
Abstract
Objective
In the Czech Republic, over 97% of all pregnant women undergo some type of antenatal screening for Down’s syndrome. In about 95% of cases with a confirmed fetal chromosomal abnormality, the pregnancy is terminated. The most commonly used test is the first trimester combined test. We investigated the impact of implementing an integrated sequential test to improve the detection of Down’s syndrome pregnancies.
Methods
Data on the incidence of congenital defects, number of births, and affected pregnancies terminated are recorded in the National Registry of Congenital Anomalies. Anonymous data on cases of Down’s syndrome diagnosed antenatally or postnatally between 2010 and 2015 in one of the large antenatal care centers were analyzed.
Results
There were 600 diagnoses of Down’s syndrome (5.7 per 1000 births), 90% of which were made antenatally. Of antenatally detected cases, 80% were indicated for diagnostic procedure by multimarker screening results. In the multimarker screen positive group, 75% cases were first trimester positive and 25% second trimester positive (most of these had positive integrated test results). Among Down’s syndrome cases indicated for antenatal diagnosis by multimarker screening results 6.25% (n = 26) were first trimester negative, and became positive after integration with the second trimester screening results.
Conclusions
Results from five major Czech antenatal centers confirm that an integrated sequential test would detect 80–85% of Down’s syndrome fetuses in the first trimester and at least an extra 5–10% of Down’s syndrome pregnancies in the second trimester of pregnancy. These are important data that should be considered in implementing the national antenatal screening program.
Introduction
Multiple antenatal screening strategies exist, with different false positive rates (FPR) and detection rates (DR).1,2 In the Czech Republic, screening for Down’s syndrome (DS) in the second trimester of pregnancy was introduced in the 1980s, but the most commonly used test here is now the first trimester combined test. This test combines biochemical test results for pregnancy associated plasma A (PAPP-A) and free beta-human chorionic gonadotrophin (free β-hCG) with ultrasound fetal nuchal translucency (NT) and maternal age, and has a DR of 80–85%, and an FPR of about 5%. Second trimester screening is performed by measuring three (in some systems four) maternal serum biochemical markers, alphafetoprotein (AFP), hCG, and free estriol (and in some systems inhibin A). This screening method has a DR of about 65–70%, and an FPR of about 6–7%. As ultrasound and non-invasive tests are now widely utilized, performing a separate screening test in the second trimester may seem almost obsolete, but it is crucial to maintain both for women who present late for screening, and as part of the integrated test procedure. 3
Although the use of a combined test in the first trimester of pregnancy currently predominates, the use of the integrated test is also considerable. The sequential integrated test is a modification of the integrated test, in which a high risk pregnancy can be identified through the PAPP-A, free β-hCG, or NT measurement in the first trimester, thus not losing the advantages of an early assessment. NT is given greatest weight in the algorithm for calculating the risk. 4 If the result of the combined test in the first trimester indicates low risk, the woman then continues with biochemical screening in the second trimester. This procedure has a DR of up to 95%, with an FPR of 5%. 5 Many European countries only use a first trimester combined test, whereas in the USA the integrated test is increasingly being used. 6 In cases where no accredited measurement of NT is available, a serum integrated test could be used, testing only the biochemical parameters in both trimesters. 7 Screen positive women are offered an invasive diagnostic procedure, either amniocentesis or chorionic villus sampling, with subsequent karyotyping. 8
This paper aims to investigate the impact of implementing an integrated sequential test, making it possible to find at least an extra 5–10% 9 of DS pregnancies, which had passed through the combined test in the first trimester as negative. Several such cases from five major Czech antenatal centers are documented here.
Methods
In the Czech Republic there are more than 40 DS screening laboratories, all of which participate twice yearly in quality assessment, where the results of different biochemical parameters are evaluated, and the ultimate risks in model cases are assessed. The Register of screening DS laboratories, administered by the Department of Clinical Biochemistry and Laboratory Medicine of the First Faculty of Medicine, Charles University in Prague (http://ulbld.lf1.cuni.cz/), records number of tests performed, the algorithm used to determine the risks, and the immunoassay methods for all laboratories. The laboratories are governed by regularly updated national expert guidance on the implementation of screening for congenital defects. Data on the incidence of congenital defects, number of births, and cases of affected pregnancies terminated are recorded in the National Registry of Congenital Anomalies of the Czech Republic (www.vrozene-vady.cz/). This National Registry is the cooperation center for both the International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR) and EUROCAT (European Surveillance of Congenital Anomalies) organizations.
Biochemical examination solely in the second trimester of pregnancy is only rarely performed. Invasive testing is recommended for women at high risk, while for women of intermediate risk a non-invasive prenatal test (NIPT) may be recommended. Cases where the outcome of the first-trimester test was negative but a second-trimester positive test revealed a fetus with DS have been collected since 2010. There are data available from five Czech antenatal centers, annually investigating about a quarter of all pregnant women in the Czech Republic. The information about the screening tests used, cut off, software, as well as the populations of pregnant women can be found in Table 1.
Prenatal screening centers—used tests, software, cut off and age distribution of tested pregnant population. The center number corresponds to the affiliations.
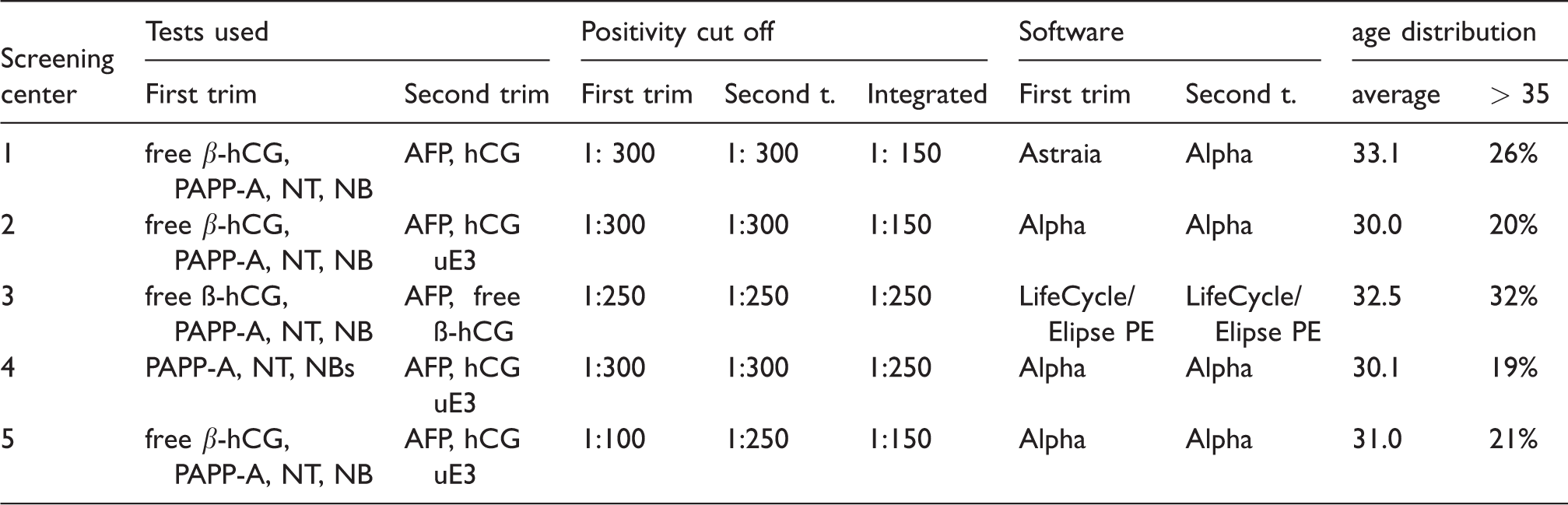
β-hCG: beta-human chorionic gonadotrophin; PAPP-A: pregnancy associated plasma A; NT: nuchal translucency; AFP: alphafetoprotein; uE3: unconjugated estriol. The center number corresponds to the affiliations.
Results
We here present results from the Czech National Center for the Detection of Congenital Defects and from the records of the Register of DS screening laboratories. The total number of second trimester tests alone declined between 2009 and 2016 from 64,400 to 17,600 (a drop of 72.6%), the number of tests performed in the first trimester has increased from 24,400 to 40,000 (an increase of 63.4%), and the number of integrated tests has been stable on a long-term basis (at about 30,000, see Figure 1).
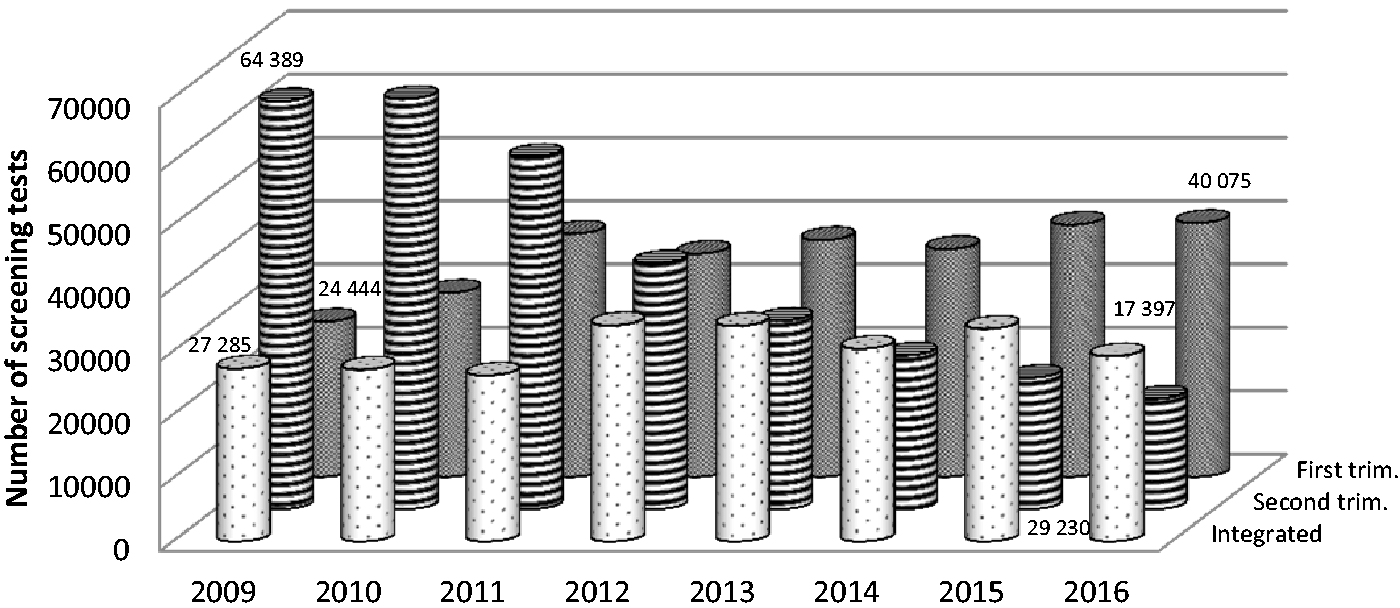
The number the second trimester tests has declined in last 8 years, the number of combined tests has increased and the number of integrated tests remains almost the same.
Recent European statistics show that around 82–85% of pregnancies with DS are terminated. In the Czech Republic 95–98% of all antenatally diagnosed DS pregnancies are terminated. During 2015, 110,800 children were born in the Czech Republic. In total, 271 DS pregnancies were antenatally diagnosed, 264 (97.4%) of which were terminated. A further 36 children with DS were born without any defects in pregnancy having been detected.
The collected data suggest that fetal DS detection is being made increasingly earlier in pregnancy. The average DS diagnosis was made at 20.3 weeks gestation in 1994, but 14.5 weeks in 2015. Figure 2 shows an overview of diagnosed and terminated cases of DS since 1994. Second trimester screening in the mid 1990’s resulted in a rise in the detection of fetuses with DS, and a further increase was seen after introduction of the combined test (2005). The average age of mothers at the birth of their first child has increased from 22.9 in 1994 to 28.2 in 2015.
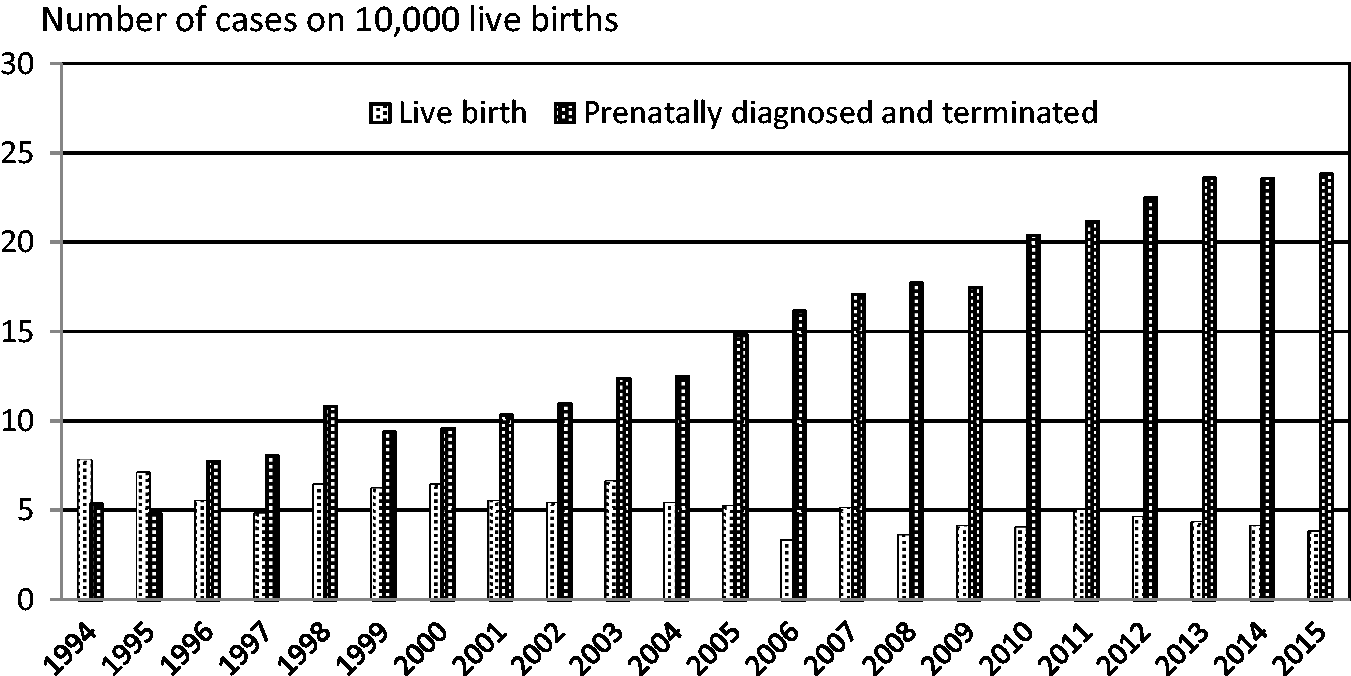
The number of live birth and terminated cases of DS 1994–2015 calculated on 10,000 live births.
In recent years about 80% of all DS cases have been detected by screening, about another 15% using only ultrasound, and the last 5% of diagnostic procedures were recommended because of age or for other reasons. Positive findings based on a screening test amount to 75% in the first trimester, and 25% on the basis of results obtained in the second trimester. We have gathered data that show that biochemical testing in the second trimester leads to the discovery of an important percentage of cases.
Results from several antenatal centers confirm that the sequential integrated test detects 80–85% of DS fetuses in the first trimester, and another 5–10% of cases in the second trimester of pregnancy. The positivity of the individual tests varies slightly with regard to the age of the pregnant women, but is generally about 3% for the combined test, about 5% for the second-term test, and 2% for the integrated test.
Sequential serum integrated test
One of the large antenatal care centers (Center for Medical Genetics, Ceske Budejovice) which performs DS screening for 97% of the population of South Bohemia (about, 8000 women per year) uses both an integrated sequential test and an integrated sequential serum test. PAPP-A testing is provided for all pregnant women at 10 weeks gestation, and women with PAPP-A below 0.35 multiplies of median (MoM) (around 2–3%) are invited for NT measurement, with other minority DS markers being measured by ultrasound. For all other pregnancies, tests of biochemical parameters are carried out in the second trimester of pregnancy (AFP, hCG, and unconjugated estriol (uE3)). The assessment of results from both trimesters allows for a high DR for fetuses affected by DS as well as other chromosomal aberrations. The DR of this type of antenatal screening has been around 95% for some time. In 2007–2015, over 68,000 pregnant women were examined at the center, with 136 fetuses with DS diagnosed antenatally, and women with screen-negative results giving birth to seven children with DS. The overall incidence of DS in an unselected population (1:500) corresponds to the findings published in the EUROCAT study. 10
Sequential integrated test
Another antenatal diagnosis center (GENNET Center for genetics and fetal medicine Prague, Czech Republic), annually processes at least 15,000 screening results, and has diagnosed 141 fetuses with DS in the last five years. This center often investigates pregnancies from smaller centers to resolve positive screening results. In 105 cases, DS has been diagnosed on the basis of a positive combined first trimester test. A total of 29 fetuses with DS (20%) were diagnosed in women who did not have the results of the first trimester combined test, and in another seven cases there was a positive integrated test with a negative combined test in the first trimester. There were 6.25% of DS cases that would not have been detected had the test in the second trimester not been performed, and had the overall risk been determined by the sequential integrated test.
DS with a negative combined test
We summarized the information from some other Czech laboratories of DS cases only detected by a sequential integrated test, where women had a negative combined test (see Table 2). These results confirm the statistical significance of the NT measurement, which is of considerable importance in the risk calculation algorithm. The determination of biochemical markers in the second trimester of pregnancy allows for the detection of approximately a further 5–10% (9) of fetuses with DS.
Examples of Down syndrome fetuses with positive results of sequential integrated screening in case of a negative combined test. The identified risks are highlighted.
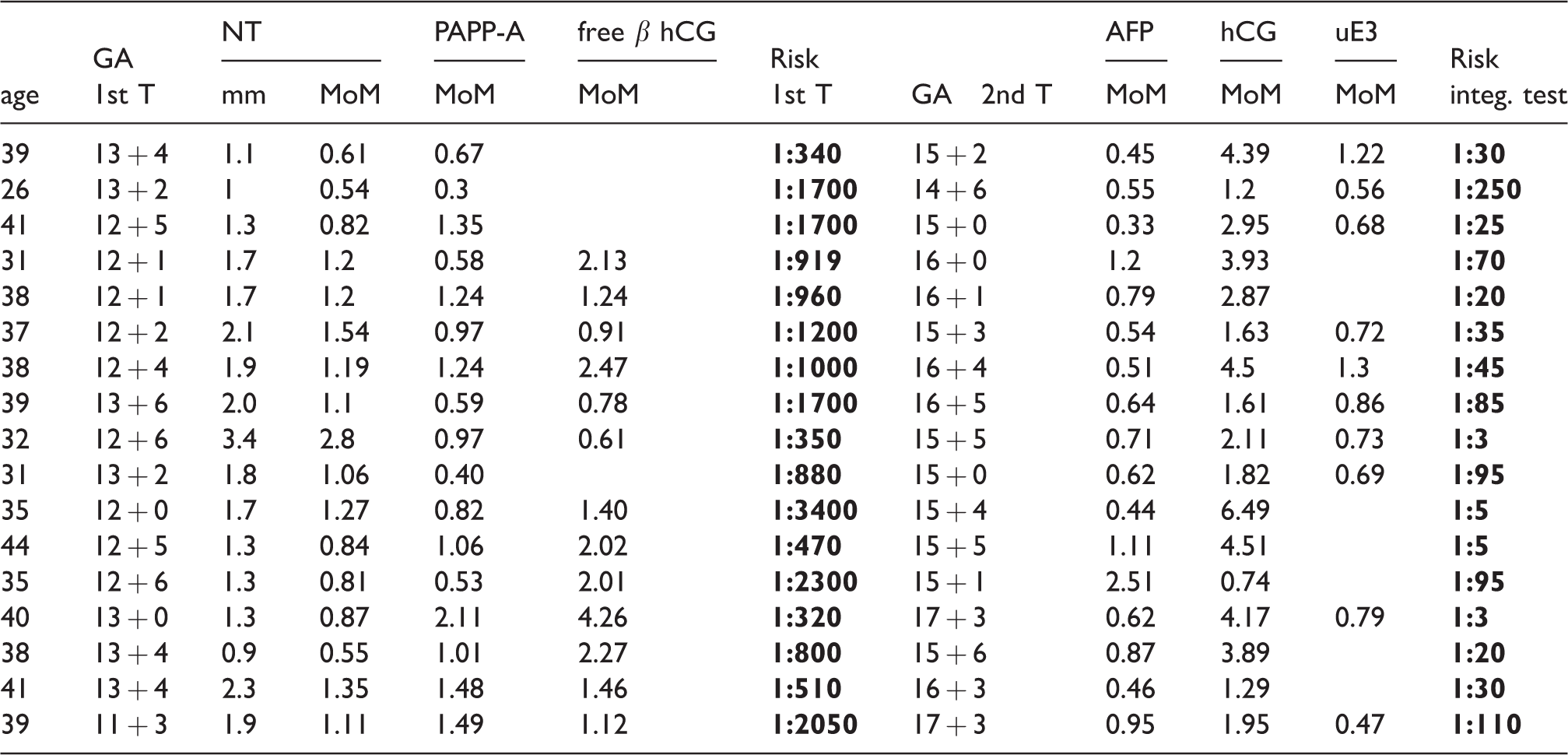
GA: gestation age; MoM: multiplies of median; AFP: alphafetoprotein; uE3: unconjugated estriol; β-hCG: beta-human chorionic gonadotrophin; PAPP-A: pregnancy associated plasma A; NT: nuchal translucency.
Discussion
The number of antenatally diagnosed and terminated pregnancies, along with the number of live births with DS, has doubled over the last 20 years in the Czech Republic. This may be due to the previously mentioned increased age of the mothers (by 5.3 years). In addition, due to the increased use of the combined test, the gestational age at which the diagnosis of DS in the fetus is determined has been reduced (by almost 6 weeks). In about 30% of cases, fetuses affected by DS ended in a spontaneous miscarriage between the first and second trimester of pregnancy. 11 An investigation of the chromosomal defects in an aborted fetus is usually not performed. The increase in the occurrence of DS (Figure 2) is primarily evident in the group of terminated pregnancies. It can be assumed that an examination in the first trimester will reveal a positive result, and offer the termination of pregnancy, which even without intervention would often result in a spontaneous abortion. After the second trimester of pregnancy there are no such recorded spontaneous losses, and so the data on the efficiency of the screenings carried out in the first and second trimesters are not fully comparable.
In about 80% of cases using the combined test, ultrasound, or sequence variant, DS has been detected in the first trimester. When collecting data and evaluating the effectiveness of screening tests, it is difficult to distinguish whether the test is second trimester screening or an integrated test sequence. Similarly, it is difficult to distinguish whether this is the combined test alone, or whether it is the first part of an integrated sequential test. The integrated test in the Czech Republic has been implemented for some time, and the results suggest that its application has had considerable effectiveness in terms of yield and cost.
NIPT with the detection of cell free fetal DNA (cffDNA) currently is still methodically and financially demanding, and so is not suitable as a general population screening test. Screening algorithms that use cffDNA determination include changes in decision-making not only between countries but also between antenatal centers. A properly configured system of biochemical and ultrasound screening together with invasive diagnostics also enables the detection of other autosomal abnormalities that are not detectable in the basic NIPT variant. We have gathered data showing that in the second trimester a significant percentage of cases are detected. These represent a lifelong change for each family concerned. If it is possible to detect the fetus in a timely manner and to make use of an inexpensive system of established biochemical tests, it is appropriate to use them. The best solution seems to be use of an integrated test that combines examinations in the first and second trimesters, with a DR of around 90%. Additionally, if NIPT is used in cases with medium risk, the DR will be increased to around 95%.
Footnotes
Acknowledgements
We thank Dr A Sipek Sr and Dr A Sipek Jr for the statistical data provided, and Dr M Macek Sr and Dr M Vlckova from the Department of Biology and Medical Genetics of the Second Faculty of Medicine, Charles University and University Hospital Motol for their help.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by grants: MZ CR RVO-VFN64165, CZ.2.16/3.1.00/24022OPPK, 00064203 (6003) and LM2015091.