
Abstract
Objective:
Mushroom poisoning is still a significant health-care problem, with the potential to affect blood parameters. The present study analyses the effect of mushroom poisoning on complete blood cell parameters, cell ratios, and cell volume indices and the effect of the mentioned parameters on prognosis/hospital length of stay.
Methods:
The study involved the retrospective assessment of 48 patients who became symptomatic after ingesting mushrooms. Patients who were 18 years and above and who spent at least one day in hospital were included in the study. The control group comprised individuals with similar characteristics to the patient group. The complete blood cell parameters, platelet indices (mean platelet volume, plateletcrit (PCT)), neutrophil to lymphocyte ratio (NLR), and platelet to lymphocyte ratio levels were compared between the two groups, and these ratios were analyzed for any correlation with length of hospital stay.
Results:
NLR was significantly higher and PCT was significantly lower in the mushroom-poisoned group, while all other parameters were similar between the groups. NLR had a positive correlation and PCT had a negative correlation with length of hospital stay.
Conclusion:
NLR and PCT levels can provide information about prognosis and can aid in the prediction of hospital stay in mushroom-poisoned patients. Further investigations are needed to investigate effects of intoxication on hematological system elements.
Introduction
There are around 5000 species of mushrooms around the world, 3% of which are known to be toxic. Turkey is home to a host of mushroom varieties. Cases of mushroom poisoning increase in spring and summer months, 1 and in 2014, 5228 cases of mushroom poisoning were reported in Turkey. 2 Mushroom poisoning is a serious condition that can result in serious morbidity and mortality, with severity depending on the type and quantity of mushroom ingested. Ingestion may require emergency services and hospital/intensive care admission, especially in cases of community consumption. In Turkey, the leading types of toxic mushrooms are Amanita muscarina, Amanita xanthoderma, Amanita citrina, Amanita phalloides, Clitocybe dealtaba, Lepiota helveola, Inocybe fastigiata, Neomataloma fasciculare, and so on. 3 The basic mechanism in mushroom poisoning involves the toxins produced by the fungus affecting, most commonly, the gastrointestinal tract, the urinary tract, and the nervous system, as the most frequently affected areas. The initial symptoms are usually gastrointestinal complaints, and the laboratory values of the patients may indicate leukocytosis, thrombocytopenia, hyperbilirubinemia, elevation of transaminases, impaired renal function tests, deterioration of coagulation tests, and microscopic hematuria. 4
The neutrophil to lymphocyte ratio (NLR) is calculated by dividing the number of neutrophils in the complete blood count by the number of lymphocytes. NLR reflects the balance between neutrophils, the innate immunity element, and lymphocytes with adaptive immunity, with increased levels usually associated with systemic inflammation. 5 NLR has been investigated in many diseases, and it has been shown to determine prognosis for some cancers and has been associated with cardiovascular morbidity and mortality. 6 In the present study, we investigate varying hemogram parameters, cell ratios, and volume indices in patients presenting with mushroom poisoning and the effects of the mentioned parameters on prognosis and length of hospital stay.
Materials and methods
The case-controlled study included 48 patients aged 18 years and above who had spent at least one day in hospital with symptoms starting after the ingestion of mushrooms. The cases were all admitted to the Çorum Hitit University, Erol Olçok Training and Research Hospital, Emergency Room between June 2017 and June 2018. Age, gender, length of hospital stay noted in the archive and the file records of patients, and laboratory data upon admission to the hospital were recorded, along with hemoglobin, leukocyte count, neutrophil count, platelet count, mean platelet volume (MPV), plateletcrit (PCT), mean erythrocyte volume (MCV), bilirubin and transaminase levels, and blood gas parameters. The NLR and platelet–lymphocyte ratios were calculated using the PCT = Platelet count × MPV/10,000 formula for the calculation. The Charlson comorbidity index was used to evaluate comorbidities, for which 17 comorbidities, such as diabetes, heart disease, lung diseases, liver diseases, and malignancies, are investigated. All the above levels were compared with the values of 40 cases with no history of mushroom poisoning, no systemic inflammation, and a similar control group in terms of age, symptoms, and comorbidity. All medical records were investigated retrospectively. Institutional approval was obtained for the use of the data.
Statistical analysis
The IBM SPSS version 25 software package was used for all analyses, and a Shapiro–Wilk test was used to evaluate distributions. Numerical values without normal distribution were recorded as minimum–-maximum, and mean ± standard deviation values were calculated for the normally distributed values. The Mann–Whitney U test was used to compare grouped values; the Spearman’s correlation analysis was performed to identify the relationship between values; and the multiple regression analysis was performed for significant values and a p < 0.05 was considered significant.
Results
Within the study, 48 cases of mushroom poisoning were evaluated. The median age of the sample was 46.5 (minimum 18 and maximum 77), and 27 of the patients were female. The main reasons for admission were gastrointestinal symptoms such as nausea, vomiting, and abdominal discomfort in 44 patients, and neurological symptoms such as dizziness and headache in 4 patients. The characteristics of the patients and the laboratory levels at the time of presentation are summarized in Table 1. The types of mushrooms ingested were unknown, as the patients did not bring samples to the hospital and they had no knowledge of their names. NLR was significantly higher in patients with mushroom poisoning than in the control group, and PCT levels were significantly lower (p < 0.01). There were no significant differences at other levels (Table 2). The length of hospital stay was positively correlated with NLR, while there was a negative correlation with PCT levels (r = 0.398, p < 0.01 and r = −0.313, p < 0.01, respectively) (Figure 1 and 2). In a multiple regression analysis for a causality evaluation, a significant correlation was noted between NLR and PCT (p < 0.01 and p = 0.01, respectively) (Table 3).
Patient characteristics and laboratory upon hospital admission of poisoning patients.

MPV: mean platelet volume: PCT: plateletcrit; MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; aPTT: activated partial thromboplastin time; INR: international normalized ratio.
Values of groups comparisons.
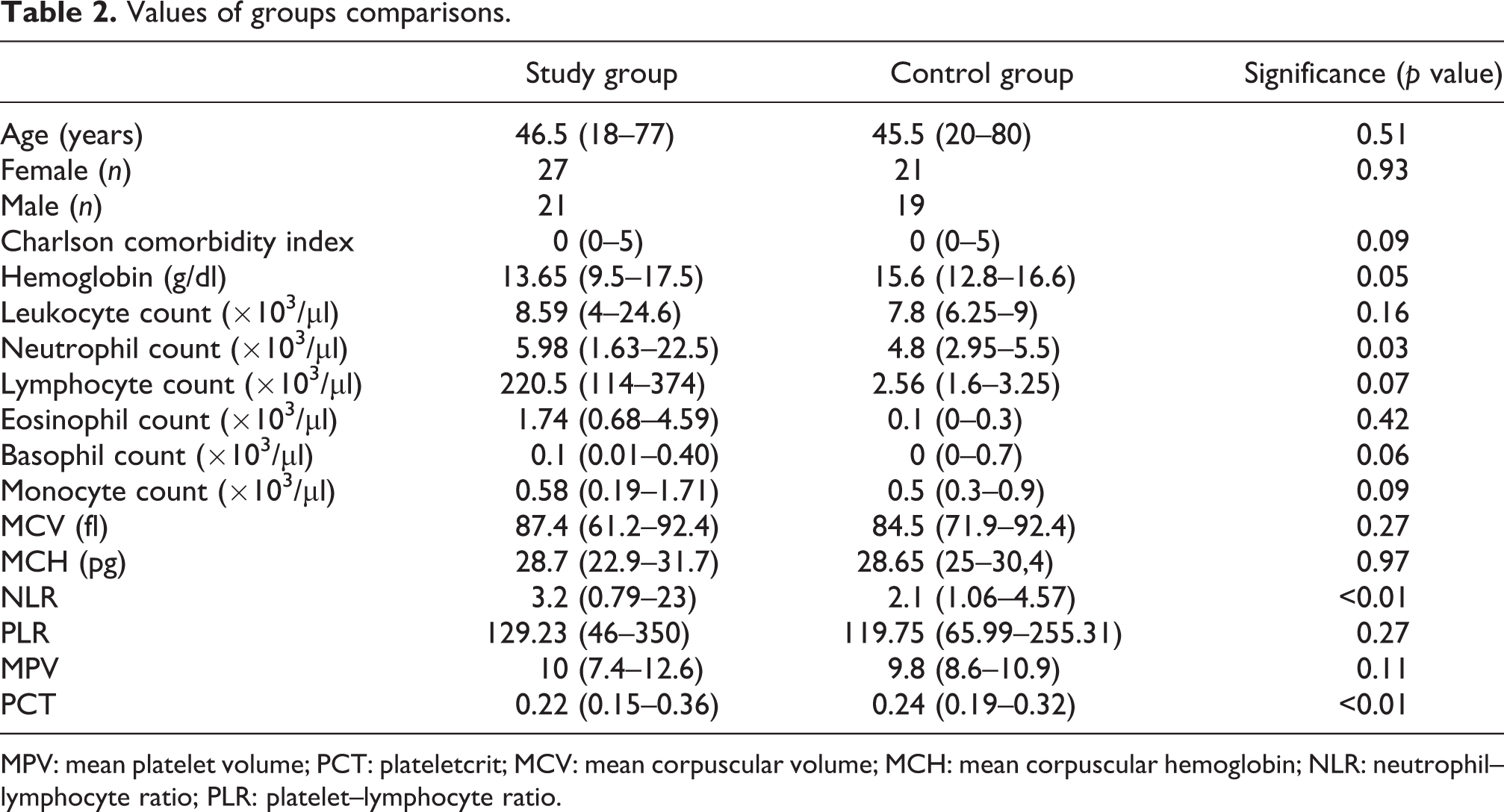
MPV: mean platelet volume; PCT: plateletcrit; MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; NLR: neutrophil–lymphocyte ratio; PLR: platelet–lymphocyte ratio.

Length of hospital stay and NLR. NLR: neutrophil–lymphocyte ratio.
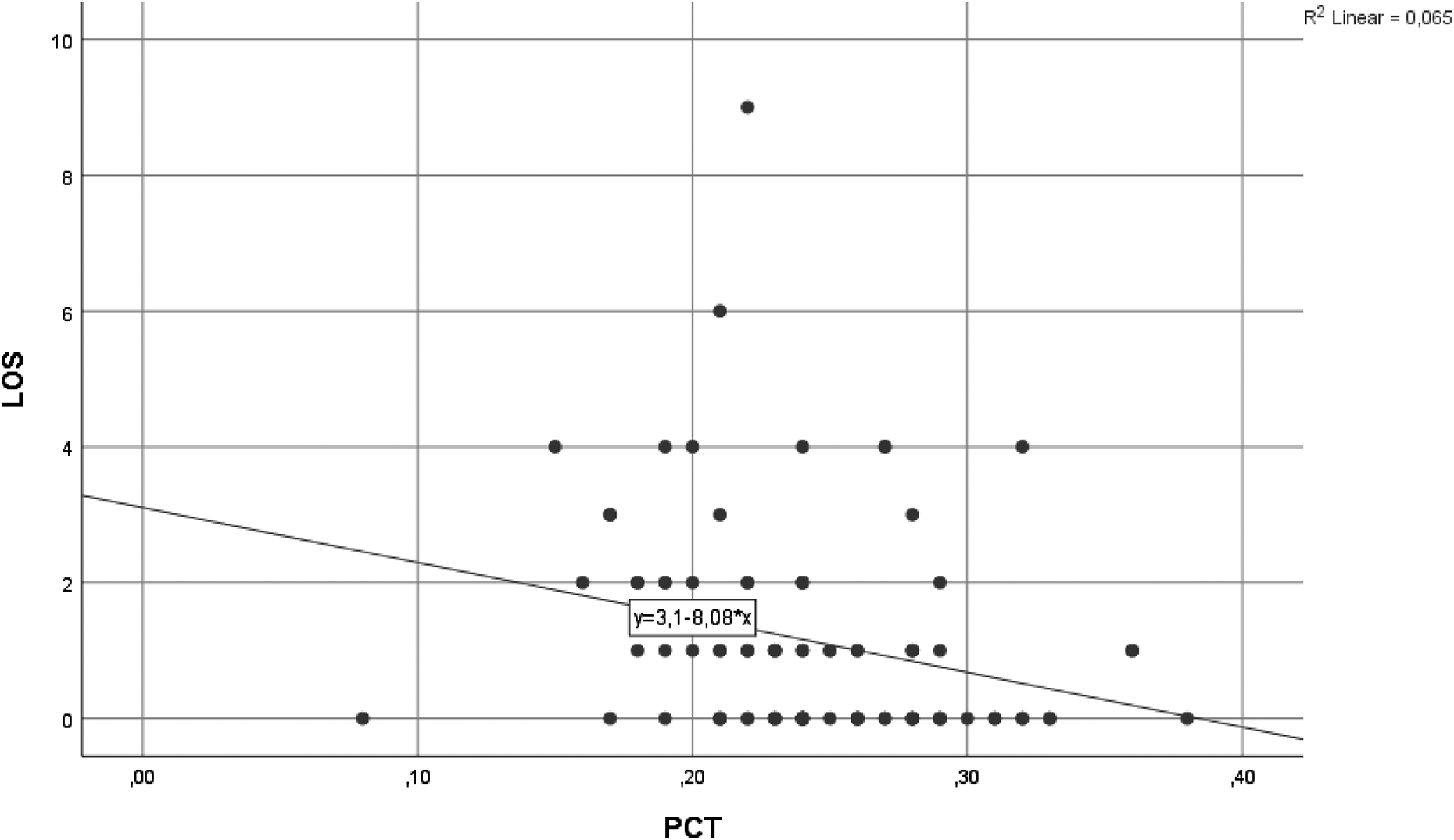
Length of hospital stay and PCT. PCT: plateletcrit.
Multiple linear regression analysis between hospital length of stay and PCT and NLR.

PCT: plateletcrit; NLR: neutrophil–lymphocyte ratio.
Discussion
Mushroom poisoning is a serious public health problem that results in mortality and that is still common in many countries. Such poisoning most often affects the gastrointestinal and nervous systems. 7 The effects of mushroom poisoning on the immune system have to date not been studied in detail. Although it is known that poisoning can lead to leukocytosis, the effects of other complete blood count parameters are not clear. 8,9 NLR has emerged as a frequently searched, cheap, and easy-to-use test in recent years. Studies have shown that a high NLR correlates with elevated IL-6 and C-reactive protein (CRP) levels, and accordingly, NLR is thought to reflect the systemic inflammation and stresses to which the body is exposed. 10 NLR has proved to be prognostic in many cardiovascular diseases, malignancies, and noninfectious pathologies, with high levels being associated with morbidity and mortality, and chronic systemic inflammation leading to endothelial damage has been shown to be the main mechanism. 5,10 –12
One of the most frequently studied substances in investigations of the inflammatory and immune system effects of intoxication is alcohol. The negative effects of the overconsumption of ethanol on natural and adaptive immune system elements have been shown previously. 13
There has to date been no study analyzing NLR values in cases of mushroom poisoning in the literature, and accordingly, the present study may be the first research into this issue. In the present study, NLR was found to be higher in patients with a history of mushroom poisoning than in the control group, which may indicate that mushroom poisoning can cause damage to the immune system as well as systemic inflammation. These values are also found to affect the length of hospital stay until laboratory or clinical improvement is achieved. This may be an indication that the higher the NLR levels, the greater the severity of the disease, or the poorer the prognosis. There were no significant differences in the blood count parameters or rates, which may be due to the fact that these parameters do not change in an acute event, although it could be attributed to the characteristics of the sample. A study investigating the relationship between NLR and poisoning by Gunaydın et al. 14 looked at NLR levels in cases of carbon monoxide intoxication, although no relationship was identified between prognosis and the severity of the disease.
Patients with a history of mushroom intoxication had lower PCT levels. PCT has been suggested as guiding thrombocyte dysfunction in recent studies 15 and so has been the subject of research into coronary artery diseases, in which high PCT values in particular are found to be a risk factor for acute coronary syndrome. 16,17 There have also been studies showing that platelets may be defective in the presence of low PCT levels and may be a risk factor for coronary artery disease. 16 It was suggested in the present study that a low detection of PCT may indicate a negative effect of toxins on platelets or the vascular system in the acute phase, although original and more detailed studies are needed to support this. A review of the literature identified no previous investigations into the relationship between PCT and mushroom poisoning.
The study has several limitations. It is a retrospective analysis of cases from a single center, and not all medical records were available. The types of mushroom ingested were generally unknown, and data were based on patient history. In addition, only cases of mild-to-moderate severity were evaluated, while those requiring intensive care or transplantation, those that resulted in mortality, or those at high risk were not evaluated. Inflammatory markers such as CRP at the time of admission were not available. There were also limitations related to study design and statistics. R2 was low and the description of significance was difficult. The control group may not have been well-matched, and the fact that not all mushrooms behave in the same way was ignored. Each subject has a different immune system and reactions may vary. There is a need for more comprehensive, multicenter observational studies that reflect society as a whole and that are more specific to the immune and hematological system.
In conclusion, NLR and PCT values may provide insight into the prognosis of mushroom poisoning and can help in the prediction of hospital stay durations. It may be necessary to take attention in patients with high values. Further investigations into mushroom poisoning are needed to identify the effects on blood parameters before these parameters can be adopted as prognostic tools.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.