
Abstract
Worsening renal function and azotemia in patients with heart failure (HF) are strongly associated with disease severity and poor prognosis. Increasing interest in this correlation led to the description and classification of cardiorenal syndrome (CRS). We evaluated the role of neutrophil gelatinase–associated lipocalin (NGAL) in the early detection of CRS in dogs with HF. Ten healthy dogs and 31 dogs admitted with HF were included in our study. NGAL and troponin-I were measured on samples collected on the day of admission; creatinine was measured on admission and again on day 7. The CRS group was defined as subsequently developing renal azotemia. Of 31 dogs with HF, 20 were included in the HF group, and 11 were included in the CRS group. The admission NGAL concentrations of the CRS group were significantly higher than those of other groups (p < 0.001). The severity of HF evaluation based on the modified New York Heart Association classification showed significant correlation with NGAL (p < 0.001) and troponin-I (p = 0.009) concentration. However, only serum NGAL concentration at admission was significantly associated with the development of CRS in dogs with HF (p = 0.021). The admission serum NGAL ≥ 16.0 ng/mL (optimal cutoff value) had a sensitivity of 90.9% and specificity of 90.0% in predicting the development of CRS.
Introduction
The heart and kidneys are interrelated organs, and their interactions are involved in the regulation of blood pressure, vascular tone, diuresis, intravascular volume homeostasis, and hemodynamic stability.3,5,28 Worsening renal function and azotemia in patients with heart failure (HF) are significantly associated with disease severity and poor prognosis.16,18 Increasing interest in this correlation has led to the description and classification of cardiorenal syndrome (CRS). The broad term CRS refers to a complex pathophysiologic disorder of the heart and kidneys in which acute or chronic dysfunction of one of these organs may lead to acute or chronic dysfunction of the other.23,24 In human medicine, CRS has been classified into 5 subtypes according to the time course of interaction and the primary organ; patients with acute HF whose renal function worsens are classified as having type 1 cardiorenal syndrome. 2
Neutrophil gelatinase–associated lipocalin (NGAL), also called lipocalin 2 or lcn2, is a glycoprotein that is synthesized in the bone marrow during granulocyte maturation.2,10,19 Although NGAL was initially found in activated neutrophils, many other cells, including epithelial cells of the renal tubules, colon, liver, and lungs, may produce NGAL. 26 NGAL is markedly released during injury of these cells, and its concentration is significantly elevated by epithelial damage. Many human studies suggest that NGAL could be a novel biomarker for identifying renal injury earlier than creatinine.1,2 Accordingly, earlier prediction of renal dysfunction associated with worsening HF is the principal strategy for improved prognosis, and elevated NGAL may predict CRS development.1,2,7,14,22
In veterinary medicine, elevated urine or serum NGAL concentrations occur in acute kidney injury or chronic kidney disease in dogs.8,15,25 However, the relationship between NGAL and renal dysfunction in cardiovascular disease, especially valvular disease, has not been reported in dogs, to our knowledge. We assessed serum NGAL in dogs with HF caused by degenerative valvular disease to determine the usefulness of NGAL as an early marker of CRS in HF dogs.
Materials and methods
Animals
Dogs admitted for HF caused by degenerative valve disease between January 2014 and August 2015 were prospectively enrolled. Our study was approved by the Institutional Animal Care and Use Committee. Congestive HF signs and physical examinations as well as hematologic, radiographic, and echocardiographic examinations were performed for diagnosis of HF. Dogs with HF were categorized in accordance with the modified New York Heart Association (NYHA) functional classification on the basis of a clinical examination. 4 Dogs were eligible whether acute HF was diagnosed for the first time, or deterioration of chronic HF signs was observed with a rise in at least one modified NYHA class.
Dogs with anemia, inflammatory disease, infectious disease, neoplasia, and other systemic diseases including neurologic, adrenal, thyroid, and hepatobiliary disease were excluded. Dogs that had been administered nephrotoxic drugs, including aminoglycoside, and dogs that did not satisfy all inclusion criteria were also excluded from the study.
Among the HF dogs, the cases in which renal dysfunction occurred within the first 7 d from admission, including dogs without azotemia on presentation but later development of renal dysfunction, were classified as belonging to the CRS group. Renal dysfunction in dogs with CRS was defined as a serum creatinine concentration >140 µmol/L (1.6 mg/dL), according to the International Renal Interest Society acute kidney injury criteria. 25 If azotemia resolved within 24 h of correction of pre-renal factors by fluid therapy and/or water supplementation, the dog was considered to have been in a pre-renal azotemic state and was excluded from the study. Healthy dogs with no history of cardiopulmonary and other disease, and with normal hematologic, radiographic, and echocardiographic evaluations, were enrolled as the control group.
Cardiovascular assessment
Physical examinations included body weight, body condition score (1–5 scale), body temperature, heart rate, respiratory rate, murmurs with a point of maximum intensity, and systolic blood pressure (SBP). The SBP results were obtained using the indirect method with an oscillometer (Cardell 9401 blood pressure monitor, Sharn Veterinary, Tampa, FL). Right lateral and ventrodorsal thoracic radiography (Digital X-ray, TATIN 200M, Comed Medical Systems, Seoul, South Korea) and echocardiography (Prosound alpha 6, HITACHI Aloka Medical, Tokyo, Japan) were performed to evaluate cardiac state and function. On radiographic assessment, lung field, presence of cardiomegaly (vertebral heart scale), dilation of the pulmonary artery and vein, and tracheal elevation were examined. Echocardiographic assessment included cardiac remodeling, valvular degeneration, fractional shortening, ejection fraction, and left atrium-to-aorta ratio (La:Ao).
Sample collection and laboratory assessment
A complete blood cell count (VetScan HM2 hematology system, Abaxis, Union City, CA); serum chemistry (Cobas C III instrument, Roche Diagnostics, San Francisco, CA), including urea and creatinine; and electrolyte analysis (9180 electrolyte analyzer, Roche Diagnostics) were performed for evaluation of the general condition of patients.
For NGAL evaluation, venous blood samples on admission were placed into serum separation tubes, and the serum was promptly separated in a refrigerated centrifuge (15 min at 1,500 × g). The samples were then stored up to 6 mo at −70°C until assayed.
Serum NGAL concentration was determined using a commercial canine NGAL sandwich ELISA (Dog NGAL ELISA kit 043, Bioporto Diagnostics, Denmark), according to the manufacturer’s instructions. The concentration of NGAL was determined by measuring the absorbance of the solution at 450 nm using a plate reader and calculating from a standard curve using curve-fitting software (Softmax Pro 5.0, Molecular Devices, Sunnyvale, CA).
Serum troponin-I concentration was evaluated by a commercial laboratory (Sam-kwang Medical Laboratories, Seoul, South Korea) using a chemiluminescence immunoassay (UniCel DXI, Beckman Coulter, Carlsbad, CA).
Statistical analyses
Data analysis was performed using commercial software (SPSS 22.0, SPSS, Chicago, IL). The normal distribution of data was analyzed using the Kolmogorov–Smirnov test. Data were presented as mean with standard deviation, or proportions and frequencies, as appropriate. The chi-squared independence test (χ2 test) was used to compare categorical variables. ANOVA and independent 2-sample t-test were used to compare normally distributed continuous variables. The Wilcoxon signed-rank test was used to compare NGAL concentrations in dogs with CRS before and after an abrupt increase in serum creatinine concentrations. The correlation between NGAL and other variables among study groups was evaluated by a Pearson correlation test. A receiver operating characteristic (ROC) curve was used to determine the cutoff values of NGAL that gave the best sensitivity and specificity for the early prediction of CRS.
Results
In total, 10 healthy dogs and 33 dogs with HF caused by degenerative valvular disease were enrolled. Two dogs diagnosed as having pre-renal azotemia were excluded from further analyses. Among the 31 remaining HF dogs, the cases in which renal dysfunction (serum creatinine concentration > 140 µmol/L) occurred within the first 7 d of admission were classified as belonging to the CRS group (n = 11). Other HF dogs remained in the HF group (n = 20). Dogs in the control group were significantly younger than dogs in the HF and CRS groups (p < 0.001; Table 1). Dogs in the CRS group had significantly higher respiratory rate (p = 0.028) than dogs in the HF group. No statistical difference was found between the HF and CRS groups for other parameters, including body weight, modified NYHA class, heart rate, SBP, vertebral heart scale, fractional shortening, ejection fraction, and La:Ao ratio.
Clinical characteristics of control, heart failure, and cardiorenal syndrome dogs upon admission.
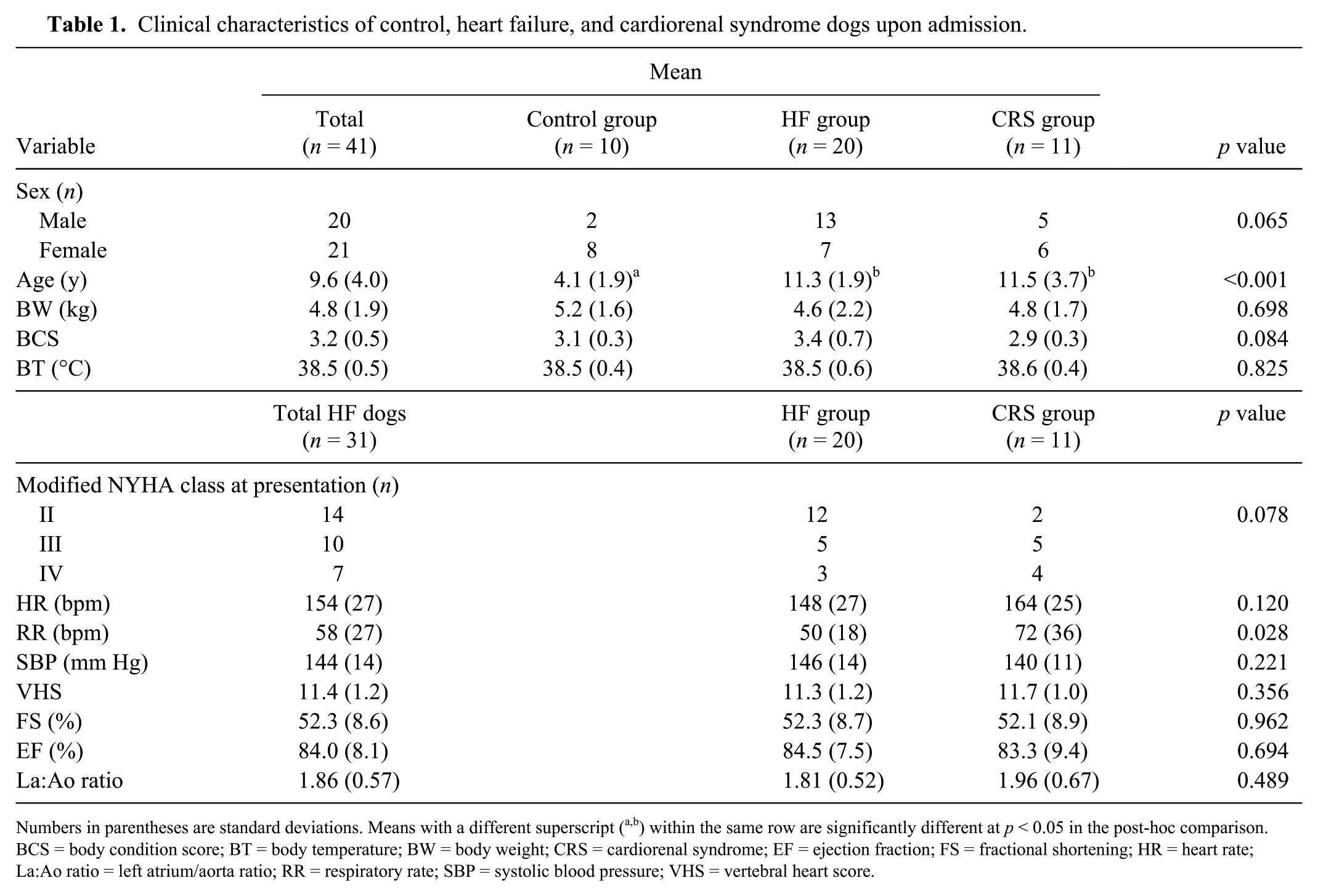
Numbers in parentheses are standard deviations. Means with a different superscript (a,b) within the same row are significantly different at p < 0.05 in the post-hoc comparison. BCS = body condition score; BT = body temperature; BW = body weight; CRS = cardiorenal syndrome; EF = ejection fraction; FS = fractional shortening; HR = heart rate; La:Ao ratio = left atrium/aorta ratio; RR = respiratory rate; SBP = systolic blood pressure; VHS = vertebral heart score.
Serum urea and creatinine were significantly different among the 3 groups (p = 0.003; Table 2). The control group had lower urea and creatinine concentrations than HF and CRS groups, even if those test results were within the reference interval. Serum urea and creatinine values between the HF and CRS groups at the time of admission did not differ (p > 0.05).
Comparison of hematologic and serum biochemical data between control, heart failure, and cardiorenal syndrome dogs upon admission.
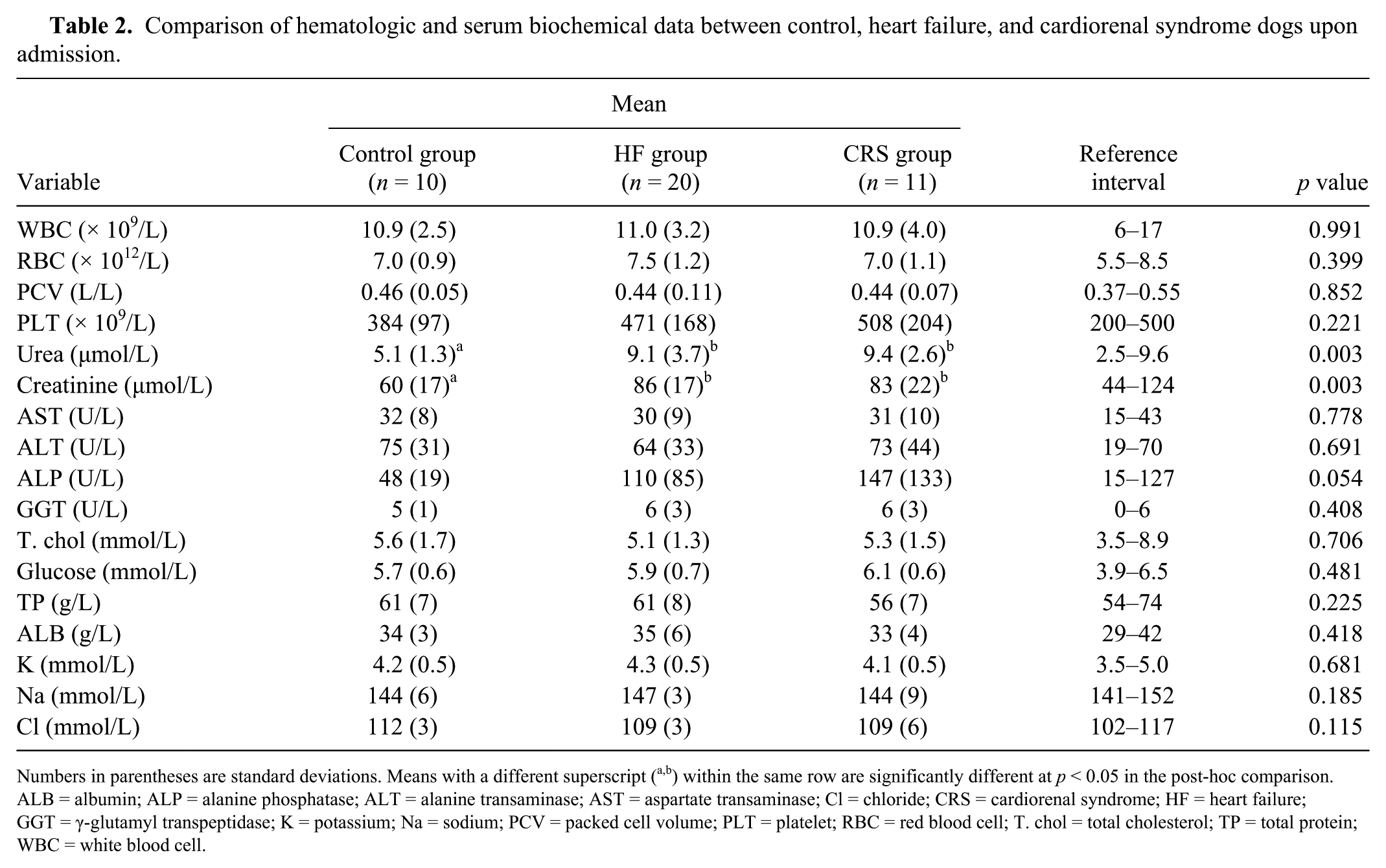
Numbers in parentheses are standard deviations. Means with a different superscript (a,b) within the same row are significantly different at p < 0.05 in the post-hoc comparison. ALB = albumin; ALP = alanine phosphatase; ALT = alanine transaminase; AST = aspartate transaminase; Cl = chloride; CRS = cardiorenal syndrome; HF = heart failure; GGT = γ-glutamyl transpeptidase; K = potassium; Na = sodium; PCV = packed cell volume; PLT = platelet; RBC = red blood cell; T. chol = total cholesterol; TP = total protein; WBC = white blood cell.
There was a statistically significant difference of serum NGAL concentrations among the control, HF, and CRS groups (mean ± standard deviation; 5.9 ± 1.7 ng/mL, 10.9 ± 3.8 ng/mL, and 30.4 ± 16.6 ng/mL, respectively; p < 0.001; Fig. 1). In addition, a post-hoc multiple comparison test revealed that the on-admission NGAL values of the CRS group were significantly higher than those of the control and HF groups. In comparison, troponin-I concentrations at admission were not significantly different among the control, HF, and CRS groups (0.02 ± 0.01 ng/mL, 0.24 ± 0.33 ng/mL, and 0.26 ± 0.15 ng/mL, respectively; p > 0.05; Fig. 1). Furthermore, serum NGAL concentrations the day after azotemia occurred were significantly higher than serum NGAL concentrations on admission (30.4 ± 16.6 ng/mL and 34.0 ± 17.8 ng/mL, respectively; p = 0.021).
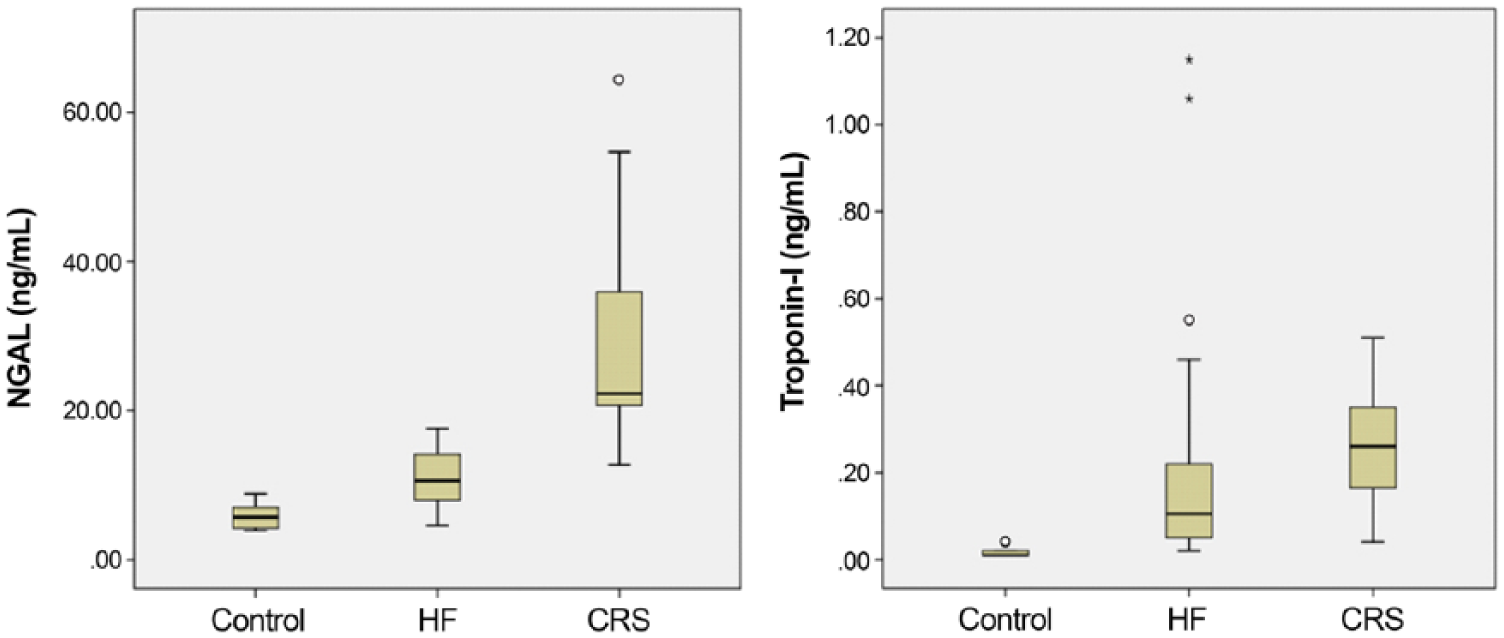
Box plots of neutrophil gelatinase–associated lipocalin (NGAL) and troponin-I concentrations on admission in the control (n = 10), heart failure (HF; n = 20), and cardiorenal syndrome (CRS; n = 11) groups.
On admission, 31 dogs with HF caused by degenerative valvular disease were classified based on the modified NYHA functional classification (Table 3). There was a gradual increase and significant difference in NGAL concentrations with HF severity (p < 0.001). In the post-hoc multiple comparison test, modified NYHA classes III and IV dogs had significantly higher NGAL concentrations than the control group. The NGAL concentrations of the modified NYHA class IV group were significantly higher than those of the modified NYHA class II and control groups. Serum troponin-I concentrations were also significantly different among the control and modified NYHA class II, III, and IV groups. In the post-hoc comparison test, only the modified NYHA class III group had significantly higher troponin-I concentrations than the control group.
Neutrophil gelatinase–associated lipocalin (NGAL) and troponin-I concentrations based on modified New York Heart Association (NYHA) functional classification.
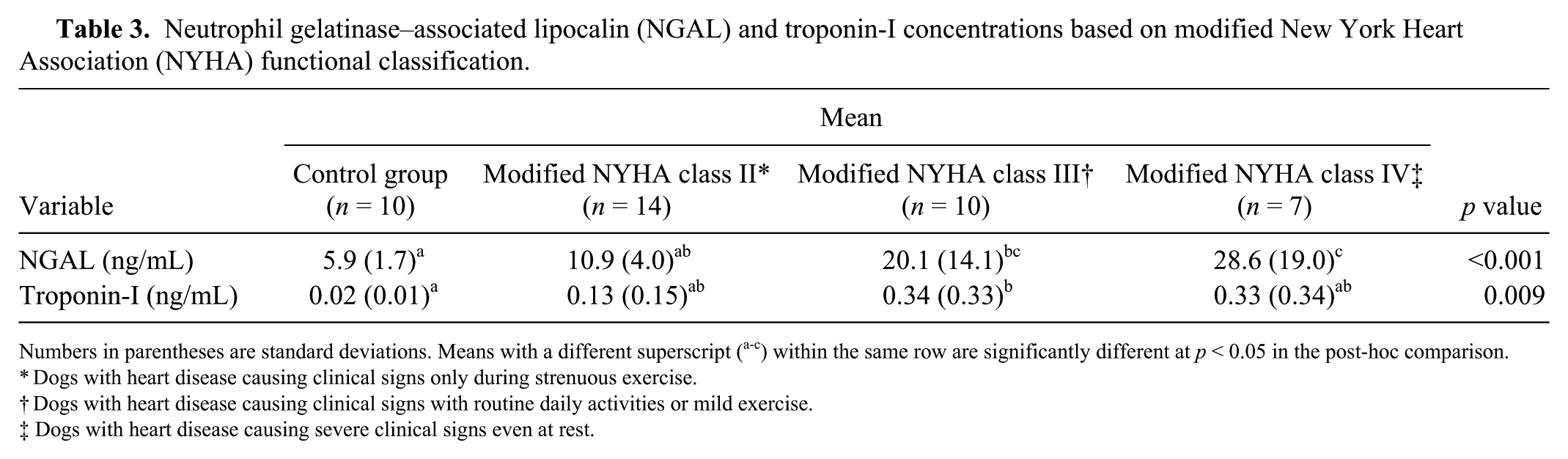
Numbers in parentheses are standard deviations. Means with a different superscript (a-c) within the same row are significantly different at p < 0.05 in the post-hoc comparison.
Dogs with heart disease causing clinical signs only during strenuous exercise.
Dogs with heart disease causing clinical signs with routine daily activities or mild exercise.
Dogs with heart disease causing severe clinical signs even at rest.
A strong positive correlation between serum NGAL concentrations and La:Ao ratio was found (r = 0.540; p < 0.001; Table 4). No significant correlations were found between NGAL concentrations and serum creatinine or troponin-I. The troponin-I concentration was found to be positively correlated with SBP (r = 0.468; p < 0.01) and La:Ao ratio (r = 0.527; p < 0.001).
Correlation of neutrophil gelatinase–associated lipocalin (NGAL) and troponin-I with select biochemical analytes and clinical factors in dogs with heart failure and cardiorenal syndrome.
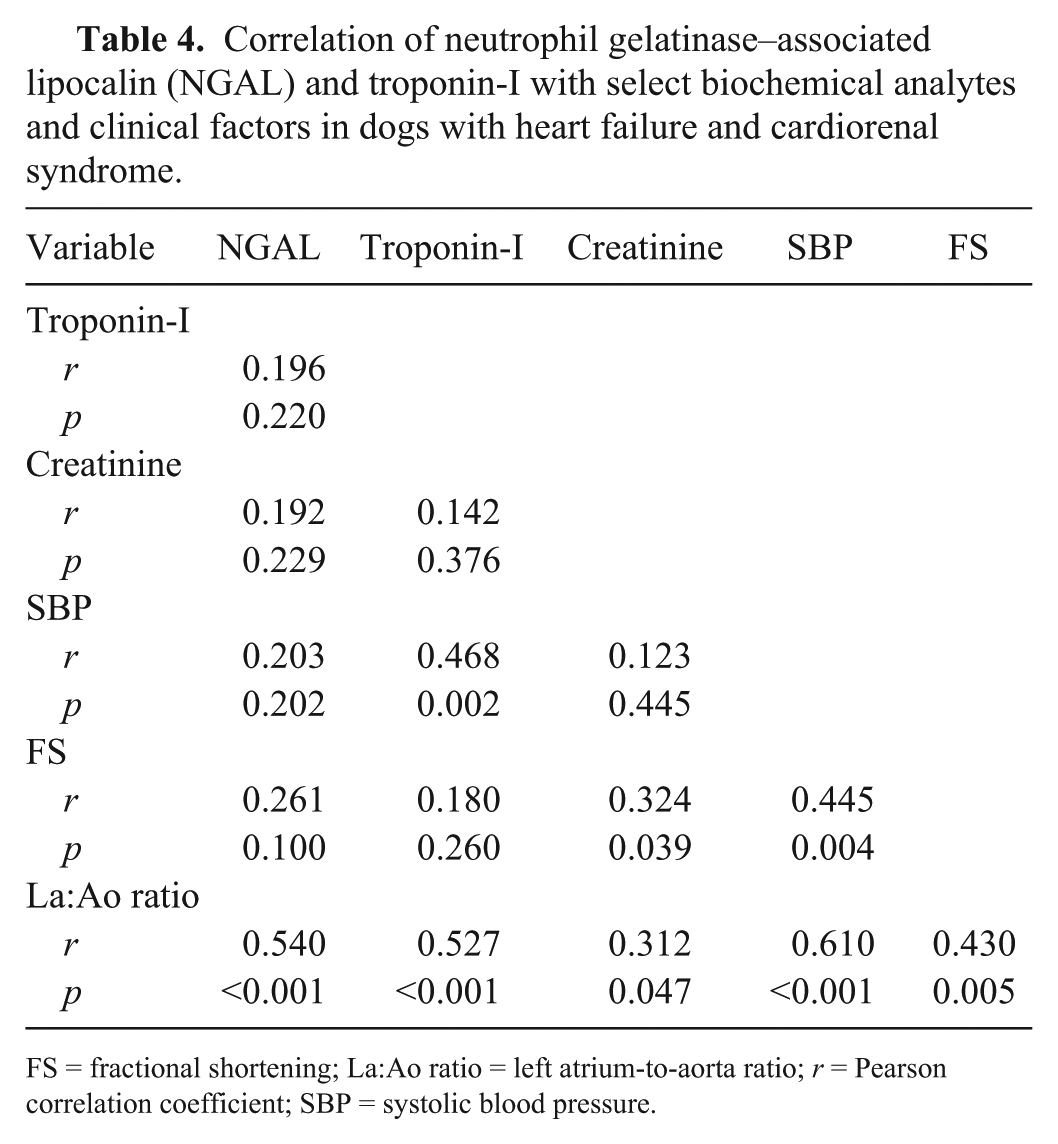
FS = fractional shortening; La:Ao ratio = left atrium-to-aorta ratio; r = Pearson correlation coefficient; SBP = systolic blood pressure.
ROC analysis showed that serum NGAL showed good predictive value, describing an area under the curve (AUC) of 0.96 (95% confidence interval: 0.90–1.00, p < 0.001) with an optimal cutoff value of 16.0 ng/mL (sensitivity 90.9%, specificity 90%). The positive and negative likelihood ratios for NGAL were calculated as 9.09 and 0.10, respectively. Furthermore, the optimal cutoff value for NGAL of 16.0 ng/mL had a positive predictive value of 83.3% and negative predictive value of 94.7% (Fig. 2).
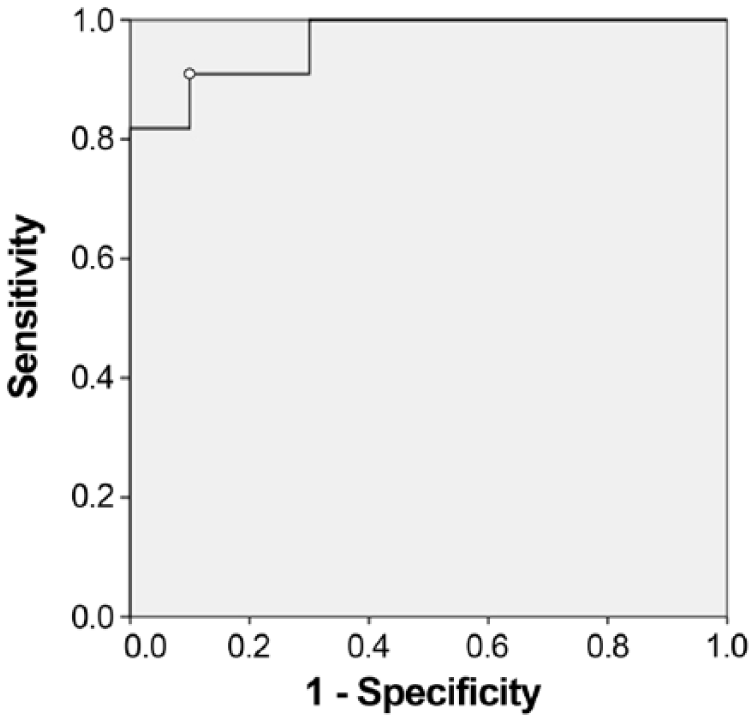
Receiver operating characteristics curve analysis of on-admission neutrophil gelatinase–associated lipocalin (NGAL) for predicting the development of cardiorenal syndrome in dogs with heart failure. The area under the curve is 0.96 (95% confidence interval: 0.90–1.00; p < 0.001). The cutoff value for NGAL was >16.0 ng/mL, with sensitivity and specificity of 90.9% and 90.0%, respectively.
Discussion
In our study, serum NGAL concentrations became elevated before serum creatinine increased in the CRS group within 7 d of admission. On-admission creatinine concentrations in dogs that would subsequently develop CRS were not significantly different from those in dogs without CRS. A previous study of acute kidney injury in dogs also demonstrated NGAL elevation preceding the increase in creatinine. 21 In a study using a canine model of gentamicin-induced nephrotoxicity, NGAL and serum creatinine were found to increase significantly on days 3 and 10, respectively. 15 Several studies in human medicine also demonstrated that the rise in NGAL occurs 24–48 h before the serum creatinine increase.9,13 The earlier detection of NGAL elevation compared with serum creatinine can be explained by the mechanisms underlying elevations of these biomarkers. Serum creatinine concentrations are not altered until at least 75% of the total nephron function has been lost. 6 An increased NGAL concentration suggests tubular injury, which precedes renal functional loss by several days; increased serum creatinine suggests subsequent loss of renal excretory function. 12 Because the tubule is more susceptible to decreased perfusion and hypoxic damage as a result of HF, it is possible that the tubule can be injured while the renal cortex remains intact, maintaining the glomerular filtration rate (GFR). 29 In addition, renal blood flow can decrease by 30–40% without apparently affecting the GFR. Taken together, these factors make tubular markers, such as NGAL, more sensitive than creatinine. 29 Therefore, our findings suggest that the presence of CRS, undetectable with routine examinations in HF dogs, can be predicted by elevated on-admission NGAL concentrations.
Troponin-I is a useful ancillary tool for diagnosis of heart disease and evaluating HF severity in dogs. 27 In humans, troponin-I is known to be one of the most cardiac-specific biomarkers, although its concentration may also increase in some patients with renal insufficiency.11,17 In our study, dogs that developed CRS had higher concentrations of NGAL and troponin-I than dogs who did not develop the condition; however, troponin-I performed worse for predicting CRS than did NGAL. Only the NYHA class III group had significantly higher troponin-I levels than the control group. Troponin-I is a cardiac-specific biomarker, as suggested in previous studies11,17; NGAL is a tubular injury marker.12,29 Therefore, NGAL is more useful than troponin-I for predicting CRS.
The modified NYHA functional classification is clinically useful to categorize HF severity based on clinical signs and physical activity. 4 In our study, a significant relationship was found between serum NGAL concentrations and HF severity (p < 0.001). These results suggested that increased HF severity was associated with renal tubular injury. These findings are in agreement with previous studies in dogs and humans, which demonstrated that renal impairment increases with the severity of HF.20,22
In our study, the La:Ao ratio showed significant correlation with NGAL and troponin-I, representing renal tubular injury and cardiac damage, respectively. This is in accord with a previous study in which the La:Ao ratio was positively correlated with the severity of HF and development of renal dysfunction. 20
One major limitation of our study is that many factors (e.g., types of drugs, duration of drug use, renal function of the dog prior to admission, etc.) that may have contributed to the development of CRS were unknown. Urine samples were not collected routinely from HF dogs in our study; therefore, we did not evaluate urine NGAL, which is known to be a valuable renal biomarker. Additionally, survival time and mortality analysis are required to assess the prognostic value of NGAL in dogs with HF. Such data should be evaluated in future studies. Study of additional cases is necessary to enable standardization of an optimal cutoff value for predicting the development of CRS in dogs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.