
Abstract
Objective:
The objective of this article is to study the correlation between neutrophil gelatinase-associated lipocalin (NGAL) and soluble CD14 subtype (presepsin) on the severity and prognosis evaluation of acute paraquat poisoning (APP) patients.
Materials and methods:
We studied 120 APP patients who were divided into three groups: light (28 cases), moderate (52 cases), and heavy poisoning (40 cases) groups. Twenty healthy volunteers were enrolled as controls.
Results:
Acute kidney injury (AKI) occurred in 86 APP patients (71.7%, 86 of 120). In AKI group, urine NGAL was elevated 3 h after treatment, serum NGAL was elevated 24 h after treatment, and serum creatine (SCr) was elevated 2 days after treatment, which were all significantly higher than non-AKI group. Compared with control group, there were significant differences in presepsin and acute physiology and chronic health status (APACHE) II score of different poisoning groups. There were significant differences in detection indices 24 h, 3 days, and 7 days after treatment among different poisoning groups. There was a positive correlation between urine NGAL and serum paraquat concentration, urine NGAL, and AKI morbidity (r 1 = 0.974, r 2 = 0.766, p < 0.001), suggesting higher urine NGAL level indicated higher AKI morbidity. Receiver operating characteristic curves analysis suggested serum presepsin level and urine NGAL level had higher sensitivity and specificity than APACHE II score when predicting 28-day mortality of APP patients.
Conclusion:
Serum and urine NGAL level is elevated earlier than SCr, which is important for the early diagnosis of APP. Serum presepsin and urine NGAL levels can be used as markers to diagnose the severity of AKI and predict the mortality of APP patients.
Keywords
Introduction
Paraquat (PQ) is a nonselective pyridine herbicide that can affect multiple organs after poisoning. It can lead to multiple organ dysfunctions (MODs) and acute respiratory distress syndrome, and its mortality is more than 70%. 1 Acute paraquat poisoning (APP) usually causes kidney damage. 2 Light poisoning can cause proteinuria and hematuria, and heavy poisoning can lead to renal failure which requires renal-replacement therapy. 3,4 PQ mainly leads to ischemia and toxicity of renal tubular epithelial cells and directly affects prognosis if kidney damage occurs. 5,6 However, effective and objective indicators for judging the condition, efficacy, and prognosis of APP are lacked.
Neutrophil gelatinase-associated lipocalin (NGAL), also called lipocalin 2, is a member of the lipocalin superfamily which is present in neutrophils. The molecular mass of NGAL is 25 kDa and is consisted of 178 amino acids in the form of monomers and homodimers. 7 NGAL, synthesized in renal tubular epithelial cells, is a glycosylation protein that is involved in antibacterial properties, inflammatory response, and apoptosis. 8 When the kidney is damaged, the NGAL level is released in large amounts in the blood and urine. 9 Therefore, it can be used as a marker for early diagnose of acute kidney injury (AKI) after PQ poisoning.
Soluble CD14 subtype (presepsin) is the soluble N-terminal fragment of membrane marker/receptor protein CD14, and can be acted as a marker of sepsis. 10 Recent studies also shown that presepsin can be acted as markers of hemophagocytic syndrome, inflammatory bowel disease, and emergency critically ill disease. 11,12 Our previous report showed that presepsin can be acted as a marker for assessing the severity of APP patients. 13 However, whether it can be used as a marker for judging the severity of AKI and can predict the mortality of APP patients is still not known.
In this study, we detected serum presepsin, serum NGAL, and urine NGAL in APP patients at different time points after treatment, and discussed the clinical value of presepsin and NGAL in assessing the prognosis of APP.
Materials and methods
Patients
This study was approved by the Ethics Committee of Harrison International Peace Hospital Affiliated to Hebei Medical University, and all patients signed informed consent. From May 2015 to October 2018, 120 APP patients (56 males and 64 females) from Harrison International Peace Hospital Affiliated to Hebei Medical University were enrolled in this study. Diagnostic criteria of APP were referred to national occupational health standards “Occupational acute paraquat poisoning diagnosis” (GBZ246-2013). Patients were aged from 18 to 52 years, with an average age of 40.18 ± 8.21 years. AKI was diagnosed by kidney disease improving global outcomes clinical practice guidelines. 14
Inclusion criteria include (1) orally taking poison; (2) the time from poisoning to treatment is less than 3 h; and (3) oral dose 5–100 mL, with an average dose of 30.78 ± 7.65 mL.
Exclusion criteria include (1) other ways of poisoning; (2) APP combined with other drugs such as organic phosphorus; (3) patients who had a history of heart, lung, liver, and kidney diseases; and (4) patient who died within 7 days of hospitalization.
Groups
AKI occurred in 86 APP patients (AKI group), and the rest 34 patients did not have AKI (non-AKI group). Urine PQ levels were detected in all APP patients at admission. Patients were divided into light, moderate, and heavy poisonings according to 2014 Taishan expert consensus: light poisoning (urine PQ level < 10 μg/mL, 28 cases), moderate poisoning (urine PQ level 10–30 μg/mL, 52 cases), and heavy poisoning (urine PQ level > 30 μg/mL, 40 cases). According to the 28-day prognosis, they were divided into survival group (42 cases) and the death group (78 cases). There were no significant differences in sex, age, body mass index (BMI), time of gastric lavage, and addiction among the groups (p > 0.05). Twenty healthy volunteers were enrolled as controls.
Treatments
After admission, all patients were treated with gastric lavage, vomiting, magnesium sulfate, mannitol catharsis, and orally taken kaolin. They underwent high-dose glucocorticoid combined with cyclophosphamide shock therapy. Reduced glutathione and vitamin C were used for antioxidation; Edaravone was used for eliminating oxygen free radicals, proton pump inhibitors for inhibiting acid, and rhubarb-based traditional Chinese medicine detoxification group prescription for detoxification. Conventional treatments were used to maintain water and electrolyte balance, and a large amount of fluid was used to promote metabolism, supplemented by nutritional support. All patients underwent bedside blood perfusion with the JF-800A blood perfusion machine within 2 h after admission for 3 days.
Detection indices
Acute physiology and chronic health status (APACHE) II score and 28-day mortality were recorded from all APP patients. Venous blood (10 mL) and urine (10 mL) were collected from all APP patients before treatment at 3 h, 12 h, 24 h, 2 days, 3 days, 5 days, and 7 days after treatment. Serum and urine NGAL level, serum presepsin level, tumor necrosis factor (TNF)-α level, and interleukin 6 (IL-6) level were detected by enzyme linked immunosorbent assay; serum creatine (SCr) and C-reactive protein (CRP) levels were detected by an automatic biochemical analyzer (Hitachi, Japan). Plasma PQ concentration was detected using liquid chromatograph/mass spectrometer (LC/MS) method.
Statistical analysis
Data were analyzed using SPSS 23.0. The t-test was applied for the comparison of between groups. Correlation analysis was analyzed by the Pearson test. Receiver operating characteristic (ROC) curve was used to evaluate the predictive value of NAGL for AKI and the correlation between blood presepsin, urine NGAL, APACHE II, and 28-day mortality, with p < 0.05 considered statistically significant.
Results
Higher dose of PQ was more likely to cause AKI
As presented in Table 1, there was a significant difference in PQ dose between AKI group and non-AKI group (p < 0.05). There were no significant differences in sex, age, BMI, and systolic pressure between AKI group and non-AKI group (p > 0.05). These results indicated that a higher dose of PQ was more likely to cause AKI.
Comparison of clinical data between AKI group and non-AKI group (

AKI: acute kidney injury; BMI: body mass index.
a p < 0.05 versus non-AKI.
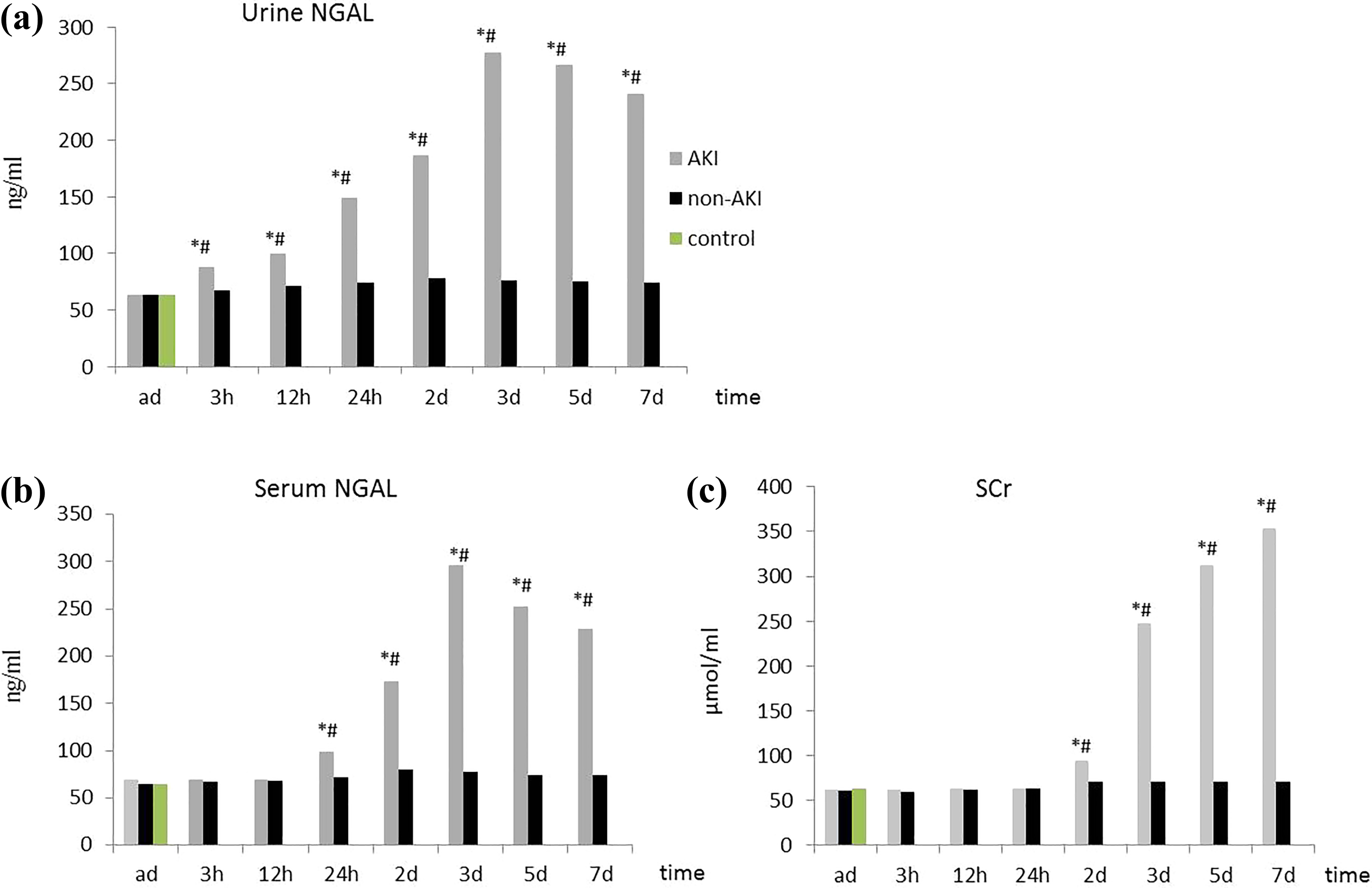
Comparison of serum and urine NGAL level and SCr level between AKI and non-AKI groups at different time points
As presented in Figure 1, there were no significant differences in serum and urine NGAL level and SCr level between AKI group and non-AKI group (p > 0.05) at admission. In AKI group, urine NGAL level was elevated 3 h after treatment, serum NGAL level was elevated 24 h after treatment, and both urine NGAL level and serum NGAL levels reached the highest on third day. There were significant differences in SCr level on second day after treatment between the AKI group and the non-AKI group (p < 0.05).
Comparison of serum and urine NGAL level and SCr level between AKI and non-AKI groups at different time points (
Serum NGAL can be markers to diagnose the severity of AKI in APP patients
ROC curve was used to evaluate the predictive value of serum NAGL, urine NAGL, and SCr for AKI. Twenty-four hours after treatment, blood and urine samples were collected and ROC curve was drawn. The area under urine NGAL curve was 0.886 (95% confidence interval (CI) 0.802–0.969), sensitivity was 74.4%, specificity was 88.2%, and cutoff value was 84.1 ng/mL (Figure 2). The area under serum NGAL curve was 0.807 (95% CI 0.699–0.915), sensitivity was 74.4%, specificity was 88.2%, and cutoff value was 80.0 ng/mL (Figure 2). The area under SCr curve was 0.683 (95% CI 0.545–0.820), sensitivity was 37.2%, specificity was 94.1%, and cutoff value was 77.25 μmol/L (Figure 2). With the prolonging of hospital stay, the kidney injury of APP gradually aggravated, and AUC gradually approaches 1, suggesting that the sensitivity and specificity of serum NGAL are higher than SCr for diagnosing AKI, which can be used for early diagnosis of kidney damage of APP.
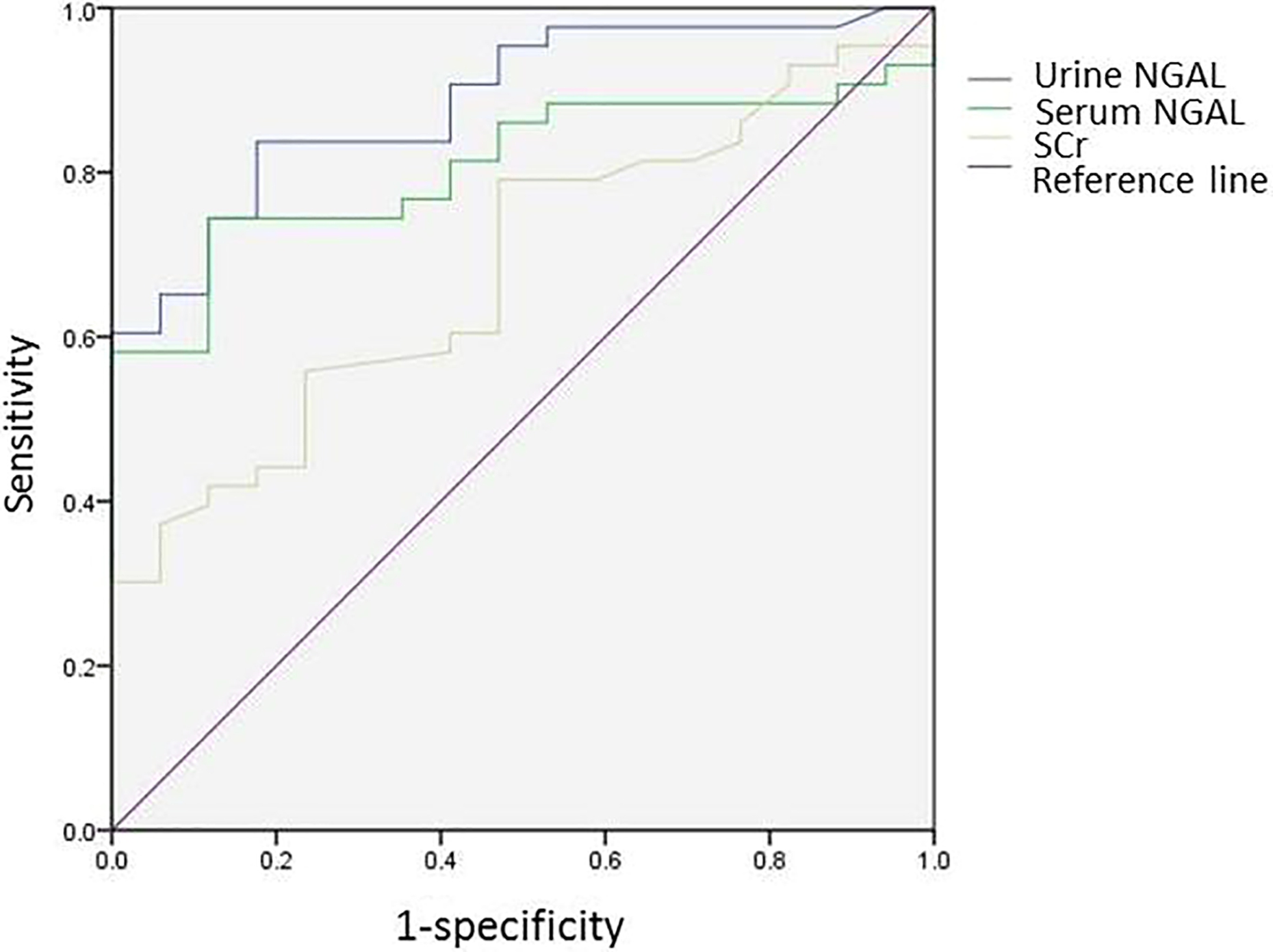
ROC curves of serum NGAL, urine NGAL, and SCr. ROC: receiver operating characteristic; NGAL: neutrophil gelatinase-associated lipocalin; SCr: serum creatine.
Higher urine NGAL level indicated higher AKI morbidity
As shown in Figure 3, there was a positive correlation between urine NGAL and serum PQ concentration, urine NGAL, and AKI morbidity (r 1 = 0.974, r 2 = 0.766, p < 0.001), indicating that the higher urine NGAL level, the higher AKI morbidity.

Correlation of urine NGAL level and PQ concentration. The concentration of PQ and NGAL were analyzed. NGAL: neutrophil gelatinase-associated lipocalin; PQ: paraquat.
Comparison of detection indices among poisoning groups
There was significant difference in initial value of serum presepsin between control group and different poisoning groups (p < 0.05), while there was no significant difference in the initial value of other detection indices between control group and different poisoning groups (p > 0.05) (Figure 4). At other time points (24 h, 3 days, and 7 days), there were significant differences in serum presepsin level, urine NGAL level, TNF-α level, CRP, IL-6 level, and APACHE Ⅱ score among light poisoning group, moderate poisoning group, and heavy poisoning group (p < 0.05). The morbidity of light poisoning group, moderate poisoning group, and heavy poisoning group was 21.43%, 71.15%, and 87.50%, respectively (Figure 4).

Comparison of detection indices among poisoning groups (
Comparison of detection indices between the survival group and the death group
As shown in Figure 5, there were significant differences in initial values of presepsin level and APACHE II score between the survival group and the death group (p < 0.05), while there were no significant differences in initial values of other detection indices between the survival group and the death group (p > 0.05). Twenty-four hours after treatment, there were significant differences in presepsin level, urine NGAL, TNF-α level, CRP, IL-6 level, and APACHE II score between the survival group and the death group (p < 0.05). The levels of presepsin and urine NGAL increased continually in the death group, while gradually decreased in the survival group (Figure 5).
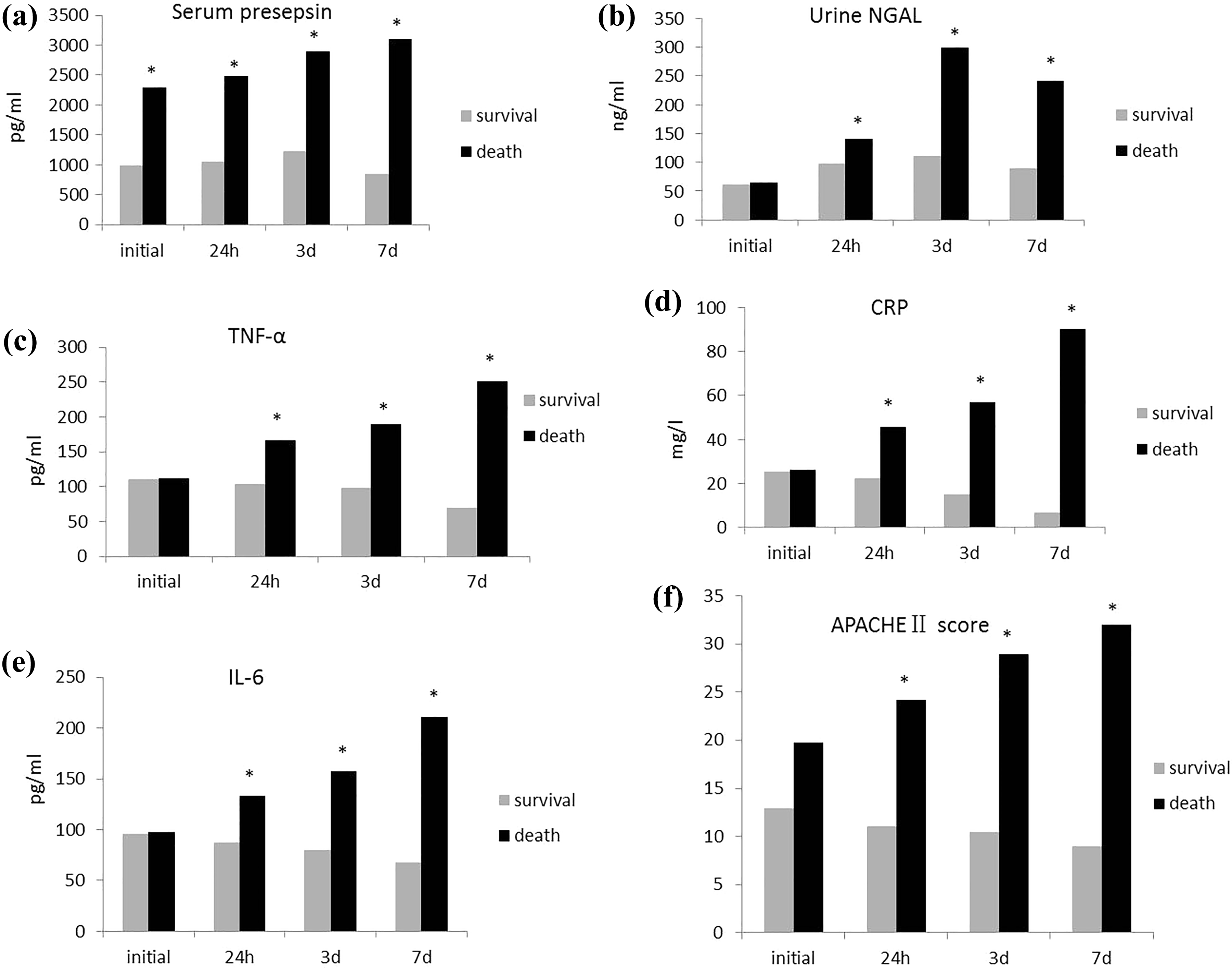
Comparison of detection indices between survival group and death group (
Comparison of predictive ability of serum presepsin level and urine NGAL level in 28-day mortality of APP patients
As shown in Table 2 and Figure 6, predictive ability of serum presepsin level at admission and urine NGAL level at 3 h after treatment in 28-day mortality of APP patients was higher than APACHE II score. The predictive ability of serum presepsin level was higher than urine NGAL level. The sensitivity was serum presepsin level > urine NGAL level > APACHE II score. The specificity was urine NGAL level > serum presepsin level > APACHE II score (p < 0.05).

ROC curves of serum presepsin level, urine NGAL level, and APACHE II score in 28-day mortality of APP patients. ROC: receiver operating characteristic; presepsin: soluble CD14 subtype; NGAL: neutrophil gelatinase-associated lipocalin; APACHE II score: acute physiology and chronic health status II score; APP: acute paraquat poisoning.
Comparison of predictive ability of serum presepsin level at admission and urine NGAL level at 3 h after treatment in 28-day mortality of APP patients.

NGAL: neutrophil gelatinase-associated lipocalin; APP: acute paraquat poisoning; AUC: area under the curve; presepsin: soluble CD14 subtype; APACHE II score: acute physiology and chronic health status II score; CI: confidence interval.
Discussion
Orally taking PQ reaches the peak plasma concentration at 0.5–4 h with a lethal dose of 2–6 g and can be distributed in multiple organs throughout the body at 2 h after absorption in the gastrointestinal tract. 15 The concentration of PQ in the kidney is the highest on early stage, and renal excretion is the main route of excretion of PQ. When the function of kidney is impaired, the clearance rate of PQ can be reduced by 10–20 times. The incidence of AKI can be high to 50%, and 30% of APP patients can be developed into renal failure. 16 Currently, the prognosis is often diagnosed according to the dose of PQ and the early treatment time. For patients who took a large dose of PQ, they died because of pulmonary edema, pulmonary hemorrhage, and acute renal failure within 1–3 days. For patients who did not take a large dose of PQ, they had dyspnea on seventh day after poisoning and died because of respiratory failure at 2–3 weeks. 17 The mortality of APP patients increased with the increase of PQ dose, but there were still surviving patients with the dose > 100 mL. There were many death cases with very small doses. However, the underlying causes of deaths are still not clear, which may be related to individual differences, drug concentration, drug efficacy, and inaccurate description of PQ dose. Therefore, it is important to find early indicators that can objectively and effectively evaluate the prognosis of APP patients.
Presepsin is a glycoprotein that mediates the pathophysiological effects of lipopolysaccharide and activates macrophages to trigger an inflammatory cascade. 18,19 In healthy people, the concentration of presepsin is very low. Presepsin is often induced by bacteria-released endotoxin, which can activate mitogen-activated protein kinase and tyrosine protein kinase, trigger inflammatory response, and activate fibrinolysis/coagulation systems, resulting in septic shock, MODs, and diffuse intravascular coagulation. 20,21 Studies have shown that presepsin could evaluate the prognosis of septic patients, and be used as an effective indicator for early diagnosis of septic patients, 22 so early intervention to improve survival rate has been widely used in clinical practice. Our previous report also studied the correlation of presepsin and PQ poisoning. 13 The lower serum presepsin level, the higher survival rate, and serum presepsin level were negatively correlated with the survival rate of APP patients. In this study, we found that serum presepsin was elevated at admission, while the other detection indices were changed 24 h after treatment. Serum presepsin was positively correlated with the severity of AKI, which can be a marker for the diagnosis of APP severity.
NGAL is a secreted protein widely expressed in neutrophils, which plays an important role in systemic inflammation, antioxidant stress, and myocardial infarction. 23 –25 NGAL is closely related to kidney injury, and NGAL level is helpful for the early diagnosis of AKI. 26 –28 It can induce the apoptosis of neutrophils in the tubulointerstitial and prevent the damage of kidney tissue from inflammatory cells. 29 Under normal circumstances, NGAL is expressed at very low levels, but when renal tubular epithelial cells are damaged by inflammatory response, the kidney tubules will secrete large amounts of NGAL. 30 In this study, we found that there was a positive correlation between urine NGAL and serum PQ concentration, urine NGAL, and AKI morbidity, indicating that the higher urine NGAL level, the higher AKI morbidity. ROC curves analysis suggested that serum NGAL level and urine NGAL level had higher sensitivity and specificity than SCr in diagnosing AKI, indicating that NGAL can be used for early diagnosis of kidney injury of APP patients. In addition, urine NGAL level can be elevated 3 h after treatment, while the elevation time of serum NGAL level was later than urine NGAL, so urine NGAL is preferred to monitor renal function. Currently, APP patients need to adjust blood purification program and drug dose on the third day after poisoning if they refer to traditional indicators. But if urine NGAL is used as indicator, the treatment method can be adjusted on the first day, which is meaningful for early diagnose.
In conclusion, NGAL has higher sensitivity and specificity in diagnosing AKI, and urine NGAL is more sensitive than serum NGAL, which can be used as a marker to diagnose the severity of AKI at early period and predict the prognosis of APP patients. Serum presepsin and urine NGAL levels can be used as markers to diagnose the severity of APP, which is meaningful for adjusting the therapeutic regimen.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Hebei Provincial Science and Technology Projects (162777109D).