
Abstract
Objectives
In 2013, the Swiss Medical Board (SMB) concluded that for three breast cancer screens over 13 years in Switzerland, cost-effectiveness was negative, with no additional benefits in quality-adjusted life-years gained. We compared these suggested predicted effects with other estimates.
Methods
We used an extensively validated model on the natural history of breast cancer in Switzerland, comparing a 13-year time frame, a life-time perspective, and a continuous screening programme, per 10,000 Swiss women. Both approaches used the Swedish randomized controlled trials for the theoretical effect.
Results
Over 13 years, both approaches yield comparable life-years gained (56 versus 67), but in expectation in 10,000 women’s lifetimes 444 life-years are gained, and in a continuous screening programme (instead of three screens) 839 years. The SMB estimate of 56 life-years gained is counterweighted by 57 negative quality of life adjusted years, primarily resulting from a 5% annual loss for 10% of women, being false-positive results. International literature is consistent with more than four times lower losses on false-positives. The estimate of overdiagnosed cases in the 13-year time frame was four times higher than in the long-term perspective.
Conclusions
By restricting life-years gained to a 13-year time frame the SMB prediction on benefits of mammography screening is unrealistically low. Predicting long-term harms and benefits, specifically tailored to observations, regarding the clinical situation before screening commences, and possible data during a screening programme, are crucial for women, professionals, and policymakers.
Background
In a 2000 analysis of the published reports from the eight RCTs on breast cancer screening, 1 Gøtzsche and Olsen claim that ‘screening for breast cancer with mammography is unjustified. If the Swedish trials (apart from the Malmo trial) are judged to be biased, there is no reliable evidence that screening decreases breast-cancer mortality’. Several multidisciplinary committees subsequently weighed the evidence (part of it the same) and concluded that the (unbiased) trials showed breast cancer mortality reductions due to screening,2–5 and that there were no grounds to stop existing organized breast cancer screening programmes. The Cochrane group also avers that the trials showed benefits, stating that ‘screening is likely to reduce breast cancer mortality’. 5
Around 2005, further questions were raised about the negative side-effects of breast cancer screening, claiming a 57% overdiagnosis rate. 6 A systematic literature survey concluded that the most plausible estimates of overdiagnosis in European mammographic service screening programmes range from 1–10%, and that higher reported estimates are due to the lack of adjustments for risk and/or lead time. 7 Again, committees evaluated the evidence; the UK independent committee concluded that the RCTs and observational studies had shown a 20% relative risk reduction in breast cancer mortality, and that overdiagnosis was in the order of 19% in the trials (given the time frame of invitations). 8 The Health Council of the Netherlands in 2014 also confirmed a favourable harm-benefit ratio for breast cancer screening in that country. 9
In 2013, the Swiss Medical Board (SMB) estimated the benefits, harms, and cost-effectiveness of organized breast cancer screening in Switzerland. 10 Earlier reports had estimated organized and opportunistic breast cancer screening to be cost-effective using an extensively validated model on the natural history of breast cancer in Switzerland, but had estimated that the cost would be double in an opportunistic setting. 11 The 2013 report, however, concluded the cost-effectiveness to be negative, with no additional benefits in quality-adjusted life-years gained, against 223 Swiss francs per woman screened (undiscounted). Biller-Andorni and Juni 12 recently summarized their view of the evidence, although the SMB agrees that there have been no evaluations on breast cancer mortality (reductions) or other evaluation characteristics in Switzerland yet, unlike in many other countries. 13
We here compare the estimated predicted effects of both approaches, and show the importance of predicting long-term effects, specifically tailored to observations made in the countries, regarding the clinical situation before start of screening and possible data during a screening programme.
Discussion
Swiss report on reported effects
The data used to estimate the effectiveness of screening in Switzerland were based on systematic reviews and meta-analyses. The SMB analysis considered three category changes due to screening: false positives from the screening mammogram, additional breast cancers detected (that otherwise would never have been diagnosed), and a decrease in women dying from breast cancer. Calculations are presented for 10,000 women aged 50–69, screened for six years (three times every two years) and followed up for another seven years (ie. some women were followed up until age 63, others until age 82). Decrements in quality of life (QoL) are based on Karnofsky scores.
Amongst these 10,000 women, 140 (1.4%) would have been diagnosed with breast cancer without a screening programme, and 175 were diagnosed with the screening programme, ie. 35 more women, representing a 25% overdiagnosis rate (in the given time frame). Instead of 57 (0.57%) breast cancer deaths without a screening programme, there were 41 with it, meaning 16 breast cancer deaths could be prevented (amongst 10,000 women), or a 28% decrease. The SMB expected 1,025 false positives, or 10% of test results in three screenings. The ratio between breast cancer deaths prevented and overdiagnosed cases was about 1 to 2.2. Only considering life-years (unadjusted for QoL), these 10,000 women would, according to the SMB, live for 129,800 years without screening (concurring roughly with the 13-year follow-up the SMB considers), whereas with screening they would live for 129,856 years, representing a small gain of 56 years (0.4%) within this time frame (Figure 1, dark grey bars).
Showing expected effects of (a maximum of) 3 mammographic screens, 80% attendance rate, based on a natural history model for Switzerland (light grey bars), versus predicted effects by Swiss Medical Board (dark grey), both considering a 13 years follow-up period. Swiss population aged 50–69 in 1999; results per 10,000 women. The black parts of the ‘Screen detected BC’ bars represent the overdiagnosed cases.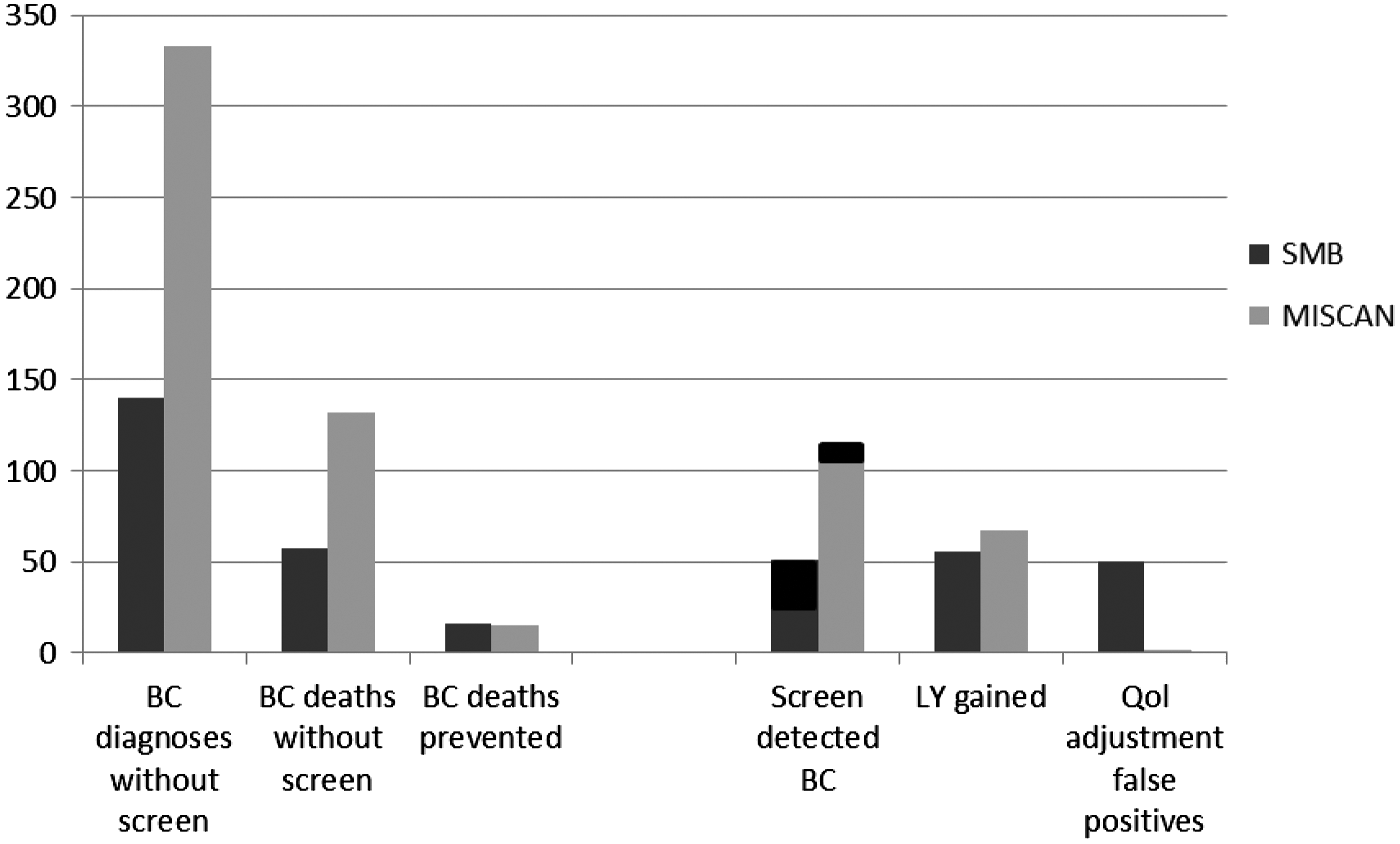
Comparison with a validated natural history model of breast cancer screening for Switzerland
In 2009, we published the results of a cost-effectiveness analysis of breast cancer screening for Switzerland, which used a validated model of the natural history of breast cancer specifically tailored to observed background data in Switzerland and the impact of screening and early treatment on this natural history. 11 Briefly, the natural history of breast cancer was calibrated for Switzerland with observed breast cancer data in the canton Vaud, where a long-standing cancer registry including pre-screening years (1974–1985) and the largest Swiss centrally organized screening programme operate.14,15 We modelled the Vaud female population, using the 1999-Swiss life table. The mean durations of the pre-clinical tumour stages and the test sensitivity were estimated by fitting the model predictions to the stage distribution in the years before screening, and to the detection rates and interval cancer rates after the introduction of the screening programme.
Figure 1 (light grey bars) shows the results per 10,000 women aged 50-69. The figure shows the results based on a 13-year follow up (as done by the SMB), and we compare these to the SMB-estimates. With (a maximum of) three screens, we would expect 333 breast cancer cases without and 354 cases with a screening programme. The underlying incidence level is considerably higher in practice than the SMB assumed (333 instead of 140), but the number of additional breast cancers diagnosed almost 60% of what the SMB assumed. More importantly, the estimated number of overdiagnosed cases is 10, compared with 35 in the SMB prediction. The overdiagnosis rate, therefore, is likely to be 3% (10/333), and not 25% (35/140) as suggested by SMB. We would expect about the same number of deaths prevented at this short follow-up (15 versus 16), and only 67 life-years gained (SMB: 56).
Given the natural history of breast cancer and the time lag for an effect of screening to happen, a 13-year time frame is insufficient to capture all possible benefits. Figure 2 shows the differences in effect comparing the estimates from the model over a 13-year time frame to a life-time perspective. For this “limited programme” of maximum three screens, 444 life-years are gained (per 10,000 women), instead of the 56 predicted by the SMB. According to the SMB, the 0.16% change in deaths prevented due to screening leads to a 0.4% difference in life-years gained. It appears that a woman with breast cancer surviving this time frame lives 6.5 years after diagnosis, whereas a woman with breast cancer dying from the disease lives three years after diagnosis, and therefore ‘only’ loses three years (in this 13-year time frame). In many developed countries life-years lost due to breast cancer are around 15 years or more.
Showing expected effects of mammographic screening, 80% attendance rate, based on natural history model for Swizerland, for respectively a 13-years follow up and 3 screens maximum (dark grey), a lifetime period and 3 screens maximum (light grey), and a lifetime period and continuous screening between 50–69 (white bars). Swiss population aged 50–69 in 1999; results per 10,000 women.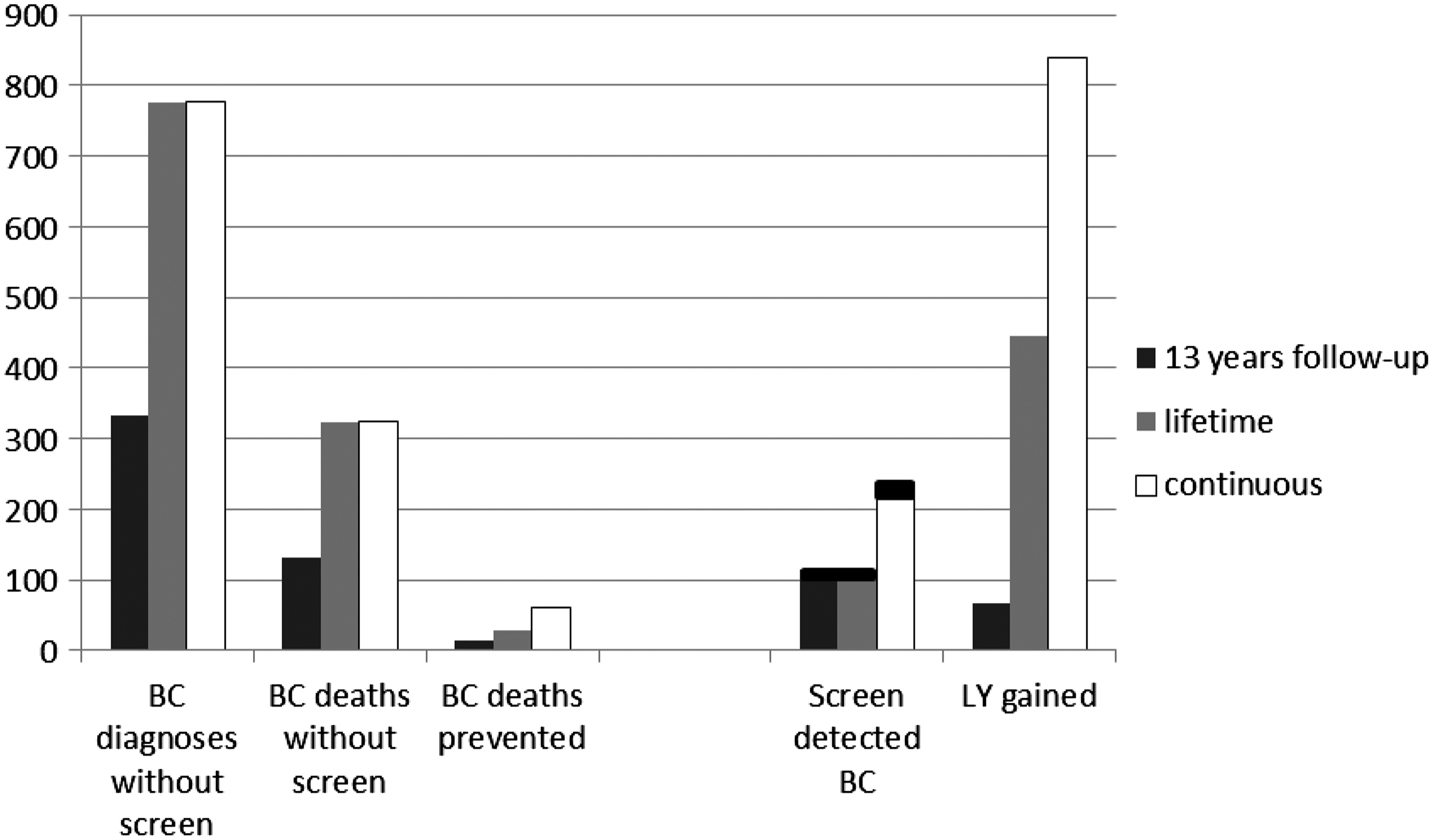
The tables (and SMB-report) above focussed on a maximum of three screens. The scenario of six years of screening with a further seven years of follow up is not practiced anywhere in the world. It would seem more important to predict the effects of a continuous breast cancer screening programme in Switzerland (white bars). Women aged 50–69 will be invited every two years, and may have a maximum of 10 screens (instead of three in the SMB report). We would expect a 19% reduction in this 1999 Swiss population, with 60 breast cancer deaths prevented (per 10,000 women) and 839 life-years gained. The 28% reduction in breast cancer deaths (in the targeted age range) seems consistent with the international literature. However, the 28% relative reduction correlates, according to the SMB, to an estimate of 56 life-years gained (per 10,000 women), and is therefore likely to be a gross underestimate of the actual effect of breast cancer screening in Switzerland.
The 25% overdiagnosis rate in this age range is relatively high. The UK independent panel estimated this at 19% in the old trials, but as the SMB state, the ‘newest estimates based on adequately performed observational studies are in the range of 1–10%’. 7 The SMB used a higher percentage than indicated by the literature, which is primarily a result of the short 13-year time frame: an excess incidence is not yet fully compensated for by a drop in incidence after the stop ages. 16
Swiss report on QoL decrements
The SMB assumed decrements in QoL (Karnofsky) of 10% for six months if falsely referred after a screening mammogram, and 7% during ten years for the 51 cases in which cancer was detected earlier, because women experience side-effects of treatment. They assumed a 50% increase in QoL for three years where breast cancer death was prevented. A decrement of 50% for three years for advanced cases (now being prevented) is consistent, and even somewhat more favourable than assumed by us in earlier analyses. 17 Data on long-term outcomes of cancer in general is scarce, but there is some literature on prostate cancer screening. We have previously considered decrements of 5-6% (life-long) for breast cancer; those used for prostate cancer were 5% for up to ten years. 18
A 10% (cumulative) false positive rate is a reasonable estimate for Switzerland. A report for 2010 shows a 2.9% false positive rate. Because around 70% of these false positive referrals only need non-invasive diagnostics to exclude cancer, most are halted within weeks, so the assumption of a QoL decrement of 10% for six months is pessimistic and unreliable, and is not supported by the literature. Figure 1 shows the assumed decrement is as large as the SMB assumed effects on life-years gained. For some women, there may be long-lasting negative outcomes on some psychological subscales, 19 but there is nothing in the literature to support such a long-lasting impact on utilities for all these women. This assumption appears to be quite influential in the Board’s analysis, as when assuming a decrement of only two months, there are 33 QALYs gained (instead of 1 QALY lost in the SMB base scenario and conclusion). A systematic review 20 cited by the SMB concludes that women who received false positive results had higher, but not apparently pathologically elevated levels of distress and anxiety. A closer review of the 23 eligible studies shows that only two found significantly more symptoms of distress at five to six months, while one found significantly fewer at eight months.21–23 Aro et al. found significantly fewer symptoms of anxiety after 12 months, 24 and Lampic found significantly fewer generalized symptoms of depression at 12 months. 25 Apart from the fact that these are not utility values, there is no strong evidence to support the reported 10% decrease over six months.
International literature on QALYs gained
Vilaprenyo et al 26 estimated the QALYs for the different breast cancer disease states, using the health related quality of life (HRQoL) measures obtained from the EuroQoL EQ-5D self-classifier in the Lidgren et al study. 27 These provided HRQoL measures for the first year after primary breast cancer (EQ-5D = 0.696); the second and following years after primary breast cancer or recurrence (EQ-5D = 0.779); and the metastatic breast cancer state (EQ-5D = 0.685). For false-positive mammograms they assumed an average annualized QoL loss of 0.013 (v SMB: 0.05). To obtain the 0.013 value they assumed that 50% of women with a false-positive result would have anxiety sufficient to increase the mood subscale of the EuroQol instrument from 0 to 1, lasting two months. According to the United States EQ-5D tariffs, such a change for an entire year represents a decrease in the QALY value of 0.156 which, divided by 12 (1/2 women _ 1/6 years) is 0.013. In the sensitivity analysis they assessed the impact of changing the disutility by false-positives to 0, and to 0.026; still substantially different from the SMB assumption.
The 1991 Dutch analysis of cost-effectiveness and QoL included estimates on 15 phases induced and/or prevented by the screening programme. 28 It appeared that 85% of decrements in QoL due to screening were due to the additional years in follow-up after diagnosis (of which around half were due to earlier detection, half to life-years gained). False positives comprised only a small component, as did the initial years of overdiagnosed cases. However, around 66% of the decrements were counterbalanced by gains. Seventy per cent of these gains imply reductions in palliative treatments for the advanced disease.
We had estimated that when adjusted for QoL there would be 3% fewer life-years gained. The most unfavourable sensitivity analysis estimated a 19.7% decrease. Had we followed the SMB estimate of false positives, we would expect an additional 6% decrement in QALY for the Dutch situation. Had we further accepted the SMB estimated QoL decrement of six months (as opposed to five weeks), we would expect a 36% decrement in the Dutch situation, a substantial difference, but not exceeding a 100% decrement and zero QALYs gained.
Cost-effectiveness analyses for Switzerland
Two cost-effectiveness analyses have been published for Switzerland,11,15 citing between 11,512 and 53,677 Euros per life-year gained. An opportunistic screening programme was estimated to cost 25,541 Euros per QALY gained. 11 These estimates were largely based on Swiss costs, and estimates on screening and stage distributions from the Vaud region, on which the most data are available. A recent report extending to the regions of Wallis, Geneva, Fribourg, and BJN (Bern, Jura, Neuchatel) confirms these data to be largely representative. 29 The cost-effectiveness ratio of breast cancer screening in Switzerland is high compared with estimates for other countries. 30 Health care costs in Switzerland are among the highest in Europe. The estimated cost of a mammogram under the screening programme is 2.5 times higher than in the Netherlands. WHO guidelines define interventions that are 1–3 times the per capita GDP as ‘cost-effective’, so with a per capita GDP of around 35,000 Euros, the earlier reports show breast cancer screening to be cost-effective, even with an opportunistic approach (though doubling the cost).
Conclusions
We agree with the SMB that the RCTs do not represent present breast cancer care, and that the trial results may therefore differ from the present-day practice and effect of screening. However, all well-performed evaluations of mammographic service breast screening in Europe show effects equal to or larger than those seen in the RCTs. Such studies have specifically analysed the effect of mammographic service screening as distinct from the existing effect of better treatment, and this therefore conflicts with the SMB report that the effect must be less than the 20% reported in trials. Njor et al. report that the most likely impact of European service mammography screening programmes was a breast cancer mortality reduction of 26% among invited women followed for 6–11 years. 31 Broeders et al state that, where sufficient longitudinal individual data are available to directly link screening history to cause of death, the best European estimate is a 25–31% reduction for invited women (and 38–48% for women actually screened). 13
In Switzerland there are around one million women aged 50–69, and approximately 5,000 new cases of breast cancer and 1,400 breast cancer deaths annually. Differences such as incidence or clinical stage distribution may have huge impacts on the cost-effectiveness of intervention programmes,30,32 but in practice, estimates of effectiveness due to screening and/or treatment are known to be most influential. The SMB report is fundamentally flawed in respect of several elements of an appropriate cost-effectiveness analysis. The prediction of benefits is unrealistically low, by restricting life-years gained to a 13-year time frame, and the predictions on unfavourable side-effects are pessimistic, due to the assumption of a long-lasting strong effect for all false-positive women and considering the excess of cases in the first 13 years to be overdiagnosis.
Summary of essential differences between SMB predictions and validated natural history model for Switzerland.
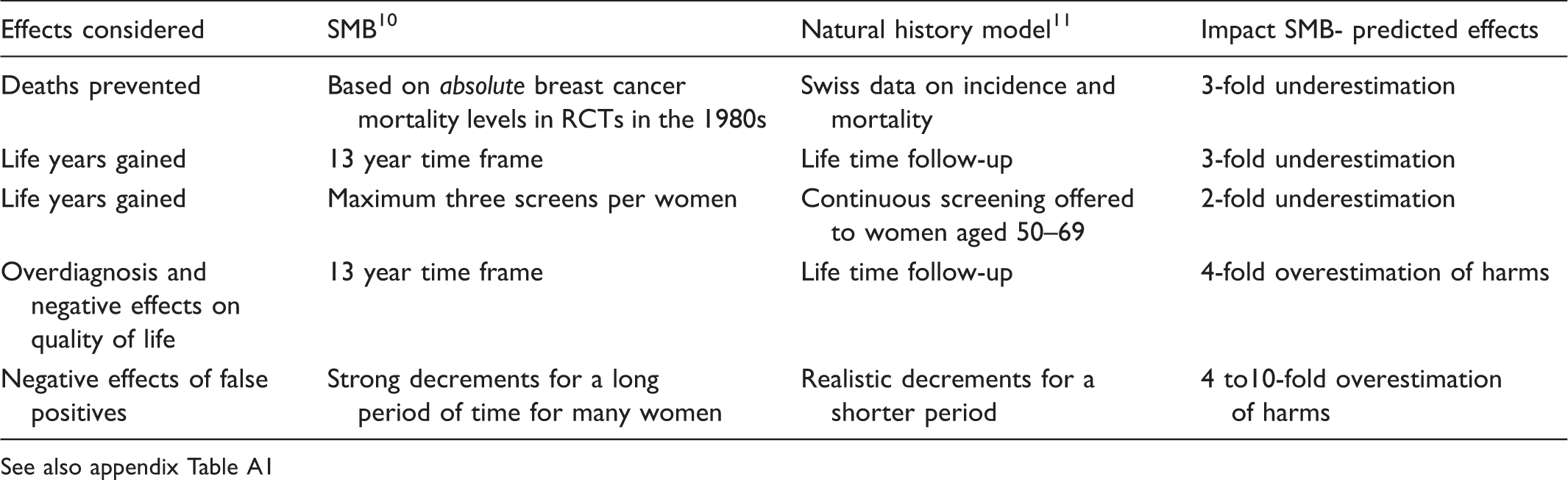
See also appendix Table A1
Footnotes
Conflict of Interest
Swiss Cancer League and SCOR Global Life SE provided grants.
Role of the Funding Source
Swiss Cancer League funded the review, but had no role in the conduct, interpretation, preparation or approval of the manuscript.
Review and development of Swiss model funded by Krebsliga Schweiz (Swiss Cancer League).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.