
Abstract
In this study, we aimed to show the effect of adenosine 5′-triphosphate (ATP) on sunitinib-induced cardiac injury in rats. The rats (n = 30) were divided equally into three groups as sunitinib group (SG), sunitinib plus ATP group (SAG), and healthy group (HG); 2 mg/kg ATP was injected intraperitoneally (ip) to the SAG group. Same volume normal saline as solvent was administered ip to the other two groups. After 1 h, 25 mg/kg sunitinib was applied orally via catheter to stomach in the SAG and SG groups. This procedure was repeated once daily for 5 weeks. At the end of this period, all animals were sacrificed and their cardiac tissue was removed. Malondialdehyde (MDA), total glutathione (tGSH), tumor necrosis factor α (TNF-α), and nuclear factor κB (NF-κB) levels in rats’ cardiac tissues and troponin I (Tp-I) levels in rats’ blood samples were evaluated. Histopathological analysis was also performed in cardiac tissues of the animals. MDA, TNF-α, NF-κB, and Tp-I levels were higher in the SG group compared to the SAG and HG groups (p < 0.001). tGSH levels of the SG group were lower than the SAG and HG groups (p < 0.001). The structure and morphology of cardiac muscle fibers and blood vessels were normal in the control group. In the SG group, obvious cardiac muscle tissue damage with dilated myofibers, locally atrophic myofibers, and congested blood vessels were observed. In the SAG group, marked amelioration in these findings was observed. We showed this for the first time that ATP administration exerts a protective effect against cardiac effects of sunitinib.
Introduction
Sunitinib malate (Su-11248; Sutent1; Pfizer Inc., New York City, New York, USA) is a multitargeted, oral, small molecule, tyrosine kinase inhibitor (TKI) and has antiangiogenic activities besides its anticancer effects. It is currently approved by the US Food and Drug Administration and by the European Commission for the treatment of several malignances including advanced renal cell carcinoma, 1 treatment of gastrointestinal stromal tumor after progression under imatinib therapy or for patients intolerant to imatinib, 2,3 and treatment of advanced stage pancreatic neuroendocrine tumors. 4 –6 In addition, the compound is currently under evaluation for the treatment of various solid tumors and efficacy was reported in colorectal cancer, non-small cell lung cancer, malign melanoma, chronic myeloid leukemia, and breast cancer. 7
Its mechanistic targets include various receptors for growth factors and cytokines including vascular endothelial growth factor receptor, platelet-derived growth factor receptor, the stem cell factor receptor, colony-stimulating factor 1 receptor, FMS-like tyrosine kinase-3, and rearranged during transfection receptor tyrosine kinase. 8 –11 Sunitinib targets the adenosine 5′-triphosphate (ATP) binding site of these receptors, and via inhibition, it prohibits cellular signaling and leads to interruption of angiogenesis and proliferation of tumor cells. As a consequence, tumor vascularization reduces and apoptosis of tumor cells is initiated. 9 But the inhibition of these wide range of kinases was considered to be the cause of undesired collateral toxic effects. 12 –15
An increasing number of cardiovascular toxicities (drug-induced cardiac injury) were reported with sunitinib. These serious adverse events such as the development of hypertension and angina pectoris might be resulted with acute ischemic myocardial damage, QT prolongation, symptomatic congestive heart failure, left ventricular systolic dysfunction, and sudden death. 10,11,16 –33 The underlying molecular mechanisms involved in the pathogenesis of these cardiotoxic effects are still unclear, but dependence of cardiomyocytes to aerobic metabolism and ATP was reported as an important factor for cardiotoxicity of sunitinib. 11,34,35 It was determined that being an ATP analog, sunitinib competitively inhibits the ATP binding domain of its target proteins. 36,37 The magnitude of the cardiotoxicity was usually reported to be dose dependent and cumulative. 38
The aim of this study was to explore the potential cardioprotective effects of ATP on sunitinib-induced cardiotoxicity as well as the effects of sunitinib on malondialdehyde (MDA), total glutathione (tGSH), tumor necrosis factor α (TNF-α), and nuclear factor κB (NF-κB) levels in rats’ cardiac tissues and troponin I (Tp-I) levels in rats’ blood samples.
Materials and methods
Animals
In this experiment, a total number of 30 male rats from albino Wistar species weighed between 265 g and 280 g were used. All of the rats were provided from Ataturk University Medical Experimental Practice and Research Center. The animals were sheltered at normal room temperature (22°C) in proper laboratory environment and were fed appropriately.
The protocols and procedures were made according to guidelines for experimental animal procedures and approved by the Atatürk University’s local animal ethics committee (Ethics Committee Number 2018/09 dated August 29, 2018).
Chemical materials
From the drugs used in the experiment, sunitinib (Sutent) was supplied by Pfizer, thiopental sodium (Pental Sodium) was supplied by I.E. ULAGAY (Istanbul, Turkey), and ATP was supplied by Zdorovye Narodu (Kharkiv, Ukraine).
Experiment groups
The rats that were planned to be used in our study were divided into three groups as sunitinib group (SG), sunitinib plus ATP group (SAG), and healthy group (HG).
Experiment procedure
ATP at a dose of 2 mg/kg (0.2 mL/kg) was injected intraperitoneally (ip) to the SAG group (n = 10). This dose was shown to protect ovarian tissue from oxidative ischemia reperfusion injury in a previous study. 39 Same volume normal saline (0.9% NaCl) as solvent was administered ip to the other two groups including SG (n = 10) and HG (n = 10). After 1 h from administration of ATP and 0.9% NaCI, 25 mg/kg sunitinib was applied orally via catheter to stomach in the SAG and SG groups. This procedure was repeated once daily for 5 weeks. Blood samples were collected from the tail vein before the animals were killed. At the end of this period, all animals were killed with high-dose thiopental sodium (50 mg/kg) and their cardiac tissue was removed. MDA, tGSH, TNF-α, and NF-κB levels were evaluated in the cardiac tissues of the animals and Tp-I levels in their blood samples. Histopathological analysis was also performed in cardiac tissues of the animals.
Biochemical analysis
Phosphate-buffered saline solution was used to rinse animal tissues prior to dissection. Tissue homogenization was made in the ice-cold phosphate buffers (50 Mm, pH: 7.4). After homogenization, samples were centrifuged at 5000 r/min for 20 min at 4°C, and in the result of this procedure, the supernatants were extracted for measurements of NF-κB, TNFα, tGSH, and MDA. Tissue protein levels were determined by the method of Bradford. The Bradford assay relies on the binding of the dye Coomassie Blue G250 to protein. Binds to protein has an absorbance maximum at 595 nm. 40 All the results were given by dividing to G-protein. Microplate reader (Bio-Tek, Winooski, Vermont, USA) was used for all spectrophometric measurements.
MDA analysis
Thiobarbituric acid and MDA formed a pink-colored complex. The measurement of the absorbance of this complex (a method by Okhawa et al. 41 ) was used for measurement of MDA. The homogenate sample (25 µL) was added to a solution containing 25 µL of 80 g/L sodium dodecyl sulfate and 1 mL mixture solution (200 g/L acetic acid + 1.5 mL of 8 g/L 2-thiobarbiturate). Firstly, we incubated at 95°C for 1 h. After cooling, 1 mL of n-butanol:pyridine I at the rate of 15:1 was added to the sample. And the sample was vortexed for 1 min and centrifuged at 4000 r/min for 10 min. We measured the absorbance of the supernatant at 532 nm and obtained standard curve using 1,1,3,3-tetramethoxypropane. 41
tGSH analysis
We made tGSH analysis according to the method by Sedlak and Lindsay. 5,5′-dithiobis [2-nitrobenzoic acid] (DTNB) disulfide is reduced easily by sulfhydryl groups. During this reduction, a yellow color is produced, and this is measured by spectrophotometry at 412 nm. For measurement, a solution containing 5.85 mL 100 mM Na phosphate buffer, 2.8 mL 1 mM DTNB, 3.75 mL 1 mM NADPH, and 80 µL 625 U/L glutathione reductase was prepared. 0.1 mL metaphosphoric acid was added to 0.1 mL tissue homogenate and centrifuged at 2000 r/min for 2 min. We added 0.15 mL cocktail solution to 50 µL of this supernatant and obtained the standard using glutathione disulfide. 42
TNF-α and NF-κB analysis
We measured tissue homogenate NF-κB and TNF-α concentrations using enzyme-linked immunosorbent assay Rat NF-κB ELISA immunoassay kits (Cat. No:201-11-0288; SunRed, Shangai LZ, Shangai, China) and Rat TNF-α ELISA kits (Cat. No: YHB1098Ra; Shanghai LZ, Shanghai, China). Instructions of manufacturers were followed for making analyses. Rat-specific NF-κB and TNF-α monoclonal antibodies were coated onto the wells of the microplates. Also tissue homogenate, standards, and specific biotinylated monoclonal antibody and streptavidin-horseradism peroxidase enzyme were pipetted into these wells and then incubated at 37°C for 60 min. Chromogen reagent A and chromogen reagent B were added after washing, which are acted upon by the bound enzyme to produce a color. It was incubated at 37°C for 10 min. The stop solution in which intensity of this colored solution is directly proportional to the concentration of rat NF-κB and TNF-α present in the original specimen was added lastly. The well plates were read at 450 nm. We used standard graphics to calculate the absorbance of the samples.
Tp-I analyses
Tp-I levels in plasma obtained from animals were measured using VIDAS Tp-I Ultra Kit, enzyme-linked fluorescent assay technique. All process of the test was performed automatically with VIDAS machine by prepared test reactants in the kit. The sample was transferred to well containing anticardiac Tp-I antibodies marked with alkaline phosphatase conjugate. Adherence of the antigen to Tp-I attached to the inner wall of solid-phase connector and conjugate was achieved by pulling and releasing the sample conjugate mixture into solid-phase connector. The unbound ingredient was removed by washing. Conjugate enzyme catalysis hydrolyzes of substrate known as 4-methylumbelliferone phosphate to 4-methylumbelliferone, a product that’s fluorescent measured at 450 nm. Density of the fluorescent is proportional to the antigen concentration in the sample.
Histopathological examination
We used 10% formaldehyde solution to fix all of the tissue samples for microscopic examination. After this procedure, samples were washed under tap water in cassettes for 24 h. Conventional grade of alcohol (70%, 80%, 90%, and 100%) was used to remove the remaining water within tissues. After passing through xylol, tissues were embedded in paraffin. We cut 4- to-5-µm sections from the paraffin blocks and hematoxylin–eosin staining was made. Their photos were taken using the Olympus DP2-SAL firmware. A pathologist who was blinded for the study groups made histopathological examinations.
Statistical analysis
The results obtained from experiments were stated as “mean value ± standard error” (x ± SE). We checked distribution by Shapiro–Wilk test. Parameters matched normal distribution. The significance degree of the difference between groups was determined by one-way analysis of variance test. After that Fisher’s post hoc analysis with Tukey’s test was performed. All statistical processes were performed with IBM SPSS Statistics Version 22 program and a probability value of p < 0.05 was considered to indicate statistical significance.
Results
Inflammatory marker results
MDA, tGSH, TNF-α, and NF-κB levels were evaluated in the cardiac tissues of the animals and Tp-I levels in their blood samples (Table 1). MDA, TNF-α, NF-κB, and Tp-I levels were higher in the SG group compared to the SAG and HG groups, and the difference was statistically significant (p < 0.001). tGSH levels of the SG group were lower than the SAG and HG groups, and this difference is also statistically significant with a p value of 0.001. These results suggested that sunitinib had inflammatory effects on the subjects and these effects had important roles on sunitinib-induced cardiotoxicity. Another important finding was the protective effect of ATP on this undesired cardiotoxicity. All inflammatory marker results were similar in the SAG and HG groups supporting protection of ATP (Table 1).
Effect of adenosine triphosphate on sunitinib-induced cardiac injury in rats.a
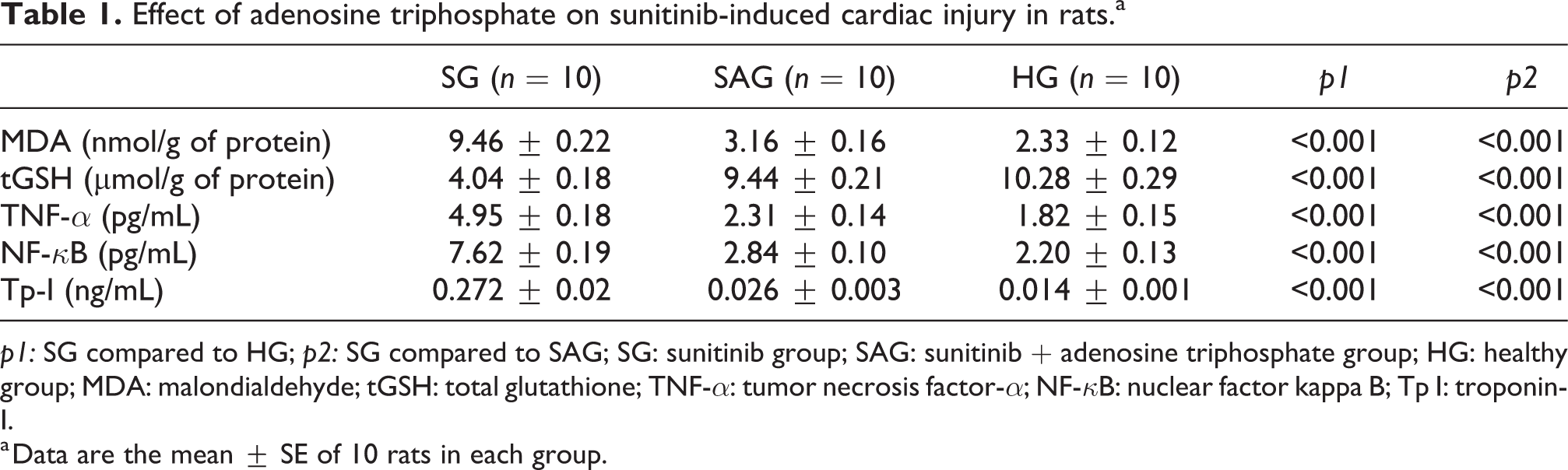
p1: SG compared to HG; p2: SG compared to SAG; SG: sunitinib group; SAG: sunitinib + adenosine triphosphate group; HG: healthy group; MDA: malondialdehyde; tGSH: total glutathione; TNF-α: tumor necrosis factor-α; NF-κB: nuclear factor kappa B; Tp I: troponin-I.
a Data are the mean ± SE of 10 rats in each group.
Histopathological results
According to the conducted microscopic evaluations of cardiac muscle tissue, the structure and morphology of cardiac muscle fibers and blood vessels were normal in the control group (Figure 1(a) and (b)). In the sunitinib group, microscopic examinations showed obvious cardiac muscle tissue damage. Dilated myofibers and locally atrophic myofibers were outstanding across the tissue. Congested blood vessels were observed at the same time (Figure 1(c)). In rats treated with ATP prior to sunitinib, marked amelioration in these findings and normal blood vessels were evidenced (Figure 1(d)).

Hematoxylin–eosin staining in cardiac muscle tissue. (a) Healthy group: →: muscle nuclei; *: blood vessel; >: muscle fiber ×200. (b) Healthy group: →: muscle nuclei; *: normal blood vessel; >: muscle fiber ×200. (c) Sunitinib group: →: muscle nuclei; *: congested blood vessel; >: dilated and atrophic muscle fibers ×100. (d) Sunitinib + adenosine triphosphate group: →: muscle nuclei; *: normal blood vessel; >: muscle fibers ×200.
Discussion
Targeted therapies including TKIs that inhibit molecular pathways have changed the course of many different solid tumors. Sunitinib is one of the most commonly used TKIs and is approved for the treatment of many different cancer types, and research studies are ongoing with sunitinib in various malignancies. 1,2,5 But like other TKIs, sunitinib may lead to drug-induced cardiac toxicity, an undesired adverse effect of this group of drugs. Primary pharmacological effects were defined to be the most important underlying reason of cardiotoxicity because of overlapping of regulatory signaling pathways of tumor growth and survival with cardiac function permanence mechanisms. The most frequent manifestation of cardiotoxicity was reported to be the decrease in left ventricular ejection fraction. 43,44
Over the past few years, many different underlying mechanisms of sunitinib-induced cardiotoxicity were established in various in vivo and in vitro studies. These mechanisms include deterioration of the structure and functions of mitochondria, activation of apoptosis, and depletion of ATP. 33,45,46 Besides determination of these mechanisms, the extent of cardiotoxicity, the effect of cardiotoxicity on prognosis and survival of the patients, and potential cardioprotective agents that could prevent the heart from damage were also defined.
In this present study, we explored the potential cardioprotective effects of ATP on sunitinib-induced cardiotoxicity and also analyzed the effects of sunitinib on MDA, tGSH, TNF-α, and NF-κB levels in the cardiac tissues of the animals and Tp-I levels in their blood samples. We found higher levels of MDA, TNF-α, NF-κB, Tp-I, and lower levels of tGSH with sunitinib administration. These findings showed that sunitinib had inflammatory effects on cardiac tissue of the rats. Similar findings reported in various studies. 28 In two other studies, dose-dependently increased LDH levels were defined with sunitinib administration. 16,47 We observed that addition of ATP to sunitinib reversed these effects in the cardiac tissue samples.
In this study, according to the histopathological analysis of cardiac muscle tissues, the structure and morphology of cardiac muscle fibers and blood vessels were normal in HG (Figure 1(a) and (b)). We determined obvious cardiac muscle tissue damage in SG including dilated myofibers, locally atrophic myofibers, and congested blood vessels (Figure 1(c)). In this study, the pathological specimens of the patients who experienced heart failure due to sunitinib treatment were evaluated. The microscopic findings were determined as hypertrophy in cardiac myocytes and abnormalities in mitochondria of these cells such as swelling, membrane whorls, and effaced cristae. 19 The authors also have reported similar findings in tissues obtained from mice after sunitinib administration. In another study, an increase in the collagen deposits was determined in hearts of rats treated with sunitinib. 28 Also, pro-inflammatory findings were reported in the rats that isolated heart perfused with sunitinib in the same study.
When we evaluated the samples of the rats treated with ATP prior to sunitinib, evident improvement with normal blood vessel features was observed (Figure 1(d)). Thus, we found that cardiotoxic effects of sunitinib were blocked by ATP. Although this finding could be considered to be a new protective way, it is not clear if ATP administration with sunitinib will reduce antitumor efficacy of sunitinib. Various agents evaluated for cardioprotection failed to demonstrate a clinical benefit because of reduction in antitumor efficacy of the primary agent. 48 Contrary to these results, attenuation of sunitinib-induced cardiotoxicity was determined with the A3 adenosine receptor selective agonist IB-MECA without influencing the antitumor efficacy of sunitinib. 49
Conclusion
TKIs and some other biological agents inhibiting kinases maintained an important clinical benefit for cancer patients with added cardiac toxicity. As being a member of TKI class, cardiotoxicity is also a problem of sunitinib treatment. Our results suggest that sunitinib has inflammatory effects on cardiac myocytes, and MDA, TNF-α, NF-κB, and Tp-I may have important role in sunitinib-induced cardiotoxicity. We also found that ATP administration exerts a protective effect against cardiac effects of sunitinib. Future clinical trials evaluating potentially cardioprotective agents against drug-induced cardiotoxicity and less cardiotoxic therapies with more efficient anticancer treatment modalities will ensure patient safety and improve outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study conformed to the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments and was approved by the ethics committee at the University of Seville. The manuscript does not contain clinical studies or patient data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.