
Abstract
Objective:
The aim of our study is to determine whether there is a change in the plasma levels of copeptin and there is a relationship among the plasma levels of carboxyhemoglobin (COHb), lactate, and copeptin levels in patients presenting to the emergency department with carbon monoxide (CO) poisoning.
Methods:
Fifty-seven patients admitted to the emergency department with CO poisoning were included in the study. The blood samples of the patients were collected on arrival 0th, 6th, and 12th hours for copeptin, lactate, and COHb levels. Data were analyzed using SPSS-17 statistical software.
Results:
Arrival serum copeptin levels of the patients were compared to copeptin levels of healthy individuals and a statistically significant difference was found between them (p = 0.008). There was a statistically significant difference between the arrival levels of copeptin and 6th-hour (p = 0.006) and 12th-hour (p = 0.001) levels of copeptin. There was no significant difference between 6th-hour and 12th-hour copeptin levels (p = 0.51). In terms of serum lactate levels, there was a significant difference between arrival and 6th h (p < 0.001), arrival and 12th h (p < 0.001), and 6th and 12th h (p < 0.001). Likewise, in terms of serum COHb levels, there was a significant difference between arrival and 6th h (p < 0.001), arrival and 12th h (p < 0.001), and 6th and 12th h (p < 0.001). There was a positive correlation between COHb and lactate levels on arrival (r = 0.52; p = 0.001).
Conclusion:
Copeptin as a stress hormone can be used in the diagnosis and monitoring of patients with CO poisoning. However, the copeptin level was not superior to COHb and lactate levels.
Introduction
Carbon monoxide (CO) poisoning is still a significant cause of morbidity and mortality all around the world. Every year, especially in the fall and winter seasons, thousands of people die due to CO poisoning. CO shows its toxic effect with several mechanisms. The most important of these is tissue hypoxia. It shows this effect when binding to the respiratory pigments such as hemoglobin and myoglobin and binding to some enzymes that are present in inoxidative processes. Elevated serum lactate level is detected in CO poisoning in addition to ischemia.
Copeptin, the C-terminal portion of pro-vasopressin, is a glycosylated polypeptide comprising 39 amino acids and containing a leucine-rich core segment. Copeptin is released concomitantly with the hypothalamic hormone vasopressin from the hypothalamus. Since uncleaved progine is part of arginine vasopressin (AVP) and occurs evenly to AVP, it can be used as an indirect marker for AVP. AVP and copeptin are secreted upon hemodynamic or osmotic stimuli. AVP is also involved in the endocrine stress response. Copeptin may remain stable for days in circulation compared to AVP, but its function is unclear. Release of copeptin increases with stress response, and there is a strong association between the level of copeptin and severity of illness. 1,2 Copeptin has been shown to be useful in the diagnosis and prognosis of many diseases such as respiratory tract infection, cardiac insufficiency, multiple organ failure, and hemorrhagic and septic shock. 2 –6 There are also studies that show the association between copeptin level and subarachnoid hemorrhage, traumatic brain injury, and ischemic stroke. 7 –9 But there is limited data on serum copeptin level and CO poisoning. Copeptin results are available within 1 h, which is crucial for any useful biomarker in the emergency department setting. 2
As a product of anaerobic glycolysis, lactic acid is related to insufficent oxygen supply, and it may be used as a prognostic parameter for the patients with CO poisoning. There are also studies which concluded that serum lactate level can be used as a prognostic biomarker in CO poisoning. 10,11
The main purpose of our study was to investigate whether there is any difference in serum levels of copeptin in patients admitted to the emergency department with CO poisoning. Our second objective is to determine whether there is a relationship between COHb, copeptin, and lactate levels in CO poisoning.
Methods
This observational prospective study was carried out in line with research regulations, including the approval of the Ethics Committee of our institute numbered 2012/137 and according to the principles of the “World Medical Association Helsinki Declaration.”
This study was conducted at a tertiary care university hospital emergency department. Fifty-seven patients who are older than 16 years and admitted to the emergency department with CO poisoning were included in the study. As an inclusion criterion, CO poisoning was defined as COHb levels 5% in nonsmokers and 10% in smokers with clinical symptoms. Exclution criteria were patients younger than 16 years, sepsis, heart and lung disease history, acute and chronic renal insufficiency, cardiovascular problems, and cerebrovascular events.
Age, gender, vital signs, symptoms, and blood parameters of the patients were recorded. Blood samples of the patients were collected on arrival and 6th and 12th h for copeptin, lactate, and COHb levels. Three mililiter of blood sample was collected in a tube with ethylenediaminetetraacetic acid. After shaking the tube, blood was transferred to the centrifuge tube, and blood serum was separated by centrifuging for 10 min at 3500 r min−1. The samples were stored at −70°C until biochemical analysis. Human copeptin test kit (code: EK-065-32 of Phoenix Pharmaceuticals, Inc. (Burlingame, USA)) was used to analyze the copeptin level with sandwich enzyme-linked immunosorbent assay method. Serum copeptin levels were measured quantitatively.
The concentrations of COHb and lactate were assessed in the arterial blood of all patients with suspected CO poisoning directly in the emergency department, using Radiometer ABL 800-flex blood gas analyzer (Radiometer Medical ApS, Bronshoj, Denmark).
In our study, control group was formed from 30 healthy volunteers, and blood samples were taken for serum copeptin level. Active smokers, patients with chronic diseases, anemia, and similar blood disorders were not included in the control group.
All patients were given high-flow normobaric oxygen therapy for 6 h. Hyperbaric oxygen therapy was not administered to any patient. There was no hyperbaric oxygen treatment center in and around our hospital. For this reason, patients with indication for hyperbaric oxygen therapy had to be transferred to another city. During the study period, 68 patients with acute CO poisoning were admitted to the emergency department. Hyperbaric oxygen therapy was indicated in 29 patients. Eleven of these patients were referred to another center for hyperbaric oxygen therapy and were excluded from the study. Patients who denied were transferred to another city, although the indication for hyperbaric oxygen therapy was included in the study. As a result, 57 patients were included in the study.
Data of the study were analyzed using SPSS-17 statistical software. Normal distribution of data was evaluated using one-sample Kolmogorov–Smirnov test. Friedman test was used to compare the levels of copeptin, lactate, and COHb in the study periode (0th, 6th, and 12th h). The value of p < 0.05 was considered statistically significant. Post hoc Bonferroni correction method was applied to the test. Pairwise comparisons of copeptin, lactate, and COHb within themselves were performed using Wilcoxon test. The value of p < 0.017 was considered statistically significant. To determine the correlation of copeptin, lactate, and COHb with each other, Spearman’s correlation test was used. For the comparison of two groups, Mann–Whitney U test was used for the normal non-distributed data. Student’s t-test was used to compare the normally distributed data. The value of p < 0.05 was considered statistically significant.
Limitations
The first limitation of the study is the small sample size with less number of patients showing severe symptoms. The second limitation of our study was that duration of exposure was not standardized. The median time between poisoning and arrival in the emergency room was 1 h, but the range was between 25 min and 8 h. The most important limitation of this study was that the patients who received hyperbaric oxygen therapy were not included in the study. However, it is still unclear that whether hyperbaric oxygen therapy is superior to normobaric oxygen therapy for improving long-term neurocognitive outcomes. We also believe that problems such as difficulty of reaching to the hyperbaric oxygen therapy due to unstable condition of the patients sould be kept in mind in understanding these limitations.
Results
The mean age of the patients presenting to the emergency department with CO intoxication was 37.2 ± 16.1 (range 16–96) years, and 57.9% were female (Table 1). The mean age of healthy volunteers was 35 ± 17.2 (range17–78) years, and 52.7% were female. In all, 89.5% of the patients were symptomatic. The COHb value of eight patients was between 5% and 10%. The median time between the occurrence of intoxication and admission to the emergency department was 1 (interquartile range 2.5) h. The symptoms of the cases are presented in Table 1. In all, 96.5% of the patients reported a coal stove as the source of exposure (Table 1). None of the patients had ischemic electrocardiographic changes. For patients who underwent brain computerized tomography (CT) scan and magnetic resonance imaging (MRI) due to transient loss of consciousness, there was no pathological findings. All patients were given high-flow normobaric oxygen therapy for 6 h. In addition, all patients were brought to the emergency room with an ambulance. Therefore, all patients were given oxygen therapy in the ambulance.
The symptoms and vital signs of the patients.

CK: creatine kinase, CK-MB: creatine kinase–myocardial band, SD: standard deviation.
There was statistically significant difference between the serum copeptin level of patients’ admission and healthy individuals (p = 0.008). But there was no significant difference between patients’ 6th-hour (p = 0.78) and 12th-hour (p = 0.28) serum copeptin levels and healthy individuals’ serum copeptin levels (Table 2). Patients’ 0th-, 6th- and 12th-hour serum copeptin levels were compared with each other by using Friedman’s test. There was statistically significant difference (p = 0.05). When the groups were evaluated as pair, there was statistically significant difference between the 0th and the 6th-hour (p = 0.006) and between 0th-hour and 12th-hour (p = 0.001) serum levels of copeptin (p < 0.017). But there was no significant difference between the serum levels of copeptin on 6th and 12th h (p = 0.51) (Figure 1(a)).
Copeptin levels (ng mL− 1 ) of the cases.a
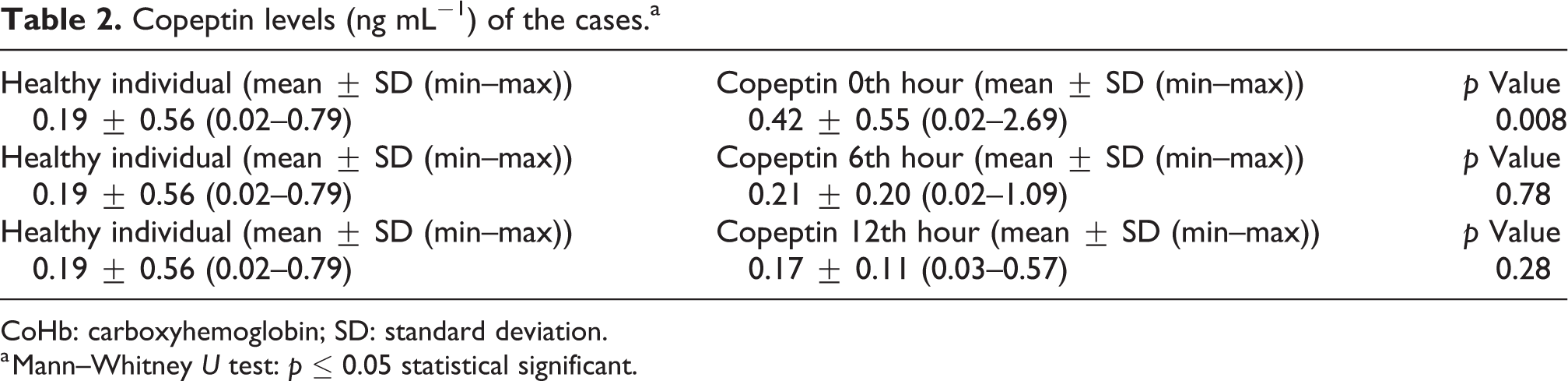
CoHb: carboxyhemoglobin; SD: standard deviation.
a Mann–Whitney U test: p ≤ 0.05 statistical significant.
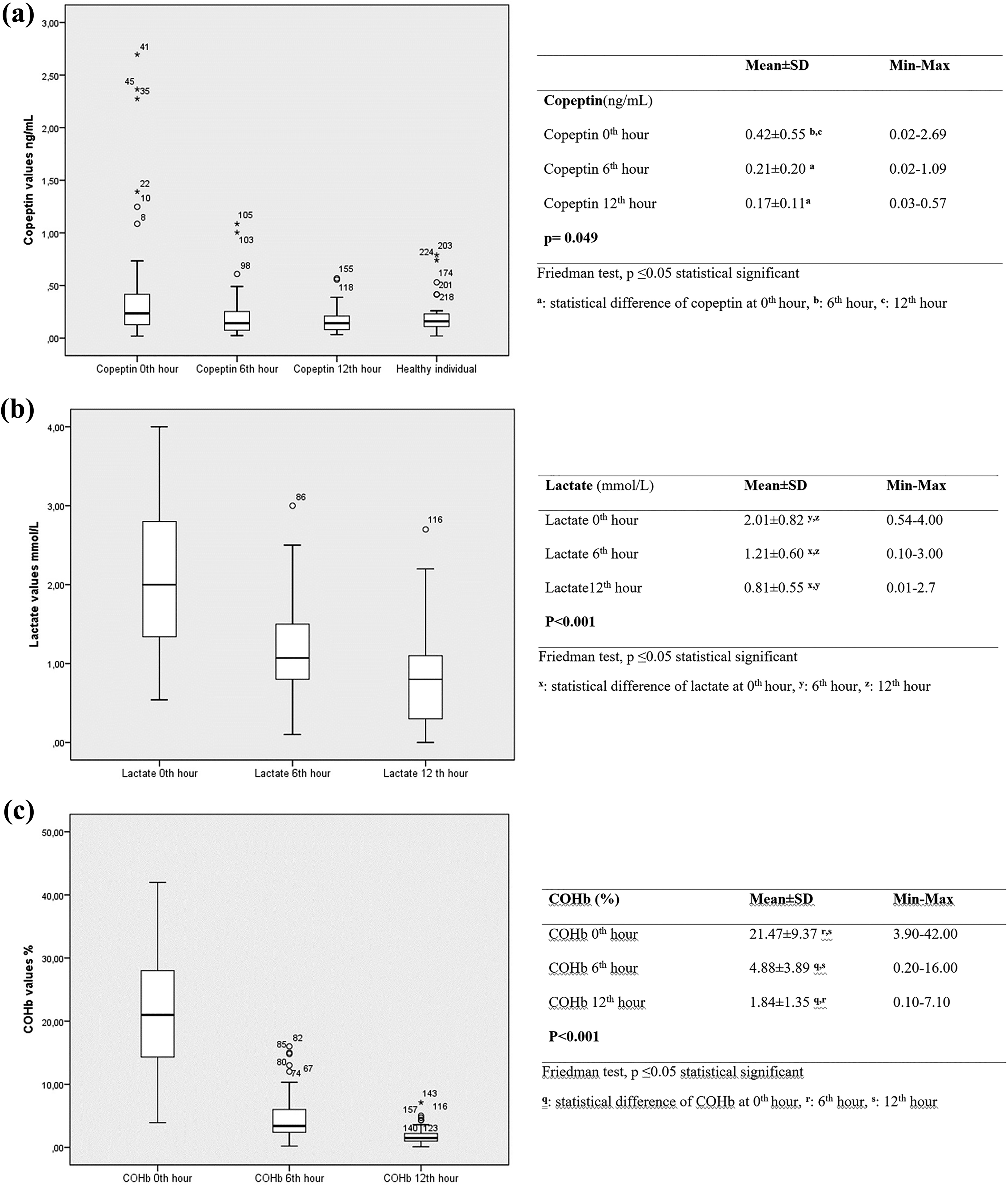
(a) Copeptin, (b) lactate, and (c) COHb levels of the patients according to time. COHb: carboxyhemoglobin.
Then, 0th-, 6th-, and 12th-hour serum lactate levels of the patients were compared with each other using Friedman’s test. There was statistically significant difference among the groups (p < 0.001). When the groups were evaluated as pair, there was statistically significant difference between 0th to 6th h (p < 0.001), 0th to 12th h (p < 0.001), and 6th to 12th h (p < 0.001) serum lactate levels (p < 0.017) (Figure 1(b)).
Patients’ 0th-, 6th-, and 12th-hour serum COHb levels were compared with each other using Friedman’s test. There was statistically significant difference (p < 0.001). When the groups were evaluated as pair, there was statistically significant difference between 0th to 6th-hour (p < 0.001), 0th to 12th-hour (p < 0.001), and 6th to 12th-hour (p < 0.001) serum levels of COHb (p < 0.017) (Figure 1(c)).
When the correlation among copeptin, lactate, and COHb levels were evaluated, a positive correlation between lactate and COHb levels upon arrival (r = 0.52, p < 0.001) was revealed. There was no positive correlation observed between copeptin, lactate, and COHb levels on 0th, 6th, and 12th h (Table 3).
Correlation between blood copeptin, lactate, and COHb levels.a

COHb: carboxyhemoglobin.
a Spearman’s correlation test: p ≤0.05 statistical significant.
There was no statistically significant difference between the patients with and without transient loss of consciousness in terms of plasma copeptin, COHb, and lactate levels upon arrival (p > 0.05) (Table 4). A statistically significant difference was found between the patients with and without transient loss of consciousness in terms of lactate levels on 6th h and copeptin levels on 12th h (p ≤ 0.05) (Table 4).
Relationship between level of consciousness and copeptin, lactate, and COHb levels.a

COHb: carboxyhemoglobin; SD: standard deviation.
a Mann–Whitney U test.
b Student’s t test: p ≤ 0.05 statistically significant.
Discussion
CO poisoning is a medical emergency with high mortality among acute poisoning cases, which is the primary cause of tissue hypoxia and multiorgan failure. Copeptin consists of a 39-amino acid sequence of glycoprotein and serves as a new biomarker. 12 Secretion of copeptin from the hypothalamus increases as part of a stress response. 13 Due to its relatively high sensitivity and poor specificity. 12 Copeptin may provide crucial information for risk stratification in a variety of clinical situations. 2 In the literature, we could reach very limited study of plasma copeptin levels in CO poisoning. There was a significant difference between the serum copeptin levels of healthy individuals and poisoned patients’ arrival copeptin levels in our study. Pang et al. showed that plasma copeptin levels of patients with CO intoxication were significantly higher than those of the healthy subjects. 13 Li et al. determined that the first 2 h of plasma copeptin levels in patients with acute CO poisoning were significantly higher than the healthy subjects. 12 Our result was compatible with these two studies. In the light of these results, copeptin is preferred for the diagnosis of acute CO poisoning.
In our study, there was a statistically significant difference between the 0–6th-hour and 0–12th-hour serum levels of copeptin (p < 0.017). But there was no significant difference between the serum levels of copeptin on 6th and 12th hours. There was no statistically significant difference because the copeptin level decreased significantly in the 6th h. Irem et al. reported that there was a statistically significant difference between the 0th-hour and the 4th-hour plasma copeptin levels of the patients with acute CO poisoning. 14 Also in their study, blood copeptin levels after treatment at hour 4 were significantly lower than the levels at presentation. 14 The results of our study were similar with their study. Plasma copeptin levels increase in the early stages of acute developing diseases. Copeptin is a stress hormone synthesized together with vasopressin, and it is a new diagnostic biomarker for patients presenting with acute diseases. Plasma copeptine levels may regress to normal levels in the early period of the treatment. 2,4,15 We believe that this condition may be associated with a relative decrease in the copeptin levels with treatment.
Chai et al. reported that the level of plasma copeptin increased in 0–4th hour in acute myocardial infarction and decreased after the 6th hour. 4 Ipekci et al. have shown that plasma copeptin levels are high at the time of admission in patients with multitrauma and that they decreased in the early phase of treatment. 15 In our study, plasma copeptin level was found to be high in the first hours of CO poisoning and started to decrease with treatment. Also in this study, it was observed that increased plasma copeptin levels in CO poisoning were decreased to normal levels earlier than other parameters. Copeptin responded earlier to treatment compared to lactate and COHb. This result may be particularly useful in determining the course of the acute disease.
CO has an affinity to hemoglobin more than 210 times from oxygen. It causes tissue hypoxia because of lowered oxygen delivering capacity of blood. This situation affects especially brain and heart, because these organs are very sensitive to hypoxia. 16 Pang et al., in their study, reported that there is a significant difference in plasma copeptin levels between the unconscious and the conscious groups. 13 Also in the study of Pang et al., it has been shown that plasma copeptin levels could be used as a novel biomarker for predicting delayed neurological sequelae after acute CO poisoning. 13 Irem et al. reported that the copeptin levels at hour 0 of patients neurologically affected after CO poisoning (syncope, convulsions, etc.) were significantly higher than those of patients not neurologically affected. Also in the study of Irem et al., there was no statistically significant difference in the levels of copeptin at hour 4 between the groups. 14 In our study, no significant difference was observed between patients with and without transient loss of consciousness in terms of plasma copeptin, COHb, and lactate levels on arrival. There was also no significant difference between COHb and lactate levels. We believe that small sample size may be a factor in this situation, and also we did not investigate the delayed neurological sequelae of these patients. In addition, there were no pathological findings on brain CT and MRI of the patients with transient loss of consciousness in our study. Transient consciousness changes that do not cause pathological findings in the brain in the acute period may not have caused a significant change in copeptin levels. Previous studies have also shown a correlation between the degree of brain injury and copeptin levels. 6 –9 In the study of Irem et al., there was no information regarding whether imaging was performed. 14 In addition, Pang et al. reported no information about the imaging findings of the patients in the acute period. 13
At the 6th hour of lactate and at the 12th hour of COHb, there was a significant difference between those with and without consciousness changes. However, these differences could not be attributed to any reason.
The relationship between severity of clinical signs and increased serum lactate levels as an indicator of the tissue hypoxia was investigated in CO poisoning. In the study of Benaissa et al., it was reported that there is a significant association between serum lactate levels and the severity of neurological impairment in CO poisoning, although plasma lactate levels were mildly elevated in their study population. 17 In another study, it has been reported that serum lactate levels could reflect the severity of CO poisoning. Also it is insisted that COHb levels are not useful predictors in CO poisoning due to reasons such as delayed sampling and preoxygenization before arrival. 11 Additionally, two different studies reported that the initial lactate level can be used to determine the severity of acute CO poisoning, need for hospitalization, and the indication for hyperbaric oxygen therapy. 18,19 In our study, it has been determined that there are significant elevated lactate levels in patients with CO poisoning.
We also found no significant correlation between plasma copeptin levels and COHb-lactate levels in our study. This may be due to the fact that the level of copeptin decreases to the normal level earlier than the other two parameters. At the same time, the number of cases included in the study may also have affected the outcome. We couldn’t find any other study related to this subject in the literature. All the patients included in the study were discharged from the emergency service with complete healing after treatment. We believe that early decrease to the normal levels of plasma copeptin levels compared to COHb and lactate levels in acute CO poisoning can be used to evaluate the early response to treatment.
There are only three studies in the literature on CO intoxication and copeptin. The number of patients was low in all studies, including our study. Therefore, studies with a large number of patients about the value of copeptine in the prognosis of CO intoxication are needed.
Conclusions
It was observed that serum copeptin levels increase during CO poisoning and decrease to normal levels with treatment. Detection of serum copeptin levels in the emergency department may help to determine the diagnosis and monitoring of CO intoxications. However, the copeptin level was not superior to COHb and lactate levels.
Footnotes
Authors' note
S Ozkan and A Sen are now affiliated with Faculty of Medicine, Istanbul University-Cerrahpasa, Istanbul, Turkey and Van Training and Research Hospital, Van, Turkey, respectively.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.