
Abstract
Apelin has been reported to regulate mitochondrial function in myocardial ischemia-reperfusion injury and cerebral ischemia-reperfusion injury. However, the role of apelin-13 in lung ischemia-reperfusion injury (LIRI) remains unclear. This study established an experimental rat model to evaluate the underlying mechanisms of apelin-13 on LIRI. Twenty-four rats were randomly divided to sham operation group (group SM), ischemia/reperfusion group (group IR), and apelin-13 treatment group (group APL). The effects of apelin-13 on LIRI were determined histologically using H&E staining, while the wet/dry weight ratio was used to assess lung edema caused by LIRI. Inflammatory cytokines were also detected in Bronchoalveolar lavage (BAL) fluid by ELISA. The protein expression of UCP2 and the morphological changes of mitochondria were determined by western blotting and electromicroscopy, respectively. The results demonstrated the structural damage of lung tissues and lung edema in group IR. An increased level of inflammatory cytokines including IL-1β, IL-6 and TNF-α was observed in rats with LIRI using ELISA. After that, oxidative stress and morphological damage of mitochondria were also shown in group IR. Yet, the application of apelin-13 reversed all these deleterious effects in group APL. The protective effects of apelin-13 were indicated by decreased reactive oxygen species (ROS) and elevated UCP2 expression levels in rats. In conclusion, this study revealed that apelin-13 had protective effects against LIRI via attenuating lung edema, the production of inflammatory cytokines, oxidative stress and mitochondrial dysfunction.
Introduction
Lung ischemia-reperfusion injury (LIRI), especially the severe form pulmonary edema or acute respiratory distress syndrome, is an important cause of mortality in patients. 1 LIRI often occurs after reperfusion to the ischemic lungs, resulting in oxidative stress and inflammatory response that may lead to the development of lung tissues damage. 2 It is commonly recognized that the pathogenesis of LIRI is related to many factors including mitochondrial function disorders, 3 free radical damage, 4 inflammatory response, complement activation, microcirculatory disorders and increased permeability of intracellular calcium superoxide.
Mitochondrial dysfunction and the overproduction of reactive oxygen species (ROS) have been reported to mediate the pathogenesis of LIRI. Previous study has clarified that mitochondrial respiratory chain dysfunction lead to an increase in ROS after reperfusion begins. 5 The production of ROS can attack mitochondrial membrane, trigger lipid peroxidation, and activate the opening of mitochondrial permeability transition pore (MPTP). 6 Chen et al. 3 have suggested that exogenous irisin through intravenous administration can improve mitochondrial function to alleviate LIRI. Besides, suplatast tosilate can also prevent hypertoxic lung injury by reducing oxidative stress caused by ROS, such as scavenging hydroxyl radicals. 7 Nevertheless, no effective treatments for LIRI have been developed at this stage. Therefore, it is urgent to explore therapeutic methods for the regulation of mitochondrial function to alleviate LIRI.
The G protein-coupled receptor APJ and Apelin (homologous ligand to APJ) are widely expressed in different tissues of the body, and participated in a variety of important physiological and pathological processes, such as cardiovascular function regulation, energy metabolism regulation, neuroprotection and fluid homeostasis. 8,9 Numerous studies have shown that apelin can regulate mitochondrial function in myocardial ischemia-reperfusion injury by inhibiting dynamin-associated protein 1 (DSP-1) 10 and mitochondrial ROS. 11 The Apelin-APJ system may be an optimistic therapeutic target for ischemic-reperfusion related diseases. 12 Zhang et al. 13 have suggested melatonin attenuates bleomycin-induced lung injury by modulating apelin-13, and thereby improving mitochondrial dysfunction, suggesting the protective effect of apelin-13 on LIRI. In spite of its increased clinical application on the effects of apelin-13 on cerebral ischemia-reperfusion injury and myocardial ischemia-reperfusion injury, the protective mechanisms of apelin-13 on the LIRI are still unclear.
Uncoupling protein 2 (UCP2) is an anionic carrier protein located on mitochondria that regulates mitochondrial ATP and ROS production, 14 and is one of the important second messenger signals in cells. 15 UCP has high antioxidant activity, which can not only increase superoxide dismutase (SOD) activity, but also improve cell survival in a reduced ROS environment. Thus, we speculated that apelin-13 may protect against mitochondria dysfunction and ROS production in lung injury via regulating UCP2.
Therefore, the aim of this study was to discover the beneficial role of apelin-13 in regulating mitochondrial dysfunction, and to develop a new therapeutic approach for lung injury in clinic setting. The results revealed that apelin-13 can improve mitochondrial function and anti-oxidative stress by regulating UCP2 protein levels, and protect lung against ischemia-reperfusion injury.
Materials and methods
Experimental animals
All animal experiments were approved by the animal care and use committee of Wenzhou Medical University. Adult male Sprague-Dawley (SD) rats weighing 280–320 g were purchased from Shanghai Slac Experimental Animal Co., Ltd. (Shanghai, China). All rats were kept in plastic cages in Wenzhou Medical College Animal Center with a 12 h day/night cycle at 55–60% of humidity and temperature of 19–25°C. All animals were provided with a standard laboratory nutrition meal and sufficient water. The experimental protocol was approved by the institutional Committee on Animal Care and Use of Wenzhou Medical University (No. wydw 2015-0121).
Study groups
Rats (n = 24) were randomly divided into three groups: a) group SM: the chest were exposed but not operated, b) group IR: lung ischemia-reperfusion with 5 ml saline injection before reperfusion, and c) group APL: apelin-13 administration prior to reperfusion.
The construction of lung ischemia-reperfusion model in rats
The rats were fasted for 12 h prior to the experiments with free access to water. Rats were anesthetized on the day of the experiment with an intraperitoneal injection of 80 mg/kg ketamine and 5 mg/kg diazepam. Then, animals were intubated via tracheotomy and connected to a small animal ventilator (HX-300; TME Technology Corporation, Chengdu, China) for mechanical ventilation. The clinical parameters were present as follows: tidal volume = 12 mL·kg−1; respiratory rate = 90–100 breaths min− 1 ; inspiratory/expiratory ratio = 2/3. After that, the right femoral artery and vein were cannulated for infusion. The rats’ chest was firstly opened through the 4th intercostal space. The subcutaneous tissues were separated and the exposed pleura was cut in the expiratory phase. The tidal volume was then adjusted appropriately to reveal the left thoracic cavity, allowing the exposure of left hilar. Unfractionated heparin (300 U/kg) was administrated to the portal vein through the femoral vein, followed by 10 min stable equilibrium of rats. To achieve lung ischemia-reperfusion, the left hilar was occluded by a non-invasive vascular clamp for 1 h. Signs of successful blockade were no vasomotor in the hilar and no ventilation in the left lung. Before releasing the vascular clamp, 5 ml of saline was given intravenously in the group IR, while 1 μg/kg of Apelin-13 was added in 5 ml saline (pumping time of 10 min) for group APL. 16 Moreover, the vascular clamp was released after 60 min and the left lung was completely re-expanded with blood supply for 2 h. Hydration of the animals were given by infusion of 3 ml·kg−1·h−1 saline. 17 The heart rate and blood pressure of the rats were continuously recorded throughout the entire procedure using MedLab U/4C051 system (Nanjing Medease Science and Technology Corporation, Jiangsu, China). The depth of anesthesia was maintained by 0.5% sevoflurane with oxygen during the experiment. Body temperature of the rats were also kept at 37 ± 0.5°C.
Experimental protocols
After the construction of lung ischemia-reperfusion model, all animals were euthanized at the end of the 3 h of reperfusion during anesthesia with sevoflurane. Subsequently, the lung tissues and BALF samples were obtained to analysis the inflammation level, pulmonary pathology, lung W/D ratio, arterial blood gas (ABG), the content of IL-6, IL-1β and TNF-α in BALF, the activity of SOD, and the levels of MDA and UCP2.
Bronchoalveolar lavage fluid (BAL fluid)
The left lung was divided into upper and lower lobes of left lung after euthanisation. The left upper lobe tissues were prepared for subsequent experiments, while the left lower lobe lung tissues were used for BAL fluid. 18 Phosphate buffered saline 5 ml was slowly injected into the lungs, and this procedure was repeated three times. The extracted lavage fluid was collected and stored in the refrigerator at 4°C. The BAL fluid was then centrifuged at 1,500 r/min for 10 min. After that, the supernatant was gathered and stored at −80°C for further analysis.
Arterial blood gas analysis (ABG)
In this experiment, pulmonary function was evaluated using arterial blood gas analyzer (i-STAT Corporation, East Windsor, New Jersey). Before induction of lung ischemia-reperfusion, 0.5 ml of arterial blood was drawn and measured; while after reperfusion, another 5 ml of blood was drawn at the end of 3 h reperfusion.
Histological examination and lung injury score (LIS)
Biopsies of the lung tissues were fixed with 10% formalin at 4°C for 24 h. The tissues were then dehydrated and embedded in transparent paraffin. For the histological examination, the lung tissue samples were serially cut into 5 µm sections and stained with hematoxylin and eosin (H&E). Each stained tissue sections were observed under Olympus BX-51microscope (HPF, ×200, Japan). A scoring system called lung injury score (LIS) was used in this study to evaluate the degree of lung injury. 19 The assessment of histologic features included edematous changes of alveolar wall, hemorrhage and thickening of pulmonary interstitial. Besides, each histological characteristic was scored from 0-normal to 5-severe, and the overall scoring of lung injury was categorized as follows: 0–5: normal to minimal injury; 6–10: mild injury; 11–15: moderate injury; 16–20: severe injury. 20
Measurement of wet-to-dry ratio of the lung
The upper lobe of left lung was taken and weighed to determine the lung wet/dry weight ratio, allowed the measurement of water content in lung tissues. Each lung was weighted before and after being placed in an oven at 80°C for 48 h. The lung wet/dry ratio was calculated as the wet weight divided by the dry weight of each lung.
Enzyme-linked immunosorbent assay (ELISA)
The expression of tumor necrosis factor (TNF)-α, interleukin (IL)-1β and IL-6 in the BAL fluid was measured using ELISA kits (Westang biotechnology Co. Ltd., Shanghai, China), in accordance with the manufacturer’s instructions.
Malondialdehyde (MDA) levels, superoxide dismutase (SOD) activity in lungs
Several samples from left upper lobe lung were carefully cut into small segments, then homogenized in phosphate-buffered solution (0.1 M·ml−1, pH 7.4) by a homogenizer. The homogenate was gathered and centrifuged (12,000 × g, 30 min, 4°C), followed by gathering the supernatant fraction to detect the levels of SOD activities and MDA in lungs. All detection steps were tested according to the standard protocol of the kit (Nanjing Institute of Bioengineering Institute, Nanjing, China). MDA levels represented the rate of peroxidation which expressed as nmol/mg protein, while SOD activity was determined by the superoxide radicals which expressed as U/mg protein in tissues. 20
Western blot analysis of UCP2 in lung tissue
Lung tissues were placed in lysis buffer, incubated on ice for 30 min and centrifuged at 13,500 rpm for 10 min. Protein concentrations were determined using a bicinchoninic acid (BCA) Protein Assay Kit (Thermo Scientific, USA). Lysate (30 µg protein) was separated by 12% SDS-PAGE and electrophoretically transferred to a PVDF membrane. Membranes were blocked with 5% skim milk, followed by incubation at 4°C overnight with a specific primary antibody recognizing UCP2 (1:1000, ab97931, Abcam) and GAPDH (1:1000, 8884, Cell Signaling Technologies). After incubation with the HRP-conjugated secondary antibodies (1:10,000, BS13278, Bioworld Technology), immunoblots were developed using ECL. Luminescence was finally detected with Bio-Rad automated rapid gel imaging system and analyzed using ImageLab software.
Ultrastructure
Preparation of left upper lobe lung tissues were described in our previous study. 20 The pneumocytes on the grid were examined using H-7500 electron microscopy (HPF, ×20,000, Hitachi, Japan).
Statistical analysis
The number of animals in each group were determined according to the results of the preliminary study (n = 5). The arterial partial pressure of oxygen (PaO2) at the end of experiment were 95.00 ± 3.46, 78.60 ± 6.35 and 92.40 ± 4.45 in group SM, group IR and group APL, respectively. Based on a two-tailed type one error at 5% and type two error of 10% (α = 0.05, β = 0.1), the size of 5 in every group were calculated by PASS (Power Analysis and Sample Size; 11.0). In consideration of the potential attrition, eight rats were recruited per group. The data were analyzed by SPSS (version 19.0; SPSS Inc., Chicago, IL) with values displayed as mean ± standard deviation (SD). Multiple comparisons between groups were analyzed by one-way ANOVA. Least significant difference (LSD) test was also performed when variance was uniform, while Dunnett’s T3 test was performed for heterogeneity of variance data. P < 0.05 was considered as statistically significant.
Results
ABG analysis
No significant differences in baseline values of ABG parameters, including potential of hydrogen (pH), PaO2, arterial partial pressure of carbon dioxide (PaCO2), lactic acid (Lac) and base excess (BE), were found among the three groups (Table 1). Compared with the baseline values, both PaO2 and Lac values among three groups were dropped at the end of reperfusion, while the final BE was only reduced in IR group (Table 2). Additionally, PaO2 and BE values in group IR were relatively lower (P < 0.05) than those in group SM, whereas PaCO2 and Lac values were increased (P < 0.05). Compared with group IR, both PaCO2 and Lac values were significantly diminished in group APL (P < 0.001), while PaO2 and BE were enhanced (P < 0.05).
Baseline values of ABG parameters in rats (n = 8 in each group).a
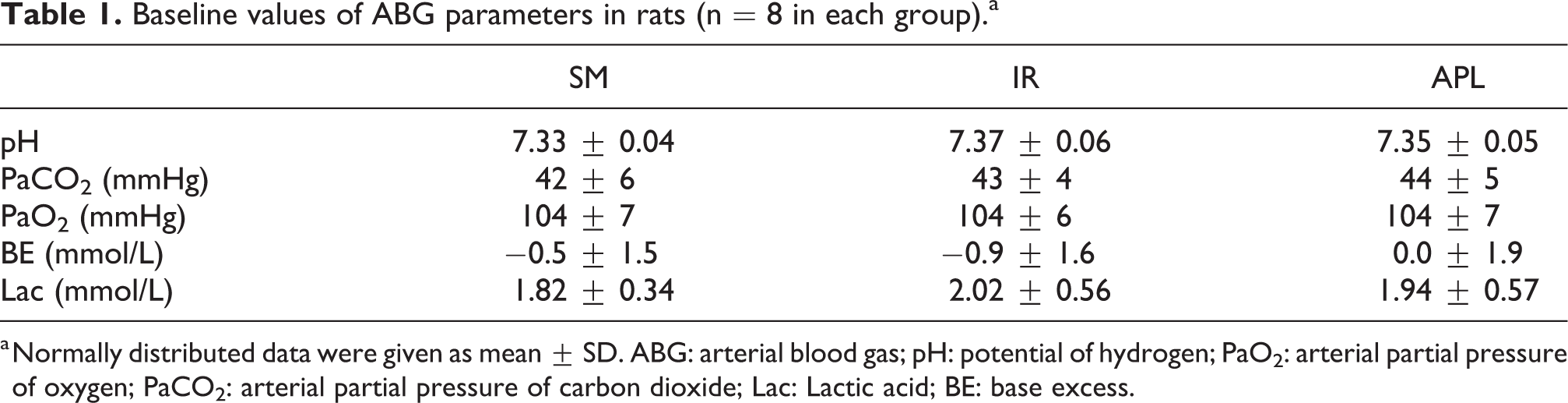
a Normally distributed data were given as mean ± SD. ABG: arterial blood gas; pH: potential of hydrogen; PaO2: arterial partial pressure of oxygen; PaCO2: arterial partial pressure of carbon dioxide; Lac: Lactic acid; BE: base excess.
ABG parameters at the end of reperfusion in rats (n = 8 in each group).a

a Normally distributed data were given as mean ± SD. ABG: arterial blood gas; pH: potential of hydrogen; PaO2: arterial partial pressure of oxygen; PaCO2: arterial partial pressure of carbon dioxide; Lac: Lactic acid; BE: base excess.
*P < 0.05 (vs. group SM); #P < 0.05 (vs. group IR).
Histology examination, lung injury score (LIS) and W/D weight ratio
To determine whether apelin-13 can protect against LIRI, the histologic characteristics were evaluated by light microscopy. As shown in Figure 1, no obvious histological abnormalities were observed in lung tissues of mice in group SM, while the structure of alveoli was disrupted severely and widely in group IR with intra-alveolar edema, hemorrhage and interstitial thickening. These histopathologic damages were markedly alleviated with administration of apelin-13, which showed as lighter damage in alveolar structures and less presentation of erythrocytes and inflammatory cells. These findings were consistent with the results of lung injury score (Figure 2B). The lung injury score of group SM was below 5, which was within the range of normal to minimal injury. The LIS of group IR was about 15, while the LIS of group APL was remarkably decreased from moderate injury to mild injury after the administration of apelin-13. To determine changes in lung edema caused by reperfusion, the lung wet/dry weight ratio was measured (Figure 2A). Group IR exhibited an increase of the lung wet/dry weight ratio compared with the group SM (P < 0.05), however, a decreased lung wet/dry weight ratio was shown after injection of apelin-13 (P < 0.05).

Apelin-13 reduces the structural damage in LIRI rats’ model. Histopathological changes in the lung tissues observed by H&E staining with the magnification 200× in group SM, group IR and group APL. Eight rats were recruited in each group. Scale bar, 50 µm.

Lung wet/dry weight ratio, lung injury score, concentration of inflammatory cytokines, SOD activity and MDA level in lung tissues. (A) The lung wet/dry weight ratio (W/D) was assessed in those experimental groups. (B) The lung injury scores (LIS) was determined by a pathologist, who was blinded to the grouping. (C, D) The expression levels of IL-1β, IL-6 and TNF-α in BAL fluid were detected by ELISA. (E) SOD activities and (F) MDA level in lung tissue. BALF: Bronchoalveolar lavage fluid; SOD: superoxide dismutase; TNF-α: tumor necrosis factor-α; IL-1β: interleukin-1β; IL-6: interleukin-6; MDA: malondialdehyde; *represented P < 0.05 vs. group SM; #represented P < 0.05 vs. group IR.
Inflammatory cytokines
The expression levels of IL-1β, IL-6 and TNF-α in BAL fluid in different groups were then evaluated by ELISA. Compared to the group SM, the rats treated with saline before reperfusion had higher levels of IL-1β, IL-6 and TNF-α in the group IR (all P < 0.001) (Figure 2C–2D). As expected, rats treated with apelin-13 prior to reperfusion attenuated those inflammatory cytokines (P < 0.001, P < 0.001 and P = 0.034, respectively), whereas IL-1β, IL-6 and TNF-α expression levels in group APL were still higher than those in group SM.
Oxidative stress
As shown in Figure 2E and 2F, group IR showed increased MDA levels (P < 0.001) and decreased SOD activity (P < 0.001) when compared with group SM. After administration of apelin-13, the MDA level was lower in group APL than that in group IR (P < 0.001), however, the SOD activity of group APL was higher than that of group IR (P = 0.006).
Morphological change of mitochondria and UCP2 protein expression
Morphological changes of mitochondria among different groups were observed under electron microscope (Figure 3). The appearance of mitochondria in group SM was round with intact structure, and most of cristae was lamellar. In group IR, there was swelling of the mitochondria, and shorter and less cristae. The mitochondrial morphology of the group APL is closer to the SM group with dense cristae.

Electron micrograph of lung (magnification, 20000, n = 8). N, nucleus; Mit, mitochondria. Scale bar, 0.5 µm. Ultrastructural architecture seemed normal in group SM with normal mitochondria in type II pneumocytes.
In addition, the protein expression of UCP2 protein expression was detected by western blotting. A significant decreased UCP2 expression was observed in group IR compared with group SM (P < 0.05) (Figure 4), however, the treatment of Apelin-13 prior to reperfusion protected the expression of UCP2 in group APL, indicating a notable high expression level of UCP2 than group IR (P < 0.05).

Western Blot analysis of UCP2 in lung tissue (n = 8). *P < 0.05 vs. group SM; #P < 0.05 vs. group IR. UCP2 protein expression was significantly decreased in group IR than group SM (P < 0.05), UCP 2 protein expression was higher in group APL compared with group IR (P < 0.05).
Discussion
In the present study, we found that LIRI was clinically manifested by high levels of inflammatory cytokines, severe oxidative stress and mitochondrial injury. Apelin-13 could alleviate LIRI by reducing the inflammatory response, lung edema, LIS, oxidative stress and mitochondrial dysfunction, and improving pulmonary oxygenation in rats. Moreover, the expression of UCP2 might be involved in the apelin-13 treatment against LIRI.
LIRI is a severe disease with significant morbidity and mortality. Apelin-13 has beneficial effects on cerebral ischemia-reperfusion injury and myocardial ischemia-reperfusion injury. However, specific study on the protective role of apelin-13 in LIRI is required. Apelin is a ligand for the G-protein coupled receptor APJ. 8 Recent studies have demonstrated that apelin may be a prominent agent in lung diseases. 21 –23 Visser et al. 23 have found that apelin reduces fibrin deposition, pulmonary inflammation, right ventricular hypertrophy and partial restores alveolarization in neonatal hyperoxia-induced lung injury of rat pups. Meanwhile, apelin-APJ system is an endogenous protective mechanism against lung injury that is up-regulated in lipopolysaccharide (LPS)-induced lung injury, while exogenous apelin attenuates LPS-induced lung injury by decreasing pulmonary inflammation and improving peroxidation in lung injury. 21 Our data showed that LIRI significantly induced histological changes of lung tissues and increased the expression of inflammatory cytokines. Accordingly, the apelin-13 administration to rats model resulted in several protective effects when compared to group IR in this study, as showed by mild damage of alveolar structures and reduced number of erythrocytes and inflammatory cells. In addition, apelin-13 remarkably lowered lung wet/dry weight ratios and inflammatory cytokines (IL-1β, IL-6 and TNF-α) expression levels. The above results revealed the potential therapeutic effects of apelin-13 against LIRI.
The oxidative stress or excessive ROS may cause the activation of neutrophils and cell adhesion molecules (CAMs), followed by their migration into the local tissues to trigger severe inflammatory responses and tissue damage. 24 It is suggested that apelin can regulate mitochondrial function in myocardial ischemia-reperfusion injury via inhibiting DSP-1 10 and mitochondrial ROS. 11 Our results had the similar findings that apelin-13 increased ROS levels and MDA concentrations, and decreased the activity of SOD in rats with LIRI. Besides, the decrease in PaO2 and increase in PaCO2 were also significantly reversed by apelin-13 treatment. Therefore, apelin-13 could minimize LIRI by improving lung oxygenation and peroxidation. Furthermore, we explored whether UCP2 is involved in the underlying mechanisms of apelin-13 against LIRI.
The mitochondrial injury was observed as swelling with the presence of short and less mitochondrial cristae in the group IR, however, the intervention of apelin-13 significantly reversed the morphological changes of mitochondria. Uncoupling proteins (UCPs) are known as mitochondrial inner-membrane proteins that regulate proton leakage and control the formation of superoxide and other downstream reactive oxygen species. 25 There are three subtypes of UCPs including UCP1, UCP2 and UCP3. 26 The up-regulation of UCP1 in adipocytes and UCP3 in skeletal muscle cells by apelin were demonstrated in many studies. 27 –29 The 55% to 60% similarity between UCP2 and UCP1 was observed, as well as the UCP2 and UCP3. 30 –32 By immunodetection of yeast expressing UCP2, which found that UCP2 is only localized in mitochondria and is widely distributed in various organs such as lung, brain, spleen and kidney, 30 whereas the highest expression of UCP was observed in lungs. Moreover, UCP2 is also involved in various cell physiological functions, especially anti-oxidative stress response. 25 Accumulating reports have suggested that UCP2 plays critical roles in reducing ROS production 33 and inhibiting ROS-mediated apoptosis of lung epithelial cells. 34 Our study are in agreement with those previous reports that treatment with apelin-13 increased the UCP2 expression and attenuated IL-1β, IL-6 and TNF-α expression levels. Apelin exerted protective effects against LIRI via its anti-inflammatory and antioxidative stress. Therefore, we speculated that apelin may improve mitochondrial damage by up-regulating UCP2 to reduce inflammation, oxidative stress and lung epithelial cell damage, and ultimately causing the protection of lungs.
There are several limitations in our work as follows: (a) the specific role of UCP2 in the protective effect of apelin-13 on LIRI has not been accurately determined; (b) the lack of mitochondrial damage specific markers such as SOD2 in the study, even though the results of SOD activity, MDA level and electron microscopy have confirmed the mitochondrial ROS production and structural damage; (c) the fixed reperfusion duration could not quantify the actual lung damage impairment and its correlation with the apelin-13 treatment at various time points during ischemia-reperfusion process. Therefore, more researches are needed to explore the potential therapeutic effects of apelin-13 in treating lung ischemia-reperfusion injury.
In conclusion, our results reveal that apelin-13 may alleviate LIRI by attenuating lung edema, the production of inflammatory cytokines and oxidative stress, as well as mitochondrial damage. The above evidences provide new ideas for treatment of LIRI and suggest that apelin-13 may serve as a protective drug for lung ischemia-reperfusion injury through UCP2 protein expression.
Footnotes
Abbreviations
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publications of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by Zhejiang Provincial Natural Science Foundation of China (Number: LWQ20H310001) and Medical Health Science and Technology Project of Zhejiang Provincial Health Commission, China (Number: 2019RC209).