
Abstract
The widely used criteria of the IHS to define migraine without aura in children are highly specific but show poor sensitivity, with a large percentage of headaches being classified as migrainous disorder (MD). The objective of this study was to assess how many headache patients in a series of children met the diagnostic criteria of the IHS for migraine without aura or MD and to determine the changes required to convert the greatest number of MD into migraine without aura, without affecting classification of the remaining headache types. A prospective study was undertaken of 131 patients under 15 years old referred to our centre for headache. Patients were classified according to the IHS criteria and according to a modification of these criteria consisting of: (1) reduction of minimum time required for classification into migraine without aura from 2 h to 1 h; (2) acceptance of bifrontal location in addition to hemicranial; (3) acceptance of either phonophobia or photophobia as valid criteria instead of requiring presence of both. Using the IHS criteria, 51 (39%) children were diagnosed as having migraine without aura and 26 (20%) as having MD. According to our revised IHS criteria, 68 (52%) were diagnosed as migraine without aura and nine (7%) as MD. When the three modified criteria were applied, three tension headaches and one unclassifiable headache changed category. When only reduced duration and bifrontal location were applied, none of the headaches other than MD changed category. Application of two modifications to the IHS criteria—reduction in duration of headache to 1 h and acceptance of bifrontal location—increased sensitivity without reducing specificity in classifying migraine without aura in children.
Keywords
Introduction
Migraine is among the most frequent headaches affecting children. Depending on the diagnostic criteria applied, the maximum age included, and other methodological factors, the prevalence of this disorder ranges from 3% to 10% of the paediatric population (1–3). With the development of new drugs that are effective only for migraines, diagnostic criteria with the best possible sensitivity and specificity are needed for use in both clinical practice and research.
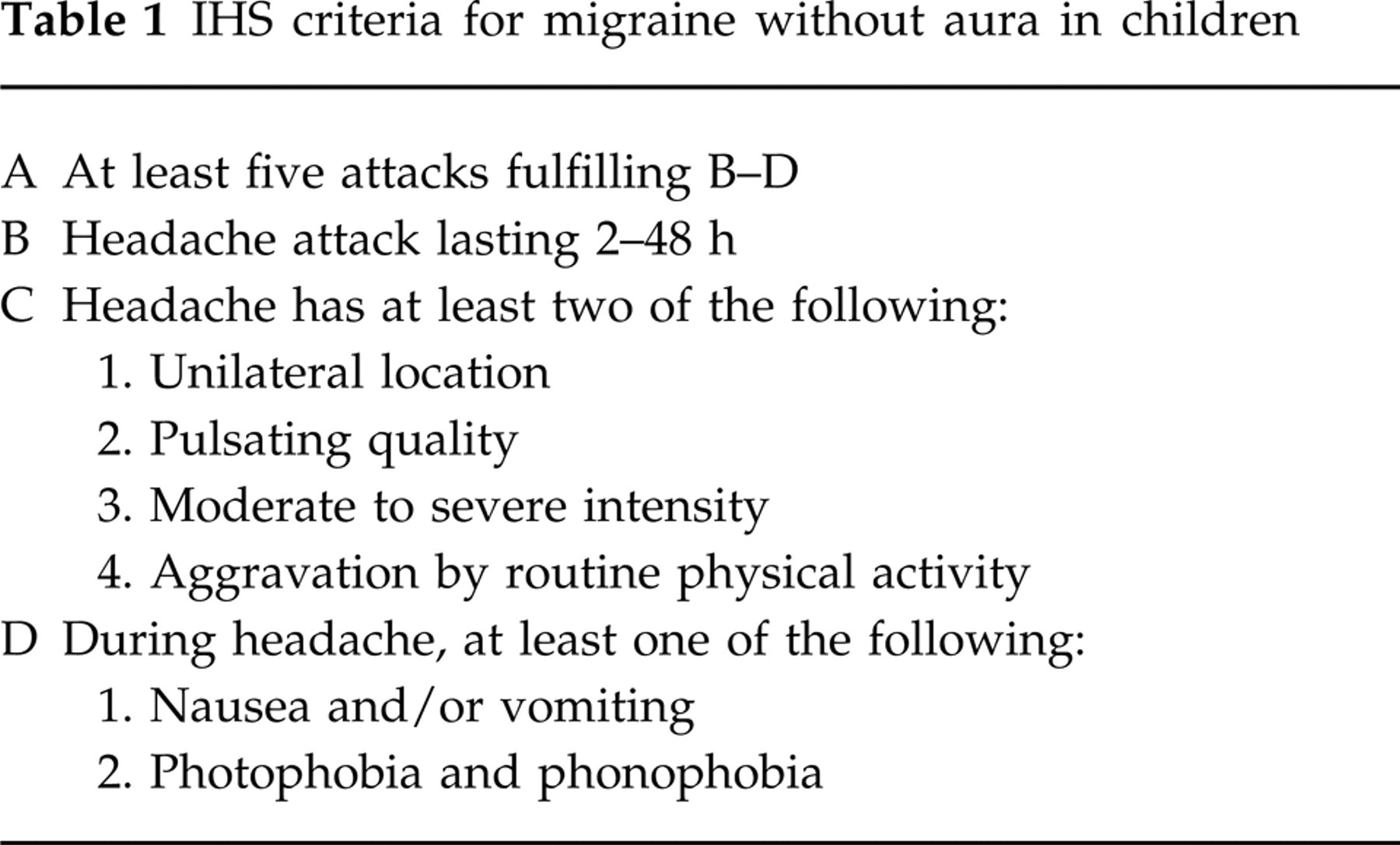
In 1988, the IHS published its proposed criteria for the diagnosis of migraine without aura (4) (Table 1). The only modification accepted for patients under 15 years old was a reduction in the required duration of episodes from 4 h to 2 h. The IHS criteria have proved to be highly specific but much less sensitive (5–8). Because of this fact, a large number of headaches are diagnosed as unclassifiable headache or as migrainous disorder (MD) not fulfilling the criteria (patients who meet all the IHS criteria for migraine but one). For this reason, various authors consider that clinical diagnosis assigned by a specialist should be the gold standard (5) for this pathology. This suggestion is open to criticism, (9) since each physician would have to formulate a personal definition of what constitutes a migraine without aura, as well as determine what clinical criteria are applied to the other headache categories (tension-type headaches, etc.). Another strategy is to validate modifications of the IHS criteria that result in incorporation of the greatest number of cases classified as MD within the migraine without aura group, in such a way that sensitivity is increased without excessive reductions in specificity.
IHS criteria for migraine without aura in children
The aims of this study were: (1) to quantify how many headache patients under 15 years old in our series met the diagnostic criteria of the IHS for migraine without aura or MD, and (2) to determine what changes are required to transform the greatest number of MD into migraine without aura, without producing reclassification of the remaining types of headaches.
Patients and methods
We prospectively studied a total of 131 consecutive patients under 15 years old (48% boys and 52% girls) aged 11.3 ± 2.6 years (mean ±
Sensitivity was calculated by considering the sum of headaches classified as migraine without aura and MD using the IHS criteria as ‘true’ migraines without aura and applying the formula: sensitivity = migraine without aura/migraine without aura + MD. Likewise, specificity was calculated as: specificity = non-migraine headache (classification alternative)/non-migraine headache IHS.
Results
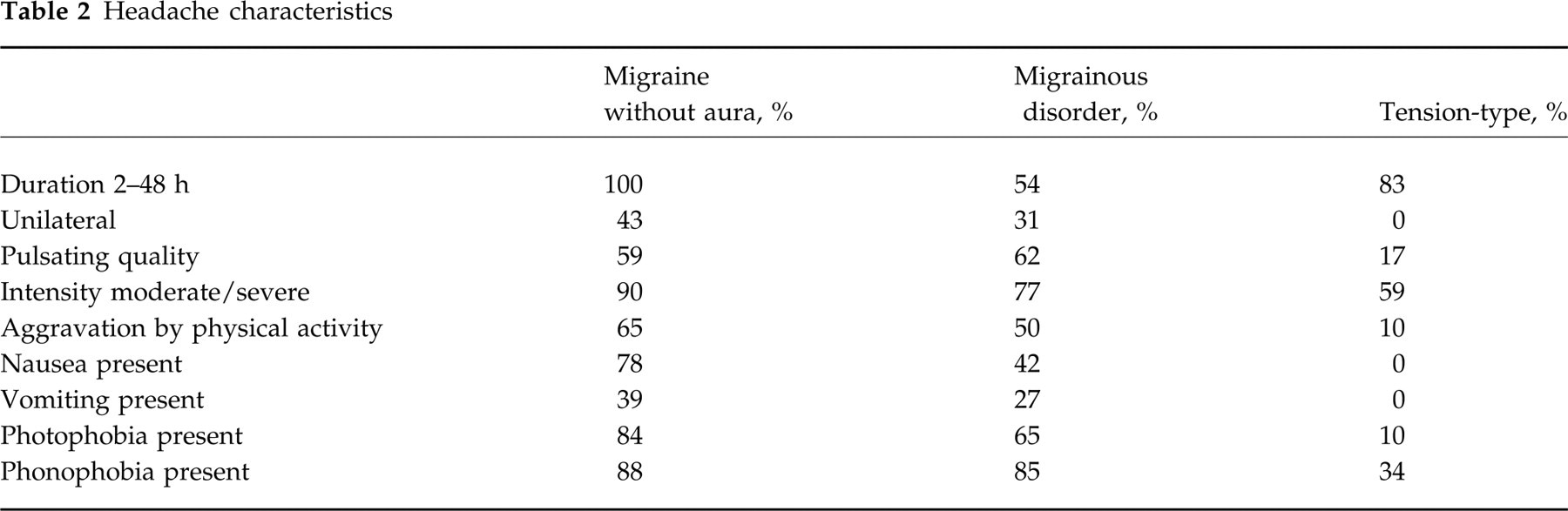
According to the IHS criteria, 51 patients were diagnosed as having migraine without aura, 26 were classified as MD and six as unclassifiable headache. The remaining patients received other diagnoses, including 29 episodic or chronic tension-type headaches and 13 migraine with aura. The distribution of the signs and symptoms recorded in each type of headache are shown in Table 2.
Headache characteristics
The modifications of the IHS criteria that most frequently resulted in change of classification from MD to migraine without aura were bifrontal location in nine cases, duration between 1 h and 2 h in eight cases, and presence of either photophobia or phonophobia in three cases. However, whereas application of the first two criteria did not induce changes in classification of the other types of headaches, application of the third criterion resulted in three tensional headaches being classified as migraine without aura. After applying our first two changes (location and duration) to the IHS criteria, the diagnoses included 68 migraine without aura and nine MD.
On the basis that the total of true migraines without aura was the sum of headaches classified as migraine without aura and headaches classified as MD, the IHS criteria showed a sensitivity of 66%, and, of course, a specificity of 100%. Using this same basis, the revised IHS criteria showed a sensitivity of 88% and a specificity identical to that of the HIS (100%).
Discussion
According to the IHS classification, fewer than half of our 131 patients under 15 years old received a diagnosis of migraine without aura. This result is in concordance with previous reports using these criteria (10, 11). Some studies include patients up to 17 years old in their paediatric group (5, 6, 12–15). Following the IHS proposal, we chose to study only children and adolescents under 15 years of age.
Migraine without aura can be diagnosed on the basis of previously defined symptom-based criteria (IHS or others) or by intuitive clinical diagnosis assigned by the physician evaluating the patient. The use of clinical diagnosis as the gold standard method for migraine without aura has been challenged by some authors (9). They contend that different doctors can have different criteria and that ultimately there would have to be a common series of signs and symptoms that induce them to think that that headache is a migraine without aura. On the other hand, the IHS criteria are also a convention. Thus, we can only try to increase the sensitivity of the IHS criteria or elaborate new criteria that can be accepted by the majority of neurologists.
We attempted to evaluate which modifications of the IHS criteria would result in the greatest number of headaches in the MD category being classified as migraine without aura
Many authors have argued that minimum headache duration required for diagnosis of migraine without aura should be reduced in the paediatric population, on evidence that headaches in children do not last as long as in adults (6, 7, 13–15). Failure to fulfil this criterion is one of the most frequent reasons why a headache cannot be classified a migraine without aura and passes to the MD category (16). There are also indications that unilateral presentation is not as common in children as in adults (5, 6, 13–15, 17). For this reason, it has been suggested that bifrontal location should be admitted as a defining criterion for migraine without aura, an idea that would not contradict the configuration of the trigemino-vascular system at this level. Finally, the suggestion of including photophobia or phonophobia as separate criteria proposed by some authors (7, 13) has the drawback that this parameter is accepted for tension-type headaches and its inclusion might produce reclassification of some tension-type headaches, as occurred in our population.
To sum up, correct classification of migrainous headaches is important for treatment and research purposes. Use of the IHS criteria for diagnosing migraine in children has evidenced important shortcomings in sensitivity that can be overcome by modifying two of its components: reduction of minimum time required for duration of the headache to 1 h, and admittance of bifrontal location. With these modifications we obtained a sensitivity of 88% (IHS 66%) in our population without altering specificity.