
Abstract
Background:
Late recovery in patients following prolonged coma from carbon monoxide poisoning have been reported, but the probability is unclear. The purpose of this research was to assess the prognosis of patients in prolonged coma after severe carbon monoxide poisoning and related clinical and imaging features.
Methods:
There were 13 patients who had been in a state of coma for >7 days after acute carbon monoxide poisoning in the retrospective observational study, and demographic data, clinical data, laboratory data, complications, and image data were collected. Outcome was assessed by means of the Glasgow outcome scale after 1 year. The relationship between complications and imaging manifestations and prognosis was also analyzed.
Results:
One year after severe carbon monoxide poisoning, two patients (15.4%) had died (GOS 1), nine (69.2%) were in a persistent vegetative state (GOS 2), one (7.7%) was moderately disabled (GOS 4), and one (7.7%) achieved a good recovery (GOS 5) with minimal disability.
Conclusions:
Most patients with prolonged coma after severe carbon monoxide poisoning had a poor prognosis, although the younger patients had a better prognosis. Respiratory failure, hypotension and renal failure during the course of the disease were associated with a poor prognosis. The prognosis of patients with injuries in two sites in early CT was poor. Multiple lesions (≥3) and extensive white matter damage (Fazekas grade (PVH or DWMH) = 3) on MRI of chronic phase were also associated with a poor prognosis.
Introduction
Carbon monoxide (CO) poisoning is one of the most common causes of morbidity due to toxic exposure, regardless of intentional or accidental exposure. 1 In the United States, 50,000 emergency department (ED) visits and 1,200 deaths occurred annually due to non-fire related CO poisoning. 2
Coma is a common symptom after significant exposure to CO. The duration of coma is related to the severity of poisoning. In previous studies,
For patients in a prolonged coma, the prognosis is generally poor; however there have been several reports of late recoveries from prolonged post-cardiac arrest coma. 5 –10 For patients with severe CO poisoning in a prolonged coma, there are also some reports of late recovery. Strohl et al. 11 reported a patient who regained consciousness after 35 days in a prolonged coma after CO poisoning. Zink et al. 4 reported two patients who regained consciousness 17 and 35 days after coma, and were able to live independently after 1 year; however, the likelihood of late recovery is unknown.
It is difficult to ascertain the probability of recovery in patients in prolonged coma. There are no large studies of outcome after prolonged coma from CO poisoning because prolonged coma occurs in <1% of severely poisoned patients. Therefore, we retrospectively investigated the outcome and related clinical and imaging findings of 13 patients who had sustained a prolonged state of coma with severe CO poisoning to provide information for making a clinical decision-making.
Material and methods
A retrospective observational study was conducted in the Hyperbaric Oxygen Department of Chaoyang Hospital (Beijing, China). Data were collected on all CO-poisoned patients admitted to the hospital and were coded with CO poisoning and toxic encephalopathy from January 2012 and January 2019. This study focused on patients who have sustained severe acute carbon monoxide poisoning (ACOP) and had been in a state of coma for more than 7 days. Data were retrieved from the online database of the hospital, including demographic, clinical, laboratory, and image data. Patients with a history of neurological disease and other drug or gas poisoning, or an inability to obtain outcome information were excluded from the study.
For patients included in the study, the following variables were collected and analyzed: CO source; age; sex; chronic diseases, including diabetes, hypertension, and coronary heart disease; carboxyhemoglobin (COHb) level; initial Glasgow Coma Scale (GCS) score on arrival in the emergency department (ED); severe complications during hospitalization (respiratory failure and the need for mechanical ventilation, hypotension (systolic blood pressure <90 mm Hg or mean arterial pressure <65 mmHg for 1 h), and renal failure with increased creatinine [Cr] >50% increase from baseline or the need for acute dialysis); and the time from coma-to-conscious.
As part of a routine examination, every patient with suspected CO poisoning underwent a CT scan on arrival in the emergency department. The CT scanner used was a SOMATOM Emotion 16 (Siemens Healthineers, Erlangen, Germany) or a BrightSpeed Elite (GE Healthcare, Chicago, IL, USA), and the scanning parameters were as follows: layer thickness, 5 mm; and layer interval, 10 mm.
Due to the influence of brain edema in the early stage and the subsequent improvement or aggravation of demyelination in the later stage of the disease, we chose to observe the MRI results of the disease entering the chronic phase (21 days after the onset). 12 Brain MRI was available for most patients. The time from CO exposure to MRI scan was 21–40 days. Three patients failed to complete MRIs due to severe complications. The MRI examination was performed with a 1.5-T MRI unit (Sigma, HDxt; GE Healthcare) using a standard head coil. The MRI protocol consisted of diffusion-weighted MR image (DWI; TR4700, TE81, and b1000), fluid attenuated inversion recovery image (FLAIR; TR8602, TE150, and TI2100), T1 weighted image (T1WI; TR1782, TE20, and TI750), T2 weighted image (T2WI; TR5200 and TE124). The scanning parameters were as follows: layer thickness, 5 mm; and slice space, 6.5. Fazekas’ grading method was used to evaluate damage of white matter. 13 This four-point scale assesses periventricular white matter involvement and deep white matter involvement. Periventricular hyperintensity (PVH) was graded as 0 = absence, 1 = caps or pencil-thin lining, 2 = smooth halo, 3 = irregular PVH extending into the deep white matter. Separate deep white matter hyperintense signals (DWMH) were rated as 0 = absence, 1 = punctate foci, 2 = beginning confluence of foci, 3 = large confluent areas. All resulting images were independently analyzed by two experienced MR radiologists with a third radiologist arbitrating on discrepant results.
Hyperbaric oxygen treatment was administered if there were no contraindications during hospitalization. Patients were placed in a multi-place chamber pressurized with compressed air. Each session consisted of a 60-min exposure to 100% oxygen at 2ATA. The compression time was 25 min and the decompression time was 40 min. 6 days per week. The total number of sessions was 20–40. At the same time, nutritional support, symptomatic treatment and bedside rehabilitation treatment were provided. The patients underwent rehabilitation in the community after being discharged from the hospital.
All patients had a 1-y follow-up evaluation and outcomes were determined. Functional status was assessed using the Glasgow Outcome Scale (GOS). The GOS score is categorized as follows: 1. death; 2. vegetative state and unconscious, but with cardiac activity and respirations, occasional opening of the eyes, yawning, and other local motor reactions; 3. severely disabled and conscious, but cognitively, verbally, and physically disabled, and needing to be cared for by others full-time; 4. moderately disabled with cognitive, behavioral, and personality disorders with mild hemiplegia, ataxia, dysphasia, and other disabilities, and marginally independent in daily life, family, and social activities; and 5. good recovery and can resume most normal activities, but may have minor residual problems.
Because of the small number of patients available, we used descriptive statistics to evaluate the characteristics of the patients included in the study. Due to the small number of severe CO poisoning patients available, a comparison analysis was deemed to be at high risk for a type II statistical error and was not undertaken.
Results
A total of 31 people was admitted to the hospital in a coma due to carbon monoxide poisoning in the past 7 years. The time of becoming conscious was different: seven within 12 hours, three within 24 hours, one within 1–3 days, and seven within 4–6 days. Thirteen people were unconscious for more than 7 days. See details in Table 1.
Number of patients with carbon monoxide poisoning admitted to the hospital for different coma time.
The mean age of patients was 51 years (range, 23–71 years); eight patients were female and five were male. During the first neurological evaluation, the patients had a GCS score of 3–5. The cause of poisoning was due to coal heating and poor ventilation. The average COHb value was 26.3% (range, 2%–40%). Four patients had hypertension, one had diabetes, and the remaining patients had no underlying disease. See details in Table 2.
Basic clinical features of 13 patients with prolonged after carbon monoxide poisoning.

F: female; M: male; GCS: Glasgow Coma Scale; GOS: Glasgow Outcome Scale; GP: globus pallidus; BG: basal ganglia (other basal ganglia except globus pallidus); CBLM: cerebellum; WM: white matter; CTX: cortex; HCP: hippocampus; CC: corpus callosum; MB: midbrain; PVH: periventricular hyperintensity; DWMH: deep white matter hyperintense signals; ND: not done.
One year after ACOP, two patients (15.4%) had died (GOS 1), nine (69.2%) were in a persistent vegetative state (GOS 2), one (7.7%) was moderately disabled (GOS 4), and one (7.7%) achieved a good recovery with minimal disability (GOS 5). The outcome scores at 1 year for 13 patients are listed in Table 2.
Eleven of 13 patients had a poor prognosis, among which 5 had respiratory failure during the course of disease and were on ventilator support, 3 had hypotension, and 1 had renal failure. Two of the 13 patients had a good prognosis with no respiratory failure, hypotension, or other complications during the course of disease.
The most common abnormal finding on early CT, which was demonstrated in 10 of 13 patients, was symmetric, diffuse, low density cerebral white matter. A second characteristic feature in 5 of 13 patients was the presence of symmetric, round, low density lesions in the globus pallidus or other basal ganglia. Lesions in other parts included the cerebellum (n = 1). The prognosis of patients with simultaneous damage to the white matter and globus pallidus or basal ganglia was poor.
Ten of 13 patients had MRI results. All 10 patients had high signal changes in the cerebral hemisphere white matter on DWI images. The white matter of the cerebral hemisphere includes the paraventricular and centrum semiovale. In critically ill patients, the white matter of the cerebral hemisphere can be extensively involved and necrotic (see Figure 1). Fazekas’ grades of PVH or DMWH in two patients with good prognosis were less than 3. On the contrary, Fazekas’ grades of PVH or DMWH in patients with poor prognosis were 3. It suggested that severe white matter lesions were associated with poor prognosis. Eight of 10 patients had globus pallidus injuries. Other affected parts included the cerebral cortex, cerebellum, hippocampus, corpus callosum, midbrain, and other basal ganglia except for the globus pallidus. The two patients with better recovery had only white matter and globus pallidus damage on the MRI, while the other eight patients with a poor prognosis had injuries involving more than two sites (see Table 2).
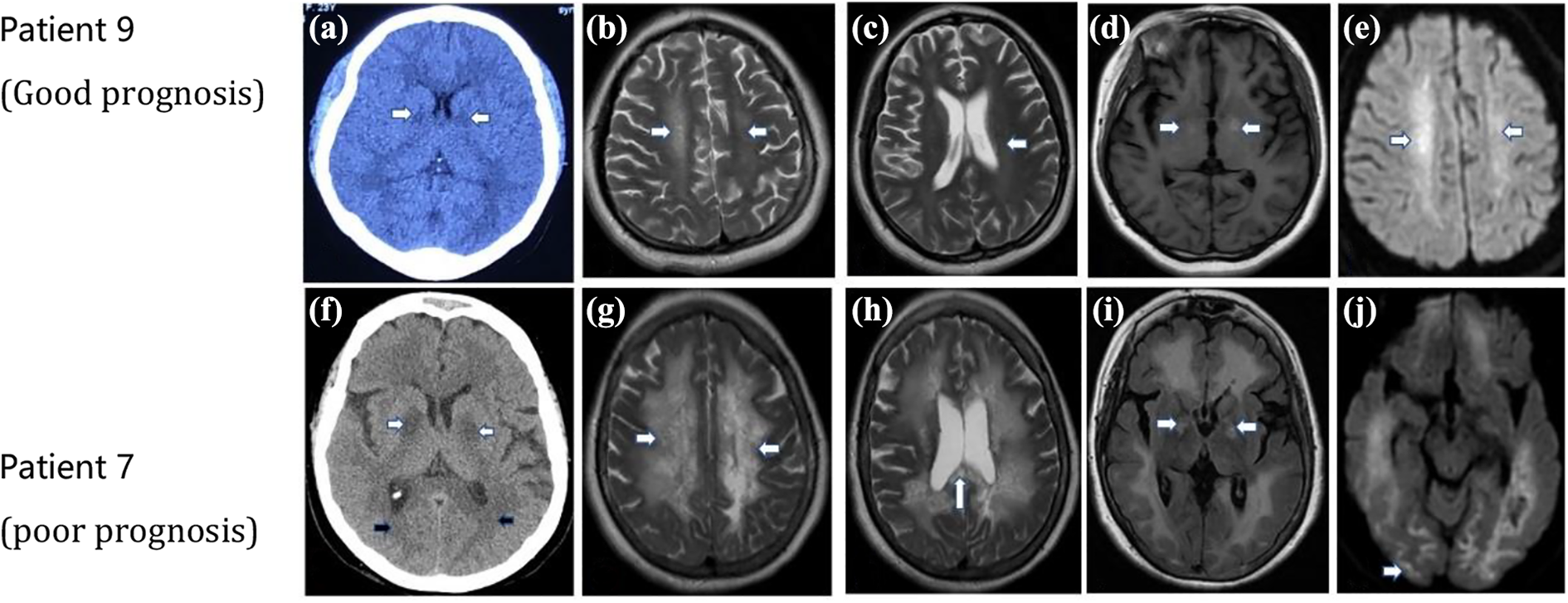
CT and MRI images of patient 9 (a to e) and patient 7 (f to j) examined after ACOP. (a) CT image of patient 9, injury of the bilateral globus pallidus (white arrow) can be observed. (b to e) MRI images of patient 9 examined 37 days after ACOP. (b, c, and e) T2WI and DWI image showed injury of the white matter (white arrow). (d) T1WI showed injury of the globus pallidus (white arrow). (f) CT image of patient 7, injuries of the white matter (black arrow) and the bilateral globus pallidus (white arrow) can be observed. (g to j) MRI images of patient 7 examined 39 days after ACOP. (g and h) T2WI showed diffuse injuries over the white matter (white arrow) and corpus callosum (white arrow). (i) FLAIR image showed injury in the globus pallidus (white arrow). (j) DWI image showed involvement of right occipital cortex (white arrow). CT and MRI images of patient 7 (poor prognosis) showed multiple sites and more serious injuries.
Discussion
In this study, 2 of the 13 patients (15.4%) regained consciousness. Patient 1 regained consciousness 25 days after the onset of ACOP and her GOS score was 4 after 1 year. She was partially self-supporting and still required the assistance of others. Patient 9 regained consciousness in 55 days and had a good prognosis after 1 year, and returned to normal life and work. These results suggested that late recovery of prolonged coma and good prognosis after CO poisoning was possible, but the proportion was small. Some examples of late recovery have been reported in the literature. Zink et al. 4 reported two patients (19 and 30 years of age) who regained consciousness 17 and 35 days after coma and were able to live on their own after 1 year. The two patients in this report were as young as the patient in our study (23 years of age) who recovered well. The time to recover consciousness among the three patients was 17, 35, and 55 days after the onset of coma. The histories of the three patients suggested it was possible that patients <30 years of age could gain consciousness and have a good prognosis 2 months after severe ACOP. Braakman et al. 14 studied the prognosis of patients in a vegetative state after a traumatic brain injury and concluded that age is an important prognostic factors. In the group of patients >40 years of age, none recovered to full independence. Among patients 20–40 years of age, 4 of 46 patients had restoration of independence. Eleven of 53 patients <20 years of age, had restoration of independence. Our results were consistent with this study.
During hospitalization we focused on the relationship between severe complications and prognosis. We found that patients who had experienced severe organ failure (respiratory failure, hypotension, and renal failure) all had a poor prognosis. The two patients with a better prognosis did not have severe complications. This was consistent with Liao et al.’s study, who found that patients with carbon monoxide poisoning had a poor prognosis for more than three organ failures. 15 According to a recent study, patients with ACOP and >1.5 days of intubation days had a higher probability of a poor outcome after treatment. 16 Another study showed that severe metabolic acidosis and need for endotracheal intubation were strongly associated with mortality. 17 These studies suggested that intubation was associated with a poor prognosis. Intubation and ventilator support ventilation all suggested hypoxemia in the patients, and previous studies also showed that hypoxemia and hypotension aggravated white matter injury in ACOP patients, 18,19 which could account for the poor prognosis. Therefore, the occurrence of respiratory failure and hypotension in the course of the disease was related to the poor prognosis, and the occurrence of these complications required enhanced monitoring and active treatment to reduce brain damage and improve the prognosis.
In patients with CO poisoning, the severity of brain injury on CT or MRI is related to the prognosis. 20,21 This study is the first case series showing a correlation between CT and MRI performance and prognosis in patients with prolonged coma. Early CT and MRI of chronic phase usually showed severe white matter demyelination and other multi-site injuries. The prognosis of patients with injuries in two sites in early CT was poor. MRI showed that damages in more than three sites or Fazekas grades (PVH or DWMH) of white matter equal to 3 were associated with poor prognosis. This discovery provided important information for decision-making and prognostication.
Limitations
ACOP with prolonged coma is uncommon and thus studies on this topic are necessarily based on a small number of cases. The number of patients we reported was insufficient to draw reliable conclusions and we could only suggest possible speculation worthy of further investigation.
Conclusion
In this study, most patients with prolonged coma after severe CO poisoning had a poor prognosis, and the younger patients had a better prognosis. Severe respiratory failure, hypotension, and renal failure during the course of the disease were associated with a poor prognosis. The prognosis of patients with injuries in two sites in early CT was poor. Multiple lesions (≥3) on MRI and extensive white matter damage (Fazekas grade (PVH or DWMH) = 3) on MRI of chronic phage were also associated with a poor prognosis.
Footnotes
Author contributions
YG and HG contributed to the conception and design, acquisition of data, analysis and interpretation of data and were involved in drafting the manuscript and revising it critically for important intellectual content. JY, LY, ZL and JZ contributed to the acquisition of data, analysis and interpretation of data. All authors have given final approval of the version to be published. Each author agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Availability of data and materials
A minimum data set may be made available from the corresponding author following reasonable request.
Consent for publication
Written informed consents were obtained from the patient and her parents for publication of this article and any accompanying images. Copies of the written consent are available for review by the Editor of this journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Approval/Institutional Review Board (IRB) is not needed because this is not a case of new intervention is performed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.