
Abstract
Since the introduction of autologous platelet-rich plasma (PRP) in medical practice, various studies have documented that implementing PRP can enhance healing and the anti-aging process, employing angiogenesis regeneration due to the multiple growth factors and cytokines involved. Numerous reports have shown promising results with the use of PRP in ovarian treatment, regarding ovarian regeneration and reactivation of folliculogenesis. This case series reports on two women with premature ovarian failure (POF) aged 40 and 27 years, respectively, and one menopausal woman aged 46 years. All patients presented with lack of menstrual cycle for over a year. The women reported previous failed in vitro fertilization (IVF) attempts, and, after rejecting the option of oocyte donation, they opted for the approach of autologous ovarian PRP treatment. Following PRP treatment, the three patients were invited to conceive naturally. The primary outcome was the restoration of menstruation following autologous ovarian PRP treatment, as well as an improvement in hormonal profile, a decrease in follicle-stimulating hormone (FSH) levels, and a concurrent increase in anti-Müllerian hormone (AMH) levels. Further to that, our patients achieved pregnancy through natural conception within 2–6 months following PRP treatment, resulting in currently ongoing complication-free clinical pregnancies – a first report in the literature for menopausal and POF patients. Implementation of PRP should be further investigated through randomized controlled trials (RCTs), as it may hold the key to successful treatment for a certain cohort of patients exploring reproductive treatment options following menopause.
Introduction
In our era of rapid-pace advances, motherhood seems to be delayed 1 . Current data reveal a significant rise in firstborn mothers’ age, ranging between the third and fourth decade 2,3 . Aging of the female reproductive system is directly associated with disruption of ovarian function and jeopardized fertility potential, ultimately leading to menopause – a stage identified hitherto as irreversible 4 . Nonetheless, the right to reproduce regardless of age, may be undeniable. Interestingly, data sourced from pregnancies involving a more advanced maternal age 5 , indicate that the right to reproductive autonomy remains intact irrespective of the perils that such pregnancies may harbor. In fact, the desire to mother a child appears to overrule the obstacles encountered, even when these are associated with irrefutable evidence of reproductive physiology compromise due to aging 6 .
Menopause is defined physiologically as the final cessation of menstruation for 1 year, originating from estrogen deficit 7 . In Caucasians, the mean age of menopause is reported to be 51 years (range 45–55 years), and is accompanied by increased levels of gonadotropins in serum, with follicle-stimulating hormone (FSH) levels increasing to more than 40 mIU/ml 8 . Unfortunately, around 5% of women aged 40–45 years may experience early menopause, with about 1% of women aged below 40 years experiencing premature menopause 7 . This can be attributed to environmental or genetic parameters, or be induced by a medical intervention 9,10 . Following a literature search attempting to delineate spontaneous or induced menopause, various definitions have been documented, with the terms ‘premature ovarian insufficiency (POI)’ 8,11 , ‘premature ovarian failure (POF)’ 11 , and ‘early or premature menopause’ all being used to describe this life stage 9 .
To fulfil their wish to have children, the aforementioned groups may turn either to assisted reproductive technologies (ART), or opt for oocyte donation 12 , surrogacy, or adoption 13 . However, these latter reproductive options fail to fulfill the parents’ desire for genetically related offspring. Although oocyte donation may represent the sole and last resort where currently available reproductive options are concerned 14 , the conundrums facing menopausal women aiming to bypass infertility related to aging still stand.
An alternative approach – autologous platelet-rich plasma (PRP) – has been pioneered by our team 15,16 . PRP consists of numerous proteins, such as cytokines, growth factors and hormones. Upon platelet activation, these proteins serve as chemo-attractants for stem cells, macrophages and neutrophils, which all contribute greatly to the post-translational modification of approximately 1500 bioactive factors 17 . Several animal and human studies have provided insights into the molecular function and structure of platelets 18 –20 . Nonetheless, the mitogenic, chemotactic, neovascular and anti-inflammatory properties of PRP can all be attributed to the numerous growth factors it contains 21 . These factors, which are concentrated in PRP following centrifugation, include: platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), transforming growth factor beta (TGF-β), connective tissue growth factor (CTGF), keratinocyte growth factor (KGF), basic fibroblast growth factor (bFGF), epidermal growth factor (EGF), insulin-like growth factor 1 (IGF-I) and 2 (IGF-II), and hepatocyte growth factor (HGF) 21,22 . All these growth factors are considered responsible for cell migration and differentiation, as well as for proliferation, activation of angiogenesis, and tissue regeneration 23,24 . Interestingly, studies have reported a correlation between aging and decreased concentrations of growth hormone and IGF-1 22 . Indeed, investigating molecular pathways leading to aging 25,26 , it is thought-provoking that factors participating in the aging process, such as IGF-1, are included in PRP 27 .
Some interesting reports documented a prematurely menopausal woman achieving a biochemical pregnancy following autologous PRP intraovarian infusion that resulted in a spontaneous abortion 28 , and poor responders reporting live births 29 . Additionally, other studies support a contribution of PRP treatment to follicular growth and maturation 30 , and, last but not least, to endometrial improvement including enhancement of thickness 31 .
The aim of this case series study was to report the effect of intraovarian PRP treatment on three menopausal women who had previously rejected the choice of oocyte donation following appropriate consultation. This case series uniquely brings to the literature the first report on natural conceptions following intraovarian PRP treatment, leading to ongoing complication-free pregnancies. This article highlights that autologous PRP treatment merits further investigation, presenting as a valid option for women faced with the challenge of exploring reproductive options employing their own oocytes after having entered menopause. In an era where cellular transplantation approaches appear to shape the future landscape of state-of-the-art treatment options, especially where aging may be concerned, application of PRP certainly presents an angle worth exploring.
Case Series Description
During our patients’ first consultation appointment, a detailed reproductive history was recorded, as required by the clinic’s protocol. The three patients presented herein were diagnosed as menopausal, based primarily on the elevated FSH levels along with amenorrhea for at least 1 year. Subsequently, prior to initiating PRP treatment, as well as after PRP treatment, their hormonal profile was assessed. In case of continued amenorrhea as described for all three patients, hormone evaluation was requested independently of a menstrual cycle. FSH, estradiol (E2), luteinizing hormone (LH), and anti-Müllerian hormone (AMH) levels were determined on an unspecified day prior to initiating PRP treatment. Hormone levels following PRP treatment were determined during day 2 of the subsequent menstrual cycle. FSH, E2, and AMH levels were determined using a chemiluminescent micro particle immunoassay on a Roche Cobas E-411 immunoassay analyzer, with inter-assay coefficients of variation of <4.6% and <5.6% for E2 and AMH, respectively. Autologous PRP was prepared with a RegenACR®-C Kit (Regen Laboratory, Le Mont-sur-Lausanne, Switzerland) according to the manufacturer’s instructions. The overall reproductive background assessment for each patient is presented briefly in Table 1.
Reproductive Background Prior to PRP Treatment.

PRP, platelet-rich plasma; FSH, follicle-stimulating hormone; AMH, anti-Müllerian hormone; E2, estradiol; LH, luteinizing hormone; AFC, antral follicle count; HR, hormone replacement.
*Patient did not receive HR
It should be stressed that a hysteroscopy was performed for all three cases in order to reveal any potential uterine pathology. This was a prerequisite prior to inviting patients to proceed with their initial desire to conceive naturally.
The required volume of PRP was extracted from 60 ml of the patient’s peripheral blood. The initial concentration of platelets in the peripheral blood sample was approximately 250,000/µL. According to our protocol, prepared PRP may be stored for 1 h at a temperature of 4°C if required. However, for the three patients included here, PRP was administered immediately following preparation. The injection of PRP is mostly an empirical process, as this constitutes a novel technique in the field of reproduction. Injecting PRP into the ovaries is a technique based on the method of transvaginal paracentesis employed during the oocyte pick up (OPU) procedure. Minimal sedation was administered to the patients. Injection and diffusion into the ovarian stroma were performed under a non-surgical, transvaginal ultrasound-guided multifocal intramedullary procedure, allowing approximately 4 ml PRP for each of both ovaries. In a more detailed description, the ovaries were identified with the guidance of transvaginal ultrasonography. Following identification, a needle was inserted, penetrating the ovarian tissue, accompanied by a resistance felt by the practitioner. Prior to initiating the injection procedure, the needle guide was aligned with the ovaries to ensure that any surrounding structures, such as vessels, were not compromised. Taking into account the anatomical position of the ovary, a 17-gauge single lumen needle was employed, moving across the central part of the ovary, carefully covering the distance from one side to the other, practicing extreme caution so as to avoid penetrating the germinal epithelium of the outer wall of the ovary into the peritoneal cavity. Activated PRP was then introduced via a syringe attached to the transvaginal probe transducer. When in place, the practitioner applied pressure to the plunger of the syringe slowly and steadily, resulting in gradual injection of PRP. To ensure that application was not localized and that all layers of the ovary were exposed to the infusion, the needle was simultaneously and gently retracted while injecting and finally exiting the ovary. Minor leakage was observed due to the width of the needle employed. However, employing a needle of a narrower opening may be associated with heightened risk of blockage during the procedure; hence, the practitioners opted to use the same needle as employed during the OPU procedure, conveying safe practice. Nonetheless, in the case of menopausal women, part of the infused PRP ends up in the peritoneal area due to the reduced ovarian volume related to the atrophied nature of the ovaries. This leads to failure by the ovaries to accommodate all of the intended injected volume, and subsequent minor leakage. A careful ultrasonography examination of the pelvis was performed after the procedure, confirming a minute amount of leakage during the procedure, as well as overall vascular integrity. Duration of the injection procedure was in the range of approximately 5–7 min. After the procedure, the patient was asked to remain in supine position for 10–15 min, and was transferred to their room thereafter to rest for a further hour. Vital signs were checked to secure the patient’s home discharge. Following PRP administration, detailed follow-up appointments were arranged at monthly intervals to monitor patients, ensuring that any complication would be documented and further investigated. Notably, this novel approach was described as a complication-free procedure for all three patients. Tables 2, 3, 4 and 5 depict patient profiles following treatment during the 6-month follow-up protocol. The Hospital Ethics Board approved the study protocol in accordance with the Helsinki declaration (number 327-11/12/2018) and all participants provided informed consent.
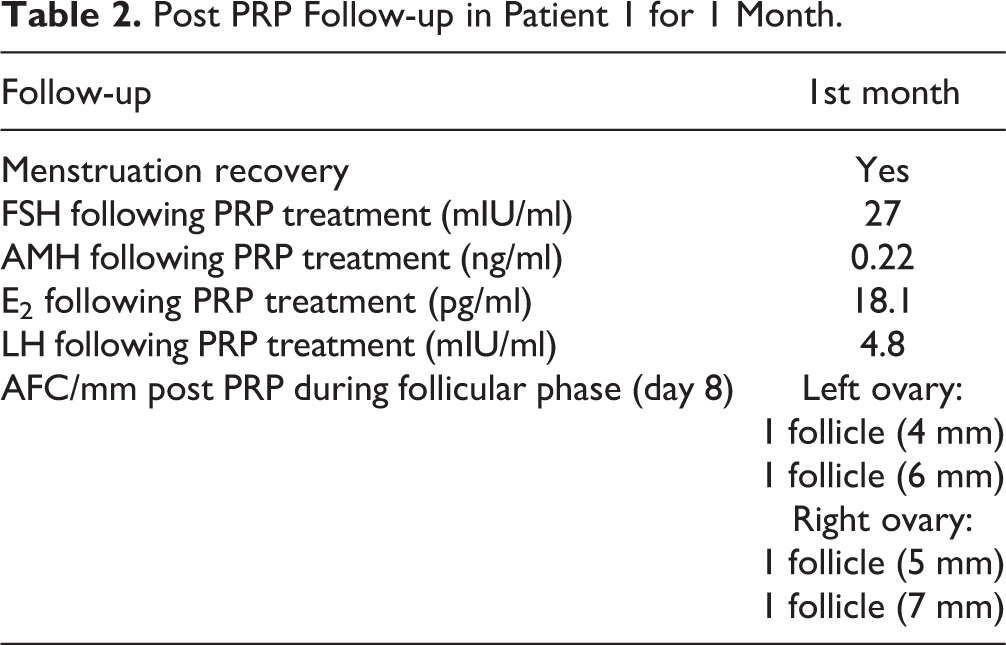
Post PRP Follow-up in Patient 1 for 1 Month.
Post PRP Follow-up in Patient 2 for 3 Months.

Post PRP Follow-up in Patient 3 for 5 Months.

Reproductive Outcome Post PRP.

Case 1
Patient 1 (aged 46 years) was referred to the clinic as a previously diagnosed menopausal patient, reporting with absence of menstrual cycle for 12 consecutive months. Hormone levels were recorded as follows: FSH 119 mIU/ml, E2 19 pg/ml, AMH 0.16 ng/ml, and LH 53.2 mIU/ml. The patient had embarked on hormone replacement (HR) for 6 months in total – a treatment that had been abandoned 3 months prior to her referring to our clinic. Following consultation, it was evident that the primary outcome this patient was seeking was fertility restoration. Hysteroscopic and bacteriologic screening tests were found to be negative for any endometrial pathologies and inflammations, respectively. Presented with the available options, the patient finally opted for PRP treatment to be performed in both ovaries as a last resort prior to embracing oocyte donation. PRP treatment was performed based on the aforementioned protocol, and, following written consent, PRP treatment was performed. A reassessment of the patient’s hormonal profile was conducted with the emergence of a menstrual cycle, which was noted 1 month post-treatment. Hormone levels recorded 1-month post-treatment were as follows: FSH 27 mIU/ml, E2 18.1 pg/ml, and AMH 0.22 ng/ml, while LH levels decreased to 4.8 mIU/ml (Table 2). Antral follicle count (AFC) was similarly assessed during the follicular phase. Prior to initiating treatment, AFC was zero for both ovaries (Table 1). However, during follow-up transvaginal ultrasound on the 1st month post-PRP, conducted during day 8 of the menstrual cycle, the AFC was reported as two follicles of 4 mm and 6 mm, respectively, in the left ovary, and two follicles of 5 mm and 7 mm in the right ovary (Table 2). Relevant data regarding the patient’s hormonal profile during the 2nd month following PRP treatment are presented in Table 2. Following restoration of the menstrual cycle a month following treatment, the patient opted not to pursue IVF treatment, and pursued spontaneous conception. Approximately 2 months following PRP treatment, the patient reported that a natural conception had been achieved. Currently, a healthy complication-free pregnancy is confirmed. The patient is at 37 weeks gestation, with normal first and second trimester prenatal screening tests, along with a reactive non-stress test (NST) (Table 5).
Case 2
Patient 2 (aged 40 years) was referred to our clinic as a previously diagnosed prematurely menopausal patient. A hormonal investigation and ultrasound evaluation were performed to confirm her status. FSH, E2, LH, and AMH levels were 65 mIU/ml, 17 pg/ml, 42 mIU/ml, and 0.06 ng/ml, respectively. The patient’s reproductive background, hysteroscopic, and bacteriologic screening were found to be negative for any endometrial pathologies or inflammation (Table 1). Embarking on PRP treatment was the patient’s sole demand, as she was familiar with this novel approach through media reports and online research. AFC was performed prior to initiating the treatment, and confirmed absent follicles for each ovary (Table 1). During follow-up transvaginal ultrasound in the 1st month following PRP, AFC recorded two follicles of 6 mm and 8 mm, respectively, in the right ovary, evaluated on day 8 of the follicular phase (Table 3). Following PRP treatment, a notable decline in FSH (10 mIU/ml), E2 (86.5 pg/ml), and LH (13 mIU/ml) levels, and a slight increase in AMH levels (0.13 ng/ml) were recorded on the first menstrual cycle 2 months following PRP. Additional relevant data regarding the patient’s hormonal profile during the first 3 months following PRP treatment are presented in Table 3. The patient’s initial request was menstrual cycle restoration to enable the possibility of a natural conception; hence she was invited to conceive naturally; 4 months following treatment the patient reported a pregnancy. Currently, a healthy, complication-free pregnancy is confirmed. The patient is at 37 weeks gestation, with normal first and second trimester prenatal screening tests, along with a reactive NST (Table 5).
Case 3
Patient 3 (aged 27 years) was referred to our clinic as a patient having entered premature menopause. Extremely high levels of FSH and low levels of E2 and AMH were recorded and confirmed her status: FSH 46.5 mIU/ml, E2 15 pg/ml, LH 21 mIU/ml, and AMH 0.17 ng/ml. Additionally to the patient’s reproductive background, hysteroscopic and bacteriologic screening were found to be negative for any endometrial pathologies or inflammations, respectively. The AFC count during ultrasonography confirmed absent follicles for both ovaries (Table 1). Following PRP treatment, the patient’s follow-up report revealed a decline in FSH (20.09 mIU/ml) and LH (19.59 mIU/ml), accompanied by an increase of AMH (0.25 ng/ml) and E2 levels (107 pg/ml), all detected during the first menstrual cycle following PRP (Table 4). Following PRP treatment, AFC interestingly measured one follicle of 6.5 mm in the right ovary, evaluated during the follicular phase of the 2nd month following PRP treatment (Table 4). Additional relevant data regarding the patient’s hormonal profile during the first 5 months following PRP treatment are presented in Table 4. Currently, a healthy, complication-free pregnancy is confirmed. The patient is at 26 weeks gestation, with normal first and second trimester prenatal screening tests, along with a reactive NST (Table 5).
Discussion
The history of PRP goes back to 1954, with the term PRP first described by Kingsley 24 while conducting blood coagulation research 24,32 . Following initial use in skin wound healing in rat models by Matras 33 , application PRP was soon adopted by a wide range of medical fields. Today PRP is applied clinically mostly in regenerative medicine 32,33 . The application of PRP in anti-aging therapy merits further investigation since results and data in a variety of studies in various fields of medicine report favorable outcomes 34 . According to research data, >95% of presynthesized growth factors are secreted within 1 h following degranulation 34 . Fibroblasts are then activated following this process 35 , while matrix metalloproteinases, stored in multiple cells such as the fibroblasts, accelerate the proliferation of mesenchymal cells – a very important step in the regeneration process 36 .
According to published research promoting intrauterine growth improvement and addressing receptivity issues, patients with fine endometrium and poor receptivity appear to present as clinically improved following intrauterine PRP infusion 18 . Many studies describe autologous PRP as an operative tool for the reproductive system 1 . Zadehmodarres and colleagues demonstrated regeneration and thickening of thin endometrium 48 h post PRP application 37 . The latter group reported good pregnancy outcomes in <50% of patients 18 . Further to that, intrauterine PRP treatment seems not only to promote endometrial growth in patients with thin endometrium, but to positively influence outcomes following assisted reproduction 17 . Autologous PRP treatment of the ovaries, with the considerable amount of growth factors and cytokines involved, has been shown to enhance ovarian regeneration as well as reactivation of folliculogenesis 19 . Today, autologous PRP treatment seems to lead to interesting results worth investigating in the field of reproductive gynaecology 15 . Our case series reports the first successful attempt to overcome the age barrier in the reproductive context, by enabling clinical pregnancies following autologous PRP ovarian infusion.
This case series describes two prematurely menopausal women and one menopausal woman, exploring their options of mothering a child using their own oocytes. Oocyte donation was thoroughly discussed; however, all three patients rejected this option. Following appropriate consultation, all three women opted for the alternative approach of autologous ovarian PRP treatment. PRP treatment was performed in 2018. Menstrual restoration following autologous ovarian PRP treatment in menopausal women presenting with amenorrhea for >1 year was the primary outcome measure of this report.
During our study, follow-up of all three cases was performed during the first menstrual cycle post PRP treatment. This was reported for all cases within the subsequent calendar month. A decrease of a previously high FSH level, and concurrent increase of very low AMH levels, were recorded. This finding was in accord with that highlighted in a case series report published in 2018 reporting the use of PRP in poor responders, with 1-month post PRP hormonal levels influenced similarly, i.e., there was a decrease in FSH levels, and a corresponding increase in levels of AMH. The positive effect of PRP on ovarian tissue and function may be viewed as being mirrored by the decrease in FSH and increase in AMH as previously documented, albeit on a case series level, by other researchers 11 . In the reproductive context, outcomes following PRP application targeting either poor responders 11,15 or prematurely menopausal women 14 have been described recently through case series reports, serving as advocates for the efficient and safe employment of PRP until the highly anticipated RCT data emerges. It is data stemming from such advanced evidence-based studies that will validate wider application of PRP.
Our patients achieved pregnancy through natural conception in less than half a year following PRP treatment. This result is heightened in the light of their challenging reproductive histories, along with the fact that achieving a pregnancy during menopause may be viewed as somewhat of a biological paradox. The importance of this report lies in the fact that these pregnancies successfully reached clinical status level, unlike a previous report documenting a miscarriage following a biochemical pregnancy in a menopausal woman undergoing PRP treatment 14 . The clinical pregnancies reported here are currently ongoing.
Accounting for the role of chance as a confounder in this case series report is challenging. However, previous studies investigating the unlikely scenario of women achieving a pregnancy using their own oocytes while on menopause referred principally to the early stages of menopause or during erratic menstruation characterized by irregularities. For such cases, where menopause is not yet fully established, perhaps a small percentage of the pregnancies achieved could be attributed to unpredictable ovarian functionality 20 . Nonetheless, all our patients had long been classified as menopausal while actively exploring alternative options and failing to establish a positive outcome. Certainly, there are reports of pregnancies in menopausal and POF patients, but these are extremely rare, and there are no reports in the literature on percentages of clinical pregnancies in any large trial on menopausal patients.
Delineating the actual role of PRP in influencing the physiology of the reproductive system in these patients constitutes a challenge that may be addressed only when evidence regarding its bioactivity emerges. Despite the fact that the preparation of PRP is established by a specific protocol, the bioactivity of the final product varies depending on the individual 20 . Caution must be exercised during the methodology used to evaluate the concentration of PRP components. Important steps during centrifugation, such as duration, and the speed and centrifugal force specified, could all contribute to affecting the potency and performance of bioactive proteins and potentially compromise the results of treatment. Published literature supports the view that increased concentration of platelets translates to increased amounts of growth factors, and, perhaps, increased effectiveness 20 . Further to that, research has shown that levels of growth factors released from the a-granules seem to be influenced by the procedure applied to activate the platelets. As anticipated, variations in the amount of growth factors present will distinguish one patient from another, thus affecting treatment efficacy. A limitation of the current study is that these differences were not recorded. Further studies should be conducted to justify the effectiveness of PRP. The current report stands as an observational case series describing and observing the implementation of PRP; thus, the authors refrain from making definitive statements on its effectiveness. On the same note, the data presented herein may not serve to adequately extrapolate on the molecular mechanisms involved, vis-à-vis ‘why PRP injection resulted in immediate menstrual cycle activation?’ and ‘what was involved in sustaining monthly menstruation?’ Any hypothesis and assumptions or any further statements regarding the possible molecular mechanisms entailed cannot be accounted for.
Regarding the short- and long-term adverse effects of PRP application in the reproductive system, there are no studies stating any side effects. Various studies highlight that PRP growth factors do not present with risk, are non-mutagenic, and are incapable of inducing tumor generation 38,39 . Nonetheless, one must account for heterogeneity in study design, with variablity in clinical parameters and clinical outcomes presenting as an issue 14,21 . Possible adverse effects or complications related to the treatment of this case series were evaluated during the scheduled follow up examination, as well as during the scheduled first and second trimester screening and NST. Hitherto, the reasons for caution are introduced only within the theoretical context. On the other hand, the retrospective nature of this case series, in line with the respective uniqueness of the three included cases, should not be overlooked. The authors acknowledge that indeed the nature of a case series study such as this, along with pilot and single case reports, fails to provide insight and convey confidence to the average practitioner regarding possible side effects or adverse effects following PRP treatment. A solid study design, consistency in the clinical parameters and clinical outcomes examined, along with inclusion of control groups, in a large sample prospective study are the minimum requirements that will enable a valid investigation into any adverse effects related to PRP treatment.
Given that case 1 discontinued HR 3 months prior to PRP treatment, the potential influence of HR requires further consideration. Several RCTs and comparative cohort studies on the effect of HR in menopausal women have shown that menopausal symptoms reoccur after 3 months of discontinuing HR 40 . In light of this data, HR administration for patient 1 may be safely viewed as an independent characteristic unrelated to the effectiveness of PRP treatment 41 . Further studies on cohort patients may hold the key to successful reproductive treatment options regarding menopause; nonetheless, they should be followed and supported by RCTs.
Menopause is the end of a woman’s reproductive timeline – an inevitable and irreversible situation. Nonetheless, the scientific community appears to challenge this by focusing on research attempting to answer the question: ‘How can we reverse menopause?’ Along with the introduction of PRP in addressing issues involving aging in medicine 42 , stem cell infusion has also been introduced as a promising option 43 . RCTs designed to further investigate the effectiveness of ovarian stem cell infusion have already been submitted; thus, this novel approach may escape its hitherto theoretical context. Perhaps the scientific community will not be content with just answering whether PRP or stem cell treatment is efficient in the reproductive context, but rather remain restless until we can understand ‘to what extent’, ‘through which mechanism’, and, most importantly, ‘which patients fit the profile of being benefitted’. With regards to identifying these patients, interestingly, an array of proteins and growth factors may be the key to portraying a distinctively different profile, helping to categorize various maturation periods 44 . Thus, assessing an individual’s molecular profile prior to, and following, novel ‘anti-aging’ techniques could be the answer, hopefully cementing the identity of novel trends such as PRP as valid options in a clinicians’ routine.
Autologous PRP has led to interesting reproductive results for this case series of patients. These include folliculogenesis, along with menstrual cycle restoration, and, most importantly, enablement of natural conception and ongoing complication-free pregnancies. Even though the successful application of PRP has been proven in various systems, much effort is still required to visualize future possibilities in clinical application. PRP implementation certainly requires serious consideration regarding its biological efficiency and the extent to which it may be applied clinically should its effectiveness be validated by robust data. The authors refrain from making generalized claims regarding the all-healing and anti-aging nature of PRP, especially in view of the lack of RCT data. Nonetheless, one cannot help but ponder whether PRP may present as a promising option in the reproductive field.
Supplemental Material
Supplementary_material - A Case Series on Natural Conceptions Resulting in Ongoing Pregnancies in Menopausal and Prematurely Menopausal Women Following Platelet-Rich Plasma Treatment
Supplementary_material for A Case Series on Natural Conceptions Resulting in Ongoing Pregnancies in Menopausal and Prematurely Menopausal Women Following Platelet-Rich Plasma Treatment by Konstantinos Pantos, Mara Simopoulou, Agni Pantou, Anna Rapani, Petroula Tsioulou, Nikolaos Nitsos, Stephen Syrkos, Athanasios Pappas, Michael Koutsilieris and Konstantinos Sfakianoudis in Cell Transplantation
Footnotes
Author Notes
Konstantinos Pantos and Mara Simopoulou should be considered as joint first authors.
Michael Koutsilieris and Konstantinos Sfakianoudis should be considered as joint last authors.
Ethical Approval
Ethical approval to report this case series was obtained from the Hospital Ethics Board (number 327-11/12/2018).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Hospital Ethics Board (number 327-11/12/2018) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.