
Abstract
Objective
To examine uptake in the first six pilot centres of the English Bowel Scope Screening (BSS) programme, which began in early 2013 and invites adults aged 55 for a one off Flexible Sigmoidoscopy.
Methods
Between March 2013 and May 2014 the six pilot centres sent 21,187 invitations. Using multivariate logistic regression analysis, we examined variation in uptake by gender, socioeconomic deprivation (using the Index of Multiple Deprivation), area-based ethnic diversity (proportion of non-white residents), screening centre, and appointment time (routine: daytime vs out-of-hours: evening/weekend).
Results
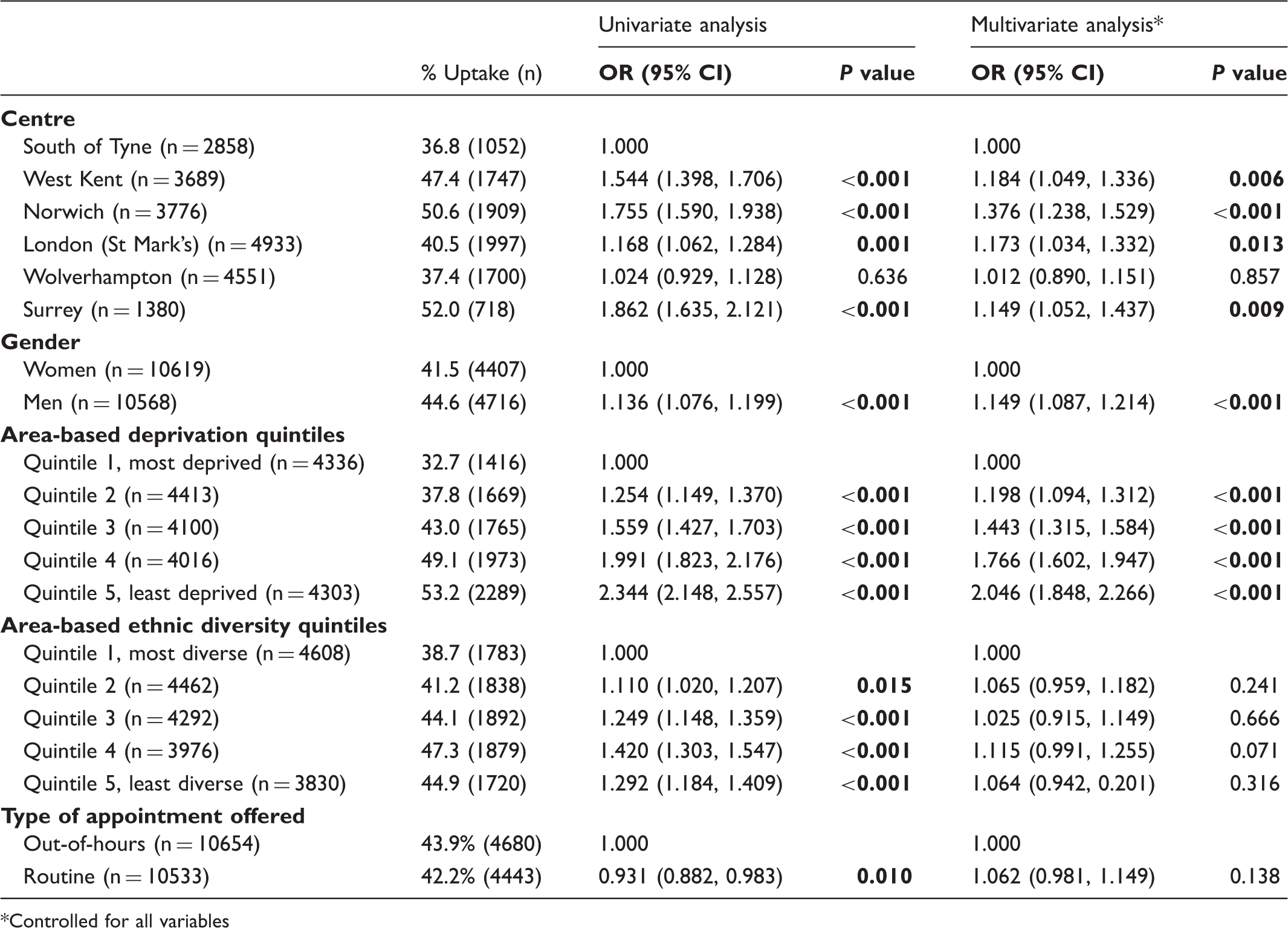
Uptake was 43.1%. Men were more likely to attend than women (45% vs 42%; OR 1.136, 95% CI 1.076, 1.199, p < 0.001). Combining data across centres, there was a socioeconomic gradient in uptake, ranging from 33% in the most deprived to 53% in the least deprived quintile. Areas with the highest level of ethnic diversity also had lower uptake (39%) than other areas (41–47%) (all p < 0.02), but there was no gradient. Individuals offered a routine appointment were less likely to attend than those offered an out-of-hours appointment (42% vs. 44%; OR 0.931, 95% CI 0.882, 0.983, p = 0.01). Multivariate analyses confirmed independent effects of deprivation, gender, and centre, but not of ethnic diversity or appointment time.
Conclusion
Early indications of uptake are encouraging. Future efforts should focus on increasing public awareness of the programme and reducing socioeconomic inequalities.
Keywords
Introduction
Colorectal cancer (CRC) is the third most frequently diagnosed cancer and the fourth leading cause of cancer deaths (700,000 per year) worldwide1,2 and the second most common cause of cancer death in the UK. 3 In 2006, the National Health Service (NHS) set up the Bowel Cancer Screening Programme (BCSP) in England. The programme is based on biennial guaiac-based Faecal Occult Blood testing (gFOBt), which is now offered to all adults aged 60-74. Trial data on gFOBt show a clear benefit in CRC mortality, but no evidence of a reduction in incidence, 4 so the test is excellent in terms of earlier diagnosis, but does not contribute to prevention.
In contrast, endoscopic screening, which can detect and remove polyps, has been shown to reduce CRC incidence as well as mortality. In the UK Flexible Sigmoidoscopy (FS) Trial, a single FS exam between ages 55 and 64 reduced incidence by 23% and 33%, and mortality by 31% and 43% in the total and screened populations respectively. 5 A subsequent meta-analysis concluded that offering FS screening can reduce CRC incidence by around 18%, and mortality by 28%, increasing to 32% and 50% respectively when screening is adhered to, supporting its potential use in CRC prevention.6,7 A more recent population-based trial from Norway provided further evidence of how FS can help significantly reduce CRC incidence and mortality with an 11 year follow-up. 8
The English BCSP started the national roll-out of the Bowel Scope Screening (BSS) programme, offering a one-off FS to everyone aged 55, in March 2013. A phased roll-out to ensure workforce capacity is in progress, which began with six screening centres (South of Tyne, West Kent, Norwich and Norfolk, London - St Mark’s, Wolverhampton, and Surrey). The BSS programme is expected to be rolled out across all centres by 2016 (see Figure 1) with full population coverage from 2018.
9
Flowchart of proposed national roll-out of centres offering Bowel Scope screening.
All screening is dependent on high uptake, but wherever CRC screening has been implemented, and whatever the modality, it has always underperformed compared with breast or cervical screening. In the gFOBt programme, uptake of the first 2.6 million invitations was 54% overall, varying from less than 35% in the most socioeconomically deprived quintile of areas in England to more than 60% in the least deprived. 10 A meta-analysis of uptake data from 14 randomized controlled trials (RCTs) of BSS indicated that uptake rates are likely to be lower than those seen for gFOBt. 11 One Dutch study found uptake of only 32.4%, compared with 49.5% for gFOBt, 12 though other studies in the meta-analysis found higher uptake, e.g. an Italian RCT with uptake of 58.3%. 13 Methodological differences in the meta-analysis trials, for example, with some recruiting from the general population but others (including the UK FS trial) inviting individuals who had already indicated interest in screening, make it difficult to extrapolate to likely uptake in the UK national BSS programme. A recent population-based RCT in Norway found BSS uptake of 63%, but again, direct comparison with the UK programme is difficult. 8
Among small-scale evaluations of uptake, two London-based feasibility studies of nurse-led BSS had uptake rates of 45% and 55%;14,15 however, both were delivered through a single screening centre renowned for endoscopic excellence, and serving a population who may have been familiar with BSS screening through the centre’s involvement in the UK FS trial.14,15 In 2011, a pathfinder study of BSS in three centres in England reported uptake of only 29%, 16 however, none of these sites used reminder letters for non-responders. Projection to uptake in the national programme is limited.
Similarly, there is uncertainty regarding gender differences in uptake of FS screening. Women are more likely to return completed gFOBt kits,10,17,18 but the opposite has been found for endoscopic screening. While the London-based feasibility studies indicated either similar or higher uptake for women,14,15 the finding was contrary to the UK FS trial data19,20 and other BSS uptake reports. 12
Our study is the first multi-centre examination of uptake in an organized BSS programme. The primary objective was to provide an indication of overall uptake of BSS and examine differences by gender, socioeconomic status, and ethnicity. A secondary aim was to compare uptake across the six participating centres, and assess the extent to which differences could be attributed to the demographic composition of the catchment populations. Previous research has indicated that flexibility in appointment days and/or times can influence attendance at various health-related appointments.21,22 We therefore also explored the extent to which the six centres offered out-of-hours appointments, and whether this was associated with increased uptake.
Methods
Participants and setting
The study population was all men and women who turned 55 during the study period (March 2013 – May 2014) and were registered at a general practice linked with the six screening centres (South of Tyne [Queen Elizabeth and South Tyneside]; West Kent [West Kent and Medway]; Norwich; London [St Marks]; Wolverhampton, Surrey [Guildford]). Ethical approval for this study was not required.
Invitation process
The English BSS programme sends a pre-invitation letter to all eligible individuals, informing them about the forthcoming BSS opportunity. A screening invitation letter, offering a dated and timed screening appointment with approximately six weeks’ notice, is sent 8-10 days later. During the invitation period covered in this study, five of the six centres offered both weekday routine and evening/weekend (termed out-of-hours) appointments; one (Wolverhampton) offered only weekday routine appointments. Invitees are asked either to return a slip attached to their invitation letter to confirm or decline attendance, or to call the centre to confirm, rearrange, or cancel the appointment. Enclosed with the screening invitation is an information booklet about the programme and a freepost return envelope for the confirmation slip. After two weeks, an appointment reminder is sent to people who have not responded. For those who confirm the appointment, a confirmation letter is sent along with a consent form, which is followed shortly by a mailed enema with instructions for self-administration on the day of the appointment.
Measures
The data used in this analysis were extracted, modified, and anonymized from data routinely collected within the BCSP.
Individual-level demographics. The gender of each invitee was added to the study dataset.
Area-level deprivation. The postcode sector of each invitee was converted to a score for area-based socioeconomic deprivation and added to the study dataset. This score was derived using the 2010 Index of Multiple Deprivation (IMD), 23 which uses census-derived indicators of income, education, employment, living environment, health and disability, barriers to housing and services, and crime, at small-area level to generate a scale from 0 (least deprived) to 80 (most deprived). For analysis, the IMD scores were categorized into quintiles of the national distribution. 24
Area-level ethnic diversity. An area-level index of ethnic diversity was produced using Census 2010 data based on the proportion of ‘non-white’ residents (all self-reported ethnic groups other than ‘White British’, ‘White Irish’, and ‘White other’) in each postcode sector. For analysis, area-based ethnic diversity was grouped into quintiles based on national census information.
Appointment slot offered. The appointment date/time offered in the initial invitation letter was documented for each person. For analysis, appointments offered on weekday mornings and afternoons were categorized as ‘routine’, while appointments offered on weekday evenings (after 5 pm) and Saturdays were categorized as ‘out-of-hours’.
Uptake. The date of attendance for individuals who attended was included in the programme database. Individuals with an entry for ‘date attended’ were classified as attended, and those with no date were classified as ‘Did not attend’ (DNA).
Statistical analysis
Demographic and service-level variation in screening uptake.
Controlled for all variables
Results
Over the study period, 21,187 screening invitations were issued across the six centres (see Appendix Table 1) with an overall uptake rate of 43.1% (N = 9,123). Differences by gender, deprivation, ethnic diversity, centre, and type of appointment offered are shown in Table 1. Uptake varied among the six centres (36.8% - 52.0%); four had uptake significantly higher than the centre with the lowest uptake (South of Tyne). Men were more likely to attend BSS than women (44.6% vs 41.5%).
Proportion of appointment times offered, attended and re-scheduled.

Of the 21,187 appointments offered, 49.7% (n = 10,533) were routine appointments (weekday mornings and afternoons) and 50.3% (n = 10,654) were ‘out-of-hours’ (weekday evenings and Saturdays mornings and afternoons). The proportion of people who went on to attend an appointment and have the BSS procedure was significantly lower in the group originally offered a ‘routine’ appointment compared with those originally offered an ‘out-of-hours’ appointment (42.2% vs. 43.9%) (see Table 1). Attendance at the exact appointment time and day offered was 16.5% and 19.8% for ‘routine’ and ‘out-of-hours’ appointments respectively (see Table 2).
A multivariate analysis confirmed that area-level deprivation remained the strongest independent predictor of uptake (OR for quintile 1 vs quintile 5 = 2.046, 95% CI 1.848, 2.266) (see Table 1). Screening centre was also predictive of uptake. Four centres achieved uptake levels significantly higher (15% to 38% higher) than the centre with the lowest uptake (South of Tyne). Gender also remained a significant predictor (OR = 1.149, 95% confidence interval (CI) 1.087, 1.214). There was no independent effect of area-based ethnic diversity or the type of appointment offered.
Discussion
England is the first country to initiate a nationwide organized, population-based CRC programme involving flexible sigmoidoscopy examinations. Since the start of the programme in 2013, the six pilot centres have invited 21,187 people for BSS, of whom 43% attended. This was considerably higher than in a recent Dutch trial comparing different screening modalities, and the recent English pathfinder study.12,16 However, uptake was lower than that reported for the two single-centre feasibility studies (45% and 55%) in the London area,14,15 and the early uptake for gFOBt screening (54%). 10
As documented in previous studies, uptake was strongly socioeconomically graded. Stratifying by quintile of area-level deprivation based on home address, uptake was almost twice as high in the least compared with most deprived areas (Table 1), and a similar gradient in uptake was seen in all six centres (see Appendix Table 2). Given the potential benefits of BSS in reducing CRC incidence and mortality, such striking inequalities are a major concern. If strategies are not implemented to reduce the gradient, it is likely that inequalities in CRC incidence will be created and inequalities in CRC mortality will be exacerbated. 10
Similar to other studies investigating uptake of FS screening we found that women had lower uptake than men.12,19 This is surprising given that women are more likely to participate in CRC screening using the guaiac based FOBT kit, 10 especially in the first invitation round. 18 The reasons why this difference reverses for endoscopic screening tests is not well understood. Perhaps more importantly, very little is known about why there is an almost two-fold difference between uptake of BSS (41.5%) and coverage of breast and cervical screening (75.9 and 77.8%, respectively).25,26 A better understanding of why women accept one invitation and decline the other could help to highlight the barriers to CRC screening.
There were significant differences in uptake rates by centre after adjusting for differences in gender, socioeconomic status, and area-based ethnic diversity. Furthermore, centre-specific differences were not attenuated by adding a potentially modifiable service-related variable (use of ‘out-of-hours’ appointments). While offering out-of-hours appointments was associated with slightly higher uptake in univariate analyses, the multivariate analysis suggested that it was not the offer of out-of-hours appointments per se, but the fact that they were preferentially offered to people who would have been more likely to attend on the basis of their demographic background (gender, area-based deprivation, and centre). Importantly, there was large variation between centres in the type of appointments offered. While the difference between routine and out-of-hours appointments was small, it might be advisable for individual centres to offer a broader range of appointments (at least to begin with) to monitor whether there is a preference for specific appointment times or days among their target population.
It is important to acknowledge that our analysis was restricted to the first six pilot centres, which covered only a fraction of the total population that will be eligible for BSS. The six pilot centres included in this analysis covered a population with a level of deprivation comparable with the rest of England (average IMD 2010 score 21.6 vs 21.7 respectively). In contrast, our analytic sample contained a higher proportion of ethnically diverse individuals compared with the general population (20.8% vs 12.9%). Given the higher propensity of invitees from ethnically diverse areas, it is probable that uptake might increase slightly once the programme invites the entire eligible population.
The finding that all our variables together have relatively low predictive power highlights the fact that there must be other important factors that could be targeted to improve uptake. These could include other service-related variables such as offering single-sex lists (i.e. endoscopy sessions inviting men or women only) and a choice of practitioner gender, and individual-level psychosocial variables (e.g. test-specific beliefs and attitudes, beliefs about CRC). Larger-scale data analysis will enable us to investigate other sources of centre differences, such as geographical variables, while a mixture of prospective and retrospective interview studies and surveys will identify psychosocial determinants of uptake. Recent projections for the national programme in England suggest that adding once-only FS to the NHS BCSP will prevent an additional 2000 CRC deaths and 10,000 CRC cases in England by mid-2030. Importantly, this projection was based on 50% uptake of BSS and 57% uptake of gFOBT, highlighting the potential benefits of increasing BSS uptake. 9 Incentive to better understand predictors of BSS uptake and to incorporate this knowledge into the development of interventions to increase uptake is therefore high.
Because of the gradual roll-out of the programme there are currently no campaigns to encourage public awareness of BSS, unlike with other screening programmes. However, in light of the substantial health benefits of BSS screening, it is imperative that messages and communication channels are established to inform the public about BSS, with a key objective being to narrow inequalities, along with improving overall uptake.
Conclusion
The UK is a pioneer in delivery of organized endoscopic screening. Programme coverage is already good for a test that is intrusive and unfamiliar in the UK. Nevertheless, more than half of those invited do not attend, and this rises to two thirds for screening centres serving a predominantly socioeconomically deprived area. The huge health gain associated with preventing a common cancer, that carries such high morbidity and mortality, makes a strong case for investment in strategies to both increase uptake and reduce social inequalities.
Footnotes
Acknowledgements
We acknowledge our grant collaborators, Carly Porter, Hayley Miller, Jacqueline Underwood, and Sarah Marshall for their support with this research.
Conflict of Interest
None to declare.
Funding
This work was supported by the Cancer Research UK [grant number C27064/A17326] to CVW.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.