
Abstract
The aim of this study was to evaluate the concordance between clinical diagnosis and the International Classification of Headache Disorders, 2nd edn (ICHD-II) in children and adolescents with primary headaches. This 6-month prospective multicentre study of 486 patients (mean 9.8 ± 3.1 years; 52.6± girls) assessed the headache features through a structured questionnaire. In 398 patients with a single type of headache, headaches were bilateral (78.1±), frontal (62.4±), pulsatile (56.1±), with associated symptoms in 84.4±. The most frequently assigned diagnoses were migraine without aura (50.8±), probable migraine (14.1±), migraine with aura (11.1±) and frequent episodic tension-type headache (7.5±). For most of the diagnostic categories, the consistency of the investigator's diagnosis with the ICHD-II criteria was good (K > 0.6 and ≤ 0.8) or excellent (K > 0.8). We conclude that migraine was predominant with regard to headache diagnoses repartition and that the ICHD-II seems usable in practice for evaluation of primary headache in French children and adolescents.
Introduction
Headache is a common symptom and also poses a significant public health problem for the healthcare systems of many countries, both in adults and children. Many individuals fail to consult a physician despite debilitating headaches (1). Previous research has documented suboptimal identification and misclassification of those with headache when seeking advice from medical providers (1, 2). Furthermore, headache disorders lack a true diagnostic gold standard, which contributes to these difficulties.
When parents take their children with headache to consult the doctor they are worried that the symptom has a serious cause, especially brain tumour. Fortunately, such causes in these patients are rare, most cases being primary headaches. Primary recurrent headache disorders represent a pathology with high and increasing prevalence during developmental age. Recurrent headaches are becoming a focus in paediatrics, but complete understanding of them has yet to be achieved. The criteria for diagnosis of primary headache in children was established by the International Headache Society (IHS) in 1988 (3) and was revised in 2004 (4). The primary headache disorders include migraine, tension-type headache (TTH), cluster headache and other trigeminal autonomic cephalalgias, and other primary headaches. These were defined on the basis of symptom profiles of the characteristics of attacks and the general and neurological examinations being normal. The basis of diagnosis is a systematic headache history, careful physical and neurological examination, and follow-up using a headache diary.
The objectives of the present study were to study clinical features and the agreement between clinical headache diagnoses by members from the French Society for Paediatric Neurology, who are child neurologists, and the second edition of the International Classification of Headache Disorders (ICHD-II) criteria (4) in primary headaches in 25 hospital departments in France during 6 months.
Methods
This was a cross-sectional epidemiological survey of primary headache in children conducted in 22 hospital neuropaediatric departments in France between November 2005 and May 2006.
Participating physicians
Investigators were recruited from the French Society for Paediatric Neurology. Physicians were selected at random in each region of France from the membership list of this society and invited to participate until the required number of centres was reached (25).
Patients
The study included children aged 2–16 years consulting a neuropaediatric centre for primary headache for the first time. Children already participating in a clinical trial or other study were excluded. Each investigator was expected to include serially the first 25 patients fulfilling the entry criteria consulting at the centre during a 6-month inclusion period.
Data collection
At consultation, a detailed clinical examination was performed. The investigators completed a questionnaire for each patient providing information on the demographic profile of the child, clinical features of the headache, triggering factors, personal and family medical history, and treatment. Each investigator made a clinical diagnosis and identified the headache type using ICHD-II.
Statistical analysis
The size of the target study sample was determined by a priori power calculations in order to determine the frequency of key variables with a precision of 5% when observed in 50% of the sample. These calculations yielded a target sample size of 384 subjects. In order to take into account potentially non-assessable subjects, it was decided to include 500 children. To include this number of patients over a 6-month period, it was estimated that 20 physicians would need to include 25 children each. In order to take into account physicians who would agree to participate but then not recruit patients, 25 investigators were considered necessary to achieve the target sample size.
The presentation of the clinical features of the headaches was purely descriptive. Intergroup comparisons between headache types were performed with the χ2 test or Fisher's exact test, as appropriate. Consistency between the investigator's diagnosis and the ICHD-II classification was assessed by estimation of κ coefficients. All tests were two-sided and a probability level of P < 0.05 was considered significant. All data were controlled, validated and analysed centrally using SAS software, version 8.2 (SAS Institute, Cary, NC, USA).
Ethics
The study was performed according to international and French regulatory guidelines and current codes of Good Epidemiological Practice. Since patient care was not altered by inclusion in the study, ethics committee approval was not necessary. With respect to confidentiality of patient records, data handling for the study was authorized by the Commission Nationale d'Informatique et de Libertés.
Results
Study population
Overall, 486 children were included in the study. Their demographic characteristics are presented in Table 1. The mean age of the study population was 9.8 ± 3.1 years and girls were slightly over-represented (52.6%). Ten children were obese and 39 overweight. Neurological examination was normal in 456 children (97.4%). Hemiparesia or hemiplegia was observed in four children, anisocoria in two and ptosis and diplopia in one child each. Unspecified neurological abnormality was reported in four other children. Nineteen children (4.2%) presented pericranial tenderness. Mean arterial blood pressure was 106 ± 13 mmHg (systolic) and 64 ± 9 mmHg (diastolic). According to their parents, 254 children (52.3%) presented symptoms of anxiety, six (1.2%) presented symptoms of depression and 22 (4.5%) symptoms of both.
Demographic characteristics of the study population

Data were missing for most variables, and the number of subjects for whom data were available is thus indicated for each variable.
Headache features
Out of the entire study population, 88 children presented with multiple headache types. These individuals are excluded from the description of headache features, which are thus restricted to the 398 children with a single headache type.
The mean time that participating children had experienced headaches was 2.3 ± 2.3 years (median 1; range 0–13) and the mean age at which headaches started was 7.6 ± 3.1 years (median 7; range 1–16). For 394 children (83.0%), the clinical presentation of the headaches had not changed between their first appearance and the time of consultation.
Headache characteristics are presented in Table 2. Headaches were most frequently bilateral (78.1% of children) and localized to the frontal region (62.4%). Pulsatile headaches were more common (56.1%) than pressure or stabbing headaches. Aura was associated with headaches in 19.9% of children, around one-third of which were atypical. Most frequently, auras were visual. Headaches were accompanied by associated symptoms of nausea, vomiting or photo/phonophobia in 84.4% of children, and by autonomic signs, typically pallor, in 79.6% of children. Headaches were preceded by a prodromal state in 47 children (11.8%), most frequently a feeling of great tiredness. The duration of headaches was < 4 h in most children (58.0%), and these most frequently occurred upon returning from school. Most children (74.3%) experienced < 10 headaches per month, and only 13 (3.4%) reported more than one headache per day. Headaches were aggravated by effort in around half of children and relieved by sleep in around two-thirds. In most children (86.3%), their headaches interfered with their daily activities to some degree, and in 42.6% led to the cessation of all activity.
Headache features in 398 children with primary headaches

Data were missing for most variables, and the number of subjects for whom data were available is thus indicated for each variable.
Precipitating factors for headache were present in 213 children (62.3%). These were identified from a predefined checklist and are listed in order of decreasing frequency in Table 3, for both systematic precipitating factors (their occurrence always or nearly always triggers a headache) and occasional precipitating factors (their presence sometimes triggers a headache). The most frequently cited precipitating factors were tantrums, school pressure, intense physical activity, heat and lack of sleep. In three children, headaches were triggered exclusively by anxiety, stress or fatigue, and in three others exclusively by physical effort.
Precipitating factors for headache in 213 children with primary headaches in whom such factors were identified, listed in order of decreasing frequency for the ‘occasional’ column

Medical history
Two hundred and five children (43.2%) had a previous medical history, principally allergy and asthma (Table 4). In addition, 156 children (34.1%) had experienced periodic symptoms that are commonly precursors of migraine. These included motion sickness (n = 100), abdominal migraine (n = 62), cyclical vomiting (n = 18), recurrent lower limb pain (n = 15), benign paroxysmal vertigo (n = 5) and benign paroxysmal torticollis (n = 1).
Previous medical history

Multiple antecedents could be reported. The percentages are calculated with respect to the 205 children with at least one antecedent.
Familial history
Three hundred and fifty-three (73.4%) had familial history of migraine, most commonly in the mother or grandmother (Fig. 1).
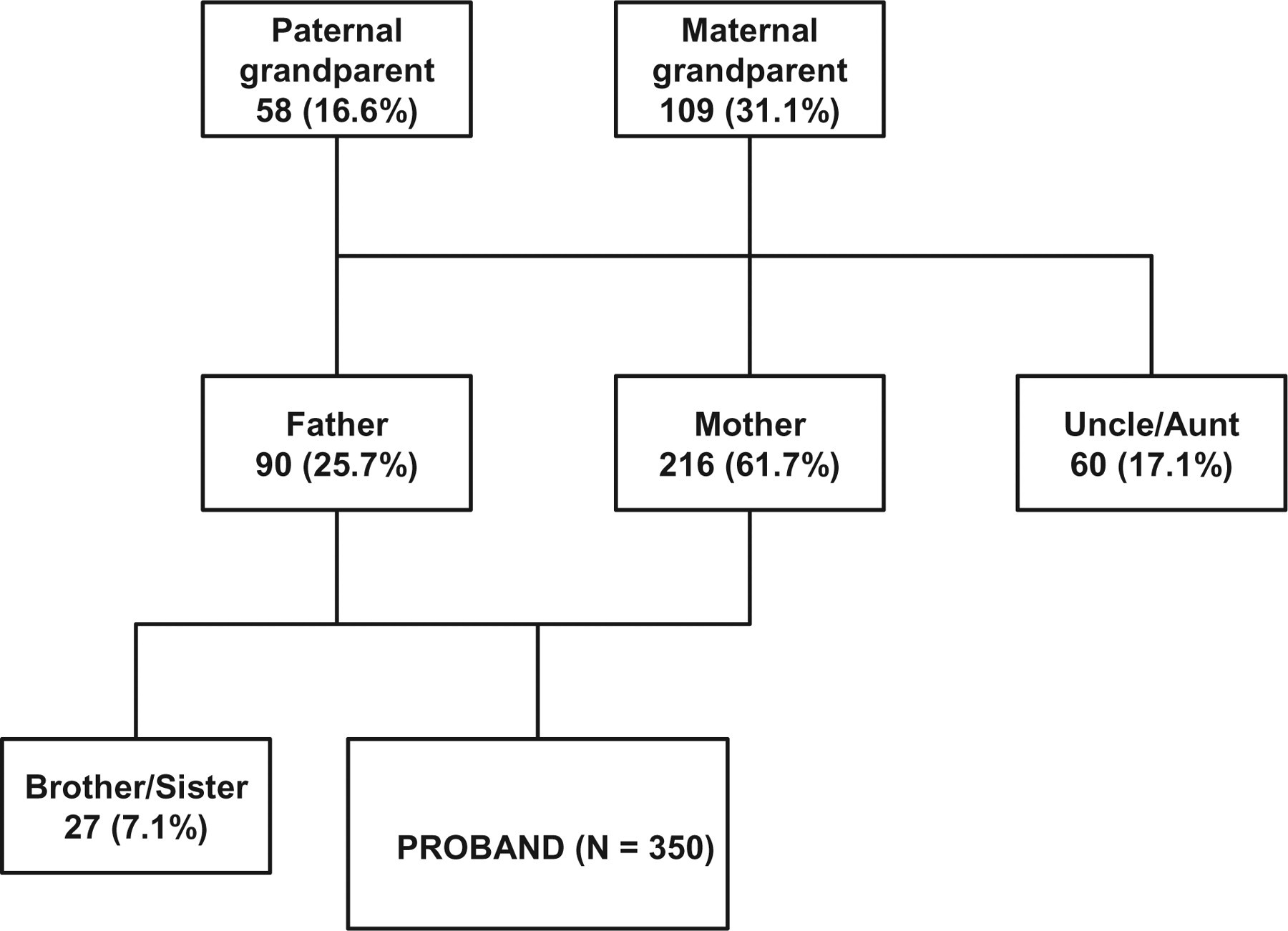
Familial antecedents of migraine. Multiple antecedents could be reported. The percentages are calculated with respect to the 350 children with at least one familial antecedent identified. For three children with familial antecedents of migraine, the affected relative was not identified.
Headache diagnosis
For the 398 children presenting a single headache type, the diagnoses assigned by the investigator are presented in Table 5. The most frequently assigned diagnoses were migraine without aura (50.8% of children), probable migraine (14.1%), migraine with aura (11.1%) and frequent episodic TTH (7.5%). Sixty children (15.1%) experienced headaches at least 15 days a month, thus fulfilling criteria for chronic headache. In 27 children (6.8%), analgesic medication abuse was suspected, in 18 of whom analgesics were taken at least 15 days a month. For six of these children, medication overuse was considered to be responsible for the headaches. The frequency of migraine headaches was evaluated as a function of age. The frequency of migraine with aura increased significantly with age (P < 0.01; χ2 test; Fig. 2). No such association with age was observed for migraine without aura or for probable migraine.
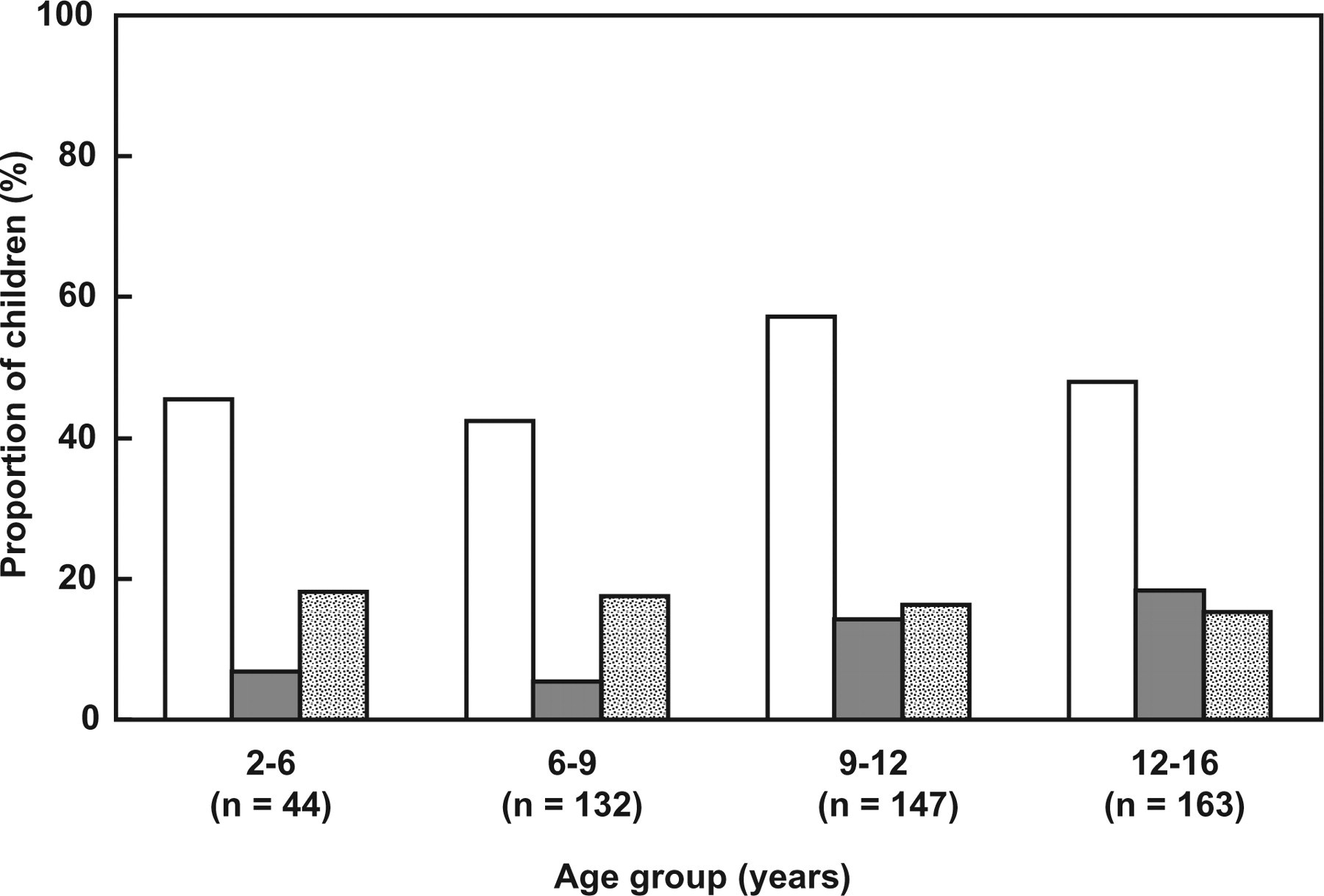
Frequency of migraine headaches as a function of age in 486 children. First column, migraine without aura [International Classification of Headache Disorders, 2nd edn (ICHD-II) class 1.1]; second column, migraine with aura (ICHD-II class 1.2); third column, probable migraine (ICHD-II class 1.6).
Headache diagnosis and consistency with the ICHD-II criteria in 398 children with a single type of headache
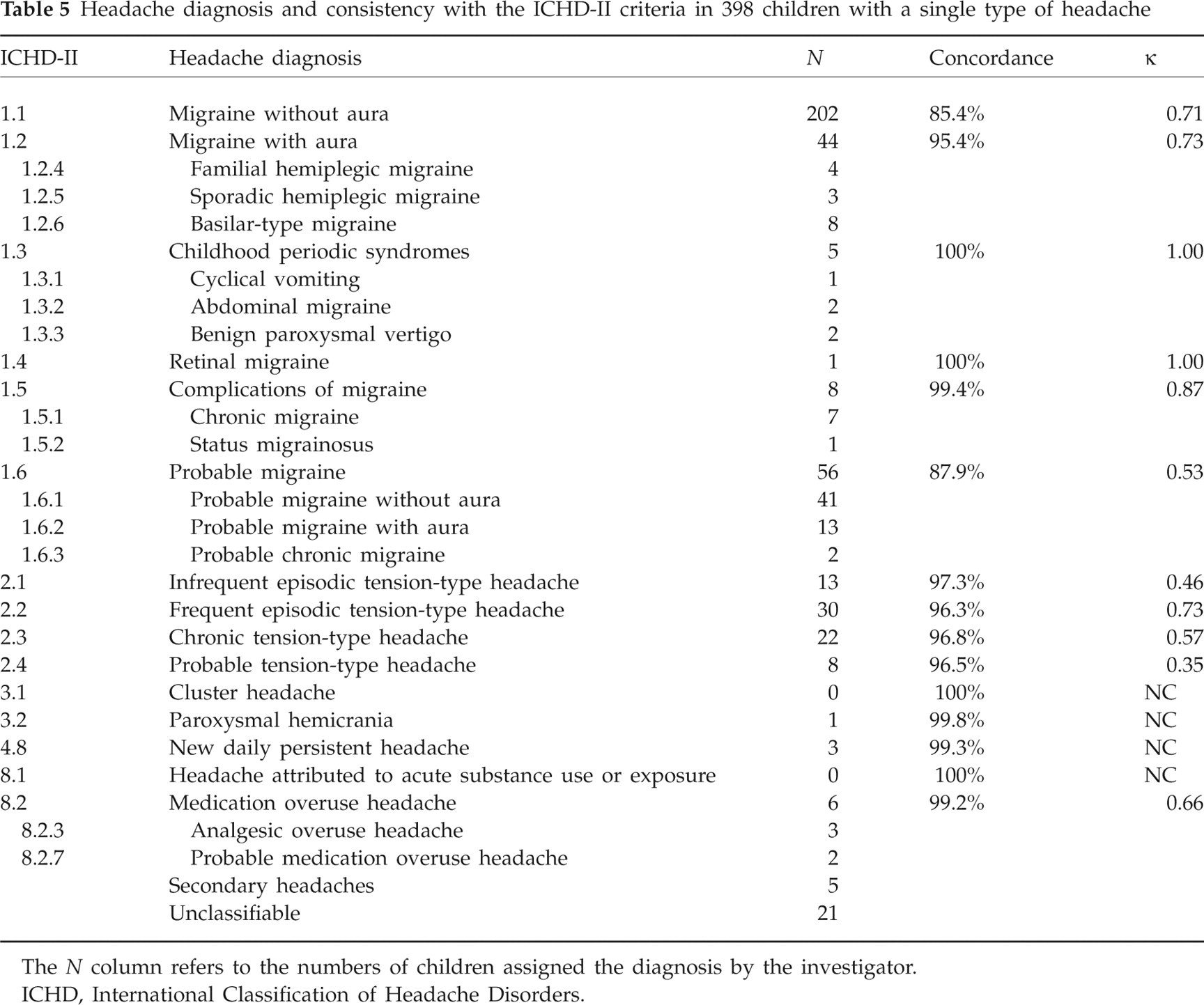
The N column refers to the numbers of children assigned the diagnosis by the investigator.
ICHD, International Classification of Headache Disorders.
The headache diagnosis made by the investigators according to their clinical judgement was compared with that made by strict application of the ICHD-II criteria (Table 5). For most of the diagnostic categories, the consistency of the investigator's diagnosis with the ICHD-II criteria was good (κ > 0.6 and ≤ 0.8) or excellent (κ > 0.8). For the most frequently assigned diagnosis (migraine without aura), diagnostic concordance was 85.4% (κ = 0.71). One child who fulfilled ICHD-II criteria for migraine without aura was not diagnosed as such by the investigator, and 17 children who did not meet the criteria were in fact diagnosed with migraine without aura by the investigator. Diagnostic categories in which concordance was moderate (κ > 0.4 and ≤ 0.6) or poor (κ > 0.2 and ≤ 0.6) included probable migraine and infrequent episodic, chronic and probable TTH.
Impact on school
Although the majority of children evaluated (n = 417; 86.9%) were in the expected class for their age, 184 (48.2%) had missed school due to their headaches. For these children, the mean number of days absent from school in the previous year was 6.6 ± 7.6 (median 4; range 1–50).
Discussion
The present study was a cross-sectional epidemiological multicentre survey of primary headache in children and adolescents conducted in France during 6 months. It is the first such French study to our knowledge.
The first edition of the International Classification of Headache Disorders (ICHD-I), established by the IHS in 1988, had set up important primary headache criteria for clinical practice and clinical research, but had been developed primarily for headache disorders in adults. For migraine, the only modification accepted for patients < 15 years old was a reduction in the required duration of episodes from 4 to 2 h. The ICHD-I paediatric migraine criteria had been later found to be too restrictive for clinical practice. Important shortcomings in sensitivity could be overcome by modifying two of its components: reduction of minimum time required for duration of the headache to 1 h, and admittance of bifrontal location. The IHS published ICHD-II in 2004, and modification has been made with regard to this. The study by Hershey et al. (5) evaluated the sensitivity of ICHD-II criteria in the diagnosis of childhood migraine. When the footnoted allowance of ICHD-II for 2-h duration was utilized, 71.9% of patients met the criteria, whereas this improved to 73.9% with 1-h duration. The applicability of the ICHD-I criteria for TTH in children had been criticized (6–8), but in ICHD-II the same diagnostic criteria are used for the diagnosis of TTH in children, adolescents and adults. Only isolated reports of cluster headache are available in paediatric patients (9). In a series of 35 patients with onset of cluster headache before age 18 years, all patients met the ICHD-I criteria for either episodic or chronic cluster headache, and all patients had clinical features and symptoms that were ‘consistent with adult forms’ of cluster (10). Only few paediatric cases of the other trigeminal autonomic cephalalgias (paroxysmal hemicrania and short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing) as well as the other primary headaches (primary stabbing headache, primary cough headache, primary exertional headache, primary headache with sexual activity, hypnic headache and primary thunderclap headache) have been reported in the literature (9), preventing the evaluation of ICHD criteria in children.
Overall, slightly more than half of the adolescents included in the present study were female. With regard to headache diagnoses repartition, migraine was clearly predominant, as 79% of diagnoses were of migraine (ICHD-II 1.1 to 1.6). The second most frequent headache group was represented by TTH. Of note, although chronic daily headache (CDH) is not considered as such in the ICHD-II, around 15% of our recruitment could be diagnosed with CDH. These figures are clearly different from the prevalence rates of these three diagnoses in the general paediatric population, with a prevalence range of 1.0–17.0% for migraine and 0.9–72.3% for episodic TTH (11). Recently, Wang et al. (12) found that 1.5% of all students aged 12–14 years in five selected middle schools in Taiwan fulfilled the criteria for primary CDH in the past year.
The reason why migraine was the predominant diagnosis could be related to the fact that migraine symptoms might be more stressful for the general practitioner because of their functional disability. The large predominance of migraine in our population also contributed to explain the typical headache profile of the child presenting to an out-patient department. Importantly for clinicians, there appeared to be high levels of disability reported by children and adolescents. The child suffered from headache slightly fewer than 10 days/month in around 74% of cases, data which are close from those of Winner et al. (13), where headache occurred for ≤ 9 days/month in just under three-quarters of children. Nearly half of children in our study had missed school due to their headaches, with the mean number of days absent from school in the previous year approaching a full week. Approximately 10% of children with migraines were found to have missed ≥ 1 day of school over a 2-week period, and nearly 1% missed 4 days (14). School absence in the past year due to headache was reported by 19, 48 and 64% of the children in the low, medium and high headache severity groups, respectively, in the study by Bandell-Hoekstra (15). For the student with recurrent headache, however, absence can become a major problem, with impact on social and academic relationships. Notably, Anttila et al. (16) have found that the incidence of headaches among children aged 6–7 years was significantly higher during their first year of school than it had been 6 months before they started school. Breuner et al. (17) found an association between poorer academic performance, symptoms of depression and decreased school attendance.
In adults, a large number of suspected precipitants for migraine and TTH have been reported, including mental and endogenous factors, absorbed factors and others. Few studies in children and adolescents have addressed this subject. In the present study, six triggers were reported by > 10% of patients: tantrums, school pressure, intense physical activity, heat, lack of sleep and noise. In a French paediatric series (18), the most frequent triggers of migraine attacks were, by decreasing frequency, heat, bright light, noise, annoyance, school pressure and shocks to the head. Rossi (8) reported that children with migraine with aura showed a higher occurrence of headache episodes induced by afferent stimulation than those with TTH.
A recent study (19) conducted in adults has found that the most frequently reported premonitory symptoms were fatigue (46.5%), phonophobia (36.4%) and yawning (35.8%). For episodic TTH, Karli et al. (20) found that head and neck movements followed stress–anxiety. Prodrome presence has not been addressed in detail in children and adolescents. In our study, 11.8% of patients reported prodromes. The commonest symptoms in the current study were a feeling of great tiredness, irritability, yawning or sighing, balance disturbance and mood change.
Co-morbidities such as recurrent abdominal pain, kinetosis, dizziness, sleep disorders, hyperactivity syndrome have been found in paediatric migraineurs (21). In our sample, a notable proportion of children and adolescents reported a history of allergy (1/3), asthma (1/4), travel sickness (1/4), neuropsychological disorders (1/6), parasomnia (1/7), gastrointestinal disorders (1/10) and hyperactivity (1/14). Bille (22) found a positive family history of allergy in 31.5% of the migraine group and 21.9% of controls, and an individual history of allergic disorders in 24.7% of children with migraine and 12.1% of controls.
Luc et al. (23), comparing children without headaches with those with headaches, found the latter to have more frequent symptoms of excessive daytime sleepiness, narcolepsy and insomnia than children without headaches. Focusing specifically on migraine patients, a significant difference was evident only for excessive daytime sleepiness and narcolepsy. In the study by Isik et al. (24), migraine headaches were mainly associated with snoring and parasomnias, as in our sample.
It had long been recognized that migraine headaches are frequently associated with gastrointestinal symptoms. Among the functional gastrointestinal disorders, cyclic vomiting syndrome and abdominal migraine are usually classified as migraine variants. The study of Boccia (25) showed a prevalence of 70% of functional gastrointestinal disorders in paediatric patients with a diagnosis of migraine. It was reported that motion and travel sickness were observed commonly in 49% of schoolchildren with headache (26). In one study (27) the frequency of associated travel sickness was significantly higher in children with headache (60.6%) than in the headache-free group (39.4%), and in children with migraine (53.2%) than in those with TTH (46.8%).
Lanzi (28) et al. found that patients affected by idiopathic headache shared some personality traits, mainly emotional rigidity and a tendency to repress anger and aggression. Common personality characteristics and psychological factors have also been noted by other authors, including depression (29, 30), anxiety (29–31) and hyperactivity (31, 32).
Conclusion
The present study is the first cross-sectional epidemiological multicentre survey of primary headache in children and adolescents conducted in France. It has provided some insight into the pattern of primary headache in French children and adolescents. The typical consulting child had headache characteristics highly reminiscent of migraine. Triggering factors, prodromes, co-morbidity and family history were also described. With regard to headache diagnoses repartition, migraine was clearly predominant, as 79% of diagnoses were of migraine (ICHD-II 1.1 to 1.6). For most of the diagnostic categories, the consistency of the investigator's diagnosis with the ICHD-II criteria was good or excellent. The ICHD-II criteria thus seem usable in clinical practice for the evaluation of primary headache in French children and adolescents.
Acknowledgements
We and the study investigators thank Laboratoire GlaxoSmithKline, France for its contribution to study implementation and data analysis for this trial.