness of LDCT, has specifically examined these metrics with respect to the YSQ cutoff.1,11,12 Because these types of analyses are imprecise, and may include subjective judgments or rely on models that incorporate numerous untestable assumptions, it would be difficult to conclusively determine a specific optimal YSQ cutoff above which LDCT screening is reasonable and below which it should not be recommended. Although the 15 year limit may be reasonable, other limits may also be valid. Further, within some range of YSQ, personal patient preferences may determine screening decisions. The choice of the 15 year YSQ limit in the NLST could not be based on an analysis of the benefits to harms tradeoff of LDCT screening, because the magnitude of the LDCT benefit was unknown when planning the trial. The requirement reflected a compromise on having an efficient trial (maximizing endpoint events per enrolled subject) that would be representative of risk groups that might benefit from LDCT screening. Within a reasonable set of parameters, the decision was to some extent arbitrary. The pilot study for NLST used a 10 year cutoff for YSQ, as does the ongoing European NELSON LDCT screening trial.13,14
The other reasoning is that it is undesirable to extrapolate beyond the population represented by the NLST criteria, as this was the only study to directly show LDCT benefit. This is a generally reasonable principle, but for a cancer screening trial, an argument can be made for at least limited extrapolation beyond some trial parameters. The effectiveness of LDCT screening, assessed through percentage reduction in lung cancer mortality, will be principally a function of the types of lung cancers (defined by histology, molecular sub-types, etc) presenting in the population, and the overall health status of the population, including ability to undergo and withstand curative lung resection. In the current study, although exploratory analyses revealed some potential differences, the overall histologic pattern was generally similar across YSQ categories, and the histology distribution for those with YSQ > 15 was actually more similar to that of current than to that of never smokers. Data on molecular sub-types are not available, however, it is unlikely that small changes in YSQ would have a large effect on molecular sub-types. Subjects with increased YSQ would be as, or more, likely to be able to withstand surgical resection. Reduction in risk of heart disease and all-cause mortality after sustained smoking cessation is well-established.
There are arguments in support of the 15 year limit. As seen in some other screening programmes (eg. prostate-specific antigen screening for prostate cancer) and medical interventions, there is a danger that factors such as the fee for services medical landscape prevalent in the United States, and pressures from patient interest groups, promote use of an intervention among groups clearly unlikely to receive net benefit from it. If the 15 year limit were relaxed, then there could also be pressures for other limits, such as the 30+ pack-year requirement, to be relaxed, with an end result of LDCT screening occurring in relatively low-risk populations.
It is also important to consider how much of a difference removing the 15 year requirement might make. An analysis of population data showed that the recommended LDCT screening guidelines of 30+ pack-years, current smoking or having quit within 15 years, and age 55 to 74 would cover 6.2% of the United States population over age 40. Removing the YSQ limitation would increase this by approximately 3 million persons, to 8.3%. 15 Based on models of smoking history and lung cancer risk, the estimated proportion of subjects with incident lung cancer who would be screened would correspondingly increase from 26.7% to 32.5%.
In conclusion, in former smokers with 30+ pack-years, lung cancer risk decreases gradually with YSQ. The 15 year YSQ limit for screening eligibility appears reasonable, but other YSQ eligibility ranges may also be supportable.
The data set for this analysis can be requested via: https://biometry.nci.nih.gov/cdas.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.