
Abstract
Massive cerebral infarction (MCI) is a life-threatening disease and may lead to cerebral herniation. Neutrophil degranulation contributes to ischemic injury in the early stage. To investigate whether neutrophil degranulating factors can predict cerebral herniation and the long-term prognosis of patients with MCI and to investigate the relationship between neutrophil degranulation and blood brain barrier (BBB) damage. In this case-control study of 14 MCI patients, we divided the patients into a cerebral hernia group and no cerebral hernia group according to whether they developed cerebral herniation within 5 days. The prognosis of MCI patients was assessed using the Modified Rankin Scale (mRS) score at 6 months, which was the primary end point. The composition of white blood cells (WBC) and degranulating factors for neutrophils in the plasma of MCI patients was determined on days 2 and 4. Baseline characteristics were comparable in both groups. The neurological functional scores and long-term prognosis showed no difference between patients with or without cerebral herniation, while the mortality rate of the cerebral hernia group in the short term was higher (P < 0.05). The WBC count, neutrophil to lymphocyte ratio (NLR) and plasma myeloperoxidase (MPO) levels of patients with cerebral hernia were significantly higher than those of patients without cerebral hernia (all P < 0.05). MPO is a better predictor of cerebral herniation, and the NLR showed superior predictive value in the prognosis of MCI patients. neutrophil degranulation may play an important role in malignant cerebral hernia during MCI. These data suggest that, MPO and the NLR might be predictive factors for cerebral herniation and the prognosis of MCI patients.
Keywords
Introduction
Massive cerebral infarction (MCI) is a common type of severe cerebrovascular disease that may cause cerebral herniation within a week after its onset 1 –3 . Unfortunately, the diagnosis of cerebral hernia currently still relies on medical imaging, which has limitations in timeliness 4 . Moreover, 70%–80% of MCI patients die from cerebral herniation in a year even after timely treatment 5,6 . We need to identify patients who will develop cerebral herniation, as well as patients who may benefit from aggressive and expensive therapies. However, studies on MCI have mainly focused on the occurrence of complications and neurological outcomes in the short term. In the present study, we performed a case-control study with a small sample size to identify predictive factors for the long-term prognosis of MCI patients.
Ischemic stroke, especially MCI, may cause a local inflammatory response, and multiple immune cells are recruited to the brain parenchyma in an orderly manner 7 . Neutrophils are the first leukocyte subset to appear in the ischemic brain and can be detected 15–60 min following reperfusion 8 . In addition, it has been reported that the early infiltration of neutrophils might be a hallmark of cerebral ischemic injury 9 . The degranulation of neutrophil toxic products has been regarded as a detrimental response in both acute and chronic diseases. Different neutrophil products, such as neutrophil elastase (NE) and myeloperoxidase (MPO), are stored in different neutrophil granules prone to release on demand 10 . Once released and activated, the enzymes released from neutrophils will further participate in the pathological process of cerebral ischemia, which might be critical to the progression and prognosis of cerebral ischemia 11 . In addition, the degranulation of neutrophils may lead to activation of the fibrinolytic system, leading to damage to the blood-brain barrier (BBB) and aggravating cerebral edema. The neutrophil to lymphocyte ratio (NLR) represents the proportion of neutrophils in inflammatory cells, and the release of NE and MPO represents the activation of neutrophils. Cellular fibronectin (cFn), one of the components of BBB and urokinase plasminogen activator receptor (uPAR), a factor of fibrinolytic system, were also detected.
This prospective study investigated the degranulating factors for neutrophils, including NE and MPO, together with NLR, that are predictive of cerebral herniation and the long-term prognosis of patients with MCI.
Materials and Methods
Patient Inclusion and Clinical Variables
This case-control study enrolled 14 patients diagnosed with acute MCI admitted to the neuro-intensive care unit (NCU) of Xuanwu Hospital in Capital Medical University from January to December 2018. The patients were diagnosed in accordance with the guidelines for the management of large hemispheric infarction by senior neurologists upon admission. The inclusion criteria were as follows: (1) age between 18 and 80 years; (2) MCI confirmed by head computed tomography (CT) or magnetic resonance imaging (MRI); and (3) unilateral MCI involving at least 2/3 of the MCA territory within 48 h of MCI onset. The exclusion criteria were as follows: (1) severe bleeding tendency, active bleeding, or the presence of hematological system diseases; (2) severe infection; (3) malignant tumors and renal or liver failure; (4) major surgery within half a year; or (5) modified Rankin Scale (mRS) >2 points before onset. The patients were recruited consecutively. In addition, as a control group, 14 healthy people aged 50 to 80 years were recruited into this study as volunteers.
The present study was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University. Informed consent was obtained from patients or their guardians. All patients underwent standardized treatment according to the Chinese Expert consensus on the Monitoring and Treatment of Large Hemisphere Infarction published in 2017. Some patients were treated with decompressive craniectomy according to the indications for surgery and whether the patients or their guardians were informed. Fourteen MCI patients were divided into a cerebral herniation group and a no cerebral herniation group based on whether they developed cerebral herniation within 5 days of onset.
Clinical Assessment and Data Collection
The baseline data, including the demographic characteristics, risk factors, and clinical features, were recorded as soon as the patients were admitted. All patients underwent standard neurological and blood assessments at 2 and 4 days after onset. The National Institute of Health Stroke Scale (NIHSS), Glasgow Coma Scale (GCS), and modified Rankin Scale (mRS) were used to assess the neurofunctions of the MCI patients. The white blood cell (WBC), lymphocyte and neutrophil count representative in neutrophil-activating, moreover, the degranulating factors for neutrophils, including NE and MPO in plasma, were detected to reflect the degranulation of neutrophils in MCI patients, and uPAR, cFn represent the activation of fibrinolytic system. The occurrence of cerebral herniation 5 days after stroke was regarded as the first but not the primary end point. Follow-up was performed at 3 and 6 months after onset, and the prognosis of the patient was assessed using the mRS score, which was the primary efficacy end point. Patients with an mRS score of no more than four were considered to have a good prognosis. Conversely, patients with mRS scores greater than four were considered to have a poor prognosis. The follow-ups were conducted by an investigator who was not involved in the inclusion and treatment of patients.
Detection of Clinical Biochemical Indexes
Blood samples from MCI patients were collected into an EDTA anticoagulant vacuum tube by venipuncture at day 2 after ischemia and immediately preserved at 4°C for routine laboratory assays. Blood samples (2×4ml samples per patient) were immediately centrifuged at 200× g for 10 min at 4°C, and the supernatant was retained as plasma for subsequent biochemical detection.
Enzyme-Linked Immunosorbent Assay
MPO and NE levels in the plasma were measured using a human enzyme-linked immunosorbent assay (ELISA) kit (Xinbosheng, China); UPAR levels in the plasma was measured using ELISA Kit for human uPAR (No. SEA141Hu) (Cloud-Clone Corp, Wuhan, China); cFn levels in the plasma were measured using a human cFn ELISA kit (No. CSB-E11850 h) (Cusabio Life Science, Wuhan, China)). The test is carried out according to the instructions.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics 22 software (IBM Corp., Armonk, NY, USA). Data with normal distributions were compared with Student’s t test and expressed as the mean ± SD, while the Mann-Whitney U test was employed to compare data with non-normal distributions, which are expressed as the median (interquartile range, IQR). The ROC curve was used to evaluate the diagnostic performance of the risk factors for cerebral herniation and the prognosis of MCI patients. The difference in the area under the ROC curve was determined to be statistically significant only when P ≤ 0.05.
Results
Baseline and Clinical Manifestation
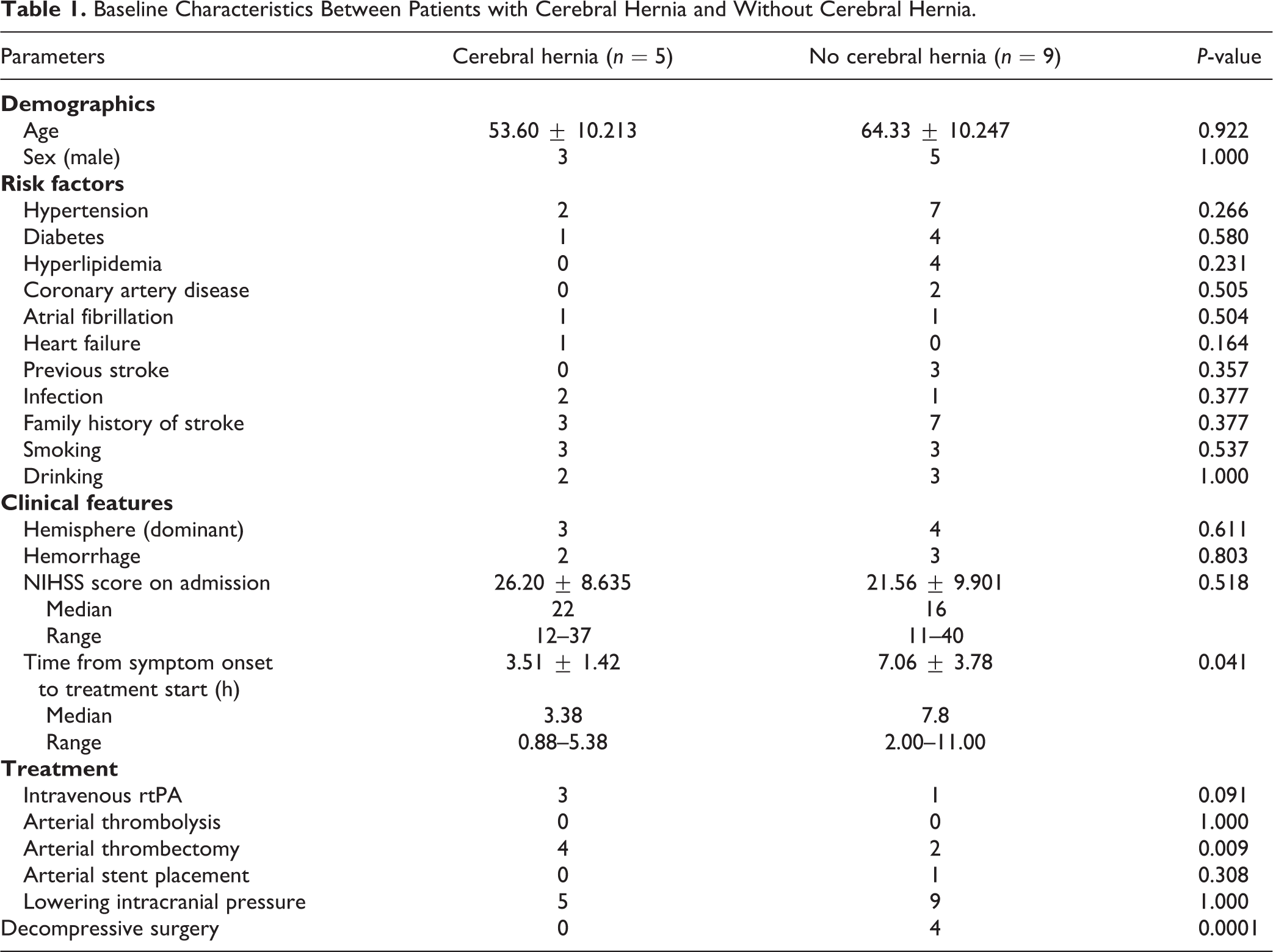
A total of 14 MCI patients were divided into a cerebral herniation group (n = 5) and a no cerebral herniation group (n = 9), and 14 healthy volunteers were enrolled in this study. The baseline characteristics are presented in Table 1. Most individuals enrolled in this study had no significant differences in age, sex, risk factors, or clinical features. However, there were imbalances in the time from symptom onset to treatment start and decompressive surgery between patients with and without cerebral herniation, which might be due to the small sample size and different conditions among the patients.
Baseline Characteristics Between Patients with Cerebral Hernia and Without Cerebral Hernia.
Prognosis of MCI Patients
In this study, the NIHSS score was used to assess neurological deficits of MCI patients at day 14 after ischemia, and the GCS score was used to evaluate the depth of the disorder of consciousness. Although the neurological function of patients without cerebral hernia seemed better than that of patients with cerebral hernia, the outcomes of these two neurological function scores showed no statistically significant difference between the cerebral hernia group (n = 5) and the no cerebral hernia group (n = 9) at day 14 after ischemia (Fig. 1A, B, P > 0.05).
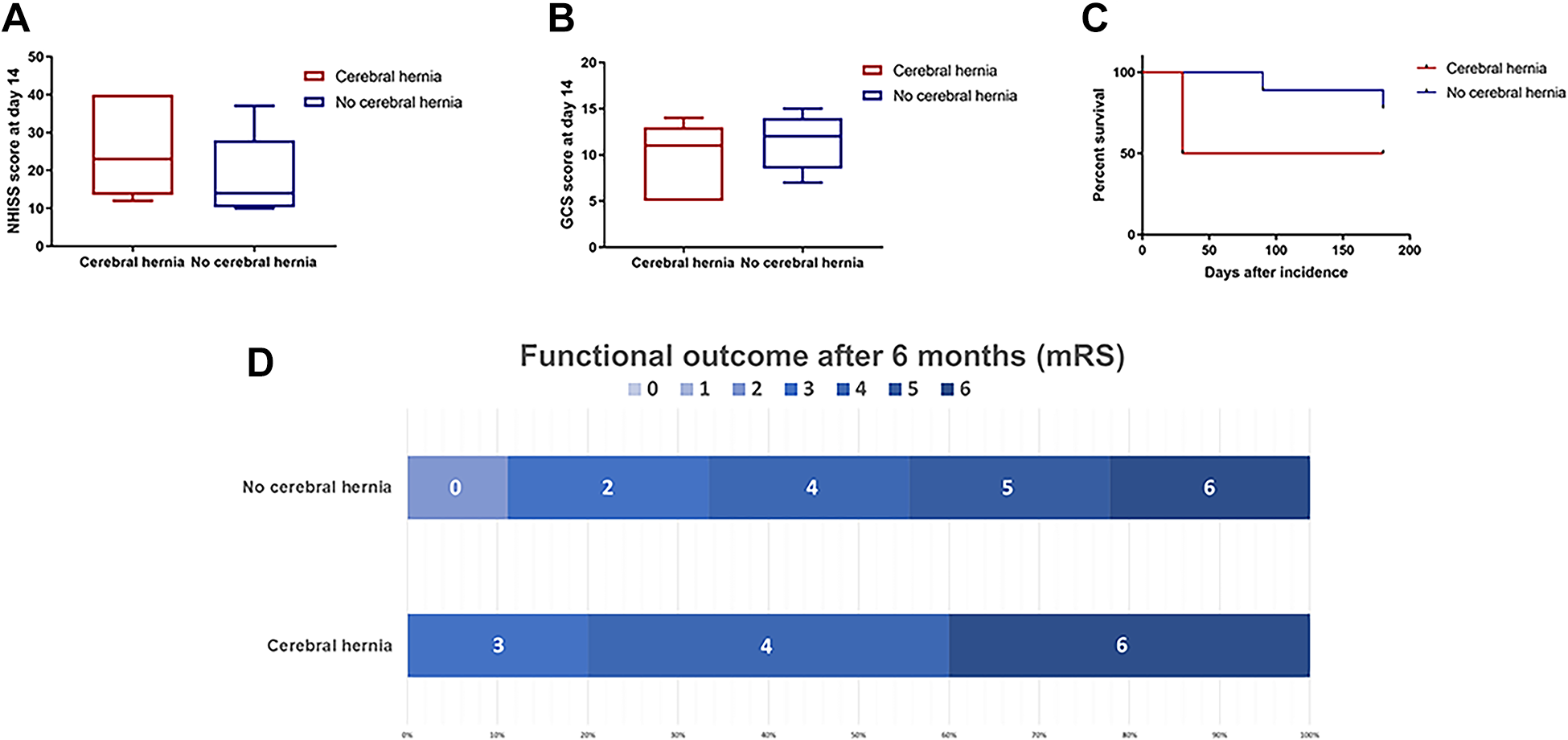
Neurological functional outcomes and survival rate of massive cerebral ischemic patients. (A) NHISS score and (B) GCS score of MCI patients with cerebral herniation (n = 5) or without cerebral herniation (n = 9) at 14 days after ischemia. (C) Survival rate of MCI patients with or without cerebral herniation at 6 months after ischemia. (D) mRS score of MCI patients with or without cerebral herniation at 6 months after ischemia (P > 0.05 compared to cerebral hernia group). GCS, Glasgow Coma Scale; MCI, Massive cerebral infarction; mRS. Modified Rankin Scale.
There was no difference in the survival rate between the cerebral hernia group and the no cerebral hernia group after six months of follow-up; the deaths of two patients with cerebral hernia due to complications both occurred within a month after ischemia, which was earlier than the deaths that occurred in the no cerebral hernia group (Fig. 1C, P > 0.05). There was no significant difference in the prognosis between the two groups (Fig. 1D, P > 0.05). However, these results may be partly attributable to decompressive surgery, which could decrease the mortality rate for cerebral hernia patients and result in better prognosis.
Changes in Immune Cells in the Venous Blood of MCI Patients
Inflammatory responses were substantially involved in neural damage after MCI. The immune system is involved in the inflammatory process that occurs after ischemia, which can be reflected in the changes in immune cells. The WBC count in the venous blood of the control group (n = 14) was much lower than that of MCI patients at 2 days after ischemia (n = 14) (Fig. 2A, P < 0.0001). More importantly, among the MCI patients, the WBC count of MCI patients with cerebral herniation (n = 5) was significantly higher than that of MCI patients without cerebral herniation (n = 9) at 2 days after ischemia (Fig. 2B, P < 0.01), the WBC count of the cerebral herniation group decreased on the 4th day compared with the 2nd day, but the change showed no statistically difference (Fig. 2B).
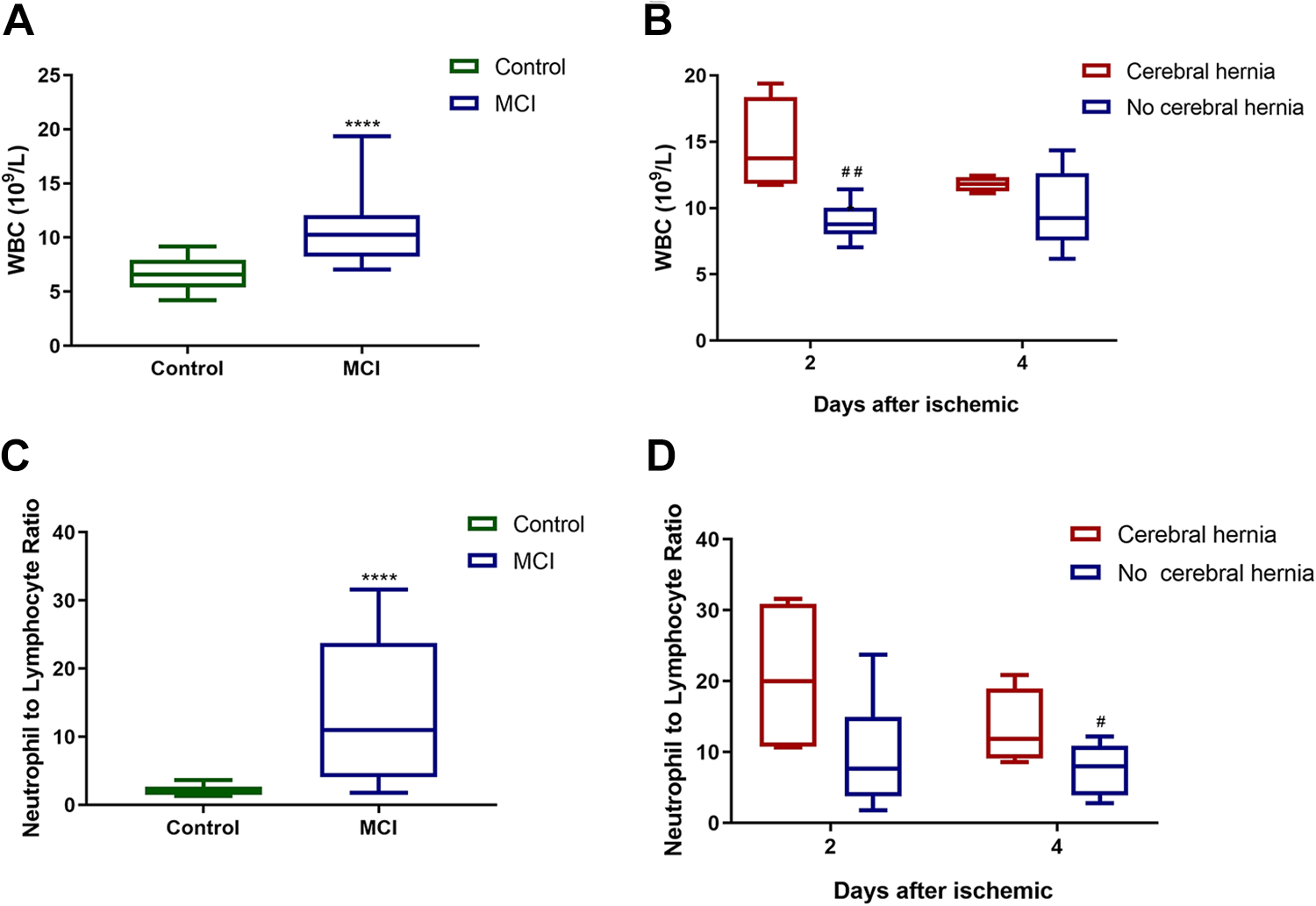
Composition of white blood cells in venous blood of MCI patients. (A) White blood cell count in venous blood of control group (n = 14) and MCI patients at 2 days after ischemia (n = 14). (B) White blood cell count in venous blood of MCI patients with cerebral herniation (n = 5) or without cerebral herniation (n = 9) at 2 days after ischemia. (C) Neutrophil to lymphocyte ratio in venous blood of control group (n = 14) and MCI patients at 2 days after ischemia (n = 14). (D) Neutrophil to lymphocyte ratio in venous blood of MCI patients with cerebral herniation (n = 5) or without cerebral herniation (n = 9) at 2 days after ischemia. (****P < 0.0001 compared to control group, ##p < 0.01 compared to cerebral hernia group). MCI, Massive cerebral infarction.
Furthermore, to investigate the composition of immune cells, we compared the neutrophil to lymphocyte ratio (NLR) in venous blood and found that the NLR of MCI patients was significantly elevated compared to the control group at day 2 after ischemia (Fig. 2C, P < 0.0001). The NLR of cerebral hernia patients was higher than that of patients without cerebral hernia, and the difference was statistically significant on the 4th day (Fig. 2D, P < 0.05), compared with the NLR of cerebral herniation group on day 2, the NLR decreased on day 4, but there was no statistical difference (Fig. 2D).
The Expression of Degranulating Factors for Neutrophils in the Plasma of MCI Patients
In addition to the increase in the number of neutrophils, we also analyzed whether the expression of inflammatory factors related to neutrophil function also changed after ischemia and whether they were related to the neurofunctional deficit of MCI patients.
The distribution of plasma MPO at 2 days after onset was detected by an ELISA kit and is displayed with box plots. The analysis indicated that MCI patients had significantly higher MPO levels than the healthy volunteers (Fig. 3A, P < 0.001), and patients with cerebral hernia produced much higher levels of MPO than patients without cerebral hernia (Fig. 3B, P < 0.001). To assess the role of MPO in stroke severity, we examined the correlation between MPO levels in plasma and neurofunctional scores, and a positive linear correlation was found between MPO levels in plasma and NIHSS score within 4 days of stroke onset (Fig. 3C, P < 0.05).
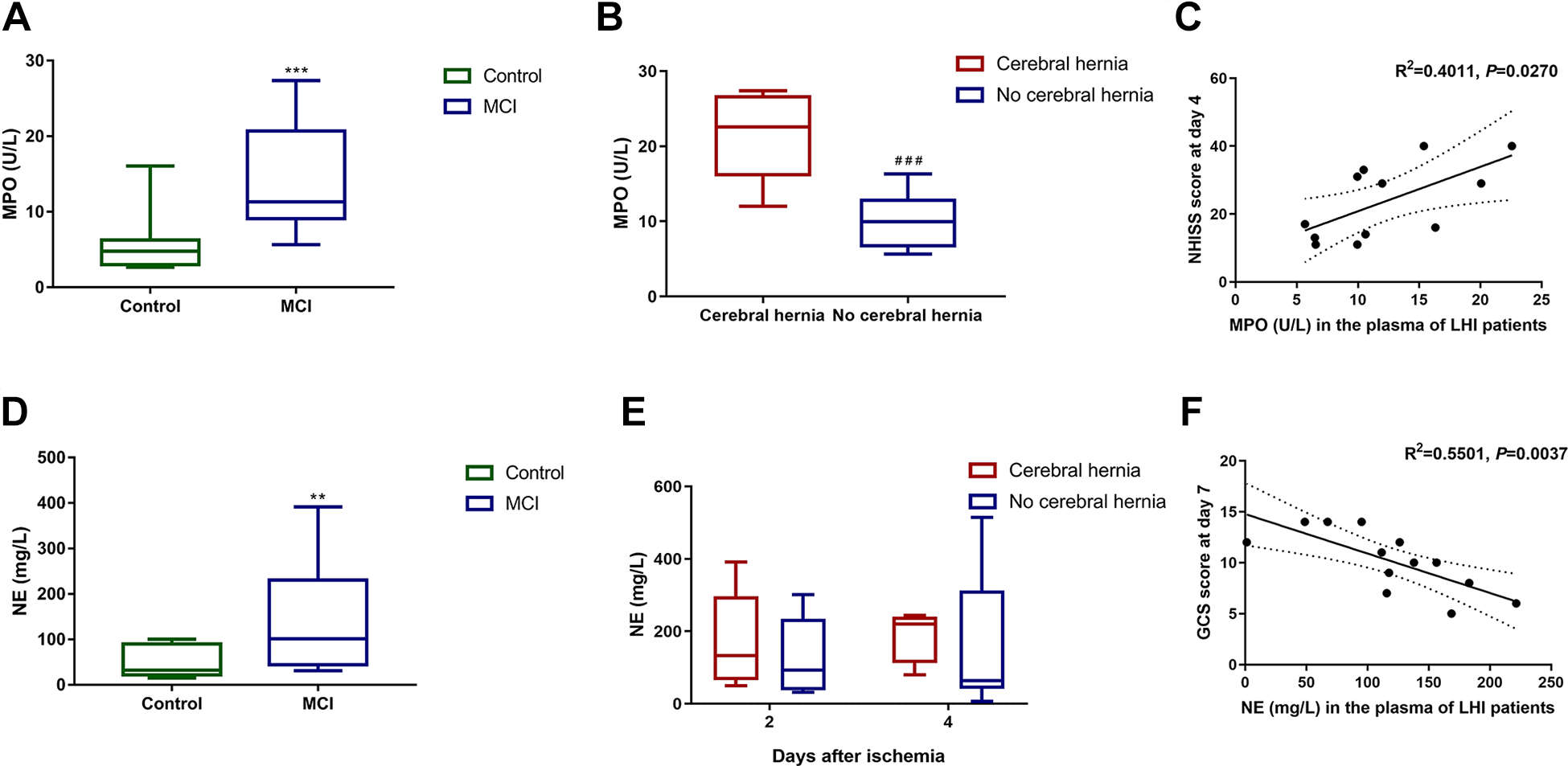
Neutrophil-activating factors in plasma of MCI patients. (A) Myeloperoxidase level in plasma of control group (n = 14) and MCI patients at 2 days after ischemia (n = 14). (B) Myeloperoxidase level in plasma of MCI patients with cerebral herniation (n = 5) or without cerebral herniation (n = 9) at 2 days after ischemia. (C) Correlations between myeloperoxidase levels in plasma and NIHSS score. (D) Neutrophil elastase level in plasma of control group (n = 14) and MCI patients at 2 days after ischemia (n = 14). (E) Neutrophil elastase level in plasma of MCI patients with cerebral herniation (n = 5) or without cerebral herniation (n = 9) at 2nd and 4th day after ischemia. (F) Correlations between neutrophil elastase levels in plasma and GCS score. MCI, Massive cerebral infarction.
NE levels in the plasma of MCI patients and healthy controls were detected using an ELISA kit. The expression of NE was significantly increased (Fig. 3D, P < 0.01). Although the levels of NE in the plasma between patients with or without cerebral hernia showed no difference either on the 2nd day or on the 4th day (Fig. 3E, P > 0.05), NE levels on the 2nd day showed a positive linear correlation with GCS score within 7 days of stroke onset (Fig. 3F, P < 0.05).
Damage of BBB in MCI Patients
Since the degranulation of neutrophil may activate the fibrinolytic system thus lead to BBB damage and aggravate cerebral hernia, we detected the factors related to BBB and fibrinolytic system in the blood of MCI patients.
ELISA kit was used to detect the distribution of plasma cFn and uPAR on the 2nd and 4th day after onset. The analysis showed that the cFn level of MCI patients was significantly lower than that of control group (Fig. 4A, P < 0.01), but there was no significant difference in cFn levels between patients with cerebral hernia and patients without cerebral hernia. The expression of plasma cFn in patients with cerebral hernia on the 4th day was higher than that on the 2nd day, but there was no statistical difference either (Fig. 4B, P > 0.05).
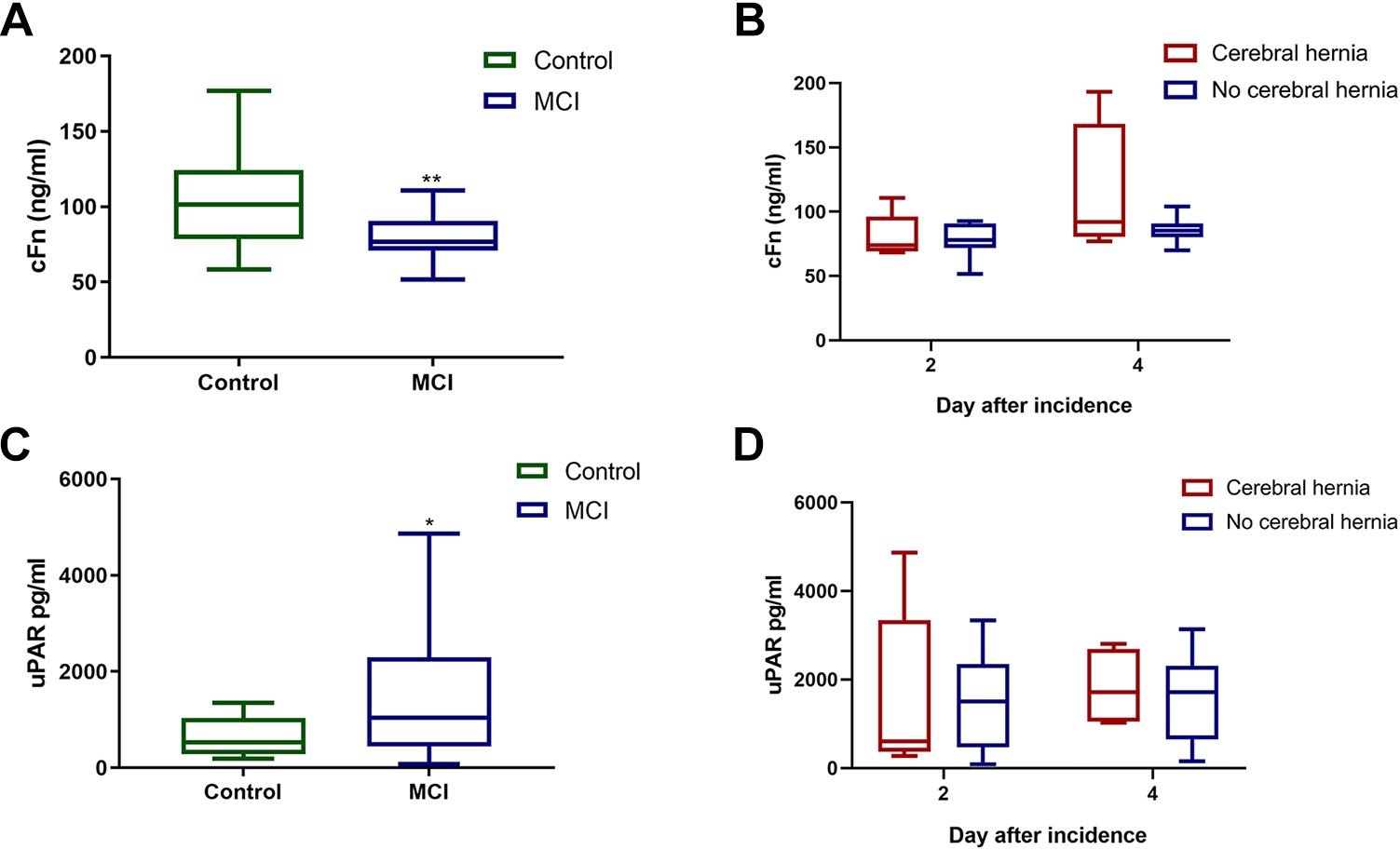
Damage of BBB in MCI patients. (A) Cellular fibronectin level in plasma of control group (n = 14) and MCI patients at 2 days after ischemia (n = 14). (B) Cellular fibronectin level in plasma of MCI patients with cerebral herniation (n = 5) or without cerebral herniation (n = 9) at 2nd and 4th day after ischemia. (C) Neutrophil elastase level in plasma of control group (n = 14) and MCI patients at 2 days after ischemia (n = 14). (E) Neutrophil elastase level in plasma of MCI patients with cerebral herniation (n = 5) or without cerebral herniation (n = 9) at 2 days after ischemia. (F) Correlations between neutrophil elastase levels in plasma and GCS score. MCI, Massive cerebral infarction.
The expression of plasma uPAR in patients with MCI was significantly increased (Fig. 4C, P < 0.05). However, there was no significant difference in plasma uPAR levels between patients with and without cerebral hernia and between different time points (Fig. 4D, P > 0.05).
The ROC Curve of the NLR and MPO
The ROC curve was utilized to evaluate the accuracy of the NLR and MPO levels in plasma as risk factors that predict the occurrence of cerebral herniation caused by MCI. The optimal cutoff value for plasma MPO as a risk factor was 11.3001. The sensitivity of the cutoff value was 100%, and its specificity was 77.8%. The area under the ROC of the MPO curve was 0.9556, which is larger than that of the NLR, suggesting that the MPO level was a superior biomarker for the prediction of cerebral hernia in MCI patients (Fig. 5A, Table 2).
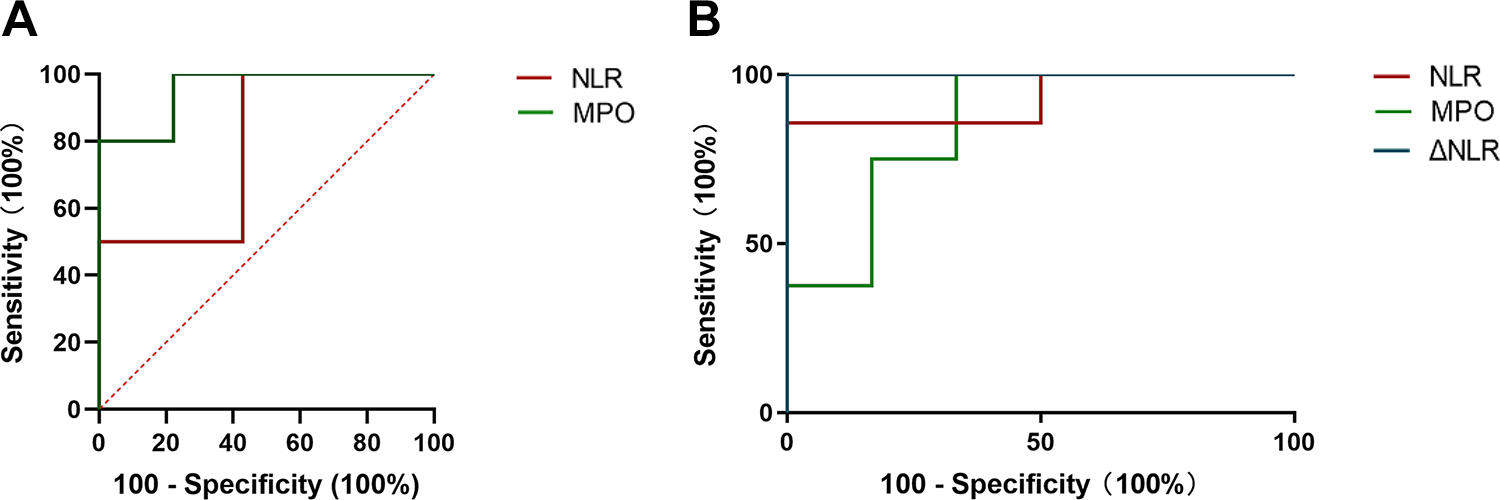
The ROC curves of the NLR and MPO levels in plasma of MCI patients. To evaluate the accuracy of the NLR and myeloperoxidase as risk factors that predict (A) cerebral herniation and (B) the prognosis of MCI patients. ROC= receiver operator characteristic (n = 14). MCI, Massive cerebral infarction; MPO, plasma myeloperoxidase; NLO, neutrophil to lymphocyte ratio.
Prediction of Cerebral Herniation Using the NLR and MPO Levels from MCI Patients Within 2 Days of Stroke Onset.

Furthermore, another ROC curve was produced to evaluate the NLR and MPO levels in plasma as risk factors for predicting the prognosis of MCI patients. The area under the ROC of the NLR curve was 0.85; the optimal cutoff value for the plasma NLR as a risk factor was 10.8278. The sensitivity of the cutoff value was 75%, and its specificity was 100%. The area under the ROC of the NLR curve was 0.85, which is larger than that of MPO, suggesting that the NLR was a superior biomarker for predicting the prognosis of MCI patients. Subsequently, we tried to predict the prognosis of patients with MCI by the changes of NLR (ΔNLR) on the 4th and 2nd day. Interestingly, the sensitivity and specificity of the cutoff value were both 100% and the ROC area under the NLR curve was 1. ΔNLR can accurately predict the prognosis of patients with MCI, but large-sample clinical trials are still needed for further verification (Fig. 5B, Table 3).
Prediction of the Prognosis of MCI Patients Using the NLR and MPO Levels from MCI Patients Within 2 Days of Stroke Onset.

Discussion
Previous studies showed that neutrophil counts in the venous blood of patients with MCI can be predictive of early death due to cerebral herniation after MCI 3 , indicating that the immune response of MCI patients may have an impact on their prognosis. In this study, we established a case-control study with a small sample size of MCI patients for further research and found the following: (1) As an indicator of neutrophil activation, the NLR value in the venous blood of MCI patients with cerebral herniation is significantly higher than that in patients without cerebral herniation. (2) MPO is a marker of neutrophil degranulation, and the expression of MPO in the plasma of MCI patients with cerebral herniation was significantly higher than that of MCI patients without cerebral herniation, which is correlated with neurological function scores in MCI patients as well. (3) The NLR and MPO have a certain predictive role in the occurrence of cerebral herniation and long-term prognosis in MCI patients, among which, MPO is a better factor in the prediction of cerebral herniation, while the NLR, especially ΔNLR is better in the prediction of the prognosis in the early stage.
As a fatal complication of MCI, cerebral herniation leads to a higher mortality rate in the short term. In addition, there was no significant difference in the neurological outcome and long-term prognosis of MCI patients with or without cerebral herniation, which might partly be due to the small sample size. Additionally, decompressive surgery, which has been proposed to reduce the development of cerebral hernia, may improve the prognosis of patients with cerebral herniation. However, over 40% of patients had a poor prognosis in our present study even after receiving decompressive surgery and/or the strongest medical treatments available.
The immune system plays a critical role in the initiation and propagation of ischemic injury. Glial cells develop an inflammatory phenotype in response to ischemia and release mediators that attract neutrophils, monocytes and lymphocytes. The NLR is an indicator of neutrophil activation, and a high NLR has been reported to be associated with the outcome of a variety of conditions. NLR is an independent predictor of mortality in patients with acute coronary syndrome 12 and bacteremia in critically ill patients 13 , as well as the poor prognostic indicator in several malignancies 14,15 . At present, there is also some available evidence between NLR and the clinical outcome of patients with cerebrovascular disease. A significant increase of NLR was found in patients with ischemic stroke, especially in dead patients 16 . NLR was also related with early neurological deterioration of patients with cerebral hemorrhage 17 . Our study indicates that the NLR might be a biomarker for the prediction of cerebral herniation, which has been proven to be a predictor of the short- and long-term outcomes of ischemic stroke 9 .
The increasing NLR in the blood of MCI patients indicated the activation of neutrophils, and as the first immune responder to ischemic brain injury, neutrophils play a complicated role. There is compelling evidence from humans and from experimental animal models that neutrophil influx incites pathological inflammation in multiple conditions 18,19 . The propensity of neutrophils to injure surrounding tissues is intimately related to their activation status 20,21 . After being recruited from the blood to the injured tissues, neutrophils usually clear the infection by phagocytosis, degranulation, and the formation of neutrophil extracellular traps 19 . Neutrophils are generated within a hypoxic bone marrow niche, are exposed to intermittent hypoxia in the circulation and are recruited to the sites of infection and inflammation, which are almost invariably hypoxic, therefore neutrophils are adapted to function in hypoxic environments 22 .
Neutrophils participate in neuroplasticity and increase after stroke 23 , yet it has also been reported that neutrophils may participate in increasing the permeability of BBB, which may lead to cerebral herniation after MCI. Studies have shown that fibronectin is an important factor in promoting neutrophil degranulation, promoting matrix metalloproteinase-9 (MMP-9) secretion, and then decomposing fibronectin to form a negative feedback cycle 24 , which may be one of the reasons for the decrease of plasma fibronectin in MCI patients. MMPs are products of neutrophil degranulation as well. Such enzymes are able to digest collagen and other component of the extracellular matrix, which can further damage BBB integrity and exacerbate oxidative stress 25,26 and play role in the edema development 27 . It is also found that the fibrinolytic system in patients with MCI may be activated by neutrophil degranulation 28 , thus may lead to a damage to BBB. However, in the present study, there is no difference in uPAR levels between patients with and without cerebral hernia, so it is not clear whether the activation of fibrinolytic system affects the occurrence of cerebral hernia and whether it further affects the prognosis of patients with MCI.
In the present study, we recognized that the degranulation of neutrophils corelated with the poor progression of MCI patients. MPO and NE are both factors produced by neutrophils and were increased in the plasma of MCI patients. Both enzymes are stored in the neutrophils’ azurophilic granules and are released following neutrophil activation, resulting in inflammation. However, the release of MPO may lead to oxidative stress, and NE may destroy the endothelium and blood-brain barrier, causing severe damage as well 29 . The levels of MPO and NE in the plasma of MCI patients were significantly increased and were positively correlated with the neurological function scores of patients after MCI. However, only MPO showed a significant difference between patients with and without cerebral herniation.
In summary, our study indicates that plasma MPO is a better predictive factor for cerebral hernia; moreover, the NLR is better than MPO in predicting the prognosis of MCI patients.
Conclusion
The present study indicates that neutrophil activation may play a role in the pathogenesis of malignant cerebral edema during MCI. MPO levels and the NLR could be used as predictive factors for cerebral herniation and the prognosis of MCI patients. However, this study only included a relatively small clinical sample size, and the results should be further validated in subsequent larger-scale studies to explore the clinical potential of these biomarkers.
Footnotes
Author Contribution
Yuyou Huang, and Fangfang Li, are co-first author
Ethical Approval
This study was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Ethics Committee of Xuanwu Hospital, Capital Medical University approved protocols, APPROVAL NUMBER: Clinical Research [2008] No. 1.
Statement of Informed Consent
Informed consent was obtained from patients or their guardians.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Natural Science Foundation of China (81971222, 81671037, 82001390).