
Abstract
Alexander Blackrie (bap. 1702, d. 1772) was a Scottish Surgeon-Apothecary who attended Aberdeen's grammar school and Marischal College. He served as surgeon-general in India and practised at Bromley, Kent, England. In later life, he suffered from the ‘gravel and stone’ i.e., urological stones. This triggered an enquiry into the lucrative medication of Dr Chittick of Bath. Blackrie deduced it to be nothing more than soap-lye (Sodium hydroxide) and went on to formulate his own version (‘Blackrie's lixivium’). Blackrie undertook comparative experiments on the efficacy of these two products at dissolving equally-sized fragments of the same urinary stone. In 1763, he published his proposal to compare the two products in patients. This called for: selection of patients ‘afflicted in the same degree’, randomisation by ‘dividing them equally by lot', the ‘experiment’ to be ‘repeated’ and the number of participations to be ‘large’. Although never implemented, Blackrie's proposal is an early model of a randomised controlled trial and may be the first description of a non-inferiority trial. His use of the term ‘decisive’ experiment and reference to James Jurin FRS may offer a link with Hauksbee the Younger's 1743 proposed ‘experimentum crucis’. Blackrie's contribution to the development of fair comparisons of treatments deserves greater recognition.
Keywords
Introduction
The origins of the randomised controlled trial (RCT) lie in the seventeenth century. Two proposals for randomised treatment comparisons were published at that time, the first by the Flemish physician Jan Baptist van Helmont (1580–1644) and published posthumously in Latin in 1648.
1
This states the following: Let us take from the itinerants’ hospitals, from the camps or from elsewhere 200 or 500 poor people with fevers, pleurisy etc. and divide them in two: let us cast lots so that one half of them fall to me and the other half to you. I shall cure them without blood-letting or perceptible purging, you will do so according to your knowledge (nor do I even hold you to your boast of abstaining from phlebotomy or purging) and we shall see how many funerals each of us will have: the outcome of the contest shall be the reward of 300 florins deposited by each of us. Thus shall your business be concluded.
1
A second proposal for a randomised treatment comparison was published in 1658 by the Anglo-American alchemist (and disciple of van Helmont) George Starkey (1628–1665).
2
Although Starkey does not state how randomisation should take place, the notion of equal odds is inherent in his proposal for selection ‘on the same lay’.
2
His proposal was published in English and includes the following: let them [patients] be divided by tens, they to divide one ten, and I another, and always the divider to have the five Patients which the chooser leaves; I will engage to perform all my cures without blood-letting, purging by any promiscuous Purge or vomiting by any promiscuous Vomit….
2
No other proposals for randomised comparisons appear to have been described before the twentieth century. The middle of the eighteenth century was a notable period for the development of the controlled trial of medical treatments. Foremost was the 1747 (published 1753) description by James Lind (1716−1794) of his trial of scurvy treatments aboard HMS Salisbury. 3 New evidence suggests that Lind's study was informed by reading the proposed ‘experimentum crucis’ (decisive experiment) published by the instrument maker Francis Hauksbee the Younger (1687–1763) in 1743. 4 This was a 10-step proposal to compare treatments for venereal disease, a condition that was also the subject of Lind's 1747 thesis at Edinburgh University. 5 A further link between Hauksbee and Lind lies in number of participants: twelve. Hauksbee also includes scope for comparison of more than one treatment by stating a desire to compare his own medication with ‘those other Medicines and Methods of Cure commonly used by the Gentlemen most noted in Practice for the cure of this Distemper’. 6 A further possible influence on James Lind is Thomas Reeve's (1700–1780) proposal for two comparisons of treatment with and without tar water published in 1744. 7
Consideration of how best to test the efficacy of medication came to a head in the mid-eighteenth century. This was especially true in the context of one condition: the ‘gravel and stone’, that is, urological stones (see Figure 1). At this time, urological stones were a common problem for patients and a profitable one for physicians and surgeons. In an age before antiseptics and anaesthetics, surgical treatment (‘cutting for the stone’) was risky, traumatic and a last resort. In the 1740s, surgeons began publishing comparative mortality figures, most notably William Cheselden (1688–1752). His surgical data were significant for considering mortality figures by age group.
8
Around this time, many patent medications emerged and were advertised as alternatives to surgery, leading to allegations of profiteering and a lack of proof due to secret ingredients. For these reasons, much energy was expended in assessing their efficacy. Most influential amongst such nostrums was one known as ‘Mrs Stephen's Medicine’: In 1738 a certain Joanna Stephens claimed that she had devised an infallible cure for the complaint, and the British government paid her the enormous sum of £5000 (around £600,000 now) to disclose her secret recipe. Its ingredients included soap, snails and burnt eggshells, and –mpa#ndash; like every such concoction dreamed up to treat the condition –mpa#ndash; it turned out to be entirely useless.
9
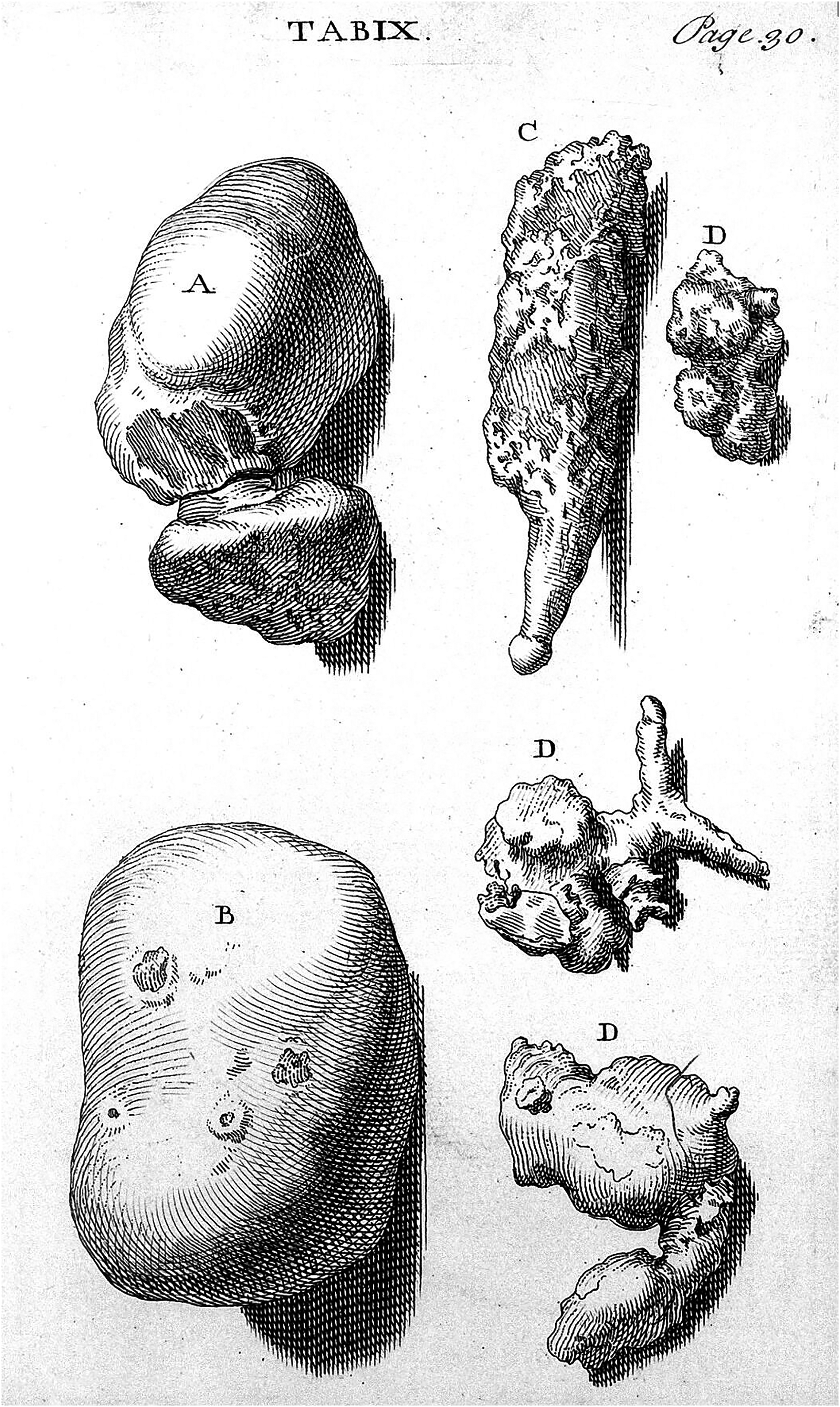
Image of urological stones from William Cheselden's (1688–1752) treatise on the high operation for the stone (1723). William Cheselden was an English surgeon who operated to remove bladder stones. Blackrie sought to dissolve stones inside the bladder and, thus, avoid the risk and pain of surgery. Image courtesy of the Wellcome Collection.
A further lixivium (alkaline solution, typically extracted from the ashes of wood) was that of Dr Chittick, a physician who practised at Bath, Somerset. Little is recorded about the identity and biography of Dr Chittick. The physician Walter Chittick is known to have practised at Bath and to have died in 1761. 10 A Chittick brother continued to peddle the lixivium later in the eighteenth century. His first name is unknown but is presumably the same ‘Chitteck’ noted to be ‘physician for the summer season’ at Brighton, Sussex, in 1784. 11
This article considers how the Aberdeen-educated apothecary-surgeon Alexander Blackrie was key in unravelling the contents of Chittick's product. In this process, Blackrie also published a proposal for (what today would be called) a basic randomised controlled trial.
Blackrie's biography and the ‘gravel and stone’
Little has been published about Blackrie. His biography is described in detail in the Oxford Dictionary of National Biography: ‘[Blackrie] was baptized on 14 June 1702 at the church of St Nicholas, Aberdeen, the seventh of the eleven children of William Blackrie and his wife, Isobel, née Fordyce. A merchant's son, he was educated at the grammar school and Marischal College, Aberdeen (1718–22), and went on to be surgeon-general on the Indian establishment. Among his friends was an East India Company director, John Hawkesworth of Bromley, Kent; Blackrie moved to the town in the late 1730s and practised there for the rest of his life’.
12
Blackrie is not included in Drew's Commissioned Officers in the Medical Services of the British Army.
13
Blackrie's absence might, however, be explained on grounds that the East India Company possessed its own army and military surgeons. In later life, Blackrie became interested in treatments for urinary stones (see Figure 1) and published on this subject. His venture into publishing about urological stones began in 1763 in the Scots Magazine.
14
An identical submission appears to have been made to the Gentleman's magazine earlier in the same year (evidenced by the Scots Magazine submission opening with the words ‘Mr Urban’, i.e., the pen name of Edward Cave (1691–1754), editor of the Gentleman's magazine). This unidentified article is also alluded to in a 1764 submission by Blackrie to the Gentleman's magazine.
15
These early submissions were published under the initials ‘A.B’. Blackrie went on to write a book entitled ‘A disquisition on medicines that dissolve the stone. In which Dr Chittick's secret is considered and discovered’ first published in 1766
16
(see Figures 2 and 3) with a second, expanded edition in 1771.
17
After Blackrie's death, a French version of the book was published in 1775
18
(see Figure 4). In his first edition he explains how he became involved in this area of enquiry: ‘About five years ago a severe fit of the gravel supervening upon the return of a painful illness to which I have been long subject, and by which I was then confined, alarmed me much, as I continued several days in great agonies and danger’
16
‘In consequence of this unexpected incident, that disease, which is at least as calamitous as any of the other lasting disorders that afflict mankind; and which more frequently occurs, as no age, sex or condition is exempted from its attacks, became so much the subject of my attention, that I have ever since spared no pains to obtain the knowledge of everything recommended to me as remarkably serviceable for the cure, or relief, of this cruel distemper….’
16
Front cover of Blackrie's book A Disquisition on Medicines that Dissolve the Stone (1766). Image courtesy of the Wellcome Collection.
Blackrie reveals in his book (A Disquisition - see above) how his initial experiment into the dissolving of urological stones was inspired by the teaching of the Dutch physician-chemist Herman Boerhaave (1668–1738).
French version of Blackrie's text: Recherches sur les remèdes capables de dissoudre la pierre et la gravelle traduites de l'anglois. This was published in 1775, i.e. after Blackrie's death.
Blackrie's enquiry into Chittick's lixivium
Blackrie's specific reasons for enquiring into Chittick's remedy have been attributed to ‘a combination of altruism and detective curiosity’.
19
Nevertheless, Blackrie's account reveals a far more personal –mpa#ndash; and painful –motivation: In the course of my enquiries, I was told of a medicine, which, for a considerable time past, has continued in high repute as a powerful lithinotriptick; and was informed, that about five years ago, it was obtruded upon the publick as a new discovery, and administered with success at Bath, by the late Dr. Chittick; and, since his death, in London and Westminster, by his brother, the present Dr. Chittick, who, as his heir, became sole possessor of this remedy, and after his brother's example, makes use of every artifice to keep it secret.
16
In particular, so circumspect in concealing his medicine does the present proprietor still continue, that, in administring [sic] it, he entrusts it unmixed with no person whatsoever; conscious, no doubt, that if but once submitted to inspection and examination, it would immediately betray itself.
16
I could not help lamenting that the custom of concealing for lucrative purposes such salutary [i.e., good for health] discoveries, should be so frequent and prevailing.
16
The terms upon which he administers this medicine, are two guineas a week, during the whole time of the cure, indiscriminately from rich and poor; for this he gives no credit, if he is not therefore regularly paid at every week's end, he refuses to medicate the broth. … [He] expects a considerable premium besides, for his pains and trouble, after the cure is completed.
16
I had the good fortune to be introduced to several gentlemen who had taken, and were taking, this broth, and had afterwards ready access whenever I went: they allowed me to taste it, and without reserve communicated to me what they knew [about it].
16
When I first tasted this medicated broth, what struck me most was a strong flavour of tansy [daisy flower], but upon carefully tasting it again and again, I at last discovered, very plainly, the effect of an alkaline matter upon my palate; and immediately said to the patient, ‘ I believe, Sir, I know the medicine….
16
Although it was reported that Chittick entrusted the unmixed lixivium to no one, it is likely that his patients witnessed the product being diluted and had access to this version for use between consultations. Blackrie consulted other patients, one of whom stated that: the doctor [Chittick] himself acknowledged to him [a patient] that these tastes [a broth of daisy and hartshorn] were given on purpose to disguise his medication.
16
I was told, that the Doctor [Chittick], in discourse with several of his patients, greatly exclaimed against the use of alkaline salts and substances…. and complained that he failed of success in several instances, only because his patients, previous to his being employed, had burned up their insides with soap-lye, lime water, and other such like caustic stuff: these speeches, however, rather confirmed me in my opinion [that they were] words of artifice…
16
For this medicine… such a high price is demanded as every person whom I have spoken to greatly complains of; so that the benefit of a remedy in several instances confessedly serviceable, so dearly [i.e., expensively] sold, and so limited in its use that it is only to be had at one place, can be enjoyed but by very few.
16
Incited therefore by no other motive than a desire of being in some measure instrumental and subservient to the general welfare, I have determined to publish these remarks, in hopes, that they may prove useful, not only to those who cannot afford the price demanded, but likewise to those whose distance from the place of the doctor's residence makes their personal attendance at all times extremely inconvenient.
16
Dr Chittick's medicine is nothing more than a weak veal-broth without fat, medicated with a greater or less quantity, as circumstances require, of soap-lye, or some substance, of which a fixt alkaline salt is the basis, not specifically different from soap-lye.
14
Blackrie's lixivium
As part of his endeavour, Blackrie created his own version which became known as ‘Blackrie's Lixivium’ or ‘Blackrie's Solvent’. The aim of Blackrie's experimental enquiry was to prove the two products to be one and the same, i.e., similarly effective. First, Blackrie undertook comparisons of the effects of the two treatments upon urological stones. His inspiration for this initial enquiry was the work of the Dutch physician-chemist the ‘most learned’ Herman Boerhaave (1668–1738)
16
(see Figure 3). This included comparative experiments of the effects of Chittick's and his own ‘broths’ upon urinary stones: ‘My broth being now the same in all sensible qualities, I proceeded to make experiments of its efficacy; I therefore took two equal fragments of the same calculus, and put one of them into a small quantity of my broth, and the other in to an equal quantity of his: the consequence was, that both dissolved in the same time.
14
Take eight ounces of pot-ash and four ounces of quick-lime fresh from the kiln; mix and put into a glazed earthen vessel; then pour upon them a quart of boiling soft spring-water; let the infusion remain twenty-four hours, stirring it now and then; and afterwards filtrate it for use.
16
None of my experiments have furnished any example of a stone which soap-lees [sic] did not speedily dissolve.
16
Blackrie's proposal for a randomised controlled trial
Blackrie makes it clear, however, that he lacked the opportunity to test the products in patients. This leads to one aspect of Blackrie's writing which appears to have been overlooked, namely his 1763 proposal for a randomised controlled trial published in the Scots Magazine.
14
Like many other proposed trials of this era, which might today be considered controlled trials, this is set down as a challenge: This experiment, therefore, I most earnestly recommend to the physicians of our hospitals, and to others in private practice, where the patient is willing: and if Dr Chittick is conscious that his medicine is essentially different, and in virtue of that difference is more efficacious, let him at once put the matter out to question.
14
by joining with some gentleman of the [medical] faculty in selecting a number of patients, supposed to be afflicted in the same degree, and dividing them equally by lot, then administering his medicine to half of them, while my preparation is administered to the other half.
14
This experiment, especially if it is repeated two or three times, or if the number be large, cannot fail of demonstrating on which preparation the advantage lies, supposing the virtue of both not to be equal.
14
Discussion
Blackrie's proposal constitutes the first proposal for a basic randomised controlled trial published in English after that of the Anglo-American alchemist George Starkey in 1658.1–3 It also appears to be the first description of a non-inferiority trial, i.e. to assess parity between two treatments. It is, of course, important to acknowledge that terms used in this article such as ‘randomisation’, ‘controlled’, ‘RCT' and ‘non-inferiority trial’ are all modern and possess a specific meaning in the context of today's research methods. To apply these terms to the eighteenth century implies an assumption that understandings were equivalent to today's notions of a fair trial.
Blackrie describes the process by which he managed to enquire about and, ultimately, to replicate Chittick's ‘lixivium’. This journey of discovery appears to have relied upon Blackrie's use of smell, taste, the opinion of patients under Chittick's care alongside his own knowledge of chemistry. There is no evidence that Blackrie ever succeeded in undertaking his randomised comparative trial. Given the scale of the proposal, that is not surprising. It remains uncertain exactly to what extent his published challenge was purely a rhetorical device to support the alleged superiority (or rather equality) of his treatment, a simple ‘thought experiment’ or a genuine call for clinical evidence. Given Blackie's enterprise and industry invested in replicating Chittick's remedy, it is the authors’ opinion that his writing was a genuine appeal for evidence to make a trusted lixivium readily accessible to those most in need. A further ambition appears to have been to dismantle Chittick's lucrative business.
The challenges of implementing a fair comparison in the eighteenth century are evident in the limited number of trials actually undertaken. Foremost amongst these was Lind's scurvy trial whose participants were stricken Royal Navy sailors under military law. 5 A much more basic example is Sir John Floyer's 1702 comparison of running speed in two boys before and after submerging one in cold water. 21 Evidence suggesting the race was implemented (probably repeatedly) lies in its simplicity, minimal risk of harm and Floyer's certainty in its outcome. 21
At first sight, Blackrie's inclusion of randomisation demarcates his writing from the ideas of Lind,3,5 Hauksbee the Younger4,6 and Reeve. 7 Due to parallels between the first two (not least inclusion of twelve participants), Hauksbee's proposal is considered to have been an influence on James Lind in his design of his 1747 scurvy trial. 4 Two pieces of evidence could also suggest a link between Hauksbee and Blackrie. First is Blackrie's reference to James Jurin (1684–1750) of the Royal Society. 14 Jurin published on smallpox inoculation in the 1720s and was an inspiration for Hauksbee. 5 Second, is Blackrie's choice of the word ‘decisive’ to describe his proposed RCT. ‘Decisive experiment’ was the term chosen by Hauksbee for his proposal 5 and has its roots in the ideas of Lord Francis Bacon (1561–1626).
The reception of Blackrie's posthumous French edition of his book
18
remains unknown. It might be revealing to examine whether his proposed methodology had any influence upon French medical researchers. That question is pertinent because the French version of his ‘mpa#lsquo;Disquisition’ was published in the decade before the 1784 French Royal Commission on Animal Magnetism, one of whose members was Benjamin Franklin. It is of note that Mesmer's 1781 proposal for a comparative trial by randomisation was published in French: Deslon [one of the Regent Doctors in the Faculté de Médecine] proposed [on behalf of Mesmer] a trial in which twenty-four patients were to be divided into two groups of twelve, one group to be treated by ‘ordinary methods’ and the other to be treated by Mesmer… To avoid any later arguments about ‘age, temperament, disease or symptoms’ the patients were to be assigned to the groups by drawing lots—‘… la répartition se feroit par la voie du sort’.
22
Conclusion
Alexander Blackrie was a Scottish apothecary-surgeon who spent most of his working life in the South East of England. His publications reveal an inquisitive, experimental and compassionate mind. He clearly had a good understanding of chemistry, at least in so far as it related to medicine. Blackrie appears to have been held in high esteem by his medical peers: Blackrie's standing with the London medical profession was evidently high, for among the advance subscribers to his [Blackrie's] 1771 [i.e., second and expanded] edition [of the 1766 book] listed in the front of the book are such men as Dr John Fothergill, Dr George Fordyce, Dr William Heberden, Dr William Hunter, Sir John Pringle; and we shall find that [Benjamin] Franklin's use of this drastic lye infusion was later approved by his counselors.
19
Blackrie's enquiry appears to have been motivated by compassion for other sufferers of the terrible ‘gravel and stone’. He bequeaths a fascinating historical example of how illness in a doctor can motivate a personal quest for new treatments. Blackrie serves as an inspirational role model for medical students as a doctor who was comfortable ‘thinking on his feet’ in unfamiliar circumstances, especially inside patients' homes. Here he listened to and showed solidarity with his patients. At every opportunity he made important deductions from inspection, smell and taste as well as learning through informative comparisons, for example comparing how quickly his two liquids dissolved equally-sized fragments of the same urological stone. His enquiring mind and ability to piece together all the evidence before him makes Blackrie an outstanding example of what it means to be the ‘medical detective’. 27 This is all in stark contrast with much modern medical education which increasingly promotes care that is arms-length, algorithmic and technological. Such an approach risks encouraging students to practise ‘medicine by numbers (sequential blood tests) and medicine by pictures (sequential scans)’. 27
Blackrie's proposal is the moment where the notion of a randomised controlled trial reappears (i.e., after George Starkey) in the English language. It also appears to be the first description of a non-inferiority trial. In the annals of independent thinkers who foresaw the value of randomising patients to compare treatments, the name of Alexander Blackrie has been overlooked. In contrast to today's pharmaceutical industry where profit remains the prevailing motivation, Blackrie offers a historical role model for medical students in the form of one doctor's humanitarian endeavour to widen access to treatment for those most in need: Having now brought this valuable secret to light, and put into the hands of the low as well as of the high that medicine which I believe to be of the greatest efficacy against the most painful of all diseases, I sit down with the pleasing reflection, that I have contributed something to human happiness.
16
Footnotes
Acknowledgements
The authors are grateful for comments received from anonymous reviewers, in particular recognition of Blackrie's enquiry as a non-inferiority trial and for suggesting the helpful phrase ‘rhetorical device’.
Authors’ contributions
MC identified source, drafted and submitted paper. SC read and commented upon drafts.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.