
Abstract
Copeptin is a hypothalamic stress hormone that is synthesized in the hypothalamus together with Arginine-vasopressin and circulated from the neurohypophysis in equimolar amounts and can indicate the individual stress level. The aim of this study was to investigate the plasma copeptin level for childhood migraine headache. In this study, total oxidant status (TOS); total antioxidant status (TAS); oxidative stress index (OSI); and copeptin were measured in the plasma samples of 61 migraine patients and 60 matched healthy participants. The median plasma copeptin levels in the patients group and control group were 298.25 and 194.35 pg/mL, respectively. Copeptin levels were significantly higher in migraine patients than in the healthy control group. The specificity and sensitivity of copeptin for 249.5 pg/dL cut off value predicting diagnosis of migraine were 67% and 64%, respectively. In addition, TOS and OSI levels were found to be higher and TAS levels were significantly lower in patients with migraine than healthy controls. Plasma copeptin levels are thought to increase in cases of childhood migraine secondary to increased oxidative stress. In the diagnosis of childhood migraine cases, it can be used together with oxidative stress biomarkers such as TAS, TOS and OSI as a complementary parameter.
Introduction
Headache is a common neurological problem, which negatively affects the quality of life in childhood and adolescence. Migraine is one of the most common causes of primary headache in childhood. 1 –3 Migraine is a chronic neurological disorder that starts early in childhood and adolescence and has a genetic basis which is multifactorial. 4,5 Even though the pathophysiology of migraine cannot be understood completely, central sensitization, neurogenic inflammation, atypical pain processes, and cortical hyperexcitability are among the widely reported hypotheses. 6,7
Oxidant-antioxidant balance is a significant mechanism for homeostasis in an organism, and it is thought that impairment of this balance plays a role in some acute and chronic diseases of the central nervous system. 8 –13 Previously, it has been suggested in various studies that the increased level of oxidative stress arising from the imbalance between the production of reactive oxygen species, such as superoxide radical anions, hydroxyl radicals and hydrogen peroxide, and their elimination by antioxidant defense mechanisms plays a role in the etiopathogenesis of various headache disorders including migraine. 8 –12 For this reason, evaluation of the total antioxidant status (TAS) and the total oxidant status (TOS) provides critical information about the in vivo dynamic balance between pro-oxidative and antioxidative molecules. 14
Copeptin, also known as Arginine-Vasopressin (AVP) related glycopeptide, was first described by Holwerda 15 in 1972 as a 39-aminoacid glycopeptide rich in leucine. Copeptin is synthesized together with AVP in the hypothalamus and released into circulation in equimolar amounts from the neurohypophysis with AVP. 16 Copeptin is also a hypothalamic stress hormone that can indicate individual stress level. 17 Contrary to AVP, it has been suggested recently that copeptin can be used as a new diagnostic biomarker for different diseases such as myocardial infarction and pneumonia sepsis, since copeptin remains stable at room temperature and can be measured relatively easily. 18– 20 On the other hand, the diagnostic value of copeptin has also been shown in various diseases in the adults, such as non-traumatic headaches, migraine, strokes, subarachnoid hemorrhages, and traumatic brain injuries, which may be correlated with headache. 21– 23
The aim of this research was to determine the copeptin level in migraine patients in childhood and to investigate its relationship with oxidative stress level.
Materials and methods
This prospective study was conducted in a pediatric neurology outpatient clinic at Turkey in Sanliurfa with of 61 migraine patients and 60 matched healthy participants. Before the study, written informed consent was obtained from the parents of the patients who participated in this study. This study conformed to the principles of the 2008 Declaration of Helsinki and was approved by the local ethics committee in Turkey (Approval date and number: June 15, 2020, Session 11, 24468).
The controls were selected from healthy age, sex, and body mass index (BMI) matched headache-free volunteers from the general population. The diagnosis of migraine was made following an examination by an expert specialist-pediatric neurology according to the International Headache Society Criteria (ICHD-III). 1 The inclusion criteria were a diagnosis of migraine without aura (MWA), migraine with aura (MA) and chronic migraine (CM), according to the ICHD-III. A childhood version of the Migraine Disability Assessment (PedMIDAS) was used for school-aged participants who could express themselves. 24 The frequency of the headache was evaluated through the diaries where patients and their parents had reported the days with headache in the last 3 months.
The patients who were diagnosed with migraine were not experiencing a migraine headache at the time of obtaining blood samples. A pilot study was conducted as there were not enough clinical studies for reference values of copeptin in pediatric migraine cases. Therefore, preliminary data from 15 patients who were not included in the data analysis were used to calculate the sample size of the study. It was selected for α-level 0.05 and for β-level 0.20 (power is 80%). We calculated the final sample size to be 121 subjects. Healthy participants were defined as the control group (n = 60) and the migraine patients as the patient group (n = 61). All blood samples taken from peripheral venous for oxidants and copeptin levels were centrifuged at 3000 × g for 10 minutes for plasma separation. The samples taken were preserved at –80°C until the day of study.
Exclusion criteria
Those who had the following health problems were not included in this study: those with obesity and protein energy malnutrition (abnormal body mass index), smoking (including passive smoking), chronic kidney or liver disease, pulmonary disease, hypertension, a history of cardiovascular or endocrinological diseases, malignancy, rheumatic diseases, chronic inflammatory diseases, infection, and degenerative diseases. In the patient group, those with any pathological findings other than migraine were excluded from the study.
Measurement of the copeptin
The concentration of copeptin in plasma was analyzed by enzyme-linked immunosorbent assay (ELISA) using commercial kits (Cusabio Biotech Co. Ltd, Wuhan, Hubei Province, China) in accordance with the manufactures’ instructions. The results are expressed in picograms per milliliter. The detection range was 78 pg/mL to 5000 pg/mL, with a detection limit of 19.5 pg/mL. The detection wavelength was 450 nm. Intra-assay and inter-assay variance was <8% and 10%, respectively.
Measurement of the TAS
The total antioxidant status measurements were made using brand commercial kits (Rel Assay Diagnostic Gaziantep, Turkey) on a microplate reader system (Varioskan Lux, Thermo Scientific, USA). Briefly, free radical reactions were initiated by Fenton reaction and monitored by absorbance of the dianisidyl radicals. This reaction was measured spectrophotometrically at 660 nm. Using this method, the antioxidative effect was measured by relative amount of free dianisidyl radicals. The precision of this test has high accuracy (less than 3% error rate). The data were expressed in mmol Trolox equivalent/L.
Measurement of the TOS
The total oxidant status measurements were made using brand commercial kits (Rel Assay Diagnostic Gaziantep, Turkey) on a microplate reader system (Varioskan Lux, Thermo Scientific, USA) according to the method of Erel. 25 Briefly, oxidants present in the sample oxidize the ferrous ion-o-dianisidine complex to ferric ion. The oxidation reaction is enhanced by glycerol molecules, which are abundantly present in the reaction medium. The ferric ion makes a colored complex with xylenol orange in an acidic medium. The color intensity, which can be measured spectrophotometrically (at 530 nm), is related to the total amount of oxidant molecules present in the sample. The assay is calibrated with hydrogen peroxide, and the results are expressed as μmol H2O2 equivalent/L.
Calculation of the OSI
To calculate the OSI, the resulting TAS units were converted to mmol/L, and the OSI value was calculated according to the following formula: OSI (arbitrary unit) = TOS (mmol H2O2 equivalent/L)/TAS (mmol Trolox equivalent/L).
Statistical analysis
Statistical analysis was performed using SPSS version 24.0 (SPSS Inc., Chicago, IL). Power analysis was performed by using G*Power v3.1.9.4 to detect the sample size. Descriptive statistics were summarized as number, percentage, median (minimum–maximum), mean and standard deviation. The suitability of variables to normal distribution was investigated using visual (histogram and probability graphs) and the Kolmogorov–Smirnov test. Continuous variables were analyzed with either Student t-test or Mann–Whitney U-test depending on distribution and homogeneity of the data. Pearson correlation testing was used to investigate the relationship between parameters. Correlation coefficient (r) was found as a result of Pearson correlation analysis. Specificity and sensitivity analysis were performed by using receiver operating characteristic (ROC) curve analysis technique. In the ROC analysis, the area under the curve (AUC) values were studied. Comparisons were considered statistically significant when the probability (p) value was less than 0.05 (p < 0.05).
Results
The study group consisted of 61 patients, (23 male (37.7%), 38 female (62.3%), between the ages of 11 and 17 years (mean age, 14.22 ± 1.61years). The control group had 60 healthy participants (27 male (45%), 33 female (55%) between the ages of 10 and 17 (mean age, 14.01 ± 1.86).The demographic characteristics of the study population are shown in Table 1. In addition, the demographic and clinical characteristics, TAS, TOS, OSI and copeptin levels of migraine patients are shown in Table 2. The patient and control groups did not significantly differ in sex, mean age and mean BMI (p > 0.05).
Demographic characteristics of the study population.

SD: Standard deviation; a: Independent sample t-test; b: Pearson chi-square test; BMI: Body mass index.
Demographic and clinical features and TAS, TOS, OSI and copeptin levels of migraine patients.

All parameters except gender are given in median (minimum–maximum) values.a: Kruskal Wallis test; b: Fisher’s Exact test; c: Mann–Whitney u test; BMI: Body mass index; PedMIDAS: Pediatric Migraine Disability Scale; TAS: Total antioxidant status; TOS: Total oxidant status; OSI: Oxidative stress index.
A significant difference was observed between the groups in the mean TOS, TAS-OSI and copeptin levels (Table 3) (Figure 1). The mean TOS value in the patient group was 15.9 ± 4.81 H2O2 equivalent/L, while it was 11.43 ± 3.03 H2O2 equivalent/L in the control group. Plasma TOS was significantly higher in patients with migraine than in healthy controls (p < 0.001). The mean TAS value in the patient group was 1 ± 0.13 mmol Trolox equivalent/L, while it was 1.52 ± 0.16 mmol Trolox equivalent/L in the control group. Plasma TAS was significantly higher in healthy controls than in patients with migraine (p < 0.001). The median OSI value in the patient group was 1.51 (0.32–3.59), while it was 0.73 (0.26–1.45) in the control group. OSI was significantly higher in patients with migraine than in healthy controls (p < 0.001). The median copeptin value in the patient group was 298.25 (125.75–4943.25) pg/mL, while it was 194.35 (87–615.75) pg/mL in the control group. Plasma copeptin was significantly higher in patients with migraine than in healthy controls (p < 0.001).
Analysis of oxidative stress parameters and copeptin level in the study population.

SD: Standard deviation; a: Independent sample t-test; b: Mann–Whitney U-test; TAS: total antioxidant status; TOS: total oxidant status; OSI: oxidative stress index.
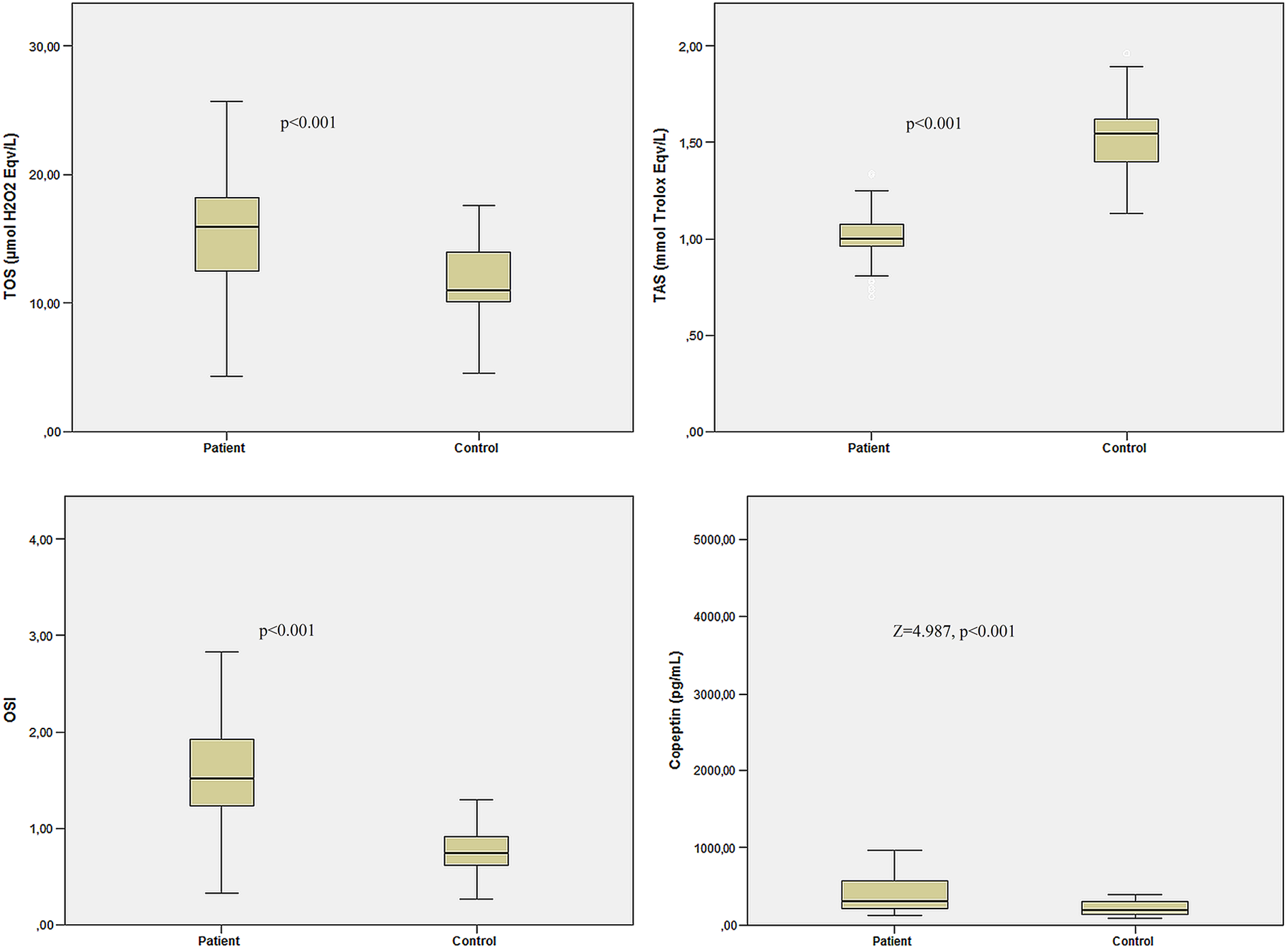
Comparison of mean TAS, TOS, OSI and median copeptin levels between migraine patients and healthy controls. Sublegend: TAS: total antioxidant status; TOS: total oxidant status; OSI: oxidative stress index.
A significant correlation was observed between TOS, TAS-OSI and copeptin levels (Table 4). The Pearson correlation analysis revealed a positive correlation between the copeptin and OSI (r: 0.802, p < 0.001) and TOS (r: 0.675, p < 0.001) levels. Moreover, a negative correlation was found between the copeptin and TAS (r: –0.511, p < 0.001) levels. Pearson correlation analysis was also performed to determine the relationship between oxidative stress parameters. There was a negative relationship between TAS-OSI (r: −0.831, p < 0.001) and TAS-TOS (r: −0.719, p < 0.001), and a positive relationship between TOS-OSI (r: 0.944, p < 0.001).
Correlation between copeptin and oxidative stress parameters.
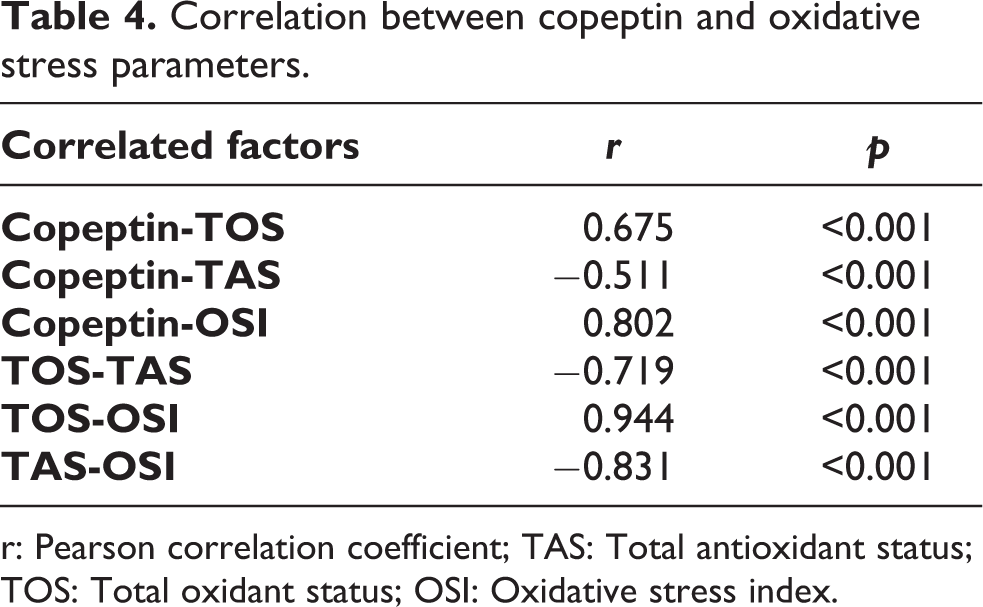
r: Pearson correlation coefficient; TAS: Total antioxidant status; TOS: Total oxidant status; OSI: Oxidative stress index.
ROC curves were plotted to compare predictive values of TOS, TAS, OSI and copeptin in the diagnosis of migraine for 121 participants (Figure 2). As a result of the analysis, AUC:0.777, p < 0.001 was found and 77% sensitivity and 77% specificity were determined for the TOS value of ≥12.44 μmol H2O2 equivalent/L; AUC:0.993, p < 0.001 was found and 96% sensitivity and 96% specificity were determined for the TAS value of ≥1.267 mmol Trolox equivalent/L, AUC:0.919, p < 0.001 was found and 82% sensitivity and 82% specificity were determined for the OSI value of ≥1.064, and AUC:0.763, p < 0.001 was found and 64% sensitivity and 67% specificity were determined for the copeptin value of ≥ 249.5 pg/mL (Table 5).
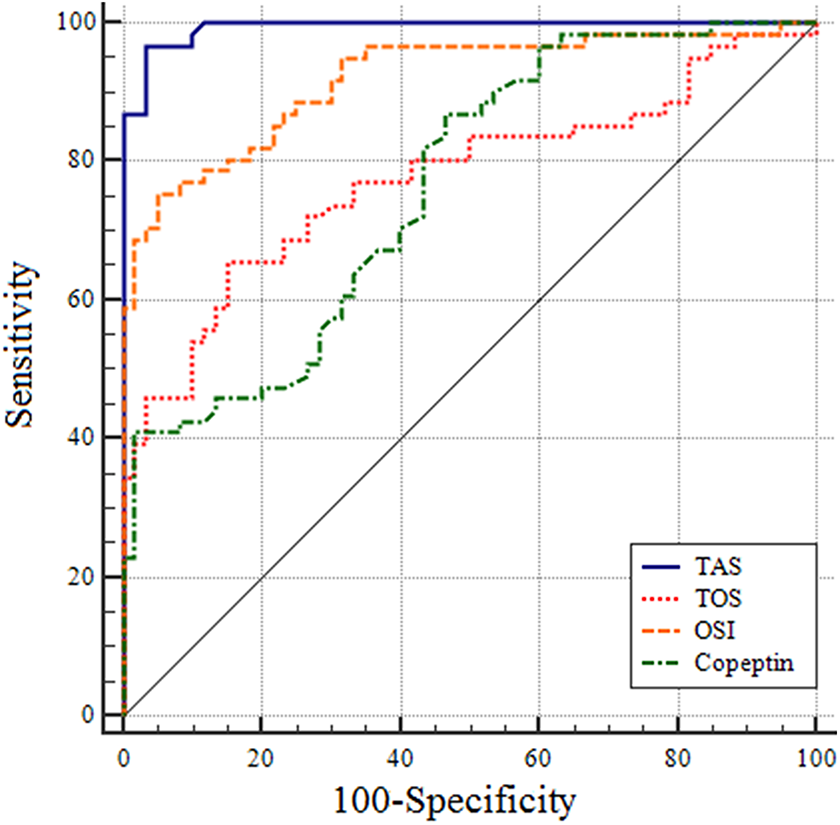
ROC analysis for TAS, TOS, OSI and copeptin values in diagnosis of migraine. Sublegend: TAS: total antioxidant status; TOS: total oxidant status; OSI: oxidative stress index.
Evaluation of copeptin and oxidative stress parameters in the diagnosis of migraine.

CI: Confidence interval; TAS: Total antioxidant status; TOS: Total oxidant status; OSI: Oxidative stress index.
Discussion
Migraine is a neurovascular disease known for a long time. There are many factors playing a role in the etiopathogenesis of migraine: Genes, food, oxidants, environmental factors, macro and micro elements, metabolic disorders or hormonal changes are the leading ones. 26 These factors negatively affect brain homeostasis and lead to the activation of hypothalamus. Ultimately, all these neurobiological processes lead to deterioration and alteration of cortical and brainstem excitability, causing migraine headaches. 26
Today, few biomarkers that may be associated with migraine have been investigated, and information about the usability of previously studied biomarkers in diagnosis and treatment is limited. 27 New biomarkers to be discovered in this context will help in early diagnosis, differential diagnosis or follow-up of treatment of migraine. In our opinion, copeptin may be a new biomarker that can be used for diagnosis and follow-up of migraines. The diagnostic value of copeptin and its relationship with headache have been the subject of research, especially in the recent past in pathological cases that may have been associated with headache. 21– 23 Zuo and Ji 21 expressed that copeptin levels can reliably predict short-term prognosis at the onset of aneurysmal subarachnoid hemorrhage in patients. Another study by Blum et al. 22 reported that copeptin level was higher in patients with severe secondary headache compared to benign forms of headache, and there was a positive correlation between them. In a study conducted by Yılmaz et al. 23 on adults recently, a significant difference was found in the mean copeptin level in migraine patients in the periods with and without migraine attacks; however, but its strength in clinical diagnosis was not satisfactory. In our current study, the median plasma copeptin level was 298.25 pg/mL in the patient group, while it was 194.35 pg/mL in the control group (p < 0.001). Our main finding in this study is that copeptin level was higher in migraine patients compared to healthy controls. In the ROC analysis carried out in our study, it was discovered that copeptin was effective at a cutoff value of 249.5 pg/dL (AUC: 0.763) in the diagnosis of migraine, whereas it did not have adequate sensitivity (67%) and specificity (64%).
In humans, if oxidant levels increase or antioxidant mechanisms are insufficient, the oxidative-antioxidant balance is impaired and oxidative stress occurs. As a result, increased levels of oxidative stress can affect many organs in the human body, including the brain, causing various diseases. The relationship between migraines and oxidative stress continues to be debated today and some studies have put forward the oxidative stress hypothesis for migraines. 8 –13 The results of the studies on the relationship between oxidative stress and migraine vary. In a study conducted by Eren et al. 8 on adult migraine patients, TAS, TOS and OSI were similar in patients with migraine and healthy control group; however, the serum thiol level, a significant indicator of antioxidant capacity, was significantly lower in migraine patients compared to the control group. Togha et al., 28 on the other hand, demonstrated that CM group patients had lower total non-enzymatic antioxidant capacity and higher oxidative stress than the healthy control group. Boćkowski et al. 29 reported that the disorders in lipid peroxidation processes and the increased antioxidant glutathione peroxidase level might be effective in the pathophysiology of migraine in pediatric age group patients. Similarly, Erol et al. 30 emphasized the increased sensitivity to oxidative stress in pediatric migraine cases. In our study, we also found that migraine patients had higher oxidative stress (TOS and OSI) and lower antioxidant capacity (TAS) compared to the control group. In the correlation analysis, a strong negative correlation was found between TOS and TAS, while a strong positive correlation was found between TOS and OSI.
Moreover, when the relationship between oxidative stress parameters and copeptin was examined in our current study, there was a positive correlation between TOS and OSI and a negative correlation between TOS and TAS. To the best of our knowledge, there are no studies investigating the relationship between copeptin levels and oxidative stress parameters in the literature. Our study, as far as we know, is the first study in the literature to examine the level of copeptin in migraine patients in the pediatric population.
Limitation of study: In our study, a more reliable result could have been obtained by comparing migraine patients, tension headaches and other primary headaches. However, this could not be achieved in the current study.
Conclusion
In our study, plasma copeptin levels were higher in pediatric patients with migraine compared to the healthy control group. In addition, it is noteworthy that there was a positive correlation between plasma copeptin level and oxidative stress level. The results of our current study indicate that the measurement of plasma copeptin level can be a marker that can be used in the diagnosis and follow-up of migraine patients. However, there is a need for comprehensive studies on this subject.
Footnotes
Acknowledgment
We would like to thank all the doctors working at the Department of Biochemistry, Harran University Medical School, and all the staff of the biochemistry laboratory.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.