
Abstract
George Archibald Grant Mitchell, OBE, TD, MB, ChB, ChM, MSc, DSc, FRCS (1906–1993) was a professor of anatomy at the University of Manchester from 1946 to 1973. He is mainly remembered for his research in neuroanatomy, especially of the autonomic nervous system. He studied medicine at the Aberdeen University, and after qualifying in 1929 he held posts in surgery and anatomy and worked as a surgeon in the Highlands. In 1939, he joined the Royal Army Medical Corps. He was based in Egypt and the Middle East, where he carried out trials of sulphonamides and penicillin on wounded soldiers; in 1943, he returned to England as Adviser in Penicillin Therapy for 21 Army Group, preparing for the invasion of Europe.
Keywords
Introduction
George Archibald Grant (GAG) Mitchell described himself as ‘a surgeon, soldier and academic’. 1 Certainly, his career falls into three parts: his medical education and posts in Aberdeen and the Highlands (1924–1939), his work in the Royal Army Medical Corps (RAMC) on the use of sulphonamides and penicillin (1939–1945) and his appointment as the professor of anatomy at the Manchester Medical School (1946–1973). However, his work during the War is not well known and that is the main focus of this paper.
The University of Manchester holds archives compiled by Professor Mitchell during the 1970s, relating to his wartime work, including the penicillin project. 2 The Manchester Museum of Medicine and Health (MMH) in the Faculty of Biology, Medicine and Health also holds some papers related to historical medical objects, which he donated to the MMH in 1974; one of these, a brass reservoir penicillin syringe (1945), is of special interest and is described in a section below. The Aberdeen University holds a collection of his anatomical publications, mainly in connection with the award of his DSc in 1950. Other information has been gleaned from Mitchell's papers on sulphonamides and penicillin in the Lancet, the British Medical Journal and the published report, Penicillin therapy and control in 21 Army Group (1945). 3
Scotland (1906–1939)
GAG Mitchell, the son of George Mitchell, a market gardener, was born in Portsoy, Aberdeenshire on 11 November 1906. He studied medicine at the Aberdeen University and graduated with first-class honours MB, ChB in 1929. 4 From 1930, he was a lecturer in anatomy under Professor Alexander Low (1868–1950) and also trained in general surgery under Professor John Marnoch (1867–1936) at the Aberdeen Royal Infirmary. 5 After Marnoch retired in 1932, Mitchell continued as a lecturer in surgery under neurosurgeon Professor James Learmonth (1895–1967), whose research on surgical sympathectomy stimulated Mitchell's interest in the autonomic nervous system (ANS). 6 In 1934, a year after he married Mary Gumming, he was asked to take over as resident surgeon in Caithness, part of the Highlands and Islands health scheme, a post which tested his surgical skills across the full range of specialities! The plan was that after 4 years he would re-join the surgical department; however, Learmonth had left in 1938, and any vacancy had lapsed. Fortunately, Robert Lockard (1894–1987), the new professor of anatomy at Aberdeen, was able to appoint Mitchell as a senior lecturer in anatomy – his future career was set. 7
World War II and North Africa (1939–1943)
Mitchell was already in the Territorials when he was called-up in 1939 to join the 15th (Scottish) General Hospital based in Aberdeen and was then posted to Cairo to help set up the No. 1 Orthopaedic Centre. The Hospital was a new building on the banks of the Nile, described by General Percy Tomlinson (1884–1951), as the ‘Millbank of the Middle East’, reserved for serious cases, with special units for orthopaedics and neurosurgery and was the main military hospital for the Middle East Force, which was embattled with General Rommel's troops in the Desert of North Africa. 8 Casualties from the El Alamein and other battles received immediate surgery at the forward base and mobile hospitals and then were evacuated to Cairo. Later Mitchell was transferred to the 42nd General Hospital in the Desert as Officer Commanding Surgical Division, and still later, as temporary Colonel, took charge of a 600-bedded hospital in Lebanon. 9
His earlier publications dealt mainly with sulphonamides and topical antiseptics. In 1941, he co-authored a report on the causes of infection and poor outcome among 700 injured soldiers, admitted from forward hospitals, who had been treated with sulphonamides. He stressed that antibiotics were no substitute for careful surgery and that ‘failures were due to incomplete or too late excision of damaged tissues, the presence of foreign bodies, tight suturing, insufficient drainage, or lack of rest; the liberal use of sulphanilamide did not neutralise the neglect of these cardinal points’. 10 He noted that the oral dose varied considerably and those on larger doses had less sepsis, he recommended a standardised regime of sulphanilamide, 4.5 g thrice daily, with sulphanilamide powder applied to the wound. However, he found that oral sulphonamides were less effective in staphylococcal infections, for which, ‘pending an adequate supply [of penicillin]’, he recommended proflavine powder mixed with a topical sulphonamide for open infected wounds. 11
In 1944, Lt. Col. Mitchell and others tested two new German sulphonamides, marfanil and prontalbin (prontosil), which had been captured in Desert battles. They were not inhibited by pus, and marfanil was found to be the most effective sulphonamide to treat infected wounds and burns. Mitchell stressed that although penicillin was more ‘uniformly successful in controlling wound infection’ it would not be available in large amounts for some time, and ‘many of the wounded…will have to be treated by less efficient substances’. He argued that marfanil was the best candidate so far, although it also was only available in limited amounts. 12 This work on sulphonamides would have been an important consideration for his later promotion as ‘adviser in penicillin for 21 Army Group’.
Penicillin in North Africa (1942–1943)
The general history of penicillin is complex. 13 This section is just a brief precis of the trials of penicillin in North Africa during 1943. Although Alexander Fleming (1881–1955) had discovered the antibiotic effect of penicillin in 1928, its clinical use was not practicable until Howard Florey (1898–1968) and Ernst Chain (1906–1979) had produced pure penicillin at Oxford. 14 In 1940, their team established the safety and chemotherapeutic properties of penicillin in animals. 15 Further experiments on the production and pharmacology of the drug were followed by clinical trials in a few patients with life-threatening infections, including a ‘hopeless case’ of meningitis, successfully treated by Fleming with intrathecal penicillin. 16 By 1943, further trials showed that it could be safely given by mouth, intravenously or intramuscular injection, and independent research in Egypt by pathologist, Lt. Col. Robert Pulvertaft (1897–1990) proved it was also effective for the topical treatment of wounds and burns. 17
The next stage was to test it on soldiers with septic wounds. A small amount of penicillin produced by ICI Dyestuffs in Manchester was available to the Army; Professor Florey and Brigadier Hugh Cairns (1896–1952), consultant neurosurgeon to the Army, decided to test its use under battlefield conditions in North Africa. They needed to develop standard dosage regimes and methods of delivery for different types of injury. Their findings were detailed in a confidential report for the War Office, Investigation of War Wounds. 18 During 1942, they visited various military hospitals across Egypt and North Africa. The penicillin trials were organised by surgeon Lt. Col. Ian Fraser (1901–1999) and pathologist Major Scott Thomson (1909–1992) at selected forward base and specialist hospitals. They monitored the bacteriology, clinical outcome and reports on how the penicillin was used in over 300 wounded soldiers. 19 At this stage, Mitchell's exact involvement in the penicillin trials is unclear; he was still based in Cairo and probably not directly involved with the trials at the forward base hospitals; however, he was asked to provide reports on the bacteriology and outcome of 163 infected compound fractures, which were not treated with penicillin – a fifth still unhealed after 3 months. 20
The recommendations of Florey and Cairns were clear; wound infection was the main factor in preventing recovery and discharge. Penicillin was an effective treatment and ‘should be used in the first instance for the early treatment of wounds and fractures at the Forward Base’. Parenteral treatment was better than topical application, and an allocation of 750,000 units should be made for each casualty. Finally, the RAMC would need an official manual about dosage regimes, treatment techniques and so on. A War Memorandum, The Use of Penicillin in Treating War Wounds (1944), was issued by the Penicillin Clinical Trials Committee. 21 In a few pages, it set out instructions on the use of penicillin for burns, soft tissue wounds, gas gangrene, compound fractures and injuries to the chest, abdomen, head and eyes. Local treatment might be adequate for burns and simple wounds; otherwise a course of intramuscular injections (15,000 units, 3-hourly injections) or an intravenous saline drip (120,000 units in 24 h) should be given. However, penicillin was scarce and to avoid waste, the supply and storage should be strictly controlled by a ‘pathology penicillin officer’ and in addition, a ‘surgical penicillin officer’ should be appointed for ‘each theatre of operation’ to oversee its clinical use.
Adviser in penicillin therapy for 21 Army Group (1943–1945)
The post of ‘surgical penicillin officer’ was critical to ensuring the correct and economical use of penicillin by the RAMC. Florey and Cairns defined the necessary qualities:
he should be an officer with extensive experience of wounds in the war with experience of penicillin. He would visit surgeons of the Command, demonstrate the use of penicillin, see that it was suitably used, and that the hospital was adequate. He should keep himself informed of all technical developments of the use of penicillin. 22
Mitchell was an experienced surgeon and well regarded for helping to set up the hospitals in North Africa (promoted to temporary Colonel during this period). His academic background and work with sulphonamides placed him in a good position for the post. He had a good working relationship with his chief in Cairo, Colonel Arthur Porritt (1900–1994), a London surgeon at St Mary's Hospital who had served in France and was later posted to Cairo. 23 In December 1943, both men were recalled to England to join the 21 Army Group. General Montgomery (1887–1976) promoted Porritt to Brigadier and ‘Consultant Surgeon to 21 Army Group,’ and Mitchell was appointed as ‘Adviser in Penicillin Therapy to 21 Army Group’. The 21 Army Group, established in July 1943, included British, Canadian and Polish troops training for the invasion of Normandy under the command of General Montgomery. Together with the United States Army, under General Dwight Eisenhower (1890–1969), they formed the Supreme Headquarters Allied Expeditionary Force, a vast army formed for Operation Overlord, the invasion of Europe. Mitchell's job was to educate the 21 Army medical officers in the correct use of penicillin for a range of different injuries. The lectures, demonstrations and memoranda were later published in an 80-page booklet Memorandum on Penicillin Therapy. 24 Porritt's introduction made it clear that the booklet was mainly written by Mitchell; he stated, ‘the symposium… is rightly headed by the Adviser in Penicillin and Chemotherapy’. It was intended as a practical guide, based on its ‘intensive use in this theatre of war’.
Mitchell's 50-page paper described the properties of penicillin followed by a detailed account of its use for all types of injuries and infections. Local application of penicillin was useful for soft tissue wounds or burns; however, more serious injuries required parenteral treatment. Three-hourly injections were painful and unpopular; Mitchell recommended an intramuscular penicillin drip as ‘simple, safe, almost painless’ – 100,000 units in 500 ml of saline, given by needle into the vastus lateralis or the pectoralis muscle from a ‘time-marked bottle’ would last for 24 h. Penicillin should be given to every injured soldier to prevent sepsis: ‘given its proper place in the campaign to fight a malady it is capable of turning defeat into victory and, this is all important, if the hostile organisms are susceptible to penicillin’. However, penicillin is no substitute for good surgical practice; as Mitchell stressed in his introduction, ‘it is not a panacea for every infection, adequate surgery and medical treatment are still essential, and the lavish expenditure of any chemotherapeutic agent will not purchase an indulgence for therapeutic sins’; prompt and careful surgery can save a life or a limb. 25 The Memorandum continued with a detailed section on correct surgical techniques for treating wounds and additional reports by specialists on dermatology, ophthalmology, venereology and laboratory techniques. 26
By June 1944, penicillin was being produced on an industrial scale in the United States. 27 The Allied invasion of Normandy included 8000 doctors, tons of medical equipment, 600,000 doses of penicillin and 50 tons of sulphonamides. 28 Mitchell landed in Normandy on D-Day, and was operational in North-East Europe until 8 May 1945, when hostilities ceased. 29 Shortly after, Porritt and Mitchell produced Penicillin therapy and control in 21 Army Group, 60 chapters authored by RAMC officers, including seven by Porritt and Mitchell, reporting the results of surgery and new techniques. 30 The publication was a record of the work of the RAMC staff in the field; an appendix of the surgical results validates their efforts: total cases, 50,201; deaths, 2564; recovered, 94.9%.
Professor of anatomy (1946–1973)
After Mitchell was discharged in January 1946, he received a phone call from Professor JSB Stopford (1888–1961), Vice-Chancellor of Manchester University, asking if he would be interested in the chair of anatomy. 31 He was appointed as professor in October 1946 to replace Frederic Wood Jones (1878–1954). 32 The Medical School, indeed the whole University, had to adapt to severe constraints during the War, and Stopford (a former professor of anatomy) had extensive plans for the post-war development of the University. Professor Mitchell's brief was to restore normality to the undergraduate anatomy course, build up the staff and establish a viable research programme (Figure 1). 33
Professor GAG Mitchell c.1960s (photograph and permission from the University of Manchester MMH).
The Victorian Medical School (1873) had been refurbished during the 1930s. 34 The dissection room (DR) was a large and well-lit room on the top floor and one of Mitchell's first acts was to replace the old dissection tables and ban smoking in the ‘DR’. 35 Each cadaver was allocated four students who were tutored by demonstrators (studying for the FRCS exam) and tested each month by viva voce. The students had access to a large anatomy museum and also had additional lectures on systematic anatomy. 36 Notable members of the staff included Eugenia Cooper (1898–1991), lecturer in histology (1923–1965), recognised for her research on the endocrine glands and nervous system. 37 Thom Ashley (1913–1972) was a lecturer in embryology (1946–1972), and Edward Louden Patterson (1910–1980), the senior lecturer, was a comparative anatomist and interested in the ANS and blood supply of nerves. 38
Professor Mitchell was indefatigable in his research on the ANS; between 1935 and 1955, he published over 25 papers on the autonomic nerve supply to the main organs of the body, which was the basis for his DSc awarded by Aberdeen University. 39 The papers were compiled in his monographs, Anatomy of the Autonomic Nervous System (1953) and Cardiovascular Innervation (1955), both beautifully illustrated by a medical artist, Dorothy Davison (1809–1984). 40 His research workers included Edward Samuel (1921–1962), who helped to develop silver staining techniques for nerves and Roger Warwick (1912–1991), who worked on the parasympathetic and oculomotor nerves of the eye. 41 Dr David (‘Dan’) Hoyte (1923–2004) 42 joined the staff in 1952 to research the embryology of the craniofacial bones. His obituary of Mitchell provides some insights into the Department; he described Mitchell as ‘supportive,’ the research was of ‘high calibre,’ and the staff, ‘a melange of personalities, ideas, wit, and friendship’. Professor Mitchell was of course involved in many activities related to the University and anatomy: dean of the medical school (1955–1960); pro-vice chancellor (1959–1963); president of the Anatomical Society (1961–1963); president of the Manchester Medical Society (1964–1965) member of the board of governors of the United Manchester Hospitals, and president of the International Anatomical Nomenclature Committee.
The senior author's (PDM) personal experiences of the department was as one of three ‘intercalated’ BSc anatomy students (1966–1967). We had our own small research room and the assistance of a helpful technician. I was fortunate to have Professor Mitchell as my tutor and he also taught the group neuroanatomy. 43 Dr Patterson ran tutorials on comparative anatomy and was a supervisor for my research project on the vagus nerve, always helpful and a vast source of anatomical knowledge. 44 The course included practical histology, electron microscopy and genetics taught by Dr Alan Emery. 45 The teaching and supervision were excellent, but the schedule was tight and we were expected to keep up, and not waste time or materials.
Mitchell's reservoir penicillin syringe
Professor Mitchell was enthusiastic about medical history. 46 During the 1970s, he worked with Dr Frederic Beswick (1925–2019), dean of the Medical School, and architect Harry Fairhurst (1925–2011) to include medical history museum display cabinets in the new Stopford Medical School Building (1973) 47 . Mitchell asked members of the Manchester Medical Society to donate old medical equipment and he donated his own collection of medical objects, one of which was a RAMC brass penicillin reservoir syringe, which is now on display in the Stopford Building foyer, home to the Medical School and MMH.
Working conditions were extremely difficult in the forward hospitals during the invasion; Harriet Low, an army staff nurse in Normandy, recalled, ‘I will never forget the bombing while we were there. At night, I used to lie on my tummy and watch the gunfire lighting up the sky’; so it is not surprising that glass syringes were easily broken and difficult to use for injections in the dark. 48 Lt. Col. Norman Logie RAMC (1904–1972), who was in one of the forward hospitals in Normandy, designed a metal reservoir syringe that could hold 20 cc of penicillin and was fitted with two valves, which allowed injections of exactly 1 cc to be given, even in a complete blackout (Figure 2). Major TJ Burness 49 of the Royal Electrical and Mechanical Engineers (REME) made the first model from an old telescope tube and called it ‘D.39’ meaning 39 days after D-Day. More syringes were improvised from other sources – Mitchell's was made from the oilcan of a Bren gun, and kept in a box marked ‘REME Product Type D.52 MK II’. 50 The total number of syringes made is not recorded – Mitchell's is the only one known to have survived. 51
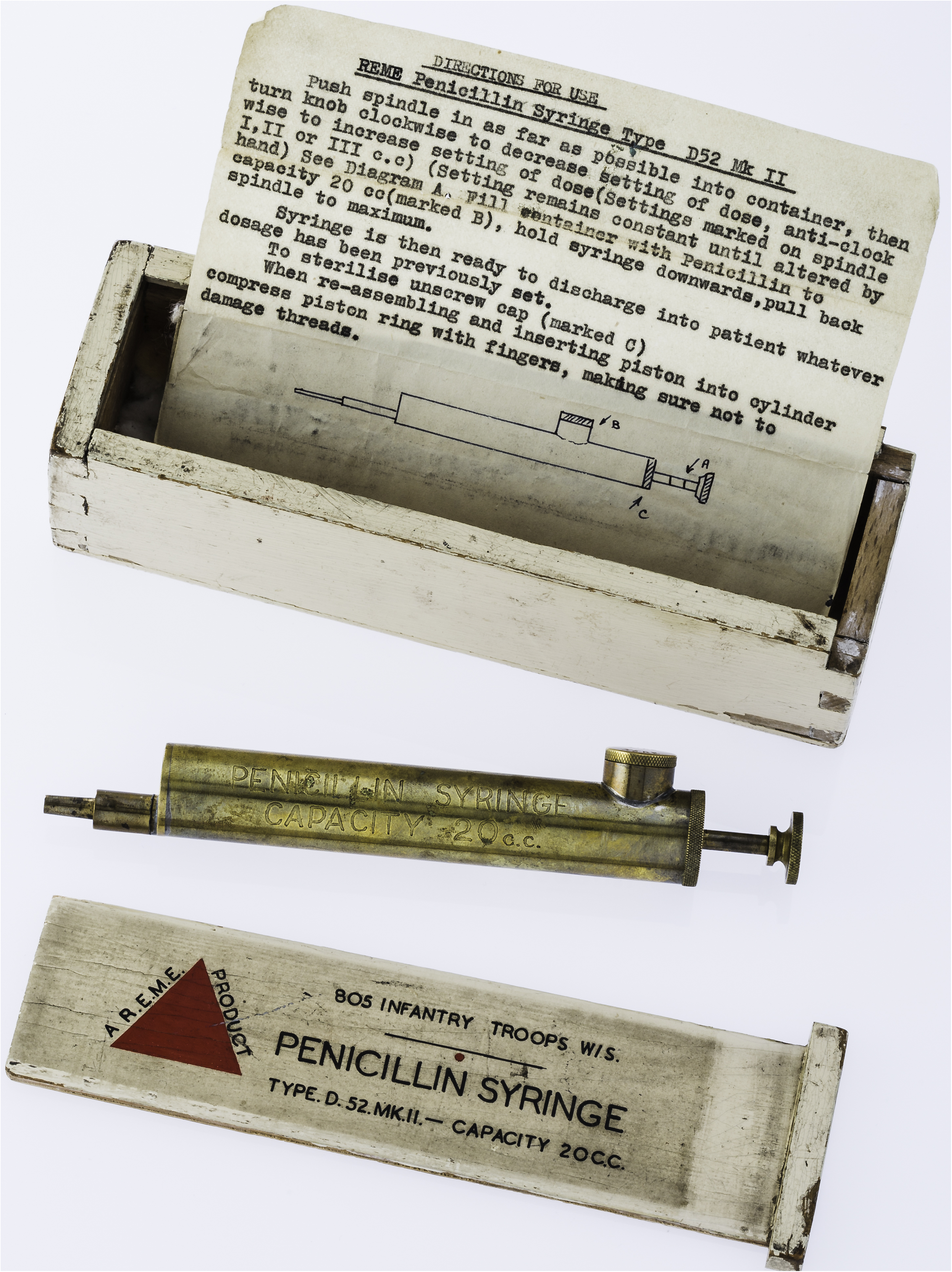
Reservoir penicillin syringe (1945), storage box and instructions. ‘D.52’ means it was made 52 days after D-Day (photograph and permission from the University of Manchester, Manchester Museum of Medicine and Health).
Discussion and summary
Those planning the Allied invasion were well aware of the high mortality from septic wounds. Penicillin was seen as an essential part of the RAMC plans, not just to reduce mortality but also to return injured soldiers to fighting fitness and boost morale.
Why was Mitchell chosen as penicillin adviser? There were other RAMC officers who had used penicillin during Florey's trials. Lt. Col. Pulvertaft had even manufactured his own crude penicillin; however, he was not a surgeon dealing with major injuries. Lt. Col. Ian Fraser was favoured by Florey, but instead he took command of the forward hospital at Bayeux. As already outlined, Mitchell had all the necessary qualities. He and Porritt had worked closely in Cairo since 1941, and when Porritt was promoted to Consultant Surgeon, he would have requested Mitchell as the Adviser in Penicillin.
It is important not to exaggerate Mitchell's contribution to the penicillin project. He was a key member of a complex organisation; however, there were thousands of RAMC staff involved, not only with penicillin but with other projects – blood transfusion, triage, sea and air evacuation, forward nursing teams and supplies, all had their ‘Advisers’.
Penicillin was only an adjunct to good surgical treatment, but conditions could be challenging – the penicillin syringe is a testament that even giving an injection could be problematic. What Mitchell provided was a set of clear guidelines for those operating under battle conditions. The policy of giving every injured soldier a course of penicillin saved time, prevented sepsis and helped to streamline the management from admission to evacuation. Porritt summed up Mitchell's contribution:
In particular I would mention Lt. Col. GAG Mitchell (Adviser in Penicillin and Chemotherapy), to whom chief credit for this brochure should rightly go, as by his sound common sense policy, his clear and astute direction and his engaging, cheerful personality, he has provided the incentive which has made the work so easy, for so many for so long. 52
The skills required by a career anatomist include attention to detail, precise description, technical expertise and careful observation. Mitchell brought these qualities to his work during the War and later as professor of anatomy. He revitalised the Department and during the 1960–1970s, supported the introduction of a new integrated curriculum and helped in the design of the new Medical School. He retired in 1973, the year the Stopford Building opened. The MMH was established mainly by the joint efforts of the dean, Dr Beswick and Professor Mitchell. The Stopford Building no longer has the old-fashioned foyer display cabinets, they were dismantled in 2011 to make way for an increase in students, but the MMH is now actively engaged in educational projects and loans for exhibitions in the University, community, schools and other museums.
Footnotes
Acknowledgements
The authors are grateful to University of Manchester archivist James Peters for his help with Professor Mitchell's records.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.