
Abstract
The survival of engineered tissue requires the formation of its own capillary network, which can anastomose with the host vasculature after transplantation. Currently, while many strategies, such as modifying the scaffold material, adding endothelial cells, or angiogenic factors, have been researched, engineered tissue implanted in vivo cannot timely access to sufficient blood supply, leading to ischemic apoptosis or shrinkage. Constructing vascularized engineered tissue with its own axial vessels and subsequent pedicled transfer is promising to solve the problem of vascularization in tissue engineering. In this study, we used the tissue expander capsule as a novel platform for vascularizing autologous smooth muscle cell (SMC) sheets and fabricating vascularized engineered tissue with its own vascular pedicle. First, we verified which time point was the most effective for constructing an axial capsule vascular bed. Second, we compared the outcome of SMC sheet transplantation onto the expander capsule and classical dorsal subcutaneous tissue, which was widely used in other studies for vascularization. Finally, we transplanted multilayered SMC sheets onto the capsule bed twice to verify the feasibility of fabricating thick pedicled engineered smooth muscle tissues. The results indicated that the axial capsule tissue could be successfully induced, and the capsule tissue 1 week after full expansion was the most vascularized. Quantitative comparisons of thickness, vessel density, and apoptosis of cell sheet grafts onto two vascular beds proved that the axial capsule vascular bed was more favorable to the growth and vascularization of transplants than classical subcutaneous tissue. Furthermore, thick vascularized smooth muscle tissues with the vascular pedicle could be constructed by multi-transplanting cell sheets onto the capsule bed. The combination of axial capsule vascular bed and cell sheet engineering may provide an efficient strategy to overcome the problem of slow or insufficient vascularization in tissue engineering.
Introduction
Tissue engineering paves a new way to restore or replace defective organs or tissues 1,2 . However, the potential clinical implementation of engineered tissues remains limited, at least in part because of the lack of effective strategies to ensure that engineered tissues are timely and adequately vascularized after transplantation 3,4 . Somatic cells are never more than 100 to 200 µm from a capillary 5 , which provides them with oxygen, essential nutrients, and transports away carbon dioxide and metabolic waste, all of which are critical for cell survival. Therefore, the successful transplantation of engineered tissue requires the construction of its own vascular network, which can anastomose with the host vasculature as soon as possible 6,7 .
To overcome the problem of vascularization, strategies, such as modifying the scaffold material, embedding angiogenic factors, 3D bioprinting technologies to create constructs containing vascular-like networks, and co-culture of endothelial cells with stem or target cells, have been researched 8 –11 . However, vascularization of thicker or complex tissues remains an unmet need in terms of clinical application 12 –14 . To ensure the implanted grafts can timely access to sufficient blood supply, it is necessary not only to construct the microvascular network of the engineered tissue itself, but also to ensure that the microvascular network can immediately anastomose with the host vascular network and transport blood.
The capsule tissue formed between an implanted device and the body’s own soft tissues was found to develop its own unique blood supply 15,16 . By placing a tissue expander close to large vessels, vascularization could be controlled and guided so that the induced capsule tissue will be supplied by an arteriovenous bundle, which was observed in our pre-experiments. The superficial circumflex iliac vessels (SCIs), adjacent to the bladder, were chosen to develop an axial capsule bed, which was then used to construct pedicled tissues to repair the damaged bladder. Cell sheet engineering is a promising technique applied to tissue engineering. This technique is capable of keeping extracellular matrix (ECM) and cell–cell interactions intact, which shows more advantages than traditional biodegradable scaffolds or cell suspension injections 17 . In this study, bladder smooth muscle cell (SMC) sheets were harvested to fabricate engineered smooth muscle tissues, as the muscle layer is the main part of the bladder tissue. To construct vascularized engineered tissue with its own vascular pedicle, we developed a three-stage rabbit model combining expander capsule tissue with cell sheet engineering. First, we transplanted a skin expander next to the separated SCIs, followed by expansion for different times, to identify which time point is the most effective for constructing an axial vascular bed. In the second stage, we compared the outcome of SMC sheets transplanted onto two different vascular beds including the expander capsule and subcutaneous tissue, which was widely used in other studies for vascularization. Finally, we transplanted multilayered SMC sheets onto the axial capsule bed twice to verify whether multi-transplantation of cell sheets was feasible to fabricate thick pedicled engineered tissues.
The objective of this study was to explore the feasibility of the tissue expander capsule as a novel platform for vascularizing autologous cell sheets and fabricating vascularized engineered tissue with its own axial vessels, which can deliver nutrients and oxygen immediately after pedicled transfer to the target region.
Materials and Methods
Animals
For the three stages of the animal experiments, male New Zealand white rabbits (stage I: n = 17; stage II: n = 15; stage III: n = 5) weighing 2.0–2.5 kg (provided by the Department of Laboratory Animal Science, School of Medicine, Shanghai Jiao Tong University) were used. All animal procedures were approved by the Institutional Animal Care and Use Committee of Shanghai Jiao Tong University School of Medicine (Ethics Number: B-2015-009).
Expander Capsule Induction
Rabbits were kept on clear fluid 12 h before surgery and received cefuroxime sodium (50 mg/kg, Esseti FarmaceuticiS.r.l, Napoli, Italy) immediately before surgery. Following general anesthesia with 2% pentobarbital sodium (30 mg/kg, Sigma-Aldrich, St Louis, MO, USA), skin incisions were cut in the bilateral inguinal region (Fig. 1A), and SCIs surrounded by the inguinal fat pad were carefully isolated (Fig. 1B). A sterile, spherical skin expander (10 ml) was placed close to the separated SCIs below the bilateral abdominal skin to induce a vascularized capsule (Fig. 1C). Three milliliters of sterile saline solution was injected into the expander before the skin incision was closed with a 4–0 nylon interrupted suture (Fig. 1D). The incisions were allowed to heal for approximately 8 days. Following this, the expanders were repeatedly inflated with 3 ml of saline solution with a 2-day interval, increasing the amount to 12 ml (Fig. 1E). To identify which time point is the most appropriate for constructing an axial vascular bed, the expander capsule was photographed and resected for histological analyses 1 d, 1 week, 2 weeks, 3 weeks, and 4 weeks, respectively, after the expander was fully expanded (each n = 6). Furthermore, to verify the blood perfusion within the capsule tissue via the axial artery, 10 ml of heparinized Indian ink was injected from an inlet of the homolateral femoral artery, and the capsule tissue with axial vessels was then resected and fixed for histological analyses (n = 4).

The induction and evaluation of the expander capsule. (A–E) A skin expander was placed close to the separated SCIs below the abdominal skin, after which the skin incision was closed with a interrupted suture. Then the expanders were repeatedly inflated with saline solution to induce a vascularized capsule tissue. (F–J) The gross appearance of the expander capsules at five different time points: 1 d, 1 week, 2 weeks, 3 weeks, 4 weeks, respectively, after the expander was fully expanded. (K–O) Masson staining of the expander capsules at five different time points, respectively. (P–T) CD31 staining of the expander capsules at five different time points, respectively. (U) Quantitative comparisons of CD31 positive microvessels within the expander capsules at five different time points, which indicted the vessel density of the capsule tissue 1 week after full expansion was significantly greater than those at other time points. The data are expressed as the mean ± SD, and the error bars represent the SD. **P < 0.01, compared with other time points. (V) The macroscopic appearance of the expander capsules infused with India ink. (W, X) Cross-sections of ink-perfused capsule tissue showed that the vascular network within the capsule was filled with the black ink, indicating that the blood supply of capsule was derived from the axial artery. Scale bar = 200 μm (K–T, W); Scale bar = 50 μm (X).
Bladder Muscular Layer Biopsy
Rabbits were anesthetized as described above, and a 3-cm vertical midline incision was made in the lower abdomen to expose the bladder. Next, 5 ml of sterile saline solution was injected into the bottom of the fat paddle at the vesical vertex to form a water sac, which was resected with ophthalmic scissors against the surface of the underlying muscle layer. Afterward, a small opening was cut into the exposed muscle layer and bluntly separated from its underlying mucosa layer with a curved clamp. Finally, an approximately 10 × 5 mm strip was excised from the muscle layer without disruption of the urothelium. The muscular incision was then sutured with 6–0 polyglycolic acid sutures.
SMC Sheet Fabrication
Muscle biopsies were incised into segments of approximately 2 mm2 with dissection scissors and incubated in Dulbecco’s modified Eagle medium (DMEM; Gibco, Grand Island, NY, USA) containing 1.5 mg/ml of collagenase NB4 (Serva, Heidelberg, Germany) and 1.0 mg/ml of dispase II (Roche, Mannheim, Germany) at 37°C for 30 min to create single-cell suspensions. The digestion was stopped by adding 1 ml of DMEM supplemented with 10% fetal bovine serum (Gibco). The isolated cells were filtered through a 70 μm cell strainer (Falcon, Corning, NY, USA), followed by centrifugation at 300 × g for 6 min. The pellets were suspended with smooth muscle growth medium (SmGM-2, Lonza, Basel, Switzerland), and the number of cells was measured using trypan blue assay. Isolated cells were plated at a density of 5 × 104 cells/cm2 and placed in a tissue culture incubator. The growth medium was refreshed every 2 days, and the cells at passage 0 were subcultured after reaching 80% confluence. Cells at passages 3 to 5 were treated with 0.25% trypsin-EDTA (Gibco) to create single-cell suspensions. Then, cells were plated onto 35-mm temperature-responsive culture dishes (UpCell, CellSeed, Tokyo, Japan) at a density of 1 × 106 cells/dish. Due to the high seeding density, the growth medium was changed every day. The cells exceeded confluence after 5 days and were transferred to a culture incubator set at 25°C for 30 min to harvest intact sheets. To trace the SMCs within the cell sheet grafts, cell sheets were labeled with CM-DiI (Invitrogen, Carlsbad, CA, USA) for 15 min in the culture incubator. The harvested cell sheets were transferred in vivo within 30 min.
Cell Sheet Viability Assay
To assess the viability of the cell sheets before and after harvest, a Live/Dead Viability/Cytotoxicity Kit (Invitrogen) was used. Green-fluorescent calcein-AM was used to indicate viable cells, while red-fluorescent ethidium homodimer-1 was used to indicate dead cells. Cell sheets before and after harvest were washed with phosphate buffered saline (PBS; Gibco) twice to eliminate the serum esterase activity present in the growth medium and then incubated in 2 μM of calcein-AM and 4 μM of ethidium homodimer-1 in Dulbecco’s PBS (DPBS; Gibco) at room temperature for 40 min. The stained cells were imaged by fluorescence microscopy (DM2500, Leica, Wetzlar, Germany). Cells killed using 70% methanol for 30 min were also stained as control. Image analysis (n = 6) was used to calculate the area of the both dyes relative to the total area to quantify the viability using ImageJ software.
Transplantation of Autologous SMC Sheets
Cell sheets were transplanted onto both the expander capsule and dorsal subcutaneous tissue in each rabbit. For the transplantation onto the expander capsule, the rabbits were prepared as described for the expander capsule induction to fully expose the capsule tissue which was used as a vascular bed to adopt cell sheets to construct vascularized engineered tissues. SMC sheets (1–3 layer, each n = 10) labeled with CM-DiI were placed onto a non-adhesive polyethylene terephthalate supporting sheet (2 × 1.5 cm) and applied face down onto the bilateral expander capsule. Then, the supporting sheet was pressed gently for 30 s and carefully removed, leaving the cell sheets on the transplanted area. With regard to 2 or 3-layer cell sheet transplantation, the cell sheet was again transplanted in the same manner with a time interval of 5 min to ensure tight attachment to the host tissue or previous transplanted cell sheets. The transplanted cell sheets were covered with 0.3 mm-thick silicone membranes to prevent adhesion and vascularization from the upper skin. Finally, skin incisions were closed with 5-0 nylon interrupted sutures. For the transplantation onto subcutaneous tissue, two L-shaped incisions (2 × 2 cm) were bilaterally made in the dorsal skin, and the incised skin was lifted to expose the underlying tissue. Then, SMC sheets (1–3 layer, each n = 10) labeled with CM-DiI were transplanted as described above. The grafts were resected and fixed at days 2 and 7, respectively, after transplantation.
Multi-Transplantation of SMC Sheets to Construct Pedicled Tissues
After the vascularized expander capsule was induced and SMC sheets were fabricated, male rabbits (n = 5) were anesthetized, and the expander capsule was fully exposed. Three-layer SMC sheets were transplanted onto the capsule bed according to the method mentioned above. Two days later, further three-layer cell sheets were repeatedly transplanted. The transplanted cell sheets were followed up for 1 month.
Morphological and Histological Analyses
Macroscopic images of induced expander capsules were photographed by a digital camera (ILCE-6000 L, SONY, Tokyo, Japan) at five different time points. Tissue expander capsules, cell sheets, parts of the subcutaneous tissue and expander capsule transplanted with SMC sheets were harvested at the specific times mentioned above. All samples were fixed with 4% paraformaldehyde, embedded in paraffin, and sagittally sectioned into 4 µm-thick sections. Hematoxylin and eosin (HE) or Masson’s trichrome staining were performed according to the standard staining protocols. For immunohistochemistry, 4 µm-thick sections were deparaffinized and blocked with donkey serum for 30 min. To accurately measure the thickness of the SMC sheets transplanted in vivo, sections were incubated with mouse anti-alpha smooth muscle actin (α-SMA) monoclonal antibody (1:1000; Abcam, Cambridge, UK). For the valuation of vascularization, sections were incubated with mouse anti-CD31 monoclonal antibody (1:500; Abcam). To verify the proliferative potential of transplanted SMC sheets, sections were incubated with mouse anti-Ki-67 monoclonal antibody (1:200; Novus Biologicals, Littleton, CO, USA). Then, specimens were treated with an EnVision™ Detection Kit (Dako, Glostrup, Denmark). For the identification of SMC sheets, sections were incubated with mouse anti-α-SMA monoclonal antibody (1:200; Abcam) and goat anti-desmin polyclonal antibody (1:100; Abcam). To evaluate the apoptosis and proliferation index of harvested SMC sheets, sections were incubated with mouse anti-Caspase-3 monoclonal antibody (1:50; Novus Biologicals) and mouse anti-Ki-67 monoclonal antibody (1:100; Novus Biologicals). To identify the existence of ECM, sections were incubated with anti-laminin (1:100; Invitrogen) and anti-collagen Ⅳ polyclonal antibody (1:100; Invitrogen). Sections were then incubated at room temperature for 1 h with appropriate fluorescence-labeled secondary antibodies: Alexa Fluor 488-labeled donkey anti-goat IgG antibody (1:200; Abcam), Alexa Fluor 594-labeled donkey anti-rabbit IgG antibody (1:300; Abcam), and Alexa Fluor 594-labeled donkey anti-mouse IgG antibody (1:200; Abcam). To detect the fluorescence of cells which were labeled with CM-DiI, frozen cross-sections of the resected grafts were sectioned sagittally into 5 μm slices. Cell nuclei were counterstained by ProLong Gold anti-fade reagent with 4’, 6-diamidino-2-phenylindole (DAPI; Invitrogen). The images were observed by fluorescence microscopy (Leica). The number of vessels was quantified at days 2 and 7 postoperative in the cell sheet grafts. Six different fields (0.01 mm2) in a 40× magnification viewing field were chosen and the number of CD31-positive lumens was counted. The density of the blood vessels was reported as mean values ± the standard deviation per square millimeter. ImageJ software was used for morphometric quantitative analyses.
In Vivo Apoptosis Assay
Two days after transplantation, the resected cell sheet grafts were detected with TUNEL staining using a cell death detection kit (TMR red, Roche) following the manufacturer’s instructions. Six microscopic fields (at 400×) of each slide were randomly selected and photographed. The number of apoptotic cells within grafts was counted separately with ImageJ software. Apoptosis assay was expressed as the percentage of TUNEL-positive cells in total cells (DAPI).
Statistical Analyses
Data were expressed as the mean ± standard deviation (SD). Statistical analyses using the Student’s t-test were performed for two-group comparisons. Multiple comparisons among three or more groups were performed using one-way analysis of variance (ANOVA) or two-way ANOVA according to the variable (GraphPad Prism v6.01). The P value <0.05 was considered statistically significant.
Results
Characterization of the Induced Expander Capsule
To determine which time point is the most effective for constructing an axial vascular bed, we set five different time points. A macroscopic vascularized capsule tissue was consistently found around the skin expander after induction at five time points (Fig. 1F–J). SCIs were located in the center of the capsule tissue as axial vessels. In addition, numerous small vessels were observed originating from the axial vessels. Expander capsules were resected and fixed for histological analyses at different time points. Masson staining showed that the capsule tissue consisted of three layers (Fig. 1K–O): cellular layer, central layer, and fibrous layer. The thin cellular layer, which is closest to the expander, contains fibroblasts, inflammatory cells, and a few collagen fibers. The central layer mainly consists of loose collagen fibers, fibroblasts, and well-developed arterioles, venules, and capillaries. The fibrous layer mainly consists of dense collagen fibers and axial vessels. As a vascular bed, vessel density is a pivotal parameter to be considered, and immunostaining of CD31 was conducted (Fig. 1P–T). Quantitative comparisons indicated that vessel density of the capsule tissue 1 week after full expansion (160.0 ± 20.9/mm2) was significantly greater than those at other time points (P < 0.01) (Fig. 1U). Furthermore, the results of Indian ink injection showed that the ink first flowed through the femoral artery and superficial circumflex iliac artery, and then diffused into the capsule tissue, which was confirmed by the macroscopic observation (Fig. 1V). Cross-sections of ink-perfused capsule tissue indicated that the vascular network within the capsule was filled with the black ink (Fig. 1W, X), confirming our hypothesis that axial SCIs sprouted new blood vessels into capsule tissue so that the blood supply of the capsule was indeed derived from the axial artery.
Characterization of SMC Sheets
Bladder SMCs were successfully isolated and exhibited a characteristic spindle morphology at passage 0 (Fig. 2A). The SMCs at passages 3 to 5 were trypsinized and plated onto temperature-responsive culture dishes at a high density. The SMCs became excessively confluent after 5-day culture (Fig. 2B). Afterward, SMC sheets were harvested by reducing the culture temperature from 37°C to 25°C for approximately 30 min. The diameter of those cell sheets shrunk horizontally to approximately 1 cm due to the contraction of the ECM (Fig. 2C). As a result, harvested SMC sheets consisted of 3–5 cell layers, and the thickness of the cell sheets was approximately 50 μm (Fig. 2D). Immunofluorescent staining demonstrated that the cell sheets expressed typical SMC markers, such as α-SMA (Fig. 2E) and desmin (Fig. 2F), and cell nuclei were counterstained with DAPI (Fig. 2G). The merged image (Fig. 2H) was in accordance with our previous study 18 . Cell viability assay showed that almost all SMCs before harvest were live (Fig. 2I–K), while the control SMCs treated with methanol showed extensively dead (Fig. 2L). The cell sheet harvest did not damage the cells (Fig. 2M–O). Quantitatively, the SMC sheets before harvest showed 99.0% (±0.4%) live cells, compared with 98.6% (±0.5%) for the cell sheets after harvest (P > 0.05) (Fig. 2P). Immunofluorescent staining of Caspase-3 also demonstrated that few cells presented apoptosis in the SMC sheets (Fig. 2Q). Furthermore, immunofluorescent staining of Ki-67 (Fig. 2R) showed that approximately 15.3% of cells remained proliferative, although the cells were very dense and exhibited proliferation inhibition. ECM is critical for high cell transplantation efficiency. Immunofluorescent staining demonstrated that collagen IV (Fig. 2S) and laminin (Fig. 2T) both existed extensively in the cell sheets.

Characterization of SMC sheets. (A) Phase-contrast micrographs of rabbit primary bladder SMCs. (B, C) Phase-contrast and macroscopic images of SMC sheets. (D) Cross-sectional views of SMC sheets colored by hematoxylin and eosin staining. (E–H) The SMC sheet was stained with α-SMA (red color) and anti-desmin (green color) antibodies, while the nuclei were stained with DAPI (blue color). (I–K) Viability assay of the SMCs after 5-day culture. Live cells (green color); dead cells (red color). (L) Viability assay of the SMCs killed by 70% methanol as control. (M–O) Viability assay of the harvested SMC sheet. Live cells (green color); dead cells (red color). (P) For the viability, there was no significant difference between the sheets before and after harvest. The data are expressed as the mean ± SD, and the error bars represent the SD. n.s. denotes not significant. (Q–T) Immunofluorescent staining of Caspase-3, Ki-67, collagen IV and laminin (red color), respectively; nuclei were counterstained with DAPI (blue color). Scale bar = 100 μm (A, B, I–O); Scale bar = 50 μm (D–H, Q–T).
Outcome of SMC Sheets Transplanted onto Two Vascular Beds
The fate of cell sheets transplanted in vivo at the early stage is critical for constructing functional engineered tissues, and we set two time points: day 2 and day 7, respectively, after transplantation. CM-DiI, a red-fluorescent dye well suited for monitoring cells, was used to track cell sheets.
On day 2, fluorescence microscopy of the cell sheets showed that cell sheets were successfully transplanted onto both vascular beds (Fig. 3, first–third column). The width of red fluorescence increased with the number of cell sheets, while the fluorescence intensity in the expander capsule transplantation group was stronger than that in the subcutaneous transplantation group. HE staining showed engineered smooth muscle tissues located on the surface of capsule and subcutaneous tissue, and erythrocytes were found in the vessels of cell sheet grafts (Fig. 3, fourth column), indicating that the vasculature of the grafts had connected to the host circulation. The thickness of the transplanted grafts was measured at five points in the α-SMA staining images (Fig. 3, fifth column) and the mean was calculated. Triplicate samples were measured for each group. There was significant difference (P < 0.01) between the SMC sheets transplanted onto capsule tissue and those transplanted onto subcutaneous tissue (1-layer: 148.0 ± 12.0 μm vs. 87.7 ± 6.3 μm; 2-layer: 211.0 ± 7.4 μm vs. 133.2 ± 9.4 μm; 3-layer: 269.5 ± 7.0 μm vs. 165.2 ± 14.3 μm, each n = 5) (Fig. 5A). Meanwhile, vessel density is a vital factor for engineered tissues. We compared the vessel density of cell sheet grafts on two vascular beds (Fig. 3, sixth column). When the SMC sheets were transplanted onto capsule tissue, a significantly higher density of blood vessels (P < 0.01) in the cell sheets was observed 2 days after implantation, compared with the SMC sheets transplanted onto subcutaneous tissue (1-layer: 440.0 ± 54.8/mm2 vs. 140.0 ± 54.8/mm2; 2-layer: 580.0 ± 83.7/mm2 vs. 300.0 ± 70.7/mm2; 3-layer: 360.0 ± 54.8/mm2 vs. 160.0 ± 54.8/mm2, each n = 5) (Fig. 5B). We next evaluated cell survival with TUNEL assay (Fig. 4). For the 1-layer and 2-layer SMC sheets transplanted onto two vascular beds, almost all cells of the grafts were live 2 days after transplantation. TUNEL assay also indicated a remarkable reduction of apoptosis in the 3-layer SMC sheets transplanted onto capsule tissue compared with those transplanted onto subcutaneous tissue. While 19.2% (±3.2%) of nuclei were positive for the latter, TUNEL-positive nuclei were reduced to 3.1% (±1.0%) in the capsule transplantation group (P < 0.01) (Fig. 5C).
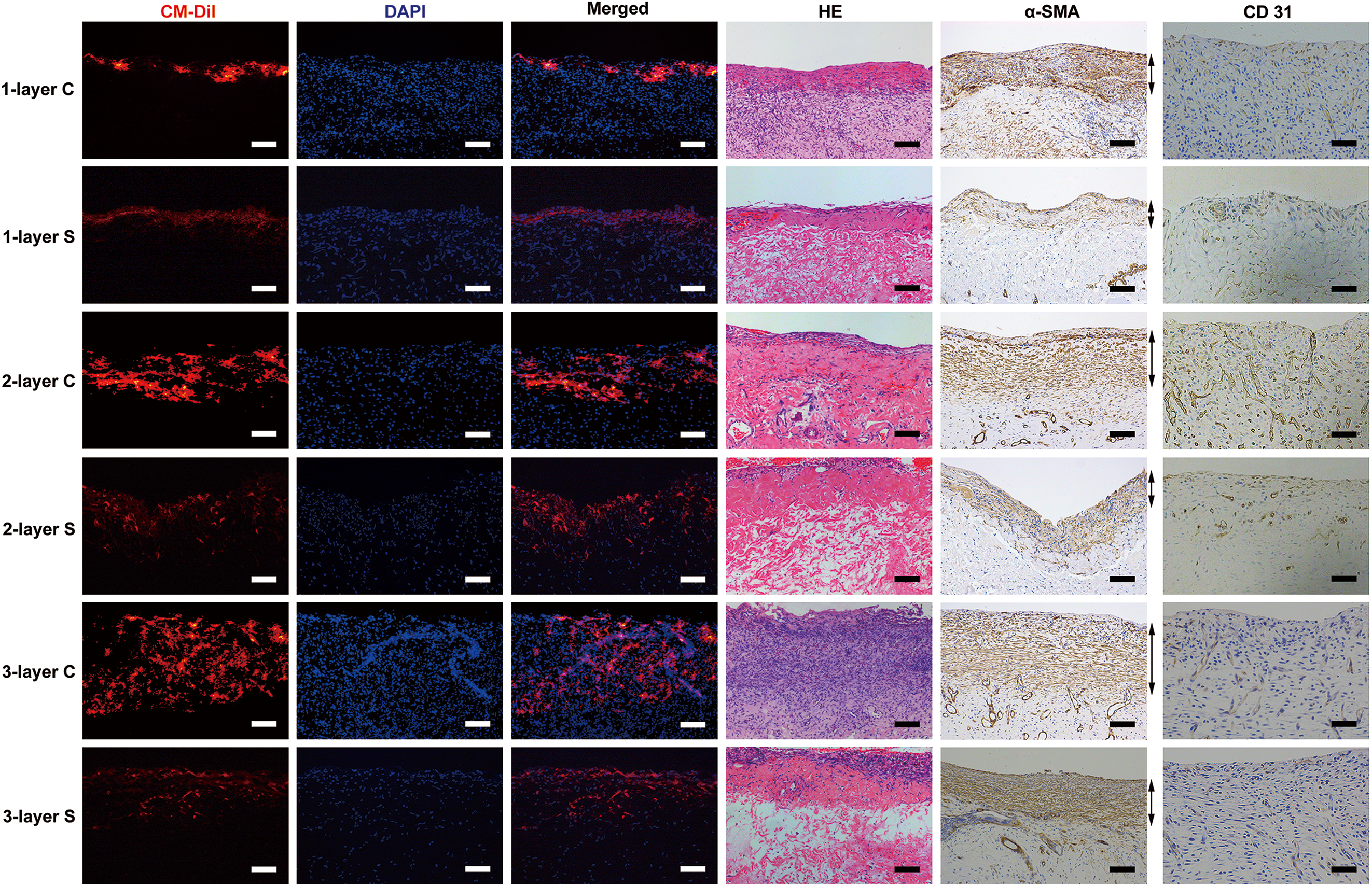
Outcome of SMC sheets transplanted onto two vascular beds on day 2. The transplanted cell sheets were labeled with CM-DiI (red color; first column). The width of red-fluorescent dye increased with the number of cell sheets, while the fluorescence intensity in the expander capsule transplantation group was stronger than that in the subcutaneous transplantation group. Nuclei were counterstained with DAPI (blue color; second column). The first and second column images were merged (third column). Hematoxylin and eosin staining of transplanted SMC sheets onto two vascular beds on day 2 (fourth column) showed engineered smooth muscle tissues located on the surface of two vascular beds and erythrocytes were found in the vessels of cell sheet grafts. Immunostaining of α-SMA was conducted to measure the thickness of cell sheet grafts (fifth column). Bidirectional arrows indicate viable cell sheet grafts. Immunostaining of CD31 was conducted to evaluate vessel density of cell sheet grafts (sixth column). “1-layer C” denotes 1-layer SMC sheets transplanted onto the capsule tissue. “1-layer S” denotes 1-layer SMC sheets transplanted onto the subcutaneous tissue. “2-layer C” denotes 2-layer SMC sheets transplanted onto the capsule tissue. “2-layer S” denotes 2-layer SMC sheets transplanted onto the subcutaneous tissue. “3-layer C” denotes 3-layer SMC sheets transplanted onto the capsule tissue. “3-layer S” denotes 3-layer SMC sheets transplanted onto the subcutaneous tissue. Scale bar = 100 μm (first–fifth column); Scale bar = 50 μm (sixth column).

TUNEL staining of cell sheet grafts 2 days after transplantation. For the one-layer and two-layer SMC sheets transplanted onto two vascular beds, almost all cells within cell sheet grafts were live. However, for the three-layer SMC sheets, apoptosis in the subcutaneous transplantation group showed an observed increase compared with that in the capsule transplantation group. TUNEL-positive nuclei (red color); nuclei were counterstained with DAPI (blue color). Scale bar = 50 μm.

Quantitative comparisons of thickness, vessel density and apoptosis of cell sheet grafts onto two vascular beds on day 2. (A) The thickness of SMC sheets transplanted onto capsule tissue was significantly larger than that of SMC sheets transplanted onto subcutaneous tissue for one-layer, two-layer, and three-layer, respectively. (B) The vessel density of SMC sheets transplanted onto capsule tissue was significantly greater than that of SMC sheets transplanted onto subcutaneous tissue for one-layer, two-layer, and three-layer, respectively. (C) TUNEL assay showed a remarkable reduction of apoptosis in the three-layer SMC sheets transplanted onto capsule tissue compared with those transplanted onto subcutaneous tissue. The data are expressed as the mean ± SD, and the error bars represent the SD. **P < 0.01.
On day 7, fluorescent images showed that the width of cell sheets traced with CM-DiI increased compared with that on day 2, indicating that the transplanted cells proliferated and formed thicker tissues. Meanwhile, some SMCs traced with red fluorescence migrated into host tissues (Fig. 6, first–third column). HE staining also showed that engineered smooth muscle tissues on two vascular beds became thicker over time and contained plenty of small vessels, which were filled with red blood cells (Fig. 6, fourth column). The thickness of transplanted SMC sheets was also measured by α-SMA staining (Fig. 6, fifth column). As with the results on day 2, there were significant difference (P < 0.01) between the SMC sheets transplanted onto capsule tissue and those transplanted onto subcutaneous tissue (1-layer: 245.2 ± 17.9 μm vs. 144.2 ± 13.1 μm; 2-layer: 355.0 ± 9.6 μm vs. 222.8 ± 26.4 μm; 3-layer: 499.5 ±22.3 μm vs. 244.3 ± 10.3 μm, each n = 5) (Fig. 7A), which indicated that the former vascular bed might be more efficient for promoting graft growth. Immunostaining of CD31 was conducted to evaluate the vessel density of the grafts (Fig. 6, sixth column). Quantitative analyses showed there were also statistical difference (P < 0.05) between the SMC sheets transplanted onto capsule tissue and those transplanted onto subcutaneous tissue (1-layer: 440.0 ± 114.0/mm2 vs. 260.0 ± 54.8/mm2; 2-layer: 480.0 ± 83.7/mm2 vs. 280.0 ± 44.7/mm2; 3-layer: 680.0 ± 83.7/mm2 vs. 340.0 ± 89.4/mm2, each n = 5) (Fig. 7B). These data also proved that the axial capsule vascular bed was more favorable to the vascularization of transplants than subcutaneous tissue.

Outcome of SMC sheets transplanted onto two vascular beds on day 7. The transplanted cell sheets were labeled with CM-DiI (red color; first column). The width of cell sheets traced with red fluorescence increased compared with those on day 2, indicating that the transplanted cells proliferated and formed thicker tissues. Nuclei were counterstained with DAPI (blue color; second column). The first and second column images were merged (third column). Hematoxylin and eosin staining of transplanted SMC sheets onto two vascular beds on day 7 showed engineered smooth muscle tissues on two vascular beds became thicker and contained plenty of small functional vessels (fourth column). Immunostaining of α-SMA was conducted to measure the thickness of cell sheet grafts (fifth column). Bidirectional arrows indicate viable cell sheet grafts. Immunostaining of CD31 was conducted to evaluate vessel density of cell sheet grafts (sixth column). The denotations are the same as those of Fig. 3. Scale bar = 100 μm (first–fifth column); Scale bar = 50 μm (sixth column).
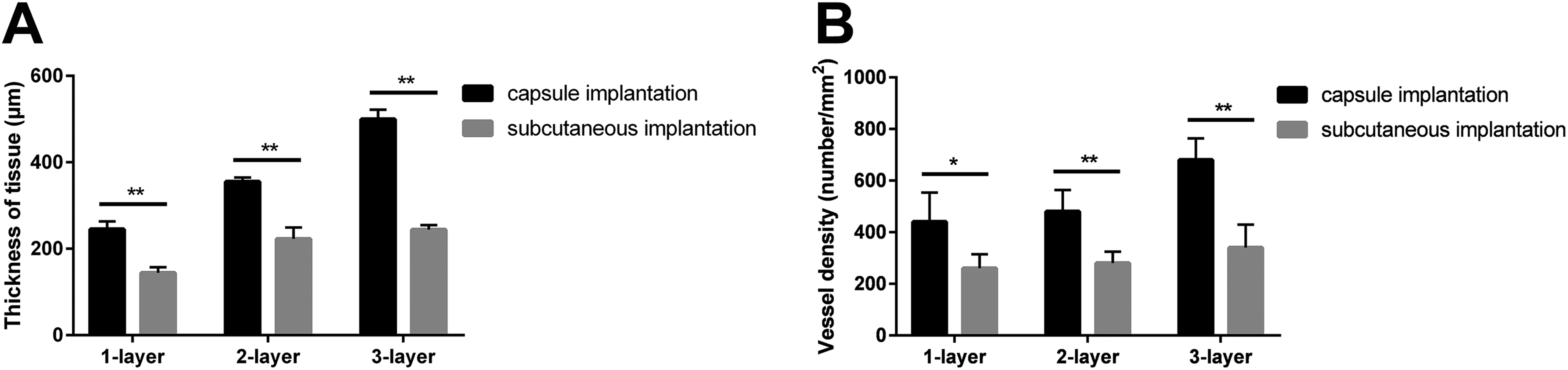
Quantitative comparisons of thickness and vessel density of cell sheet grafts onto two vascular beds on day 7. (A) The thickness of SMC sheets transplanted onto capsule tissue was significantly larger than that of SMC sheets transplanted onto subcutaneous tissue for one-layer, two-layer, and three-layer, respectively. (B) The vessel density of SMC sheets transplanted onto capsule tissue was significantly greater than that of SMC sheets transplanted onto subcutaneous tissue for one-layer, two-layer, and three-layer, respectively. The data are expressed as the mean ± SD, and the error bars represent the SD. *P < 0.05, **P < 0.01.
Thick Pedicled Smooth Muscle Tissues Constructed by Multi-Transplantation
Multi-transplantation of cell sheets after a certain time interval, which generates sufficient vascularization within the previously implanted cell sheets, could overcome the limit of cell sheet tissue thickness. The three-layer SMC sheets transplanted onto axial capsule tissue completely integrated with the vascular bed after 2 days, which was the basis for multi-transplantation. After 1 month, the transplanted six-layer SMC sheets formed macroscopically viable tissue, which could be easily distinguished from the surrounding capsule tissue (Fig. 8A). Macroscopically, the resected grafts contained axial vessels (Fig. 8B). Fluorescent images showed that the cells traced with CM-DiI still existed, and the fluorescence became sparse (Fig. 8C), indicting the transplanted cell sheets had proliferated since transplantation. Masson staining showed that the cell sheet graft was stratified (Fig. 8D): a thin layer of fibrous tissue located between two three-layer SMC sheet grafts. In addition, the graft was mainly composed of layered smooth muscle tissues, with less fibrous tissue distributed among the former. In regard to the thickness of the transplanted grafts, three points in the Masson staining images (n = 5) were randomly selected and the mean was calculated. The thickness of six-layer transplanted sheets after 1 month was 843.9 ± 39.8 μm, which had remarkably increased since transplantation. Immunostaining of Ki-67 clearly demonstrated that plenty of proliferative SMCs existed in the grafts (Fig. 8E).

Thick pedicled smooth muscle tissues constructed by multi-transplantation of SMC sheets. (A) The macroscopic image of six-layer SMC sheets transplanted onto axial capsule tissue after 1 month. The dashed lines indicate the cell sheet graft. (B) The resected grafts contained axial vessels. (C) Fluorescent images showed the cells traced with CM-DiI (red color) still existed. Nuclei were counterstained with DAPI (blue color). (D) Masson staining showed the cell sheet graft was stratified and mainly composed of layered smooth muscle tissues. (E) Immunostaining of Ki-67 showed that plenty of proliferative SMCs existed in the grafts. Scale bar = 200 μm (C, D); Scale bar = 50 μm (E).
Discussion
In the current study, we have shown the capsule tissue can serve as an axial vascular bed for constructing vascularized engineered tissue with its own axial vessels using cell sheet engineering. When repairing damaged organs or tissues, we can choose large vessels, which are adjacent to the target organ or tissue and can be sacrificed without sequelae, as axial vessels to induce an axial capsule vascular bed. Then, cell sheets or cell-scaffold composites can be transplanted onto the vascular bed for vascularization and subsequent pedicled transfer without vascular suture. This study paves a new way for the vascularization of engineered tissues.
For successful vascularization of engineered tissues, it is necessary to develop strategies to accelerate the formation of the vascular system, inosculation with host vasculature, and succeeding blood perfusion into the engineered tissues. However, under the current technical conditions, the construction of an engineered tissue with its own fully functional vasculature in vitro seems distant 9,19,20 . In vivo prevascularization has been proven as a novel promising vascularization strategy in recent years 21,22 . In this strategy, engineered tissues or constructs are vascularized at a temporary site in vivo prior to transplantation into the target position. During this period, called prevascularization, the existing vessels of the body sprout into the engineered tissues to form a new microvascular network. The frequently researched temporary vascular bed includes subcutaneous tissue, fat tissue, muscle pocket, and omentum 21,23 –26 . However, it still takes a relatively long time to reach microvascular anastomosis between host and engineered tissues, which may cause apoptosis and thus restricts the clinical application of engineered tissues. Therefore, it is urgent to overcome the problem of vascularization within engineered tissues.
The capsule tissue has been shown to possess its own unique blood supply and contain extensive blood vessels 15,27 . In addition, the arteriovenous bundle technique has been proven to help to solve the problem of post-transplant vascularization 28,29 . Hence, the combination of capsule tissue and the arteriovenous bundle technique may be very promising to reach efficient vascularization within engineered tissues. The main purpose of the expander in clinical practice was to expand skin, and capsule tissue was confirmed to provide enough vascularity to support the skin graft 30,31 . However, the study of capsule tissue as a vascular bed in tissue engineering was rare 27 , and it was unknown at which time point the capsule tissue was the most vascularized. In this study, we set five time points after the skin expander was fully expanded. The macroscopic observation indicated that the capsule tissue was the most vascularized 1 week after full expansion. Masson’s trichrome staining indicated that the capsule tissue consisted of three layers: cellular layer, central layer, and fibrous layer, which was consistent with the experimental study performed by Kostakoğlu and colleagues 32 . The central layer consisting of abundant microvessels was relatively close to the silicone expander, which was convenient and minimally invasive for engineered-tissue implantation similar to the subcutaneous tissue. Vessel density is a key parameter to evaluate a vascular bed 33 , as the principal mechanism of vascularization by the vascular bed is sprouting angiogenesis, whereby endothelial cells branch out from existing blood vessels and expand into surrounding ischemic tissue to form a new vasculature 34,35 . Therefore, the efficiency of neovascularization increases with the vessel density of the vascular bed within limits. Quantitative comparisons of CD31-positive microvessels also identified that the capsule tissue was the most vascularized 1 week after full expansion, and could be used as an axial vascular bed for vascularization. Finally, we verified that the blood perfusion within the capsule tissue was derived from the SCI artery with Indian ink injection. This is the anatomic basis for constructing a pedicled flap and subsequent pedicled transfer.
Cell sheet engineering, which has advantages compared with other constructs, has been widely researched for the vascularization in tissue engineering 36 –38 . This technique allows for a noninvasive harvest of cultured cells as an intact sheet, including the ECM, without any enzymatic digestion. In this study, we successfully harvested bladder SMC sheets using thermo-responsive culture dishes. The harvested cell sheets consisted of multilayer cells because of cytoskeleton reassembly and contraction of the ECM 39 . In addition, the SMC sheets before and after harvest both showed high cell viability, which is a vital requirement for tissue engineering. Cell-generated ECM is probably more effective in regulating cell growth and maturation than artificial scaffolds 14 . ECM molecules are crucial for the attachment of transplanted cells to the target site without suture, and assure the implanted cells are supplied by diffusion until revascularization. Previous research has shown the ECM of intracorporal individual bladder SMCs mainly consists of collagen IV and laminin 40 . We also verified this point in bladder SMC sheets. Many previous studies have co-cultured endothelial cells or endothelial progenitor cells with other cell types, resulting in a capillary-like network formation in vitro 11,37,41 . However, in the present study, only SMCs were cultured to form cell sheets, avoiding the interference of endothelial cell network in cell sheets with the capillary sprouting from two vascular beds.
Vascularizing engineered tissues under the skin is regarded as the safest, simplest, and least invasive in vivo prevascularization strategy 42 . However, it has its own limitations, as graft failure frequently occurs due to insufficient infiltration of functional vessels 43 –45 . In this research, we fabricated a novel axial vascular bed, which is also located under the skin, and compared the outcomes of SMC sheet transplantation onto two different vascular beds, the expander capsule and classical dorsal subcutaneous tissue. Meanwhile, we set two evaluation points: day 2 and day 7, respectively, after transplantation. On day 2, all cell sheets were successfully engrafted onto two vascular beds. Thus, it was verified that ECM in the cell sheets was able to adhere to both vascular beds tightly. Moreover, the fluorescence intensity in the expander capsule transplantation group was higher than in the subcutaneous transplantation group, indicating the interaction between the transplanted cell sheets and the capsule was stronger and more live SMCs existed. Regarding the thickness of transplanted cell sheets, the thickness of SMC sheets transplanted onto capsule tissue was significantly greater than those transplanted onto subcutaneous tissue, suggesting that the capsule tissue was more efficient for thicker construct incubation. In addition, the vessel density of SMC sheets transplanted onto capsule tissue was higher compared with the ones transplanted onto subcutaneous tissue, indicating the capsule vascular bed was better for vascularizing constructs. The results of TUNEL assay also verified the superiority of the capsule vascular bed. On day 7, the quantitative comparison of thickness of transplanted cell sheets showed that the SMC sheets transplanted onto capsule vascular bed were also significantly thicker than the ones transplanted onto dorsal subcutaneous tissue. This is principally because the denser blood vessels appeared to supply more oxygen and nutrients to the SMC sheets, leading to the better survival and proliferation in vivo, which was verified by the fact that the comparative results of thickness and vessel density were consistent. Moreover, the microenvironment of the capsule vascular bed, including inflammation modulation, cytokines, and their receptors, may be more efficient for transplant growth 46 . However, the cellular and molecular mechanisms behind this enhancement are unknown and need further study. Quantitative analyses of CD31-positive microvessels within cell sheet grafts also demonstrated that the capsule vascular bed was more favorable to vascularization. As the vessel density of the capsule tissue 1 week after full expansion was significantly greater than that of traditional subcutaneous tissue, we speculate that appropriately denser vessels in the vascular bed could contribute to more efficient sprouting into cell sheet grafts and enhanced neovascularization. As to the angiogenic mechanisms, inflammatory cells or noncoding RNA may be involved 47,48 . Further research is needed to clarify these points.
The above results indicated that three-layer SMC sheets (approximately 150 μm) could be successfully transplanted onto the capsule vascular bed at one time, which was inconsistent with the previous opinion that cell sheet grafts more than 100 μm could not be successfully transplanted at single time 49,50 . The possible reasons include the superiority of the capsule vascular bed and different responses to hypoxia between bladder SMCs and cardiomyocytes researched in previous studies. However, for the thickness and vessel density on day 7, there was no significant difference (P > 0.05) between the two-layer and the three-layer SMC sheets transplanted onto subcutaneous tissue, indicating that the thickness of SMC sheets transplanted onto subcutaneous tissue at one time was also limited to approximately 100 μm, as with cardiomyocyte sheets. This indicated that the responses to hypoxia between bladder SMCs and cardiomyocytes were similar. In conclusion, the capsule vascular bed was more favorable to the growth and vascularization of engineered tissues than the subcutaneous tissue.
To overcome the problem of thickness limitation, multi-transplantation of cell sheets has been conducted to construct three-dimensional thicker tissues either in vivo or in vitro 49 –52 . However, these previous studies often sacrificed the femoral artery and vein, which could cause serious sequelae, or required a complex bioreactor system in vitro. The above factors limit the possibility of clinical practice. In this study, we transplanted multilayered SMC sheets onto the axial capsule bed twice to verify the feasibility of constructing thick pedicled tissues, which was convenient and minimally invasive. The engineered smooth muscle tissue derived from the transplanted SMC sheets was visually observed above the axial vessels, which indicated that the double three-layered SMC sheets successfully survived. The resected grafts could be observed containing axial vessels macroscopically. This is the anatomical basis for pedicled transfer, which could solve the problem of slow vascularization after transplantation. Histological analyses showed that layered smooth muscle tissue existed and the mean thickness exceeded 800 μm, which was significantly larger than the total thickness of six-layer SMC sheets in vitro (approximately 300 μm). The above results demonstrated the feasibility of constructing thick pedicled tissues on the axial capsule vascular bed by multi-transplanting autologous cell sheets.
Although the results of the present study are encouraging, some limitations still exist. While we found the superiority of the capsule vascular bed over dorsal subcutaneous tissue for incubating and vascularizing engineered tissues, the underlying mechanisms are not clearly understood. Regulating and optimizing a vascular bed at cellular and molecular levels may promote the vascularization of engineered tissues. Second, we merely explored the possibility of three-layer SMC sheets, while the maximum layer of SMC sheets which could be successfully transplanted on the axial capsule vascular bed at single time was not investigated. Recent studies have attempted to increase the maximum layer of transplanted cardiomyocyte sheets in a single procedure through the addition of VEGF-releasing mats or insertion of gelatin hydrogel microspheres 53,54 . When the thickness limitation is overcome, cell sheet engineering will provide groundbreaking treatment options for injured organs or tissues. Finally, as the main objective of this study was to explore the feasibility of constructing pedicled engineered tissue by combining the capsule tissue and cell sheet engineering, pedicled transfer of the flap was not conducted. This is what we will continue to research to repair adjacent injured bladder or urethra.
Conclusion
The most vascularized axial capsule tissue can be successfully induced 1 week after full expansion when a tissue expander is placed close to the separated SCIs, which is more favorable to the growth and vascularization of transplants than classical subcutaneous tissue. Furthermore, thick pedicled smooth muscle tissues can be constructed by multi-transplantation of cell sheets on the capsule bed. The combination of the axial capsule tissue and cell sheet engineering may provide an innovative strategy to overcome the problem of vascularization in tissue engineering.
Footnotes
Authors’ Note
Zhiming Jia and Hailin Guo contributed equally to this work.
Ethical Approval
The experimental protocols were approved by the Institutional Animal Care and Use Committee (IACUC) of Shanghai Jiao Tong University School of Medicine (B-2015-009).
Statement of Human and Animal Rights
All animals received care in accordance with the guidelines of IACUC and monitored by institutional veterinary staff.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by the National Natural Science Foundation of China (No. 81470911).