
Abstract
The efficacy of melphalan (MEL) 140 mg/m2 pre-transplant conditioning versus MEL 200 mg/m2 for the elderly is still debated. We hypothesized that single-agent intravenous busulfan (BU) would show significant anti-myeloma efficacy and be better tolerated by elderly patients. A prospective 3+3 dose escalation study enrolled symptomatic multiple myeloma (MM) patients 65 years or older with SWOG performance 0–2 for treatment with intravenous BU pre-transplant at different administration levels. The primary objective was to determine the maximum tolerated dose (MTD) of BU that could be safely given over the least number of days. All patients, except one, received maintenance treatment post-transplant, mostly for 2 years. We enrolled 13 patients, mean age of 73 years (range 68–80). Pharmacokinetic analysis showed no greater than 2% accumulation in the 13 patients, confirming a lack of accumulation in the multi-dose regimen. No deaths occurred in the peri-transplant period. Grade 3/4 adverse effects were hematological, no dose-limiting toxicity was observed and MTD was not reached. Three patients developed grade 3 mucositis but none developed veno-occlusive disease. Ten (77%) patients achieved a complete remission (CR) post-transplant with a remarkably long average time to best response of 6.7 months (range: 6–14 m), and two attained a partial response. Median overall survival was 84 months (95% CI, 21–104) and the median progression-free survival was 60 months (95% CI, 9–93). Our results suggest that IV BU could be an alternative conditioning regimen to MEL 140 in elderly patients with MM, and supports future randomized trials.
Introduction
Multiple myeloma (MM) is a clonal plasma cell disorder with significant morbidity and mortality 1 . High-dose chemotherapy and autologous stem cell transplant continues to be the standard of care for transplant-eligible patients with MM. High-dose chemotherapy with autologous stem cell transplantation is associated with improved response rates and progression-free survival (PFS) even when compared with patients treated with a proteasome inhibitor and immunomodulatory imide (IMiD) treatment 2,3 . Intravenous melphalan at a dose of 200 mg/m2 (MEL 200) is the standard conditioning regimen for patients receiving autologous stem cell transplantation for MM. However, elderly patients treated with MEL 200 have increased treatment-related morbidity and mortality. Badros et al. reported an increase in transplant-related mortality of 16% with the MEL 200 regimen in patients above 70 years, leading to the recommendation for a dose reduction to 140 mg/m2 (MEL 140) for these patients 4 . MEL 140 has become the standard conditioning regimen for patients aged >70 years or with severe renal dysfunction. However, there have been no randomized controlled trials comparing these two dose levels and retrospective studies have shown mixed results. In a retrospective analysis, Saunders et al. compared the outcomes of 63 patients treated with MEL 140 and 252 patients treated with MEL 200. Even though overall response rates and PFS were similar between the two groups, the rates of complete responses and overall survival were significantly lower for the MEL 140 group 5 . However, a similar study by Katragadda et al. on 33 patients with MEL 140 and 96 patients with MEL 200 showed no significant difference in treatment-related mortality, relapse-free survival or overall survival between the groups 6 .
Busulfan is a bifunctional alkylating agent widely used as a component of conditioning regimens for autologous and allogeneic stem cell transplantation. Oral busulfan, as a single-agent conditioning regimen in MM, had an overall response rate of 46% with three treatment-related deaths of the 15 patients on the study 7 . However, oral busulfan showed significant inter-patient pharmacokinetic variability, and higher levels have been associated with increased veno-occlusive disease (VOD) and transplant-related mortality 8 –10 . The introduction of intravenous busulfan and therapeutic drug monitoring have ensured safer administration and resulted in tolerable toxicity profiles. Numerous studies in MM have used both oral and intravenous busulfan as a conditioning regimen in combination mostly with melphalan 8,11,12 but also with cyclophosphamide 13,14 , idarubicin 15 , thiotepa 16 , etoposide 17 , bortezomib 18 , carmustine 19 , and with total body irradiation 20 . However, single-agent intravenous busulfan with therapeutic dose monitoring has not been studied as a conditioning regimen for MM.
We hypothesized that single-agent intravenous busulfan would show significant anti-myeloma efficacy and would be better tolerated since severe cytopenia occurs later compared with melphalan, while the recovery time is similar, and in addition, busulfan causes less severe mucositis. If single-agent busulfan would demonstrate significant anti-myeloma activity, it could be used as an alternative conditioning regimen to MEL 140. Therefore, we designed a phase I/II open-label study of intravenous busulfan in patients with MM 65 years of age or older receiving autologous stem cell transplantation (ClinicalTrials.gov identifier: NCT00934232). The primary objective of our study was to determine the maximum tolerated dose (MTD) of busulfan that can be safely given over the least number of days to MM patients ≥ 65 years of age. Secondary objectives were to perform a pharmacokinetic (PK) analysis to evaluate the incidence, individual variability of toxicities, duration of severe cytopenia, and its relationship to each dose concentration.
Materials and Methods
Patient Population
Patients aged 65 years or older irrespective of renal function with SWOG performance of 0–2 and symptomatic MM at the time of initial clinic visit at the Huntsman Cancer Institute requiring treatment were enrolled into the study. Patients with a history of chronic obstructive or restrictive pulmonary disease were excluded from the study. Patients needed to demonstrate adequate lung function defined as ≥ 50% on FEV1, FVC, and DLCO and adequate cardiac function ≥ 40% LVEF on Echo or MUGA scan to be eligible for the study. Patients were excluded if they had transaminases >1.5 times the upper limit of normal and/or direct bilirubin > 1.5 times the upper limit of normal; were HIV positive or had active Hepatitis B or Hepatitis C infection; had a prior autologous or allogeneic bone marrow transplantation; had < 3 million CD34 cells/kg stored; were pregnant or nursing; had a prior malignancy that affects their life expectancy.
The study was approved by the Institutional Review Board of the University of Utah (IRB # 32857) and overseen by a data safety monitoring committee. The study was conducted in according to the Declaration of Helsinki International Conference on Harmonization and the Guidelines for Good Clinical Practice. Written informed consent was obtained from all patients before their enrollment in the study.
Study Design and Treatment
This was a dose escalation study with three patients in each cohort, at the following dose levels: Cohort I: 3.2 mg/kg for 3 days, Cohort II: 3.2 mg/kg for 4 days, Cohort III: 4.3 mg/kg for 3 days, Cohort IV: 5.6 mg/kg for 2 days on Day –1 and Day –3, Cohort V: 5.6 mg/kg for 2 days on Day –1 and Day –2, Cohort VI: 6.4 mg/kg for 2 days on Day –1 and Day –3, Cohort VII: 6.4 mg/kg for 2 days on Day –1 and Day –2. Ideal body weight was used for dose calculation, for males (kg) = [(height in cm÷2.54)–60×2.3]+ 50, for females(kg)=[(height in cm÷2.54)–60×2.3]+ 45.5. If the patient’s actual body weight was greater than 30% of the ideal weight then adjusted weight was used for dose calculation (Adjusted body weight (kg) = [(actual weight – ideal weight)×0.4] + ideal weight. Adverse events were scored according to the NCI CTC, Version 3.0. If no ≥ grade 4 non-hematological toxicity fitting the criteria for serious and related occurred within 30 days after infusion of the last dose of busulfan, we proceeded to the next dosing level. If 1/3 patients incurred a ≥ grade 4 non-hematological toxicity that was serious, and related to the study drug within 30 days after infusion of the last dose of busulfan, that cohort was expanded to six patients (i.e., an additional three patients will be enrolled). MTD was reached if ≥ 2/6 experienced a ≥ grade 4 toxicity (non-hematological) that qualified as serious and related. If only one of the six patients exhibited a ≥ grade 4 non-hematologic toxicity considered as being serious, and related, we proceeded to the next dose level upon approval of the Principal Investigator and the Data and Safety Monitoring Committee primary monitor. Responses were defined according to the International Myeloma Working Group uniform response criteria 21 .
All patients received busulfan (Busulfex®, Otsuka Pharmaceutical Development & Commercialization, Inc, Princeton, NJ, USA) as an intravenous infusion over 6 h through a central venous catheter using a controlled rate infusion pump. All patients were admitted to the inpatient service during busulfan infusion for safety reasons. Peripheral blood stem cell infusion at a dose of ≥ 3×106 CD34+/kg was given intravenously on Day 0 (i.e., approximately 24 h after the last dose of busulfan but no sooner than 18 h after the last dose of IV busulfan). In addition to busulfan, dexamethasone was administered at a dose of 20 mg/day on Days –4 until Day –1, and Days +2 to +5. All patients received seizure prophylaxis with either oral phenytoin or fosphenytoin. Phenytoin was loaded with 3 doses of 300 mg PO each at least 2 h apart, with the last dose to be given a minimum of 1 h before the first dose of IV busulfan; then phenytoin was given at 300 mg PO once daily for the duration of IV busulfan administration, plus 1 day after completion of busulfan. Fosphenytoin was loaded at 1000 mg IV at least 1 h before starting IV busulfan; then given 300 mg IV once daily for the duration of IV busulfan administration, plus 1 day beyond the completion of busulfan. All patients received G-CSF starting Day 6 after transplantation. All patients received antibacterial, antifungal, antiviral, and anti-Pneumocystis jiroveci prophylaxis per institutional guidelines.
Determination of PK Data
All busulfan blood samples were drawn from an inserted peripheral line or PICC line, but not from the port used for infusion. Samples were collected at baseline prior to the start of infusion, then at 3 h, 5 h 55 min (before end of infusion which is the peak sample), 6 h 15 min, 6 h 30 min, 7 h, 8 h, 10 h, 12 h, 18 h, and 24 h (trough sample). Plasma was separated by centrifugation at 1500 g for 10 min at 4°C. A complete plasma concentration versus time plot was generated for each subject. Busulfan plasma concentrations were determined using a previously validated HPLC methodology with UV detection 22 . Thirteen patients were treated with a total of 38 doses of busulfan delivered by IV infusion. A PK profile of concentrations over 24 h was assumed. Raw PK data from study data were extracted to Excel spreadsheets. Specifically, data required for analysis were extracted including patient ID, dose, dose number, time of infusion start, time of infusion end, weight, time of sample draw, and plasma busulfan concentration
Statistical Analysis
The standard “3+3”design for dose escalation was applied with an anticipated enrollment of 30 patients in a maximum of seven cohorts. Response and toxicity probabilities of interest could be estimated within ±19% with 30 patients (95% confidence interval). Any toxicity occurring with at least 10% probability was likely to be observed at least once in 30 patients (95% or greater probability).
An assessment of busulfan PK parameters was undertaken using a non-compartmental analysis (NCA) approach utilizing Phoenix® WinNonlin® version 6.3 (Certara L.P. (Pharsight, USA), St. Louis, MO). PK parameters were generated using the measured busulfan plasma concentrations versus time data from each subject. NONMEM (v. 7.3) interfaced with PDx Pop (v. 5.1) was used to develop a base model to confirm linear pharmacokinetics and investigator PK compartment structure. The duration of PFS was calculated for all patients from the day of transplantation to the time of progression, relapse, death from any cause, or reference date (February 1, 2019). Overall survival (OS) was estimated from the day of transplantation to the date of death or reference date. PFS and OS were plotted according to the Kaplan–Meier method. Adverse effects and treatment responses are presented as mean (±SD) or median values with 95% confidence intervals. All statistical analysis was done using GraphPad Prism® (version 7.00 for Windows, GraphPad Software, La Jolla, CA, USA).
Results
Patient Characteristics
Across five cohorts, we enrolled 13 patients into the study starting from September 2009 until May 2011 (Table 1). The average age of the patients in the clinical trial was 73 years (range 68–80 years). Most had advanced disease, with six of the 13 patients having ISS II and two having ISS III; for two patients the initial ISS staging was not available. Most had standard risk cytogenetic abnormality and only one patient in cohort 3 had del 17p; this patient had progressive disease and did not respond to the autologous transplant. Eight patients had received at least one line of treatment for MM before transplant. All patients were mobilized with D-PACE except for one in cohort four who received G-CSF and plerixafor. Average cell number infused was 7.48 ×106/kg across all the different cohorts in the study. As per the institutional policy at the time of this trial all patients were planned to receive 2 years of maintenance treatment, typically the first year with VTD (bortezomib 1 mg/m2 on Day 1,4, 15 and 16, thalidomide 100 mg daily and dexamethasone 20 mg Days 1–4 and 15–18 of a 28 day cycle and the second year thalidomide replaced by cyclophosphamide 500 mg orally on Days 1 and 15). Patients 1 and 2 in cohort 1 completed 2 years of maintenance with dose adjustments. Patient 3 in cohort 1 discontinued VTD after 6 cycles due to neuropathy, switched to lenalidomide/dexamethasone (RD) 15 mg Days 1–21 and continued for total of 2 years with dose adjustments. Patient 1, cohort 2 discontinued VTD after 6 cycles due to poor tolerance. Patient 2, cohort 2 received VTD maintenance for 6 months, changed to velcade/lenalidomide/dexamethasone (VRD) for 12 cycles and then completed 1 year of maintenance with dexamethasone 20 mg Day 1–4 every 3 weeks with dose adjustments. Patient 3, cohort 2, was switched from VTD to VRD after one cycle, which was continued for 1 year and then changed to VCD for second year of maintenance. Patient 1, cohort 3, received VTD, but after six cycles was changed to VRD for 3 months and then RD, but died on treatment. Patient 2, cohort 3 had progressive disease and did not receive maintenance treatment. Patient 3, cohort 3, received VTD for 1 year with dose adjustments for thalidomide and dexamethasone and then lenalidomide single agent 10 mg Day1–21 for 1 year. Patient 1, cohort 4 received only four cycles of VTD maintenance and was discontinued due to poor tolerance. Patient 2 of cohort 4 received six cycles of VTD pre-transplant and so only received six more cycles as maintenance and then continued VCD for 1 year. Patient 3 of cohort 4 received six cycles of maintenance and died on treatment. Patient 1, cohort 5, received four cycles of VTD and four cycles of VRD but discontinued maintenance due to neuropathy.
Baseline Characteristics and Different Dose Levels of Busulfan in the 5 Cohorts of 13 Patients Enrolled in the Study. ISS Staging was not Available for Two Patients. Maintenance Regimens as Noted Given for Two Years Post-Transplant. RD: Revelmid-dexamethasone; VD: Velcade-dexamethasone; V: Velcade; TD: Thalidomide-dexamethasone; VTD: Velcade-thalidomide-dexamethasone; VRD: Velcade-revlimid-dexamethasone; VCD: Velcade-cyclophosphamide-dexamethasone; (s): Single Agent; Dex: Dexamethsone.

Pharmacokinetic Analysis
The first step in this analysis was to ensure that no accumulation of busulfan was occurring. There was an error in the documentation at the time of analysis for patient ID 3 and therefore this patient was removed from the PK assessments, leaving full PK data from 12 patients for use in the analysis. Previously published work 23 , as well as the PK analysis, suggested that the half-life of busulfan is 2–3 h. Thus, accumulation was not expected as the 18-h time period between the end of one infusion, and the initiation of the next represents the passage of at least six half-lives, concurrent with ∼99% elimination of the drug. Indeed, a visual examination of concentration vs. time curves (representative curve, Fig. 1A) demonstrated no apparent increase in peak concentration (Cpeak) over 2–4 doses. In addition, there was no greater than 2% accumulation (accumulation index = 1.02) in the 13 patients, confirming a lack of accumulation in the multi-dose regimen.

(A) Representative (Patient 5, cohort 2) concentration-time profile for IV infusion busulfan delivered over ∼6 h, once daily. Green line represents the points used for NCA in this patient. (B) Semi-log plot of the elimination phase of the concentration-time (after dose) profile. Only a single slope is evident, suggesting a one-compartment model may be appropriate.
An NCA was performed using the Linear Log Trapezoidal calculation method, with a dosing interval (τ) of 24 h, examination of dose-exposure plots was linear for all patients. The NCA demonstrated a similar PK profile for busulfan as has been previously published 23 , with no accumulation over 2–4 daily doses. Visual examination of the elimination phase of the concentration vs. time profile on a semi-log plot (Fig. 1B) appeared to show only a single elimination phase slope, suggesting that a one-compartment model would provide the best fit. A base model developed in NONMEM demonstrated a proposed one-compartment structural model fitted the data the best. PK parameter estimates from the compartmental model were V = 49.2 L, CL = 10.2 L/h. During model development a two-compartment structural model was also tested; this model did not perform or fit the data as well. The PK parameter estimates for all the patients are shown in Table 2. The NCA estimated a mean steady-state clearance (CLss in L/h) of 9.85, the base one-compartment model estimated a comparable clearance (CL) of 10.2 L/h.
Individual and Mean Non-Compartmental Analysis (NCA) PK Parameters. One Patient in Cohort 1, Patient 3 Had Error in Documentation of PK Values and so is not Considered in Analysis. Tmax, Time to Maximum Concentration; Cmax, Maximum Concentration; AUC0→Inf, Area Under the Plasma Concentration-Time Curve Calculated out to Infinite Time; AUClast, Area Under the Plasma Concentration-Time Curve Calculated to the Last Available Data Point; Vz, Volume of Distribution; CLss, Steady-State Clearance.

Safety and Adverse Effects
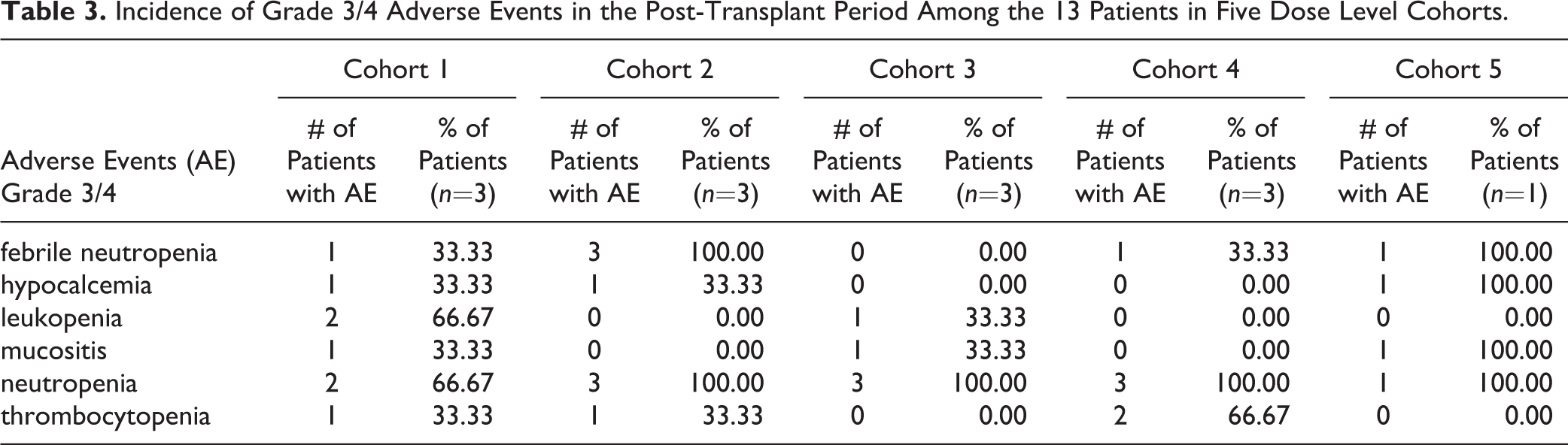
Most of the grade 3/4 adverse effects were hematological and no dose-limiting toxicity was observed in the 13 patients who participated in the study. Grade 3/4 neutropenia was seen in 2/3 of patients in cohort 1 and 3/3 in all other cohorts. The average duration of grade IV neutropenia (ANC <500/µL) was only 3 days (range 1–5 days). The average time to neutrophil engraftment (defined as the first of the three days of ANC >500/µL) was 11.5 days (range 10–13 days) with no difference between the different cohorts. Febrile neutropenia was seen in 1/3 patients in cohort 1, 4 and 5, 3/3 patients in cohort 2, and none in cohort 3. Grade 3/4 thrombocytopenia was seen in 1/3 patients in cohort 1 and 2, and 2/3 patients in cohort 4. One patient in cohort 2 and two patients in cohort 4 required platelet transfusions to keep platelet count >20,000/µL during the post-transplant period. Among the nine patients whose platelet counts dropped below 50,000/µL during the post-transplant period, the mean time to platelet recovery to level above 50,000/µL was 15 days post-transplantation (range 12–24 days). One patient each in cohorts 1, 3, 4, and 5, and all three patients in cohort 2 needed red blood cell transfusion during the post-transplant period. One patient in cohort 2 who had previously received 9.17×106 CD 34 cells/kg required a stem cell boost due to poor engraftment. Grade 3 mucositis was seen in 1/3 patients each in cohort 1, 3, and 5. One patient in cohort 3 developed grade 4 acute bullous eruptions, thought to be unlikely due to busulfan since the skin lesions developed outside the 30 day window post-treatment. Grade 3 or 4 hypocalcemia was seen in three patients, one each in cohort 1, 2, and 5. None of the patients showed evidence of VOD of the liver. There were no deaths in the peri-transplant period and no significant hepatic, pulmonary, cardiac, or neuronal toxicity. Table 3 lists the common grade 3/4 adverse events of all cohorts in the study.
Incidence of Grade 3/4 Adverse Events in the Post-Transplant Period Among the 13 Patients in Five Dose Level Cohorts.
Efficacy
Ten (77%) patients achieved a CR post-transplant with an average time to best response of 6.7 months (range: 6–14 months) after transplant (Table 4). One patient in cohort 3 had progressive disease, and two patients, one each from cohort 2 and 3, only attained a partial response (PR). With a median follow-up of 84 months since the transplant, six (46%) patients are still alive and, of those, three (23%) continue to be in CR and off all therapy for MM. Median OS was 84 months (95% CI, 21–104) and the median PFS was 60 months (95% CI, 9–93) (Fig. 2)
Treatment Outcomes of 13 Patients After Busulfan Conditioning and Maintenance Treatment Started at 3 Months Post-Transplant.


Overall survival (OS) and progression-free survival (PFS) of 13 patients treated across the five cohorts post-transplant. Median OS was 84 months (95% CI, 21–104) and the median PFS was 60 months (95% CI, 9–93).
Discussion
Even though different conditioning regimens have been studied, melphalan 200 mg/m2 continues to be the standard for patients receiving autologous stem cell transplantation in MM. However, for elderly patients a reduced dose of 140 mg/m2 is the standard of care because of its reduced toxicity profile, although it is still debated if the lower dose offers the same efficacy. Busulfan is an alkylating agent used as a component of conditioning regimens for both autologous and allogeneic stem cell transplantation and has demonstrated MM efficacy in multi-agent regimens.
In our phase I/II study, busulfan was well tolerated with no dose-limiting toxicity observed, and all patients on the study were able to complete the conditioning regimen. All patients did receive phenytoin prophylaxis and none developed seizures. None of the patients developed VOD of the liver, which is a well-known toxicity with busulfan. In the post-transplant period, cytopenia was transient and all engrafted promptly, except for one patient who needed a second stem cell infusion. Most patients developed grade 3/4 neutropenia but the duration of severe neutropenia was very short. Interestingly grade 3/4 thrombocytopenia was seen in only four of the 13 patients and the platelets recovered to >50,000/µL at a mean of 15 days compared with 41 days in previous studies with melphalan 4 . Grade 3 mucositis was observed in three patients and was comparable to that observed in MEL200 in previous studies 24 , although our patient population was older. The adverse events observed in the post-transplant period and the time to engraftment were similar to what we would have observed with a melphalan single-agent conditioning regimen 4 . Interestingly, even though the study was open to patients above 65 years, the mean age of the patients was 73 years, further strengthening the argument that busulfan at these dosing levels is safe and well tolerated. The PK analysis showed no increase in the peak busulfan concentration with multiple day dosing, nor was there any accumulation of busulfan with the repeated dosing. In agreement with previous studies, the base one-compartment structural model provided a better fit of the busulfan concentrations than the two-compartment model. Our model estimated a CL of 10.2 L/h, compared with the literature reported CL estimates which are higher in adults with value of 12.4 L/h for an equivalent to 70 kg total body weight 25 . This discrepancy may potentially be due to a difference in dosing, which was based on ideal body weight in our study.
Even though no direct comparison was made, patients in our study had a CR rate of 77%, median PFS of 60 months, and a median OS of 84 months. This compares favorably with standard melphalan conditioning regimen which was reported to provide a CR rate of 49%, median PFS of 28 months, and median OS of 60 months 26 . However, this is a phase 1 study with only 13 patients, and no firm conclusions of therapeutic efficacy in comparison to MEL 140 are possible and efficacy can only be answered by a large randomized trial. Furthermore, it could be argued that the improvement in survival and response rates seen in our study was mainly due to the maintenance regimen with bortezomib and IMiD. However, in the GEM05MENOS65 trial, patients younger than 65 years with newly diagnosed MM on Velcade/Thalidomide maintenance given for 3 years after MEL 200 achieved a CR rate of 21% and PFS of 50.6 months 27 . Busulfan conditioning combined with maintenance treatment in our study appears to achieve favorable CR rates and duration of PFS compared with melphalan. Another particular and probably important observation was that patients achieved a complete response at a mean of 6.7 months, with one patient attaining a CR 14 months after the transplant, compared with most patients achieving a CR within 3 months after MEL 200 transplants 28 . None of the long-term survivors who are still in CR have been kept on treatment after the initial 2 years of post-transplant maintenance. Even though the study did not enroll all the cohorts, and the numbers in each cohort were small, there appeared to be no difference among the different dose schedules of busulfan in terms of ability to achieve a CR or duration of response.
A significant shortcoming was that the study did not attain its anticipated end point of finding the MTD due to the principal investigator leaving the Institution. We did not see any difference in the limited patients in each cohort, leading us to believe that busulfan administration over a shorter period of time and at higher doses per day may very well be feasible. None of the patients in this study had high risk cytogenetic abnormality such as t(4:14) or TP53 deletion, except for one. Therefore, the high CR rates and duration of response could be due to better disease biology in these patients. However, most of the patients had a higher stage myeloma (ISS stage II/III) and had shown progressive disease before transplant.
Our study opens up the possibility of busulfan being used as an alternative conditioning regimen for autologous stem cell transplantation with probable benefits in myeloma patients above 65 years, and supports larger studies including a randomized trial to see if there is an advantage of IV busulfan over MEL 140.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.