
Abstract
Back pain is a common health problem that reduces the quality of life for human beings worldwide. Several treatment modalities have been reported as effective for pain relief. Generally, patients often undergo surgical interventions as pain becomes intractable, after conservative treatment. With advances in surgical techniques, those choosing spinal surgery as an option have increased over time, and instrumentation is more popular than it was years ago. However, some patients still have back pain after spinal operations. The number of patients classified as having failed back surgery syndrome (FBSS) has increased over time as has the requirement for patients receiving long-term analgesics. Because pain relief is regarded as a human right, narcotics were prescribed more frequently than before. Narcotic addiction in patients with FBSS has become an important issue. Here, we review the prevalence of FBSS, the mechanism of narcotic addiction, and their correlations. Additionally, several potentially effective strategies for the prevention and treatment of narcotic addiction in FBSS patients are evaluated and discussed.
Keywords
Introduction
A narcotic, a drug which acts directly on the central nervous system (CNS), is originally defined as any psychoactive compound that induces sleeping or causes loss of feeling or paralysis. However, it has currently become associated with opiates and opioids, commonly morphine and heroin, as well as derivatives of many compounds found within raw opium latex. The major narcotics for clinical pain relief are morphine, codeine, fentanyl, tramadol and meperidine (Table 1). While thebaine is also considered a narcotic, it is a crucial precursor in the semi-synthesis of opioids such as oxycodone, oxymorphone, nalbuphine, naloxone, naltrexone, buprenorphine and etorphine, rather than being used therapeutically.
Major Narcotics for Pain Relief.

FBSS: failed back surgery syndrome.
Addiction is a chronic and persistent disease that is characterized by compulsive substance consumption in spite of disadvantageous consequences. It is also considered to be a brain disease because drugs change the brain structure and working models. These changes in the brain will be long-lasting and may lead to distorted thinking, behaviors, and body functions 1 –4 . Individuals with addiction have a strong urge to use a certain substance, such as alcohol or drugs. They keep using alcohol or drugs, even though they know it is harmful for their health. Narcotics, usually administered by oral or venous injection, are widely used in clinics because they are very effective for pain relief. Nonetheless, narcotics (e.g., morphine) are highly addictive due to the intense euphoria they induce, as well as reducing sensitivity to pain. Narcotic dependence can happen in a very short time that is generally both physical and psychological. Those who suffer from intense and chronic pain may feel that they need to take narcotics regularly, and in the long term. With most of these drugs, the longer that individuals take narcotics, the higher their tolerance levels become. Consequently, narcotic-addicted individuals will increase the dose as narcotic tolerance increases.
Back pain is a common reason for job-related disability, seeing a doctor, and for seeking medicinal therapies. It may cause discomfort, weakness, depression, and fatigue. Several etiologies represent the underlying causes of back pain, such as degeneration, trauma, neoplasms, inflammation, infections, and congenital abnormalities. Therapeutic strategies to alleviate intractable pain include analgesics, chiropractic treatment, back braces, physical therapy, spinal injections, and surgery 5 –8 . From 1998 onward, the annual number of spinal surgery procedures increased significantly in the United States and was as high as 488,300 in 2011 9,10 . Many patients, however, do not recover from their back pain, or the pain recurs later. Some patients even develop new back pain after surgical intervention. Failed back surgery syndrome (FBSS) was coined in 1991 when the term was used to describe patients who had chronic back pain after one or more spinal operations 11 . Chronic pain often refers to pain that persists for more than 3 months 12 . Previous articles provide various definitions or descriptions of FBSS 11,13 –16 . In 1994, the International Association for the Study of Pain defined FBSS as ‘lumbar (cervical) pain of unknown origin either persisting despite surgical intervention or appearing after surgical intervention 5 . Thomson et al. 13 proposed that FBSS could be defined as chronic back and leg pain that persists or recurs despite applying back surgery to the clinical pathway. Clearly, patients with FBSS often suffer from intractable chronic back pain after spinal surgery despite multiple types of treatment. Narcotics (e.g., morphine) are common medicines used in FBSS patients searching for greater pain control, but with the increased risk of triggering drug addiction.
In this article, we review the relationship between narcotic addiction and FBSS, and explore effective strategies for the prevention and treatment of narcotic addiction.
Incidence and Risk Factors of Failed Back Surgery Syndrome
According to quoted studies, the failure rate of spinal surgery ranges from 10% to 50% 13,17 –20 . In addition, approximately 10–40% of patients suffer from FBSS after lumbar spinal surgery 11,16 . The incidence of FBSS was reported to be as high as 80,000 patients per year 21 . Several studies discuss both risk factors and etiologies of FBSS 15,17,18,22,23 . Misdiagnosis (58%) was considered a major cause of FBSS 23 . Litigation and workers’ compensation were also mentioned 17 . The risk factors accounting for FBSS can be divided into structural and nonstructural reasons. Several structural etiologies cause FBSS, such as foraminal stenosis (25–29%), painful disk (20–22%), pseudoarthrosis (14%), neuropathic pain (10%), recurrent disk herniation (7–12%), iatrogenic instability (5%), facet pain (3%), and sacroiliac joint pain (2%) 22 . Additionally, surgical complications, loss of sagittal balance, progression of spinal degeneration, and altered spinal biomechanics are included 15 . However, various nonstructural reasons are also offering some examples to cause FBSS, such as misdiagnosis, psychological factors, obesity, smoking, litigation and workers’ compensation, as well as inappropriate surgical planning 15 . Patients with depression or anxiety often have persistent pain after spinal surgery 24 . Overweight patients have an increased risk of postoperative complications 25 as well. Smoking is also associated with an increased risk of impaired wound healing, rate of infections, and rate of nonunion 17 . All risk factors including structural and nonstructural reasons should be kept in mind when considering spinal surgery for back pain.
Treatments for Failed Back Surgery Syndrome
The therapeutic strategy for FBSS treatment includes multidisciplinary medical approaches (Table 2). Thomson et al. 16 found that 87% of patients with FBSS had tried at least four types of treatment to relieve pain. These methods included analgesics, antidepressants, anticonvulsants, physical rehabilitation, neurostimulation techniques, acupuncture, psychological interventions, and repeat surgery. There has been no gold standard treatment for FBSS. Chou et al. 26 reviewed the pros and cons of current medications prescribed for low back pain. They found good evidence of acute back pain relief by taking nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and skeletal muscle relaxants. Tricyclic antidepressants were considered effective for chronic low back pain. They also reported reasonable evidence with opioids, tramadol, benzodiazepines, and gabapentin for pain relief; corticosteroids were regarded as ineffective. Several reports provided evidence that gabapentin was effective in both reducing pain and improving function 27 . Pregabalin failed to demonstrate greater efficacy than placebos in chronic lumbosacral radiculopathy 28 . For physical therapy and behavioral rehabilitation in the treatment of FBSS, Amirdelfan et al. 29 found level II evidence in maintaining daily function. With regard to neuromodulation, such as spinal cord stimulation (SCS) in the treatment of FBSS, current studies focus on the benefits and risks in FBSS patients 29 –33 . In comparison with traditional and low-frequency SCS, high-frequency SCS at 10 kHz can be more effective for reducing both low back and leg pain 29,34 . For reoperations, surgeons need to assess the indication and benefits of repeat surgery. Although more than 50% of primary spinal surgery achieved their goals, less than 30%, 15%, and 5% of patients had good outcomes after the second, third, and fourth surgery, respectively 35 . In the treatment options for FBSS patients with refractory chronic pain, reoperation demonstrated the weakest evidence 29,33 . Therefore, reoperation should only be considered as a compromise for patients with signs of spinal instability and/or acute nerve pain that are unresponsive to conservative treatment. Although many different methods were employed in treating FBSS, up to 62% of patients used opioids to alleviate pain 16 .
Treatment Options in Patients with Failed Back Surgery Syndrome.
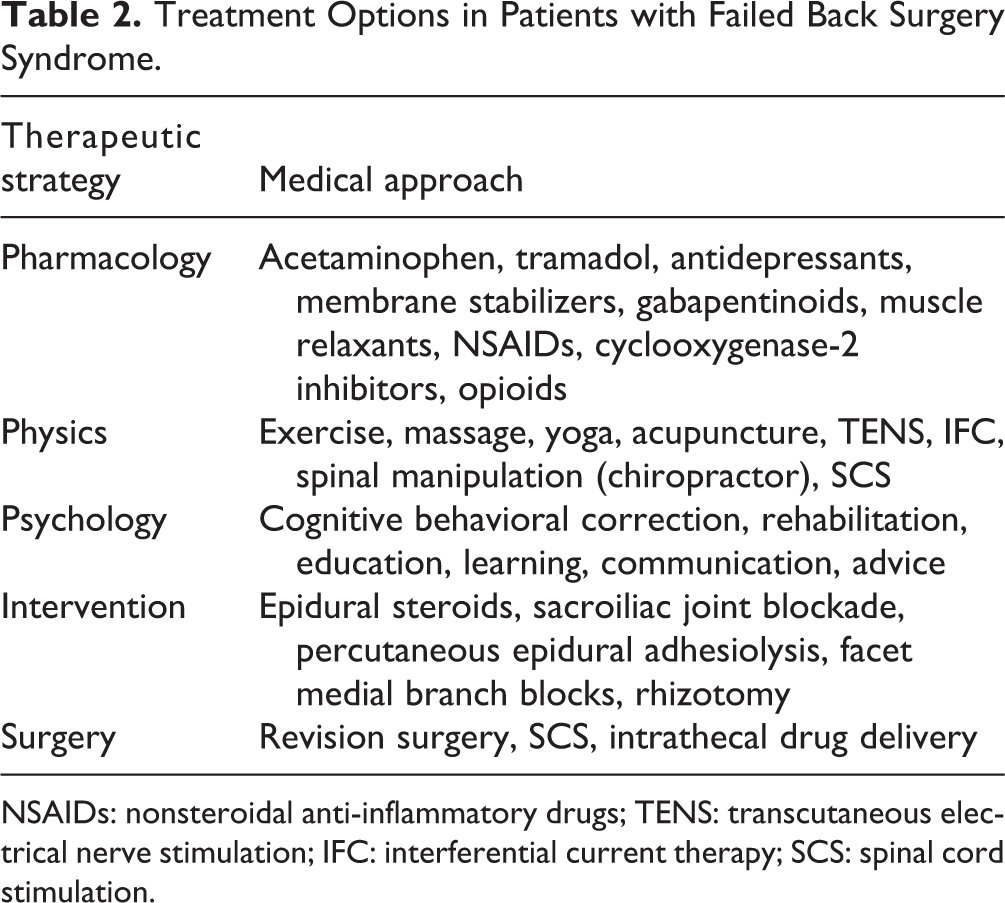
NSAIDs: nonsteroidal anti-inflammatory drugs; TENS: transcutaneous electrical nerve stimulation; IFC: interferential current therapy; SCS: spinal cord stimulation.
Narcotics and Addiction
Analgesic or Narcotics Are Used for Pain Relief
An analgesic is a drug used to achieve analgesia and relieve pain, which consists of two main types: non-narcotic analgesics for mild pain such as acetaminophens, NSAIDs, etc., and narcotic analgesics for severe pain, such as opioid drugs. Opioids or derivatives of opium belong to the narcotic family. With advances in modern science and biotechnology, the molecular basis of narcotics was discovered. The effects of narcotics, such as analgesia, sedation, euphoria, respiratory depression, vagal stimulation, obstipation, and dysphoria, are derived from the binding of receptors in the brain, spinal cord, and digestive tract 36 . In 2012, pharmacies in the United States dispensed 4.2 billion prescriptions for pain relievers, and 6.8% (289 million) were opioids 37 . The prescribed opioid drugs that can be dispensed at pharmacies include morphine, tramadol, oxycodone, hydrocodone, codeine, fentanyl, methadone, and buprenorphine 38 . Currently, increased amounts of narcotics are prescribed to stop either acute or chronic pain. In our bodies, strong stimuli on nociceptors induce pain signal transmission from peripheral nerves to the CNS. There are three types of nociceptors: Aδ fibers for fast pain, Aβ fibers for mechanical stimulation, and C fibers for slow pain. When these primary afferent nerve fibers transmit intense stimuli to the dorsal horn of the spinal cord, pain messages are sent to the brain and brain stem via multiple ascending pathways, resulting in both perception of and proper response to pain 39 . Once pain messages and reflexes persist, they may result in chronic pain 39 . Chimenti et al. 40 classified pain into five categories by mechanism: nociceptive, central, neuropathic, psychosocial, and movement system. Pain can be induced by different mechanisms. FBSS is a type of pain affecting the nervous system and is similar to neuropathic pain 13,16,41 . Neuropathic pain usually cannot be alleviated with tolerable doses of opioids, and long-term use often results in disability, psychological illness, and social problems 16 .
Narcotics Induce Addiction
Non-narcotic analgesics seldom induce addiction; however, narcotics frequently induce addiction because these chemicals result in euphoria and unwanted side effects, such as dependence and tolerance. The World Health Organization (WHO) defined drug addiction as a psychic (psychological) and sometimes physical status, due to the interaction between a living organism and a drug, that always includes a compulsion to seek the drug to experience its psychic (psychological) effects. Negative emotional states occur when the drug is not available 36 . Several studies explored the mechanisms of opioids (e.g., morphine) that mediate pain or induce euphoria 42,43 . Morphine is mainly metabolized in the liver and glucuronidated by uridine diphosphate (UDP)-glucuronosyltransferase enzymes 44 . It can be metabolized into morphine-6-glucuronide (M6G) which accounts for its analgesic effect, and morphine-3-glucuronide (M3G) which accounts for its neuroexcitatory effects 45,46 . There are three types of opioid receptors: mu, delta, kappa 38 . Opioid molecules bind mu opioid receptors (MOR) in the brain to produce both analgesia and euphoria 45,47 . For example, opioids bind the MOR in the periaqueductal gray, thalamus, cingulate cortex, and insula to regulate pain perception. Opioids that bind the MOR in the amygdala were reported to be associated with pain-induced emotional responses. Furthermore, opioids that bind the MOR in the ventral tegmental area, and the nucleus accumbens, would produce emotions of pleasure and reward, respectively 47,48 .
The blood–brain barrier (BBB) is a highly selective membrane barrier that separates the circulating blood from the brain and extracellular fluid. The BBB represents a significant challenge for narcotic delivery to the brain by virtue of its location, structure, and function. Schaefer et al. 45 claimed that the ability to cross the BBB is essential for the effects of opioids in both analgesia and euphoria. M6G could cross the BBB by direct penetration, binding the glucose transporter or a digoxin-sensitive transporter 44 . M3G may cross the BBB by the probenecid-sensitive transporter 44 . P-glycoprotein, also known as a multidrug-resistant protein, is an important cell membrane protein that pumps many foreign substances out of cells. It is an adenosine triphosphate (ATP)-dependent efflux pump with broad substrate specificity and probably exists in humans to serve as a defense mechanism against harmful substances. The previous study has shown that the p-glycoprotein transporter is a major determinant of the intracellular concentration of morphine and its two metabolites 44 . The p-glycoprotein transport system, an ATP-dependent efflux transporter at the BBB, exports opioids into the circulation 49 . Inhibition of p-glycoprotein activity increases the uptake of morphine 50 . Seleman et al. 50 found that inhibiting the p-glycoprotein transporter increases the reinforcing properties of the morphine and modulates morphine-induced transcriptional effect. The rewarding effects of opioids are the primary reasons for the development of opioid overdose and addiction. Potentially, the inhibition of the p-glycoprotein-transporter activity increases the antinociceptive effect of morphine, decreases its therapeutic dosage, and thereby decreases the possibility of drug addiction.
Many neurotransmitters are involved in drug addiction; one being glutamate. Glutamate is the major excitatory neurotransmitter in the brain that modulates the activity of the dopaminergic system 51 . There are two types of glutamate receptors: ionotropic receptors and metabotropic receptors. The N-methyl-D-aspartate (NMDA) receptor is an ionotropic receptor for glutamate and plays a key role in addiction 51 –53 . When NMDA receptors are activated, they exhibit long-lasting electrical currents that significantly increase calcium permeability 54 . This increase produces strong and/or synchronized inputs that result in long-term changes in memory. These memories enable drug-related stimuli to have powerful control over future behaviors and result in promoting addiction 54 . Daneshparvar et al. 55 found that NMDA receptor subunits (GluN1 and GluN2B) were significantly increased in the prefrontal cortex of drug abusers 51 . Mayer et al. discovered that long-term morphine use leads to excessive activation of NMDA receptors via the stimulation of MOR 56 . The activation of the functional NMDA receptors in the mesoaccumbal dopamine pathway is strongly associated with opioid-dependent behaviors. A number of studies have proved that long-term opioid use will lead to both tolerance and addiction 12,15,45,57 –59 .
Correlations Between Narcotic Addiction and Failed Back Surgery Syndrome
Using opioids does not necessarily lead to drug addiction, though narcotics are known to induce addiction. Volkow et al. 47 suggested risk factors for opioid addiction for some conditions. Medication-related factors include high daily dosage (morphine-equivalent dose > 120 mg/day) and long-term usage (>3 months) whereas patient-related factors include depression, substance-use disorder (including alcoholism), and adolescence 12 . Some conditions frequently resulted in opioid overdoses, such as long-acting or extended-release formulations, combinations of opioids with benzodiazepines, age > 65 years, sleep disorders, renal or hepatic impairment, and a history of overdose. Additionally, patients that have had an opioid overdose are more prone to opioid addiction. Hojsted et al. 60 assessed chronic pain patients with opioid addiction using both The International Statistical Classification of Diseases and Related Health Problems, 10th revision and Portenoy’s criteria. They found that 33% of patients were classified as having neuropathic pain and 21% had low back pain. More than one fifth of patients with opioid addiction were associated with FBSS. In addition to chronic pain, Thomson et al. 16 found that 78% of patients with FBSS were unable to work normally and had poor quality of life. The patients sought various therapies, hoping to recover from the pain from which they have been suffering.
There are several strategies for preventing patients with FBSS from falling into narcotic addiction. First, patients with FBSS should try a multidisciplinary approach to achieve pain relief instead of a long-term, high-dose narcotics regimen, which can easily lead to addiction 12,47 . P-glycoprotein induction enhances morphine efflux from the brain and decreases morphine’s pharmacologic activity but may result in morphine tolerance in rats 61 . Furthermore, naltrexone is an opioid antagonist acting on the MOR for treating addiction and acute opioid toxicity 38 . MOR agonist use, also for treating opioid addiction such as methadone 56 , often leads to frequent relapse. Buprenorphine, a kappa antagonist and partial MOR agonist, has also been used for addiction treatment 38,56 . Several studies were devoted to finding elective kappa opioid antagonists as effective drugs for treatment of addiction 38 . The pros and cons of these applications are still being debated in current studies. Because the NMDA receptor has important effects on drug-seeking behaviors, alteration of the NMDA receptor function may be beneficial in the management of opioid addiction 56 . Belozertseva et al. 62 found that the NMDA receptor antagonist (e.g., MRZ 2/576) could inhibit morphine withdrawal in mice. Bisaga et al. 63 found the drug (e.g., memantine) that blocks the NMDA receptor can attenuate opioid physical dependence in humans. The main causes of narcotic addiction are shown in Fig. 1 with the strategies proposed to prevent and treat narcotic (e.g., morphine) addiction in FBSS patients.
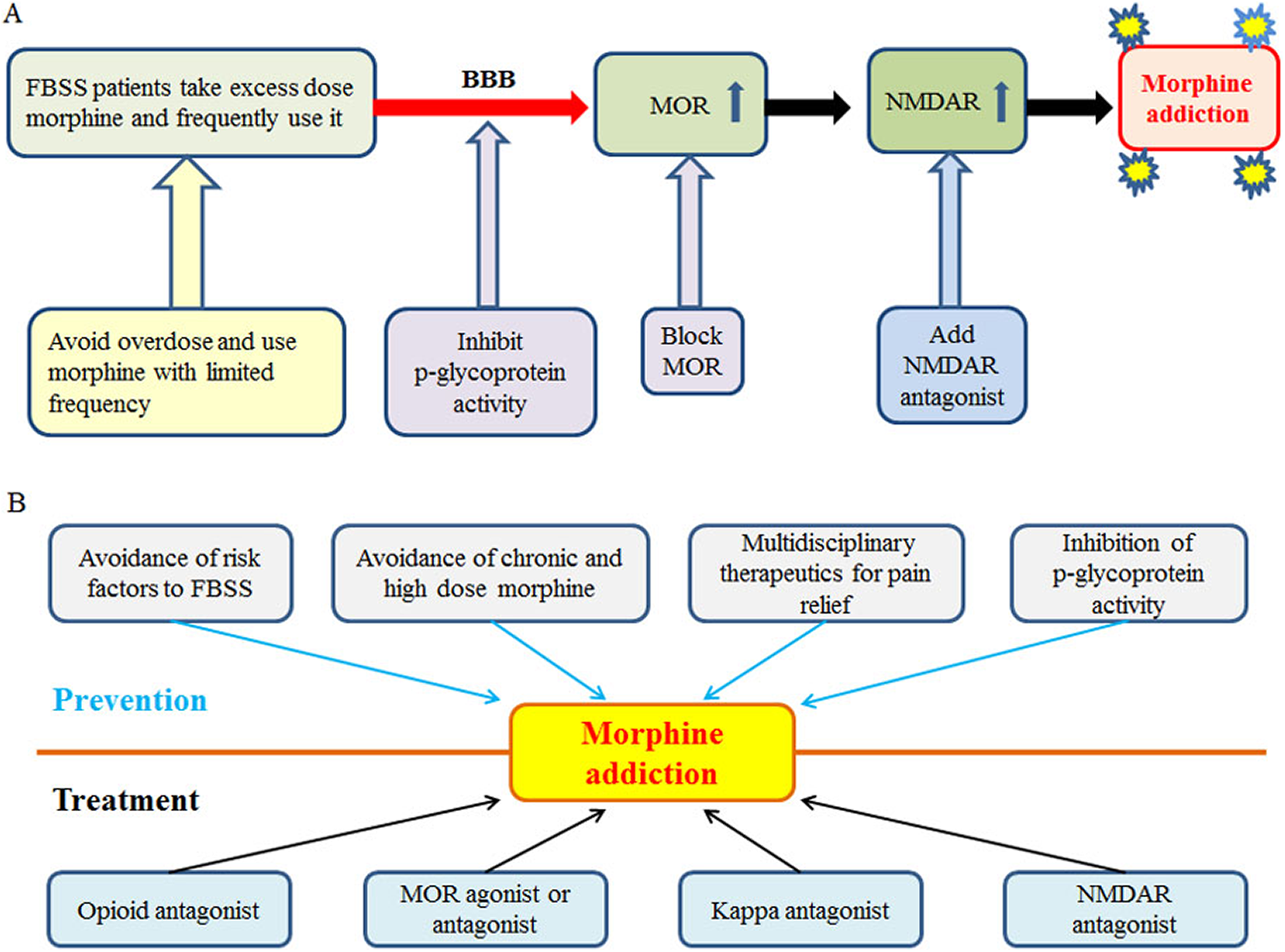
The main causes of narcotic addiction (e.g., morphine) and strategies for the prevention and treatment of narcotic addiction in FBSS patients. (A) The possible mechanism for inducing narcotic addiction and preventive strategies during the induction process; (B) strategies for the prevention and treatment of narcotic addiction (e.g., MOR agonist: methadone; MOR antagonist: naltrexone). BBB: blood–brain barrier; FBSS: failed back surgery syndrome; MOR: mu opioid receptors; NMDAR: N-methyl-D-aspartate receptor.
Pharmacological Guidelines for Avoiding Narcotic Addiction
According to the WHO analgesic ladder, medicines for mild pain should start from nonopioids with or without adjuvants, opioids for mild to moderate pain, and finally to opioids for moderate to severe pain. For severe and acute pain caused by surgery, opioids are the first-line analgesia for major spinal surgery 64 . However, the guideline of the Enhanced Recovery After Surgery (ERAS) Society suggests that multimodal analgesia can decrease the doses and side effects of opioids after surgery 64 –67 . The guideline of the North American Spine Society (NASS) also recommends multidisciplinary spinal care 65 . The multimodal analgesia uses combinations of NSAIDs, paracetamol, anticonvulsant agents, calcium channel blockers, NMDA receptor antagonists, and regional analgesia, which target different pain receptors and block pain transmission pathways peripherally and centrally 66 .
To avoid the side effects of long-term opioid therapy for chronic pain, the USA Centers for Disease Control and Prevention (CDC) have 12 recommendations for opioid usage 68 . The primary issues are summarized as follows: first, they recommend nonpharmacological therapy and nonopioid pharmacologic therapy to be ahead of opioid usage. This is consistent with our review finding that multidisciplinary approaches and multimodal analgesia could reduce overdose of opioids and should be to be a priority in relieving pain. Second, they suggest clinicians prescribe the lowest effective dose of immediate-release opioids instead of extended-release/long-acting opioids to reduce the risks for opioid misuse or addiction. Third, they suggest clinicians avoid using opioids to relieve acute pain for the long term. The appropriate duration should be less than 7 days then patient risk–benefit should be evaluated within 1–4 weeks. Fourth, they suggest the patients use nonconcurrent opioids and benzodiazepines to avoid overdose. They also emphasize the importance of a patient’s illness history and the re-evaluation of narcotic effects at predefined intervals.
Conclusion
FBSS is a disease that usually follows spinal surgery. Its exact pathophysiology is still poorly understood, though many plausible causes have been investigated. Various interventions, including SCS, epidural adhesiolysis or injection, exercise therapy, and psychotherapy have been suggested as therapeutic strategies 56 . Pain treatments, including pharmacological and nonpharmacological methods, may be very effective for alleviation, but their adverse effects are inevitable. It is recommended that patients be evaluated for the risk of narcotic addiction for commonly prescribed opioids such as morphine, heroin and oxycodone 57,69 . An exploration of medication efficacy and risk assessment for narcotics should be required to make sure that benefits outweigh risks.
Drug addiction involves a complex set of behaviors typically related to the abuse of certain drugs, developing over time with high drug dosages. Addiction demonstrates psychological compulsion to the extent that the patients insist on activities resulting in sick or dangerous outcomes. Problems with narcotics for patients usually include the following issues: not all pain is relieved, side effects outweigh the therapeutic benefits, tolerance is built over time, and an increased sensitivity to pain (hyperalgesia) occurs. Anticonvulsant medications (e.g., SCS) are effective in managing neuropathic pain for FBSS, whereas opioids are rarely beneficial 15,58 ; therefore, we regard narcotic addiction as a crucial problem. Various narcotics (e.g., morphine, codeine, fentanyl, tramadol, meperidine, etc.) have different addictive properties, and their addictive mechanisms are complex and still unclear. The narcotic clinical trend and its frequency in causing addiction can be evaluated by such patient outcome measures as improvement of functional status, health-related quality of life, return to work, and reduction in opioid use 56,70 . Based on the aforementioned scientific data and statistical analysis, healthcare professionals may choose the best narcotic for patient pain relief of FBSS.
The treatment of FBSS is a challenge for surgical doctors, pain specialists, and primary care providers. Minimizing the possibility of FBSS mainly relies on the determination of a clear etiology of the patient’s pain, recognizing those who are at high risk, and exhausting conservative treatment before going into revision surgery 17,59 . Despite this, narcotic drugs are effective for pain relief in FBSS, but their dependence and tolerance should not be ignored. Though the correlation between narcotic addiction and FBSS is complex and difficult to evaluate, narcotic dose and frequency are considered to be critical parameters in understanding addiction. For pain relief in FBSS patients, studies on regulating the administration dose and frequency, and development of personalized treatment may be needed.
Because of the increasing cases of spinal surgery, medical doctors are expecting to oversee the care of patients with FBSS more frequently than before. It is challenging enough to manage back pain without falling into the grave of narcotic addiction. To be free from pain is a human right, but it is more important to avoid narcotic addiction. Several guidelines are proposed by WHO, ERAS Society and NASS, and medical practitioners must follow these instructions and regulations. According to our clinical studies, the abuse and overdose of narcotics are closely related to the psychological mode and/or state of patients. Consequently, patients who receive narcotics for more than 14 days are recommended for psychological evaluation and treatment, particularly for patients with chronic back pain. Narcotic usage should be strictly controlled by the official drug administration. There should also be a specific committee in hospitals to monitor narcotic usage for nonmalignant diseases.
In summary, the frequency of spinal surgery is on the rise, and the number of patients with FBSS is also increasing each year, with almost 40% diagnosed after spinal surgery. These patients are likely to suffer from chronic pain despite multiple types of therapy. Narcotics are among the various medications these patients take for alleviation of pain, and theyoften become addicted after long-term use. Although pain is the fifth vital sign, FBSS is a major healthcare problem and should be seriously considered as a public health issue. Multidisciplinary treatments involve therapeutic strategies to prevent narcotic addiction. Doctors, nurses, pharmacists, physical therapists, and social workers should all be involved in the medical team for FBSS, as each can make substantive contributions in attaining the intended goals and the optimization of a patient’s quality of life.
Footnotes
Acknowledgments
We are grateful for the grant support from Mackay Memorial Hospital in publishing this article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.