
Abstract
Background
Colorectal cancer (CRC) is the second commonest cancer in England. Incidence rates for colorectal adenomas and advanced colorectal neoplasia are higher in men than in women of all age groups. The male-to-female ratio for CRC incidence rates differs for different parts of the large bowel.
Objective
To summarize the current evidence on colorectal screening and prevention, focussing on potential differences in benefits between sexes and colorectal sites.
Methods
Results
(i) Our intention-to-treat random-effects meta-analysis showed that once-only flexible sigmoidoscopy (FS) screening performed on average-risk individuals aged 55 + decreased CRC incidence by 18% and mortality by 28%, but sex-specific results were lacking. (ii) Modern quantitative FIT were superior to qualitative gFOBt in average-risk population screening in their ability to discriminate between individuals with and without colorectal neoplasia. Some recent FIT studies suggest varying operating characteristics in men and women. (iii) Evidence of an effect of aspirin on the incidence of CRC (in particular, proximal disease) in both sexes aged 40 and over at average-risk of CRC is emerging.
Conclusions
We encourage researchers of CRC screening and prevention to publish their results by sex where possible. Pilot studies should be undertaken before implementation of quantitative FIT in a national screening programme to establish the appropriate threshold. Finally, individual risk assessment for CRC and non-CRC events, will be necessary to make an informed decision on whether a patient should receive aspirin chemoprevention.
Keywords
Introduction
In England, colorectal cancer (CRC) is the second most common cancer; in men, it is the third most common cause of cancer death after prostate and lung cancer, and in women the third after breast and lung cancer. 1 Incidence rates for colorectal adenomas (CRA) and advanced colorectal neoplasia (advanced CRA and CRC) are higher in men than in women of all age groups.2,3 The male-to-female ratio for CRC incidence rates differs for different parts of the large bowel, 4 suggesting different CRC aetiologies between sexes and the potential need for sex-specific recommendations in CRC prevention.
In England, age-standardized incidence rates already showed a high male-to-female ratio (close to 1.8) for rectosigmoid and rectal cancers about the time population-based data collection commenced in the early 1970s, whereas the ratio for colon cancer was close to 1.0 1 , (web appendix Table A.0). However, between 1971 and 2005, the year before the implementation of the NHS Bowel Cancer Screening Programme (NHSBCSP), CRC incidence rates had increased by 24% in men but only by 10% in women, while CRC mortality rates had decreased by 32% in men and by 46% in women. 5 In 2009, the male-to-female ratio for rectosigmoid and rectal cancers was still close to 1.8, whereas the male-to-female ratio for colon cancer had increased from 1.0 to almost 1.4, indicating that the comparatively higher increase in CRC incidence observed in men versus women over the last three decades had been driven by an increase in colon cancer. These ratios are a current feature of most high (but not low) incidence populations, ie. westernized countries, where the male-to-female ratio for rectal cancer is consistently higher than the corresponding ratio for colon cancer (2.0 versus 1.3). 6
CRC incidence has also been observed to rise more rapidly in men than in women when emigrating from low to high CRC incidence areas. 4 These observations suggest that in addition to a potential effect of sex on incidence of rectal cancer, environmental factors which arose in developed countries over the past few decades have rendered men more susceptible to colon cancer. These hypotheses are supported by the fact that the upper and lower parts of the large bowel are derived from two different embryonic tissues, with their own vascular supplies and biological environments, 7 leading to differential sensitivity to sex hormones and consequent variation in carcinogenesis pathways between men and women.4,8
Endoscopic screening with
Results from RCTs have shown that screening by
The randomized trials have used a guaiac-based test kit (
Alongside screening, chemo-intervention offers a potential complementary approach to cancer prevention. Chronic inflammation plays an important role in the development and progression of colorectal cancer.22,23
In this paper, we perform meta-analyses of the RCTs of once-only FS and biennial gFOBt and summarize the data currently available overall, and for subgroup analyses by sex and large bowel sub-location. We also consider the results of biennial gFOBt in the context of a once-only FS screen.
In addition, we review diagnostic cohort studies assessing the gFOBt and FIT tests in the same patients, and derive the relative sensitivity (RSN), the relative false-positive rate (RFP), and the odds of a true positive for the detection of both advanced neoplasia and early CRA located in different parts of the large bowel.
Finally, in an attempt to assess the potential role of aspirin in the primary prevention of bowel cancer, (ie. as part of a national programme) we gathered the evidence currently available for average-risk populations and reviewed the results obtained for each sex and by tumour site. Any preferential effect of aspirin prophylaxis according to tumour site will be of interest in the context of a complementary approach to an already implemented prevention scheme. The potential benefits of aspirin in primary CRC prevention are presented alongside potential harms to assess whether chemoprevention with aspirin is one possible intervention to reduce the burden associated with this disease.
Methods
Data sources and study selection
We conducted electronic searches of the PubMed/MEDLINE database, and of the Cochrane Collaboration’s Library up to 31 December 2012.
Once-only FS screening in the general population
The following search terms were used concomitantly and the search restricted to the title/abstract of the article: ‘sigmoidoscopy’, and ‘random*’ (or ‘trial*’). In addition, reference lists of included studies and recent related reviews were also scanned.10,11,25
Selected studies
Abstracts of the studies identified by the above searches were reviewed by the first author and the studies with the following criteria were selected: Studies published in English; Randomized controlled trials, single or double-blind; Trials performed in individuals at average risk of colorectal neoplasia (general population-based screening /community screening); Trials comparing flexible sigmoidoscopy with no intervention; Trials recruiting individuals aged 55 or over at randomization; Trials reporting results on incidence of advanced neoplasia, and/or mortality from colorectal cancer; Trials with at least 5 years of follow-up for both incidence and mortality.
Biennial gFOBt screening in the general population
The following search terms were used concomitantly and the search restricted to the title/abstract of the article: ‘fecal' (or ‘faecal’), ‘blood test', and ‘random*’ (or ‘trial*’). In addition, reference lists of included studies and recent related reviews were also scanned.10,11,25
Selected studies
Abstracts of the studies identified by the above searches were reviewed by the first author and the studies with the following criteria were selected: Studies published in English; Randomized controlled trials, open, single or double-blind; Trials performed in individuals at average risk of colorectal neoplasia (general population-based screening/community screening); Trials comparing gFOBt with no intervention; Trials recruiting individuals aged 45 or over at randomization; Trials reporting results on incidence of advanced neoplasia, and/or mortality from colorectal cancer; Trials with at least 5 years of follow-up for both incidence and mortality; Trials offering biennial gFOBt screening.
Comparison of gFOBt and FITcharacteristics
The following search terms were used concomitantly and the search restricted to the title/abstract of the article: ‘fecal' (or faecal), ‘blood test', immunochemical' (or ‘immunologic*'),'guaiac' (or ‘chemical'). In addition, reference lists of included studies and recent related reviews were also scanned.17,25–30
Selected studies
Abstracts of the studies identified by the above searches were reviewed by the first author and the studies with the following criteria were selected: Studies published in English; Diagnostic cohort studies; Studies performed in individuals at average risk of colorectal neoplasia and which excluded individuals with a personal or familial history of CRC; Studies comparing directly at least one gFOBt and one FIT; Studies assessing both tests in the same group of individuals; Studies reporting results in individuals aged 50 and over (although lower limit for age range in population studied may be lower than 50); Studies using colonoscopy or sigmoidoscopy as a reference standard to obtain a pathology diagnosis for individuals with positive test results for either gFOBt or FIT, or for all participating individuals; Studies reporting the number of true positive and true negatives based on reference standard for colorectal carcinomas/cancers (CRC), advanced and/or early colorectal adenomas (CRA).
Prophylactic aspirin in the general population
For benefit of aspirin on incidence of and mortality from colorectal neoplasia, the following search terms were used concomitantly and the search restricted to the title/abstract of the article: ‘aspirin’, ‘random*’(or ‘trial*), and ‘colo*’ (or ‘rect*' or ‘bowel' or ‘cancer’). The reference lists of the initially selected studies were scanned for any additional relevant references. All publications describing results related to the final list of selected studies were retrieved to identify reports of harms from aspirin treatment.
For additional information on serious vascular events and other malignancies, recent systematic reviews and meta-analyses of RCTs comparing incidence of and mortality from those events between aspirin and control, were identified (January 2000 – December 2012) and scanned for any relevant results.The following search terms were used concomitantly and the search restricted as stated in brackets: ‘aspirin’ [title], ‘random*’ (or ‘trial*') [title/abstract], ‘mortality’ (or ‘fatal’, ‘death’, ‘incidence’, ‘occurrence’) [title/abstract], and ‘bleed*' (or ‘haemorrhag*’ or ‘hemorrhag*’) [title/abstract], OR ‘heart’ (or ‘cardi*’, ‘vascular’, ‘coronary’, ‘stroke’) [title/abstract], OR ‘cancer’ (or ‘carcinoma’,’neoplasm’, ‘malignant’, ‘tumour’) [title/abstract].
Selected studies
Abstracts of the studies identified by the above searches were reviewed by the first author and the studies with the following criteria were selected: Studies published in English; Randomized controlled trials, single or double-blind; Trials performed in average-risk individuals (general population-based screening/community screening); Trials comparing aspirin with placebo or no treatment; Trials reporting results on incidence of and/or mortality from CRC, cancer, and/or vascular events; Trials with at least 5-year follow-up for incidence and mortality; Trials offering an oral dose of 75 mg aspirin or more, daily or on alternate days;
No restriction was applied to age at randomization. Primary prevention trials for which patients were selected on the basis of high risk factors for vascular disease or other diseases (eg. diabetes) were not included in the selection.
Statistical methods
A standard collection form was used to extract relevant information for each study included in the meta-analyses. Summary-level effect sizes were pooled using the inverse variance method (DerSimonian-Laird random-effects model) and heterogeneity (χ2) between the studies was assessed. 31
Once-only FS screening and biennial gFOBt screening in the general population
We calculated a pooled estimate of the effect of FS or gFOBt compared with no intervention on incidence and mortality from colorectal cancer and on all-cause mortality in invited individuals. The meta-analyses were performed using intention-to-treat (ITT) summary-level rate or hazard ratio data and corresponding 95% confidence intervals (CI). Individual data were obtained for the Nottingham trial from the authors (JH Scholefield and SM Moss). We also obtained ‘per protocol’ point estimates adjusted for potential selection bias using the method of Cuzick et al., 32 with 95% CI derived using the profile likelihood method of Stryhn and Christensen. 33 Compliers were defined as those who completed their test during the first round of screening (prevalence screen).
Comparison of gFOBt and FIT characteristics
The relative sensitivity (RSN, the ratio of two sensitivities) and the relative false-positive rate (RFP, the ratio of two false-positive rates) of CRC/CRA detection using FITcompared with gFOBt were derived according to the method described by Cheng and Macaluso. 34 This allowed inclusion of data from studies where the reference standard was applied solely to the population of individuals with positive test results. 35
Briefly, if we denote by m1' the number of true positive individuals identified by FIT, and by n1' the number of true positive individuals identified by gFOBt, then an estimate of the RSN of FIT compared with gFOBt is m1' / n1'. Similarly, if we denote by m1'' the number of false positive individuals for FIT, and by n1'' the number of false positive individuals for gFOBt, an estimate of the RFP of FIT compared with gFOBt is m1'' / n1''. The denominators for the absolute sensitivity and specificity of each test (ie. the total numbers of true positive and true negative individuals, which could only be ascertained if all subjects received the reference standard investigation) cancel out in the calculation of the relative figure.
Most authors classified patients as having “advanced colorectal neoplasia” if they had CRC, at least one adenomatous polyp with diameter ≥ 10 mm, or at least one adenomatous polyp with diameter < 10 mm with tubular/villous components or high-grade dysplasia. Some authors also treated the presence of ≥3 polyps as advanced neoplasia, irrespective of their size or grade of dysplasia. 36 Patients were generally classified as having “early adenoma” if they only presented with adenomas <10 mm. Hyperplastic polyps were generally not included as neoplasia with the exceptions of Cheng et al. 37 and Graser et al. 38
For advanced neoplasia (CRC + CRA ≥ 10 mm) and both advanced and early neoplasia (CRC + all CRA), the number of individuals with a false positive test result (ie. m1'', n1'') was calculated as the difference between the total number of individuals with a positive result for a given test (ie. m1, n1) minus the total number of CRC and CRA ≥ 10 mm (or all-size CRA, respectively) actually detected by the test (ie. m1', n1').
Where available, data were reported according to the location of lesions: proximal (caecum, ascending, and transverse colon including splenic flexure) versus distal (distal to splenic flexure) location. Where more than one lesion was reported for a patient, the location was set to be the region where the largest size CRA was found.
The odds and corresponding 95% CI of individuals with CRC, advanced colorectal neoplasia or adenoma having a positive FIT only (c) versus a positive gFOBt only (a) were also derived where data for the total number of individuals with a true FIT positive (c + b = i), a true gFOBt positive (a + b = g), and concomitant true gFOBt and FITpositives (b) were available.
Prophylactic aspirin in the general population
The effectiveness of aspirin in preventing incidence of, and mortality from CRC in the average-risk populations was assessed overall, and by sex and site of neoplasia. ITT risk ratios (RR) are reported in the text wherever possible (otherwise, ‘per protocol’ values are reported). In addition, summary-level crude RR and corresponding 95% CI were derived using the original publications (unless the required data were unavailable) for the comparison of aspirin versus control, for all endpoints considered.
Results
Once-only Flexible Sigmoidoscopy screening in the general population
Overview of Flexible Sigmoidoscopy (FS) RCTs characteristics.
Overall incidence & mortality
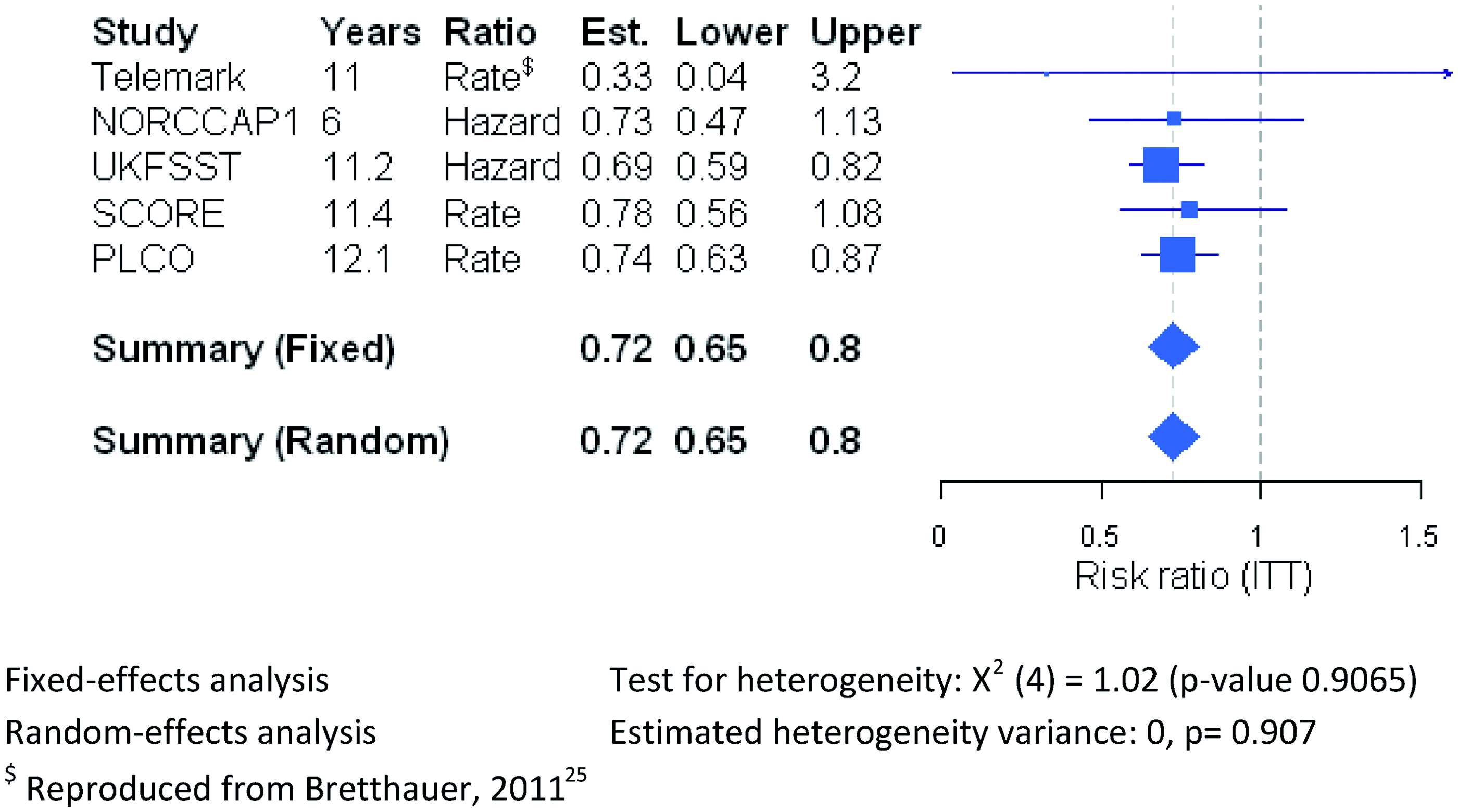
Although the first large RCT of FS versus no intervention performed in Norway did not show any reduction in CRC incidence at 7-year follow-up (NORCCAP1, Figure 1), more recent trials reported significant reductions in CRC incidence after 10-year follow-up or more, overall amounting to a significant 18% reduction in an ITT analysis (Risk ratio (RR) = 0.82, 95% CI 0.74–0.90; Figure 1 and web appendix Table A1.2). This reduction approached 30% for subjects who actually participated in screening (‘per protocol’ RR = 0.73, 95% CI 0.65–0.82; web appendix Figure A1.1b and Table A1.2). FS screening also resulted in a significant decrease in overall CRC mortality (ITT RR = 0.72, 95% CI 0.65–0.80; Figure 2 and web appendix Table A1.3). The corresponding result for the ‘per protocol’ analysis was a RR of 0.58 (95% CI 0.47–0.71). Random-effects meta-analysis of RCTs comparing once-only FS versus no screening in average-risk individuals with respect to CRC incidence (ITT analysis). Random-effects meta-analysis of RCTs comparing once-only FS versus no screening in average-risk individuals with respect to CRC mortality (ITT analysis).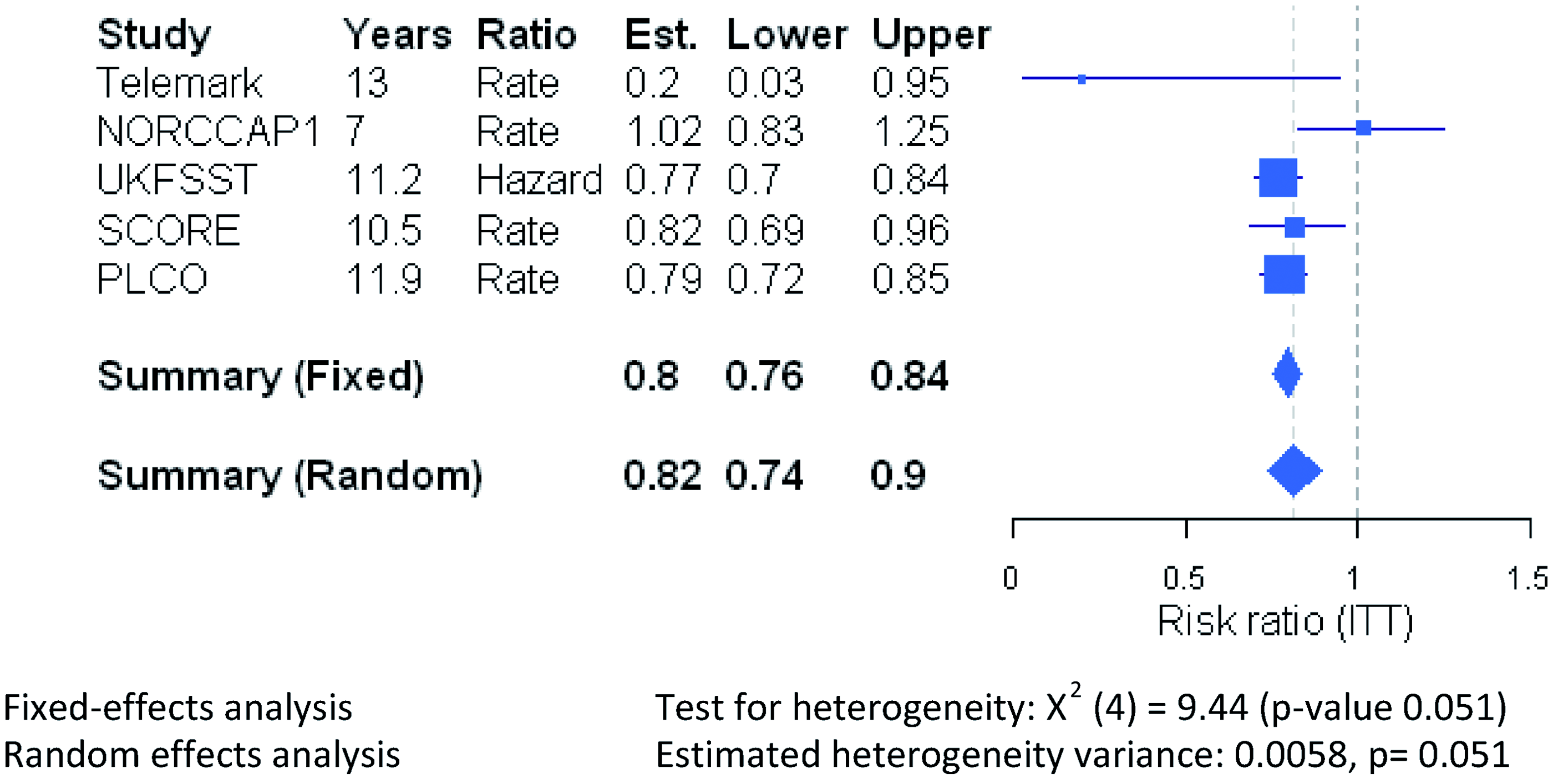
Incidence & mortality by site
Incidence of distal CRC was significantly reduced (UKFSST, SCORE & PLCO, ITT RR = 0.69, 95% CI 0.63–0.75; Figure 3 and web appendix Table A1.2), as was mortality from distal CRC (SCORE & PLCO, ITT RR = 0.58, 95% CI 0.40–0.83; web appendix Figure A1.5a and Table A1.3). Reduction in mortality from rectosigmoidal cancer was also reported in NORCCAP1 among screening attenders (HR = 0.24, 95% CI 0.08–0.76, not adjusted for self-selection bias
40
). Incidence of proximal CRC was also found to be significantly reduced (ITT RR = 0.91, 95% CI 0.84–0.99; Figure 3 and web appendix Table A1.2), although the data were more variable between trials: the UK trial showed little impact on incidence of proximal CRC compared with the United States and Italy interventions. Mortality from CRC located at proximal sites was not significantly different between intervention and control groups (Italy and United States, ITT RR = 0.95, 95% CI 0.77–1.20; web appendix Figure A1.5a and Table A1.3), even after adjusting for participation (Italy, ‘per protocol’ RR = 0.78, 95% CI 0.45–1.35; web appendix Figure A1.5b and Table A1.3). Random-effects meta-analysis of RCTs comparing once-only FS versus no screening in average-risk individuals with respect to CRC incidence at proximal and distal sites (ITT analysis).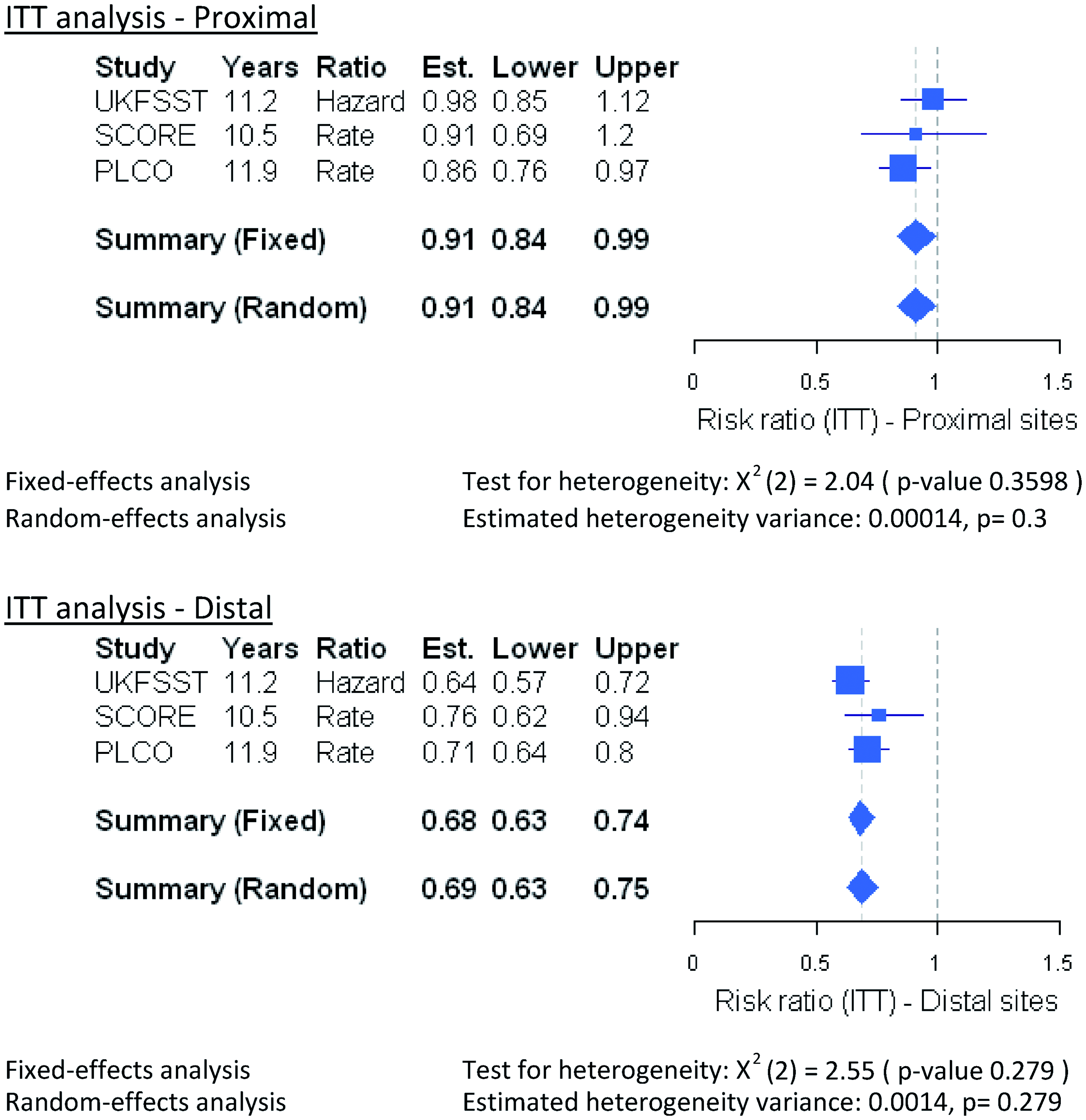
Incidence & mortality by sex
A secondary objective was to determine whether the protective effects of FS intervention differed between the male and female populations. CRC incidence data by sex showed significant reductions for both men (SCORE & PLCO ITT RR = 0.78, 95% CI 0.66–0.94), and women (ITT RR = 0.83, 95% CI 0.71–96; web appendix Figure A1.3a and Table A1.2). Interestingly, SCORE & PLCO each reported very similar effects of FS by CRC site, but opposite trends by sex. The SCORE trial conferred more advantage to women (ITT RR = 0.72, 95% CI 0.55–0.96 for women, and RR = 0.88, 95% CI 0.71–1.09 for men), while the PLCO trial conferred more benefit to men (ITT RR = 0.73, 95% CI 0.66–0.87 for men and RR = 0.86 95% CI 0.76–0.98 for women). Again, those two trials adopted a different polyp follow-up strategy. The decreased incidence with FS observed for men in the PLCO trial translated into a significant reduction in mortality from CRC (ITT RR = 0.66, 95% CI 0.53–0.81), while the mortality reduction observed for women was not significant (ITT RR = 0.87, 95% CI 0.68–1.12; web appendix Table A1.3). Data on CRC mortality by sex have so far only been published for the United States trial.
Potential harms
Alongside the benefits of FS screening, it is also necessary to consider the potential harms. Whitlock et al. 44 estimated the number of serious complications with FS from a meta-analysis of eight studies in average-risk populations to be eight times less common (0.34 per 1,000 procedures, 95% CI 0.06–1.9) than with colonoscopy (2.8, 95% CI 1.5–5.2). In another review, 9 the most common adverse event associated with FS was non-fatal bleeding (0.8–30.6 per 1,000 procedures). To our knowledge, no difference in incidence of adverse events between male and female patients has been reported.
All-cause mortality
In the more recent RCTs, all-cause mortality was consistently slightly lower in the intervention group. ‘Per protocol’ estimates were available for the SCORE & UKFSST trials (RR = 0.95, 95% CI 0.90–1.00; web appendix Figure A1.7 and Table A1.4).
Biennial gFOBt screening in the general population
Overview of biennial guaiac faecal blood test (gFOBt) RCTs characteristics.
Incidence & mortality
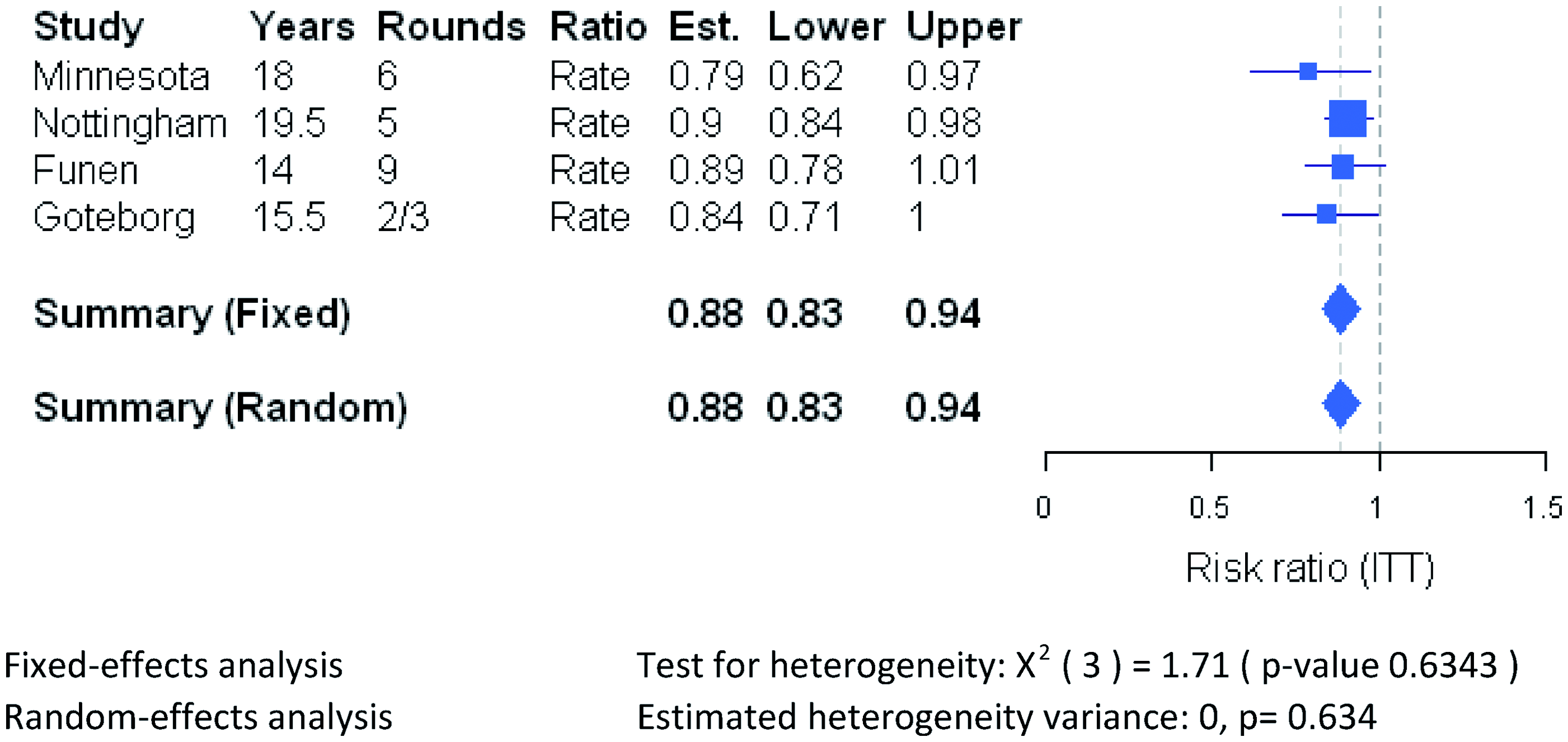
Using data with the longest follow-up available, we confirmed the absence of any significant reduction in CRC incidence by repeated gFOBt screening overall, by site or sex, including where ‘per protocol’ analyses were performed (Figure 4 and web appendix Table A2.2), and the presence of a significant decrease in CRC mortality in an ITT analysis after a median follow-up of at least 14 years (ITT RR = 0.88, 95% CI 0.83–0.94; Figure 5a and web appendix Table A2.3). The smallest reduction was observed for the Nottingham trial analysed 19.5 years after the end of the screening period, although larger reductions in CRC mortality were observed in earlier analyses of this trial (web appendix Table A2.5). ‘Per protocol’ and subgroup data were available for the Nottingham and Funen trials, which both used unrehydrated gFOBt. The meta-analysis adjusted for screening attendance for the overall data revealed a slightly stronger reduction in mortality (‘per protocol’ RR = 0.82, 95% CI 0.72–0.93; web appendix Figure A2.4b and Table A2.3). CRC mortality was similarly decreased for both proximal (ITT RR = 0.81, 95% CI 0.67–0.98) and distal (ITT RR = 0.85, 95% CI 0.74–0.98; web appendix Figure 2.5a and Table A2.3) cancers. Screening using gFOBt was equally effective at reducing CRC mortality in males and females (ITT RR = 0.84, 95% CI 0.73–0.98 for men and RR = 0.83, 95% CI 0.71–0.97 for women; web appendix Figure A2.6a and Table A2.3). Random-effects meta-analysis of RCTs comparing biennial gFOBt versus no screening in average-risk individuals with respect to CRC incidence (ITT analysis). Random-effects meta-analysis of RCTs comparing biennial gFOBt versus no screening in average-risk individuals with respect to CRC mortality (ITT analysis).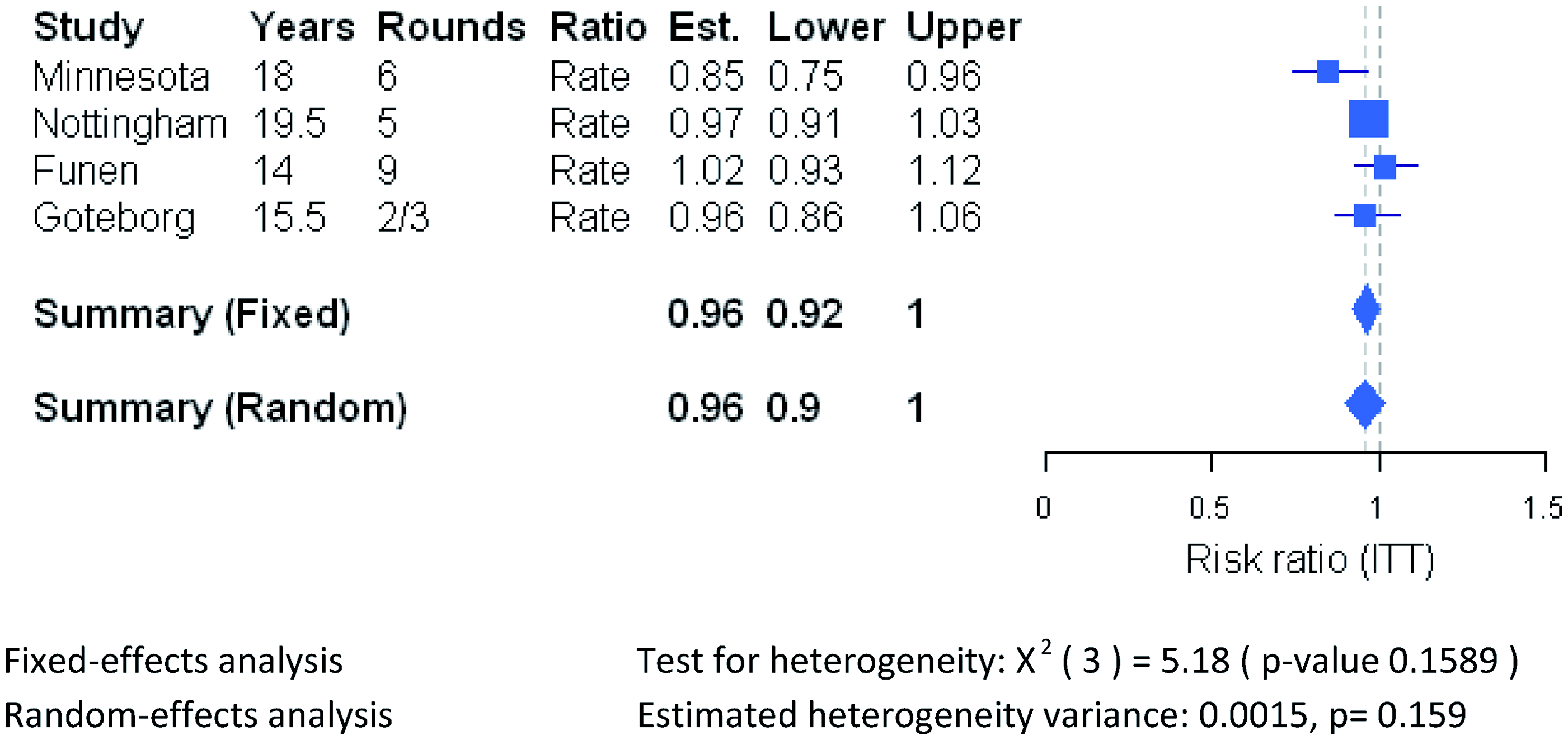
Potential harms
Screening using gFOBt per se does not cause any serious adverse events, although subsequent diagnostic testing by colonoscopy may do so 14 ; gFOBt true specificity for any dysplasia is fairly high (ie. 96–98% for Hemoccult-II as determined in patients who had all undergone colonoscopy49,50), therefore limiting the number of unnecessary colonoscopies. In addition, the anxiety caused by the receipt of an abnormal gFOBt test was shown to decrease the day after colonoscopy, and remained low one month later in patients with false positive results. 51
All-cause mortality
All-cause mortality did not differ between the intervention and control groups (web appendix Figure A2.7 and Table A2.4).
Comparison of gFOBt and FIT characteristics in the general population
Overview of characteristics of prospective diagnostic cohort studies comparing gFOBt and FIT in the same groupof screened average-risk individuals (age ≥ 50 except where*).
Overall comparison of test characteristics
Comparison of gFOBt and FIT for their ability to detect advanced colorectal neoplasia (CRC + CRA ≥ 10 mm):ratio of sensitivities (RSN) and ratio of false-positive rates (RFP).
Where data were available, the proportional odds of true positives were derived and random-effects meta-analysis results suggested that, irrespective of the type of guaiac or immunochemical method used, FIT sensitivity was overall superior to gFOBt for the detection of CRC alone, advanced colorectal neoplasia, or for the detection of any neoplasia (odds for CRC and all-size CRAs = 4.8, 95% CI 3.0–7.5; Figure 6 and web appendix Table A3.5). Comparison of gFOBt and FIT for their ability to detect colorectal neoplasia: meta-analysis of odds of positive FIT-only versus gFOBt positive-only. NS: Not Specified, NA: Not Applicable.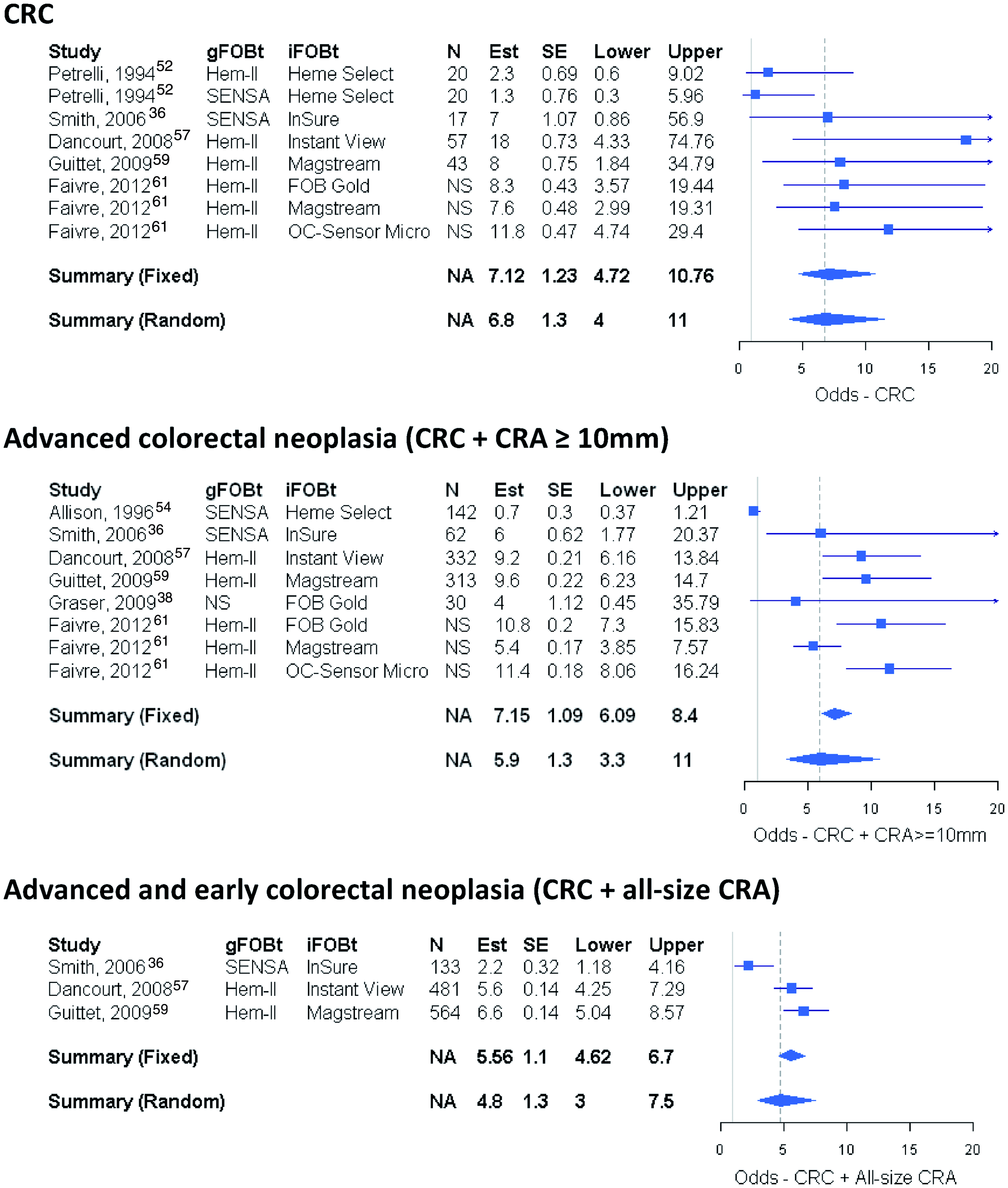
Influence of tumour site
The results obtained for HemSp/MagStream HT (100 µg Hb/g faeces, Guittet et al. 59 ) and OC-Sensor (cut-offs lower than 20 µg Hb/g faeces 21 ) suggest little difference between CRC locations for advanced neoplasia: superior sensitivity and specificity were observed both for cancer of the proximal and distal colon (web appendix Tables A3.6 and A3.7). However, Guittet et al. 59 reported increased sensitivity of HemSp/MagStream HT (100 µg Hb/g faeces) for the detection of distal versus proximal early CRA (size < 10 mm, RSN = 5.1 versus 3.9).
Influence of sex
The influence of sex on the comparative performance of the tests to detect advanced colorectal neoplasia has not been investigated with enough power in any of the diagnostic cohort studies reviewed. A recent study nested within the German screening colonoscopy programme reported a significantly greater sensitivity of Hemoccult-II gFOBt in men than in women, while the opposite was observed for specificity. 62 ImmoCARE-C (50 ng Hb/mL buffer), one of the FIT shown to have better overall sensitivity and specificity compared with Hemoccult-II 49 also showed the same trend. In contrast, a recent Spanish study found the odds ratio of having a false positive result to be at least 2-fold higher (OR = 2.82, 95% CI 2.16 – 3.68) in women compared with men when using either of the FOBt approaches, Hemascreen (Immunostics, Spain), and OC-Sensor (20 µg Hb/g faeces). 63
Prophylactic aspirin in the general population
Characteristics overview of RCTs comparing aspirin versus control treatment in average-risk individuals with respect to incidence of, and mortality from, serious vascular and malignant events. .
Overall incidence & mortality from colorectal neoplasia: Influence of sex and tumour site
A significant decrease in CRC incidence was observed when the available long-term follow-up data (10 + years, range 12–23) were pooled in a random-effects meta-analysis (crude RR = 0.86, 95% CI 0.71–1.00; Figure 7 and web appendix Table A4.1). Both the men-only UK “British Doctors' Aspirin Trial” (BDAT) and the women-only United States “Women's Health Study” (WHS) reported significant reduction, but only after 10 or more years of follow-up (BDAT 10 years or more HR = 0.64, 95% CI 0.42–0.97
64
; WHS post 10-year trial HR = 0.57, 95% CI 0.40–0.82
69
), while the men-only United States “Physicians’ Health Study” (PHS) did not after a mean follow-up of 12 years. Colorectal endoscopic screening was ruled out as an underlying cause for the difference between treatment groups in the WHS trial.
69
Random-effects meta-analysis of RCTs comparing aspirin versus control treatment in average-risk individuals with respect to incidence of CRC events.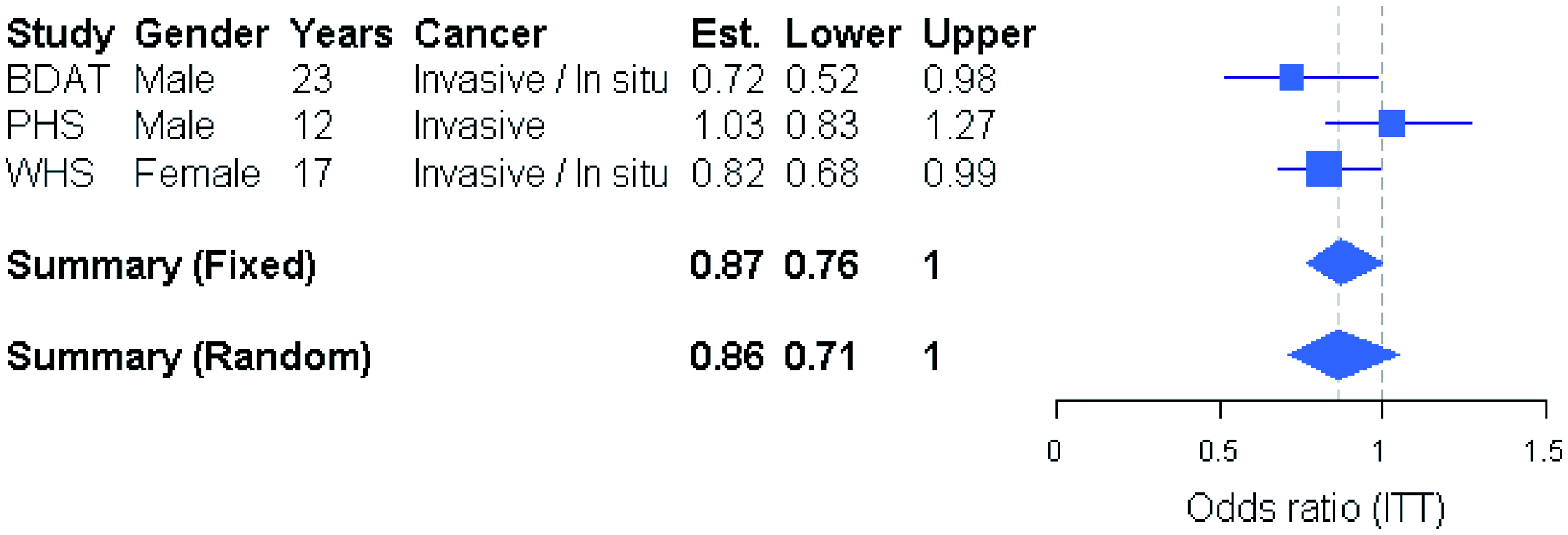
Results on the effect of aspirin on CRC incidence by site were not directly available for male BDAT and PHS trials. However, a meta-analysis by Rothwell et al., 65 which pooled data from the BDAT trial with three other trials that had recruited male patients at higher risk of vascular disease, revealed that allocation to aspirin for 5 years or longer significantly reduced the risk of colon cancer (ITT adjusted HR = 0.75, 95% CI 0.58–0.97) due to a dramatic reduction in the risk of proximal colon cancer (ITT adjusted HR = 0.35, 95% CI 0.20–0.63), but no reduction in distal colon cancer risk (ITT adjusted HR = 1.14, 95% CI 0.69–1.86). The risk of rectal cancer was also significantly reduced (ITT adjusted HR = 0.58, 95% CI 0.36–0.92). Those results were directly related to findings on CRC mortality by site in the same meta-analysis, ie. significantly reduced mortality from proximal (ITT adjusted HR = 0.24, 95% CI 0.11–0.52), but not from distal (ITT adjusted HR = 1.24, 95% CI 0.58–2.65) colon cancer, and mortality from rectal cancer reduced by over 50% (ITT adjusted HR = 0.47, 95% CI 0.26–0.87). In the female WHS trial, no significant decrease in CRC incidence was observed at any site at the end of the 10-year aspirin treatment (ITT adjusted HR = 0.92, 95% CI 0.71–1.21, in colon; ITT adjusted HR = 0.86, 95% CI 0.60–1.25, in proximal colon; ITT adjusted HR = 0.94, 95% CI 0.63–1.40, in distal colon; ITT adjusted HR = 1.20, 95% CI 0.70–2.04, in rectum). 68 However, at 17-year follow-up, the observed significant reduction in CRC incidence was primarily due to a reduction in proximal colon cancer (HR = 0.72, 95% CI 0.54–0.96). 69
Allocation to aspirin resulted in a non-significant reduction in CRC deaths at a median 23-year follow-up in the male-only BDAT trial (ITT non-adjusted OR = 0.73, 95% CI 0.49–1.10 65 ), while the female-only WHS trial found no evidence that would suggest aspirin to be effective in reducing CRC mortality after 10 or 17-year follow-up (n = 39,876; HRs not reported;68,69 web appendix Table A4.2).
Incidence of & mortality from other malignancies
There was no evidence of an effect of aspirin on incidence of any invasive neoplasm in either sex (web appendix Figure A4.1 and Table A4.1), although both BDAT and WHS reported a non-significant effect of aspirin on mortality from invasive neoplasm (web appendix Figure A4.1 and Table A4.2, pooled RR = 0.92, 95% CI 0.80–1.10).
Incidence of & mortality from vascular events
We assessed the effect of aspirin treatment in the average-risk population RCTs in terms of major vascular events (Figure 8 and web appendix Tables A4.1–A4.2). Random-effects meta-analysis of RCTs comparing aspirin versus control treatment in average-risk individuals with respect to incidence of, and mortality from serious vascular and malignant events.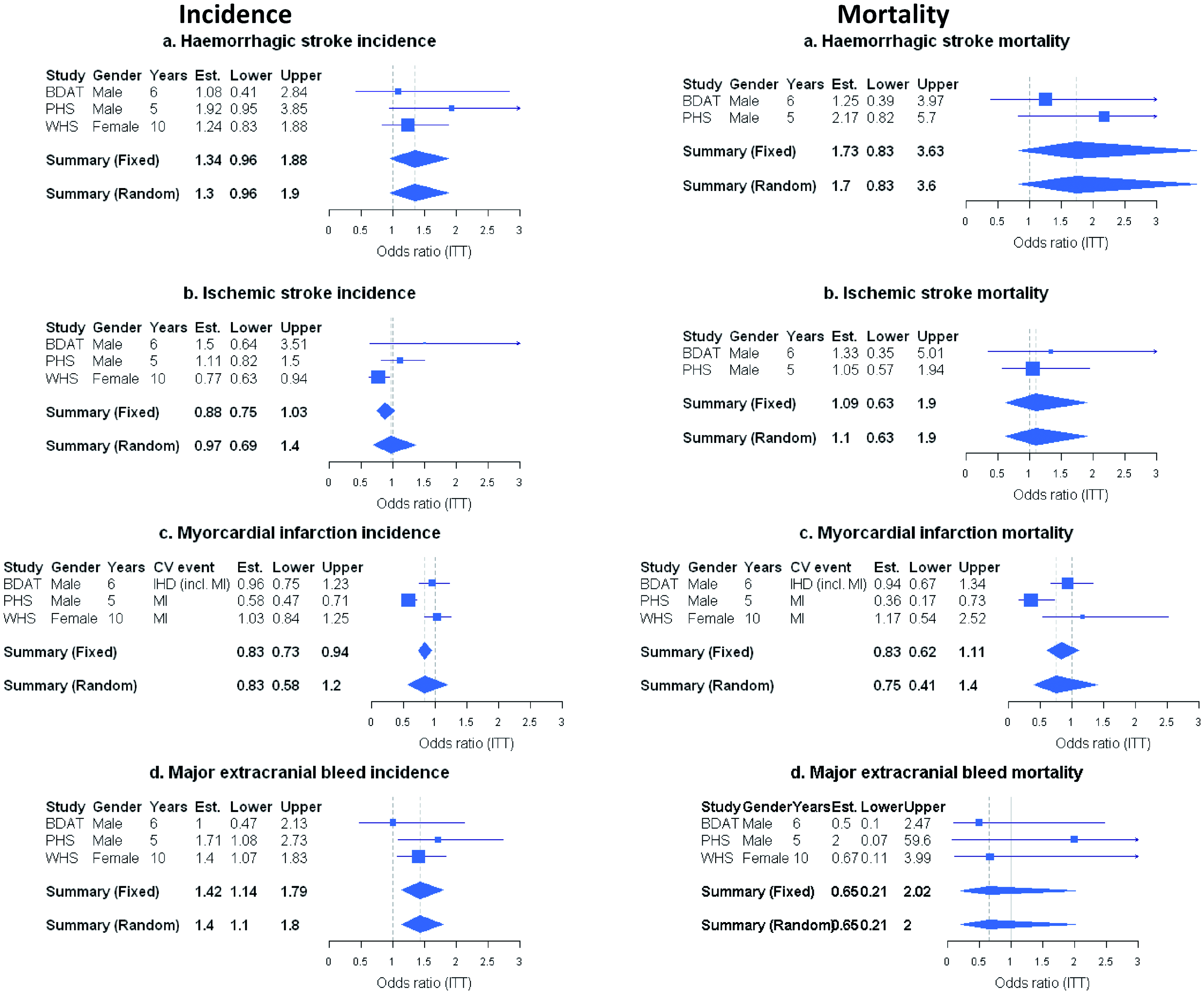
Our random-effects meta-analysis of crude risk ratios suggests an overall near significant increase in incidence of (30%) and mortality from intracranial bleeds (70%, Figure 8a). Aspirin had no impact on ischaemic strokes incidence and mortality in men, but was effective in reducing ischaemic stroke incidence in the WHS trial (Figure 8b). Overall, there was no significant benefit of aspirin on myocardial infarction (MI) incidence and mortality, although the male-only PHS trial reported a significant decrease in incidence (48%) and a non-significant decrease in mortality (64%, Figure 8c). Incidence of major extracranial bleeds (mainly GI haemorrhages) was overall significantly increased (40%) - although one of the male-only trial (BDAT) did not report any difference – while mortality from extracranial bleeds was decreased by 35%: the excess bleeds tended to be non-fatal bleeds (Figure 8d). At the end of the treatment period, the overall relative risk of fatal plus non-fatal major vascular events (strokes, ischaemic heart disease, and major extra-cranial bleeds) was 1.02 (95% CI 0.84–1.24) for the BDAT trial, 0.83 (95% CI 0.72–0.97) for the PHS trial, and 0.99 (95% CI 0.88–1.12) for the WHS trial (web appendix Table A4.1).
Discussion
The results of our intention-to-treat random-effects meta-analysis confirm that
The effect of once-only FS on incidence of CRC occurring in the distal bowel was stronger than that on incidence in the proximal (31% versus 9% reduction), and was accompanied by a significant decrease in mortality from distal CRC but not from proximal CRC (42% versus 5%), although the evidence for this mainly came from one study (PLCO). The ITT effect was the same for both sexes, although women who underwent the once-only FS intervention were reported to have a greater reduction in CRC incidence compared with men who undertook the intervention in one trial (SCORE, 21% versus 45%), while compliance was reported to be higher in men than in women in two of the other trials analyzed (ie. UKFSST 70 and PCLO 71 ). In contrast, a significant reduction in CRC mortality (34%, ITT analysis) was only observed for the male population in the PLCO trial which reported on this outcome.
This could be related to the fact that men do develop more rectal cancers than women 4 , and women are known to develop more proximal tumours with microsatellite instability with age, 4 which may have led to proportionally fewer lesions being identified by FS in women. The PLCO trial recruited patients up to the age of 74 in contrast to the other trials (upper limit of 64).
Significant 12% (ITT analysis) and 18% (‘per protocol’ analysis) decreases in CRC mortality were observed for
Endoscopic screening with once-only FS at age 50+ has been found to be more sensitive than both guaiac rehydrated 74 or unrehydrated19,75–77) Hemoccult-II, and qualitative faecal immunochemical tests for haemoglobin (OC-Sensor,19,77 Immudia-HemSp78,79) for the detection of prevalent advanced CRA. 9 The results from the long-term RCTs on the effect of the two screening approaches on incidence of CRC confirmed this observation.
Compliance with screening is an important factor in effectiveness of a screening programme. In the RCTs, compliance at first screen for gFOBt ranged from 57 to 67% (see Table 2) and for FS from 58 to 83.5% (see Table 1). For the latter, compliance in the general population is likely to be lower than among those expressing an interest to participate, while for repeated gFOBt screening compliance may diminish over time, although the UK pilot did not present evidence of substantial fall in compliance over three rounds. 80 Differences in compliance between sexes, by age and in different ethnic groups, are important and should be considered in relation to differences in risk. ‘Per protocol’ analyses of the RCTs are therefore valuable for comparisons of different modalities and subgroups. When ‘per protocol’ estimates were compared, once-only FS was still superior to repeated gFOBt screening with respect to CRC mortality reduction (42% versus 18% decrease).
Long-term studies of the impact of adding once-only FS to repeated FOBt on CRC incidence and mortality are not yet available. One trial reported significantly fewer CRC cases detected in the ‘gFOBt, plus FS group’ compared with the group allocated to ‘gFOBt only’ in the 24–62 months following the prevalent screen. 76 In a review of cost-effectiveness studies, no one screening strategy emerged as the most effective in terms of life-years saved, or as the preferred strategy for a given willingness to pay; discrepancies between modelling studies were mainly due to differences in the simulated duration of the adenoma-carcinoma sequence. 81 Using a state transition modelling approach and newly available CRC incidence data in the absence of screening, Whyte et al. 82 estimated that combining once-only FS at age 55 (based on UKFSST data) with biennial FIT age 60--74 (OC-Sensor with a threshold of 20 µg Hb/g faeces) would increase clinical (and economic) benefits over the use of a single screening modality in England. There was some evidence that once-only FS screening might benefit men more than women in terms of CRC mortality, probably due to the fact that men develop proportionally more distal tumours than women and develop advanced CRAs at an earlier age. 3 The optimal age for the greatest quality-adjusted life year gain using once-only FS was estimated to be between 52 and 58. 82
Our
Comparative results of OC-Sensor versus Hemoccult-II sensitivity and specificity were consistent between diagnostic cohort studies and parallel group trials; sensitivity was found to be superior to both unrehydrated Hemoccult-II (RSN > 2.0 at cut-offs of 10 and 20 µg Hb/g faeces,18,19 respectively) and Hemoccult SENSA (RSN > 1.5 at a cut-off of 14 µg Hb/g faeces, 83 rehydration status not reported), while specificity was inferior at those thresholds (RFP > 1.0).
Compliance at first screening round has generally been reported to be higher for FIT compared with gFOBt as assessed using meta-analysis of RCTs by Vart et al. 84 and by others85,86, while Birkenfeld et al. 87 found overall comparable compliance for the two methods with taking the kits favouring gFOBT and kit return favouring FIT. Finally, Chubak et al. 88 found uptake of 1-stool OC-Sensor to be significantly higher than 2-stool InSureFIT and 3-stool Hemoccult-SENSA. A Cochrane review to compare diagnostic accuracy of gFOBT and FIT screening for the detection of advanced colorectal neoplasia in average-risk individuals is currently being undertaken. 30 A strategy of biennial FIT (OC-Sensor), age 60–74 was found to be cost saving and to result in quality-adjusted life year gains compared with the current screening programme of biennial gFOBT age 60–74. 82 However, the results were highly sensitive to FIT threshold model parameters with higher thresholds of 30 and 40 µg Hb/g faeces associated with lower quality adjusted life year (QALY) gains but little difference in costs.
The efficacy of
Our review of RCTs performed in average-risk individuals suggests a protective effect of aspirin on the incidence of CRC in both male and female individuals after at least 5 year of treatment and 10 years of follow-up, although relative estimates were quite variable. The large study of female individuals reported a significant 14% reduction in proximal colon 69 , which was much smaller than the estimate reported for populations at high-risk of vascular disease. 65
Only one of the two large RCTs performed in males reported data on CRC mortality. This study showed a non-significant 27% reduction with a more likely favourable outcome for proximal CRC, while the only large female RCT reported no significant effect (exact ratios not reported). The 27% reduction is much less than the 42% reduction reported in the meta-analysis of males at higher risk of vascular disease. 91 In a recent large cohort study of healthy individuals, CRC mortality was only modestly reduced in patients taking aspirin (adjusted HR after ≥ 5 years of use = 0.92, 95% CI 0.83 to 1.02 92 ).
The effect of aspirin in average-risk individuals appeared to be quite specific to CRC as the RCTs did not find an overall benefit of aspirin on incidence of or mortality from all cancers after a follow-up of at least 10 years, although other primary tumours of the gastro-intestinal tract have been reported to be sensitive to aspirin prophylaxis.69,90 Those findings are in contrast to the reduced incidence of all cancers reported 91 for both men and women in a meta-analysis of 12 RCTs for primary prevention of vascular events in individuals of various health status (OR = 0.76, 95% CI 0.66 – 0.88).
Overall, the effects of aspirin treatment on risk of major vascular events (strokes, ischaemic heart disease, and major extra-cranial bleeds) suggested (i) limited benefit of aspirin on primary prevention of vascular events in average-risk individuals, but also (ii) limited harm due to major haemorrhages. 93 These observations are in agreement with the results by Rothwell et al. 91 which showed no significant difference between low-dose daily aspirin and control treatment on risk of vascular death, the trials' primary endpoint, in individuals of various health status (ITT unadjusted OR = 0.93, 95% CI 0.70–1.23). These observations were also in agreement with the results from a review of recent meta-analyses of primary prevention trials 94 showing no convincing evidence that aspirin reduces cardiovascular mortality although it had a modest significant reduction on total mortality.
The risk of bleeding associated with aspirin use has however been shown to be particularly high in individuals younger than 50 years in a prospective study with median follow-up of 5.7 years, 95 suggesting that the balance of benefits and harms may vary with life stages. In addition, a meta-analysis by the Antithrombotic Trialists’ (ATT) Collaboration 96 which used individual data from the BDAT, PHS, and WHS trials, among others, showed that aspirin increased the risk of GI bleeding in non-smokers compared with current smokers, and in patients with relatively lower 5-year predicted risk of coronary heart disease (<5%). Interestingly, the benefit of aspirin on the risk of fatal adenocarcinoma was also reported to be greatest in smokers. 97
Finally, other adverse effects of aspirin such as on renal function and the control of blood pressure98,99 and, to a lesser extent, on gut lining integrity and dyspepsia 100 as well as the discomfort caused by minor bleeding events also need to be taken into consideration.
Sequestration of angiogenesis regulatory proteins has recently been shown to be elevated in platelets of CRC patients (all stages) compared with healthy individuals, 101 and thrombocytosis (high platelet count) has been found to be associated with poor prognosis in colon cancer. 102 However, whether thrombocytosis is causal or consequent to cancer development is to be determined before we can understand whether healthy people with elevated platelet levels are at higher risk of developing cancer, and/or metastasis.
The risk of vascular events was found to be significantly higher in non-responders to aspirin compared with responders in a meta-analysis of observational studies performed in patients at higher risk of vascular events. 103 High platelet reactivity to arachidonic acid, an indirect COX-1-dependent pathway, has been associated with cardiac adverse events in a prospective cohort study of patients undergoing percutaneous coronary intervention at 12-month follow-up 104 , but not in another where COX-1 independent platelet function correlated with subsequent major adverse cardiovascular events at 2-year follow-up. 105 Whether similar patterns will be observed with respect to incidence of CRC in average-risk individuals remains to be elucidated.
The net clinical benefit over the risks presented by prolonged aspirin intake will need to be assessed on an individual basis taking into consideration each patient's risk factors.
Conclusion
Evidence for a different CRC aetiology between men and women is mounting. RCTs of biennial gFOBt screening starting at age 60 did not show a differential benefit in terms of CRC incidence or mortality between sexes, while a recent cross-sectional analysis suggests the introduction of gFOBt screening in the UK is having a greater differential impact on male than on female mortality, 106 in spite of lower compliance in men 13 (see web appendix Table A2.10). In contrast, preliminary results from once-only FS screening trials performed at age 55 or over suggest greater benefit for men in term of mortality, although the evidence is still sparse. Since March 2013, the NHSBCSP has started rolling out a once-only FS programme in six areas in England where patients are invited for ‘bowel scope screening' around the time of their 55th birthday. In time, this will provide more insight into male-female potential differences in screening benefit. The optimal age for screening initiation has been proposed to be around 5 years higher for women than for men within average-risk populations, based on 10-year CRC incidence and mortality 107 , but this assumes that screening is equally effective in both sexes, which we know not to be the case, men and women having different incidence of proximal and distal lesions and screening modalities preferentially detecting lesions located in right or left bowel. Finally, long-term effects of aspirin treatment on CRC incidence has now been shown in both men and women at average-risk of CRC or vascular events who started treatment aged 40 or over with particular benefit for proximal CRC.
Age at menopause and consequent sex hormone changes in women may be an important factor when it comes to choosing the optimal window for implementing the different approaches available for primary CRC prevention. Age- and sex-specific vascular risk factors will also have to be taken into account when considering aspirin chemoprevention as part of a national CRC prevention programme. Further investigation into the effectiveness of the various screening modalities by sex and site of lesions is warranted.
Footnotes
SWD and NJM contributed to this work as part of the programme of the Policy Research Unit in Cancer Awareness, Screening and Early Diagnosis. The Policy Research Unit in Cancer Awareness, Screening, and Early Diagnosis receives funding for a research programme from the Department of Health Policy Research Programme. It is a collaboration between researchers from seven institutions (Queen Mary University of London, UCL, King’s College London, London School of Hygiene and Tropical Medicine, Hull York Medical School, Durham University and Peninsula Medical School).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.