
Abstract
We studied occupational exposure to phthalates from first-morning-void urine sample of hairdressing apprentices by HPLC-MS/MS analyses and association with health status. Metabolites of mono(2-ethyl-5-hydroxyhexyl) phthalate (MEHHP), mono ethyl phthalate (MEP), mono-n-butyl phthalate (MnBP) and mono-iso-butyl phthalate (MiBP) were detected in all urine samples, followed by metabolites mono(2-ethyl-5-oxohexyl) phthalate (MEOHP) and mono(2-etylhexyl) phthalate (MEHP) occurring in 97.06% and 86.76% of samples, respectively. Positive associations for females were observed between MnBP and fat-free mass index (FFMI) and age; negative associations were found between MEHP, MEOHP, MEHHP, sum of MEHP, MEHHP, MEOHP and vital capacity and also between MEHP and forced vital capacity (FVC of predicted value (PV)). Lengths of exposure were associated to MnBP, MEHHP, and MEP. We also documented positive associations between anthropometry (body mass index, waist-to-height ratio (WHtR), FFMI, fat mass index) and pulmonary function FVC% of PV for females and negative associations between WHtR, waist-to-hip ratio, FFMI and ratio of forced expiratory volume in 1 s (FEV1) to FVC (FEV1/FVC). We assume that factors of occupational environment of hairdressing apprentices are affected by phthalates and resulted in negative outcomes in breathing mechanism and influence of body composition. Adipose tissue could play role as confounding factor in urine excretion of phthalates because of their lipid solubility and accumulation.
Keywords
Introduction
Hairdressing is a widespread occupation. Thousands of synthetic hazardous chemical substances used in cosmetics industry 1 and potential health hazards in occupational environment of hairdressers, including biological, chemical, physical, and ergonomic factors, have a negative impact on individual’s health. 2 An association between the occupation of hairdressing and musculoskeletal, 3 –5 dermal complications, 6 –9 cancer of breast, 10 liver 11 and bladder, 12 fertility concerns, and gynaecological health 13 –15 were documented. Chronic bronchitis, asthma, asthma-like symptoms, allergy, and other respiratory illnesses were observed in several studies. 16 –19 Hairdressers are typically exposed to a cocktail of chemicals, however, biological effects of exposure to mixtures of chemicals in general are largely unknown. 20 Phthalic acid esters are widely used as synthetic additives 21 and benzyl butyl phthalate, dibutyl phthalate (DBP), di(2-ethylhexyl)phthalate (DEHP), di-isodecyl phthalate (DiDP), di-isononyl phthalate (DiNP) and other belong to chemicals commonly found in cosmetics and personal care products (nail polish, hair sprays, aftershave lotions, soaps, shampoos and perfumes) and other fragrance preparations, because of their ability to hold colour, denature alcohol and fix fragrance. 22 –26 Phthalates have endocrine disrupting properties; they alter hormone signalling in the human and have a potential effect on the reproductive and nervous system and metabolism as well as on cancer cell proliferation. 27 Nevertheless, data on human health effects related to phthalate exposure are still limited. It should be noted that in this type of occupational environment, exposure prevention due to absence of adequate ventilation and use of personal protective equipment mostly is insufficient. 28
Our observational study is aiming to investigate health problems of hairdressing apprentices in educational facilities associated to occupational phthalate exposure.
Materials and methods
A cross-sectional study was carried out among study population comprised a pooled cohort of hairdressing apprentices attending vocational training schools (n = 68) residing in western part of Slovakia (group A). Students normally spend 6–8 h per day in the beauty hair salon. Recording information about their health and biomonitoring of phthalates was carried out in the systematic manner. More than 97% of probands were females (n = 66) and only 2.9% were males (n = 2). Their median age was 17.7 ± 1.2 years (range 16–20 years). Group B (control group) consisted of students and employees from Constantine the Philosopher University in Nitra (group B; n = 32; average age: 23.8 years; 65.6% of females and 34.4% of males). The apprentices were interviewed and examined physically. Written informed consent was obtained from each participant. This study received an approval from the Institutional Review Board of the Slovak Medical University, Bratislava, Slovakia. The following patients were excluded: those diagnosed with respiratory illness and metabolic disorders, not providing spot urine sample, subjects with incomplete answers to questions of the questionnaire and with prescription of bronchodilators or steroids. Data published in article is available to other researchers upon request.
Phthalate analyses
We collected spot urine samples (2 × 2 mL) from volunteers during work shift breaks (i.e. beginning of work not earlier than 6:00 a.m. and work duration at least 8 h per shift), at the end of the work week (Friday), and stored them in a transport box at 2–6°C and in the laboratory in a deep freezer at −73°C. Urinary concentration of mono ethyl phthalate (MEP), mono-butyl phthalate (MBP), mono(2-etylhexyl) phthalate (MEHP), mono(2-ethyl-5-hydroxyhexyl) phthalate (MEHHP) and mono(2-ethyl-5-oxohexyl) phthalate (MEOHP) was determined by high-performance liquid chromatography (HPLC) and tandem mass spectrometry (MS/MS; Infinity 1260 and 6410 triplequad, Agilent, Santa Clara, CA, USA). 29 Analytical standards were purchased from Cambridge Isotope Laboratories (Tewksbury, Massachusetts, USA). Briefly, 1 mL of urine was thawed, buffered with ammonium acetate, spiked with isotope labeled phthalate standards, β-glucuronidase enzyme (Roche, Germany) and incubated at 37°C. The samples were then diluted with phosphate buffer (NaH2PO4 in H3PO4) and loaded on SPE cartridges (ABS Elut Nexus, Agilent) conditioned with acetonitrile followed by phosphate buffer before extraction. To remove hydrophilic compound, SPE cartridges were flushed by formic acid and HPLC grade water. Elution of analytes was performed by acetonitrile and ethylacetate. Eluate was dried by nitrogen gas and reconstituted with 200 μl of H2O. An Agilent Infinity 1260 liquid chromatograph equipped with ZORBAX Eclipse phenyl-hexyl column was used for analysis. Separation was done using nonlinear gradient program. Agilent 6410 triplequad with electrospray ionization was used for mass specific detection of phthalate metabolites. Instrumental settings were as follows: spray ion voltage (−3800 V), nitrogen nebulizer gas pressure (8 psi), nitrogen curtain gas pressure (7 psi), capillary temperature (430°C) and collision gas (nitrogen) pressure (1.5 mTor). Precursor and product ions, collision energies, retention times and limits of detection (LOD) are shown in Table 1.
Phthalate monoesters: chromatographic and mass spectrometric parameters.

MEP: mono ethyl phthalate; MnBP: mono-n-butyl phthalate; MiBP: monoiso-butyl phthalate; MEHP: mono(2-etylhexyl) phthalate; MEHHP: mono(2-ethyl-5-hydroxyhexyl) phthalate; MEOHP: mono(2-ethyl-5-oxohexyl) phthalate; F: fragmentor; CE: collision energy; RT: retention time (min); LOD: limit of detection (ng/mL).
Anthropometry
Standard methods were used to collect anthropometric parameters as body height (by A 319 TRYSTOM, Ltd, Olomouc, Czech Republic), waist girth and hip girth (by a flexible non-elastic measuring tape). Body mass index (BMI), waist-to-height ratio (WHtR), waist-to-hip ratio (WHR), fat mass index (FMI) and fat-free mass index (FFMI) were calculated. Body weight, body fat percentage, muscle mass percentage and visceral fat level were estimated by bioelectrical impedance analysis using a 50 kHz current source with electrodes on each hand and foot (Omron BF510, Kyoto, Japan).
Spirometry
Pulmonary function test (PFT) was done at room temperature by a trained technician according to 2005 European Respiratory Society/American Thoracic Society recommendations 30 using a spirometer (Spirolab II, MIR, Rome, Italy) and Winspiro PRO software. We recorded the best result from three consecutive pulmonary function tests. All the PFTs were done without bronchodilator. Values for forced expiratory volume in 1 s (FEV1, L), forced vital capacity (FVC, L), the ratio of FEV1 to FVC (FEV1/FVC, %), maximal voluntary ventilation (MVV, L) and peak expiratory flow (PEF, L) were obtained. All these parameters are expressed as percentages of reference values which were designated according to age, sex, weight and height and ethnic origin.
Statistics
Concentrations of phthalate metabolites were calculated using the MassHunter workstation software, version B.04.01. Association between anthropometric parameters and pulmonary function and concentration of phthalate metabolites was examined by Pearson correlation analysis. The non-parametric Mann–Whitney U (Wilcoxon rank-sum) test was used for analyses between pack year (p/y) index, sport activity and dynamic pulmonary function and to compare urinary phthalate concentrations and pulmonary functions between study and control groups. Difference was considered statistically significant at p ≤ 0.05. For description of urinary phthalate metabolite levels in the study populations, means with standard deviations (SDs), medians and the 5th and 95th percentiles of concentrations were computed. Data were analysed using Statistica 8.0 (Stat Soft. Inc., Tulsa, Oklahoma, USA).
Results
For recruitment of study subjects, we have chosen hairdressing salons located in the schools for hairdressing apprentices rather than ordinary salons, as these students were exposed to pollutants for a longer time. We have biomonitored occupational exposure to phthalates and assessed health status and lifestyle factors of 68 hairdressing apprentices. The baseline characteristics of the study group are shown in Table 2.
Baseline characteristic of study groups.

A: hairdressing apprentices; B: control group; BMI: body mass index; FMI: fat mass index; FFMI: fat-free mass index; WHR: waist-to-hip ratio; WHtR: waist-to-height ratio; SD: standard deviation.
Over half of the hairdressers (52.4%) declared themselves to be in excellent or in very good health. We rated as a very positive finding – 79.4% of students declared to perform sports and physical activity (n = 54) such as running (37%, n = 20), fast walking (29.6%, n = 16), skating (25.9%, n = 14) and a fitness (22.2%, n = 12). Self-rated perceptions of general health problems indicate symptoms of allergy (41.2%), high blood pressure (17.7%), asthma (11.8%) and eczema (5.9%). Hair spray and hair colorants were the most widely used cosmetic products. As much as 86.8% of respondents (n = 59) reported absence of air exhaust at the workplace and no one declared using a personal protective mask. On the other hand, using personal protective equipment such as gloves reported 92.6% of probands (n = 63). Permanent waves preparation (54.4%, n = 37) and use of hair spray (13.2%; n = 9) were identified as the most irritant activity. Self-rated perceptions of disorders during cosmetics procedure were reported as follows: sneezing (13.2%, n = 9), cough (5.9%; n = 4), eye irritation (2.9%; n = 2) and dyspnoea (1.5%; n = 1).
Analysis of first-morning-void urine sample detected metabolites of MEHHP, MEP, MnBP and MiBP phthalates in all samples, followed by metabolites MEOHP and MEHP (occurring in 97.06% and 86.76% of samples, respectively). Concentrations of urinary phthalate metabolites were positively skewed. From the three DEHP metabolites, MEHHP had the highest level ratio (64.54%), followed by MEOHP (23.09%) and MEHP (12.37%). The mean excretion ratio of MEHP to MEHHP and MEHP to MEOHP was 1:5.2 and 1:1.9, respectively. Descriptive statistics for urinary concentration of phthalate monoesters in control and study group are shown in Table 3. We found higher urinary concentration and higher median in hairdressing apprentices compared to control group (median and 95 percentiles) of MEHHP, MEOHP, MEHP, sum di-(2-ethyl-5-oxohexyl) phthalate (DEHP), mono-n-butyl phthalate (MnBP), but lower 95 percentiles of mono-isobutyl phthalate (MiBP). We found significantly higher urinary concentration only of MiBP (p ≤ 0.05) in hairdresser apprentices compared to control group (B).
Urinary concentrations of phthalates metabolites (ng/mL) in study group (A) and control group (B).
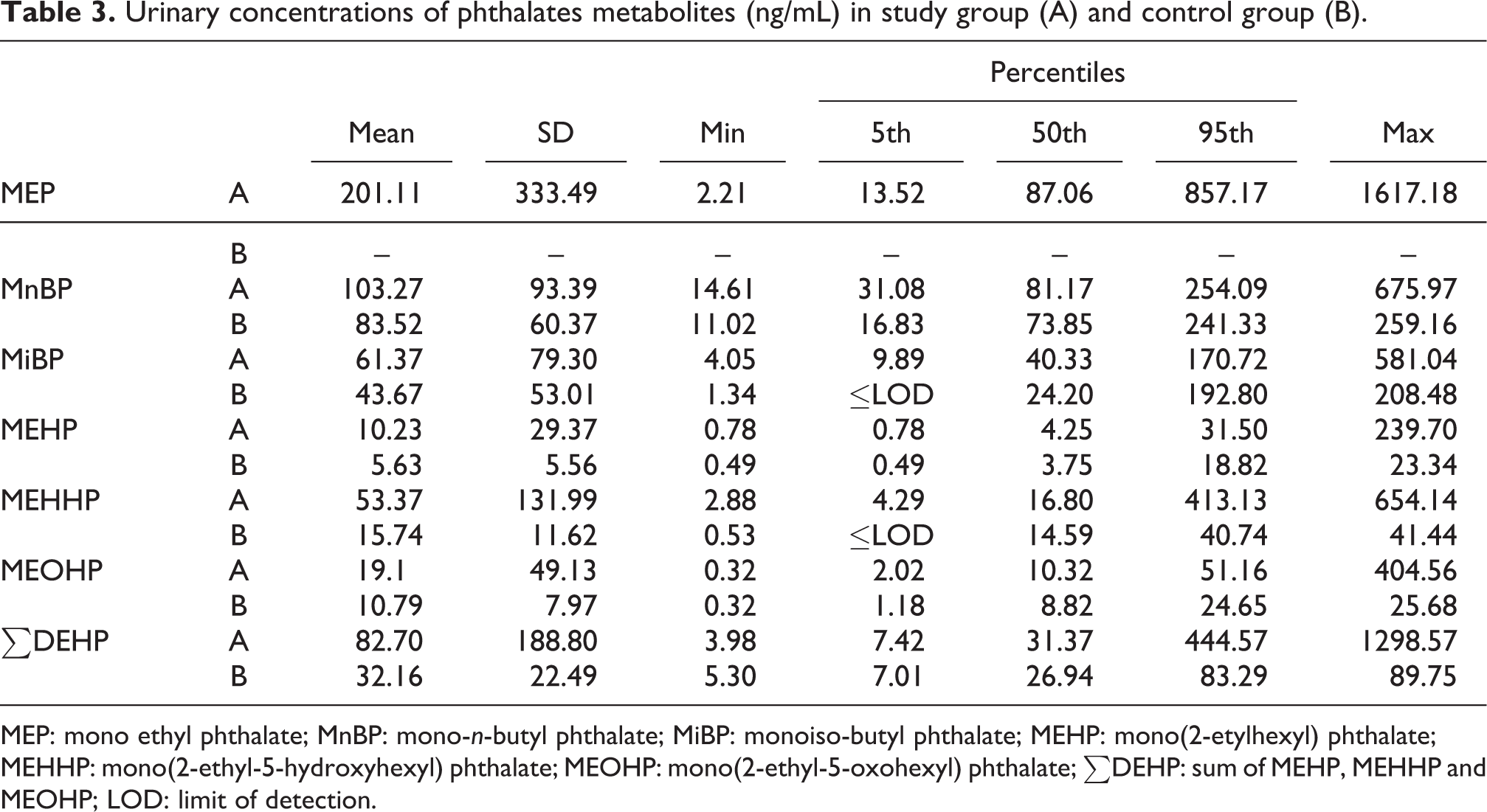
MEP: mono ethyl phthalate; MnBP: mono-n-butyl phthalate; MiBP: monoiso-butyl phthalate; MEHP: mono(2-etylhexyl) phthalate; MEHHP: mono(2-ethyl-5-hydroxyhexyl) phthalate; MEOHP: mono(2-ethyl-5-oxohexyl) phthalate; ∑DEHP: sum of MEHP, MEHHP and MEOHP; LOD: limit of detection.
With pulmonary functions, PEF and MVV, less than 10% of probands reached 100% of their optimal predicted values (PVs); on the other hand with FVC, FEV1 and vital capacity (VC), more than 73% of probands scored over 100% of their PVs. In Table 4, we show distribution of probands from studied and control group in score of pulmonary functions, with regard to reached percentage of PV.
Pulmonary function test results in study group (A) and control group (B).

FVC% of PV: % of predicted values of forced vital capacity; FEV1% of PV: % of predicted values of forced expiratory volume in 1 s; MVV% of PV: % of predicted values of maximum voluntary ventilation; VC% of PV: % of predicted values of vital capacity; PEF% of PV: % of predicted values of peak expiratory flow.
Interestingly, we found significantly higher values of pulmonary function of FVC (p = 0.05), FEV1 (p = 0.001) and VC (p = 0.001) in group A compared to control group (B).
In hairdressing apprentices, we also detected a decrease of FEV1/FVC under value of 70% and simultaneous decrease of percentage of PVs of PEF in 2.9% (n = 2) of subjects, which could be a symptom of chronic bronchitis. No associations were observed between sport activities and pulmonary function (Kruskal–Wallis test). The duration of the study period of hairdressing was associated only with MVV (χ2 = 5.76; p = 0.056).
Despite the relatively low average age of probands (17.7 ± 1.2 years, range: 16–20 years), alarmingly, almost half of them reported daily smoking (52.9%, n = 36) and, in addition, 16.2% of them were ex-smokers (n = 11). Moreover, more than 85% of probands (n = 58) are currently exposed to passive smoking and 57.4% of them (n = 39) were exposed in childhood. As expected, highest FEV1% of PV (110.08 ± 16.92), VC% of PV (126.26 ± 23.11) and MVV% of PV (84.51 ± 14.00) were observed in a subgroup of non-smokers. The Tiffeneau–Pinelli index (FEV1/FVC) reached its lowest real value in the subgroup of smokers (84.59 ± 6.84, p/y = 2.09 ± 2.61). Paradoxically, highest value of FVC% of PV was observed in subgroup of smokers (109 ± 12.77) and lowest PEF% of PV in non-smokers (82.96 ± 12.45; Table 5). Accordingly, we detected association between p/y index and dynamic pulmonary function (VC% of PV, Z = 3.54, p < 0.001; FEV1/FVC, Z = −2.3, p = 0.042 and FVC% of PV, Z = 2.04, p = 0.022) (Mann–Whitney U test in subgroups of smokers (p/y = 2.09 ± 2.61) and ex-smokers (p/y = 0.76 ± 0.75).
Results of pulmonary function test of hairdresser in relation to smoking habits.

FVC% of PV: % of predicted values of forced vital capacity; FEV1% of PV: % of predicted values of forced expiratory volume in 1 s; FEV1/FVC: ratio of forced expiratory volume in 1 s to forced vital capacity; MVV% of PV: % of predicted values of maximum voluntary ventilation; VC% of PV: % of predicted values of vital capacity; PEF% of PV: % of predicted values of peak expiratory flow; p/y index, pack year index.
We found significantly higher value of pulmonary function of VC (p ≤ 0.05) in non-smoker hairdressing apprentices compared to ex-smokers. Interestingly, we observed significantly higher value of VC (p ≤ 0.001), FVC (p ≤ 0.05) and FEV/FVC (p ≤ 0.05) in active smoking hairdressing apprentices compared to ex-smokers. We did not observe any differences in concentration of phthalates metabolites in relation to smoking habits.
Interestingly, in group A, we observed a positive association between phthalate metabolite MnBP and FFMI (r = 0.33; p = 0.006) and also between MnBP and both BMI (r = 0.22, p = 0.08) and WHtR (r = 0.21, p = 0.08) on border of statistical significance. In control group, any differences between phthalate metabolite and anthropometric parameters were observed.
We also found associations between concentration of metabolites MEHP (r = −0.27; p = 0.028), MEOHP (r = −0.26; p = 0.030), MEHHP (r = −0.25; p = 0.038), ΣDEHP (r = −0.29; p = 0.018) and VC and between MEHP (r = −0.24; p = 0.052) and %PV of FVC in group A. In control group (B), only associations between MEHHP (r = −0.46; p = 0.05) and ΣDEHP (r = −0.46; p = 0.05) and FEV1/FVC observed in females. Urinary MnBP concentration was associated with age (r = 0.28, p = 0.023) only in hairdressing apprentices. Interestingly, length of exposure was associated with concentration of MnBP (χ 2 = 6.70; p = 0.035), MEHHP (χ 2 = 7.14; p = 0.028) and MEP (χ 2 = 5.63; p = 0.06).
Association between concentration of phthalate metabolites and anthropometric parameters and pulmonary function is shown in Table 6.
Association between concentration of phthalate metabolites and anthropometric parameters and pulmonary function.

MEP: mono ethyl phthalate; MnBP: mono-n-butyl phthalate; MiBP: monoiso-butyl phthalate; MEHP: mono(2-etylhexyl) phthalate; MEHHP: mono(2-ethyl-5-hydroxyhexyl) phthalate; MEOHP: mono(2-ethyl-5-oxohexyl) phthalate; ∑DEHP: sum of MEHP, MEHHP and MEOHP.
a p ≤ 0.05.
We also observed several relationships between anthropometric and respiratory parameters in females from group A. Thus, we found a significant decrease of FEV1/FVC associated to WHtR (r = −0.25; p = 0.039), to WHR (r = −0.27; p = 0.031) and to FFMI (r = −0.31; p = 0.012). We also documented a significant increase of FVC% of PV in association to BMI (r = 0.28; p = 0.020), WHtR (r = 0.25; p = 0.039), FFMI (r = 0.34; p = 0.005) and FMI (r = 0.25; p = 0.05). In control group, decrease in FEV1/FVC associated to FFMI (r = −0.62; p = 0.05) and BMI (r = −0.45; p = 0.05) and increase in VC (r = 0.49; p =0.05) and FVC of PV (r = 0.46; p = 0.05) to FFMI were documented.
Discussion
It is generally acknowledged that hairdressing work is associated with increased occurrence of a range of health problems. 31 –33 In observational cross-sectional study based on analysis of occupational health risks in a group of hairdressing apprentices from Slovakia, we extended such observations in biomonitoring of phthalates and health-related outcomes.
Phthalate exposure can lead to many pathological effects depending on ontogeny stage of individual, levels and duration of exposure. The current self-rated perception of general health detected symptoms of allergy, asthma and eczema which is similar to results from Finland, 16 Turkey, 18 Sweden, 34 United Kingdom 33 and Rio de Janeiro. 35 In a study from Izmir province in Turkey, 35% of hairdressers reported also allergic complaints, 32 allegedly from a frequent use of hair colorants and hair sprays. Hairdressing apprentices from our cohort reported the bleaching powder and hair spray as the most irritant chemicals that provoke respiratory symptoms, which is in agreement with a hairdressers study from northeast Iran also reporting absence of air and only general window ventilation of salon. 28 Concerning individual protection measures, in contrast to our data on not wearing protective masks, some hairdressers reported less frequent use of gloves, however, use of protective clothing. 28,32 Lacking personal protective clothing or masks, documented in our study, was also stated in several studies on hairdressers from Europe 17,36 and Palestine. 37 Our finding of high prevalence of smoking (52.9% of smokers and 16.2% of ex-smokers) is consistent with international studies on hairdresser groups. 14,35,38 –40 Our data on pulmonary functions in hairdressing apprentices are comparable with those for a vocational training school from Paris. 38 Our results on PFT, however, rendered higher values for all tested functions when compared to a study from Iran 28 and also higher values for %FEV1 of PV, %FVC of PV but lower for %PEF of PV when compared to a study from New Zealand. 41 Also in a study on respiratory functions among female hairdressers in Palestine (mean age 28 years), 37 after excluding smokers, we observed lower values of FVC (3.31 ± 0.6), FEV1 (2.74 ± 0.4) and PEF (5.6 ± 1.2) than in our study (FVC: 3.9 ± 0.6; FEV1: 3.4 ± 0.4; PEF: 5.8 ± 0.9), however, the different age of probands has to be taken into account.
Significantly higher values of pulmonary function of FVC, FEV1 and VC in hairdresser apprentices could be explained by lower age of those probands (17.7 years) compared to control group (B, average age 23.8 years). We also hypothesize on potential bronchodilation effect of chemical substances in this type of work environment, but further study is needed.
Furthermore, our results indicate a relationship between body composition and the dynamics of the respiratory process, as BMI and WHtR were paradoxically positively associated with %FVC of PV which is in contradiction with some studies. 42 –44 Negative association between WHR and FEV1/FVC is consistent with data on association between waist girth and a decrease of FEV1/FVC. 45
Inter alia, pulmonary functions besides other factors are mainly determined by respiratory muscle strength. In our study, an increase of muscle mass (FFMI), but surprisingly also of fat mass (FMI), was positively associated with FVC% of PV showing that lung function is related to age- and gender-specific changes of body composition.
We assume that, we have rightly taken into consideration phthalate exposure as the main factor from potential risk factors with regard to everyday use of cosmetic products. Namely, phthalates with low molecular weight (DEP, DBP and DiBP) are commonly used as solvents and plasticizers in personal care products (e.g. perfume, shampoo, nail polish). 46,47 Under similar exposure scenario, a relationship between self-reported personal care product use and urinary phthalate metabolite of MEP and MBP concentrations was documented in pregnant females from the United States. 48 We confirmed exposure to these compounds contained in cosmetics, such as presence of MEP, MnBP and MiBP phthalate metabolites, was detected in all urine samples. Moreover, MnBP, MEP and MEHHP were positively associated with length of exposure in our study, which underscores potential health risks for lengthy exposed students and workers in this occupational environment. Exposure to phthalates may also occur through inhalation of cigarette smoke. In our study, no differences were observed in concentration of phthalate metabolites in relation to smoking habits, however, this observation requires a larger sample size and further study.
Long-chained phthalates (DEHP, DiDP and DiNP) are commonly used in building and construction materials, clothing and floorings, food package materials and so on. 49 , in children and adults products, including toys, plastic bags, gloves and shoes. 24,50 In our study, volumetric urinary concentrations of MEHHP (100% of samples), MEOHP (97.06% of samples) and MEHP (86.76% of samples) signalized high exposure to parental diester which may be health endangering. These data differ from excretion patterns of primary and secondary DEHP metabolites we found previously (MEHP:MEHHP – 1:9.7; MEHP:MEOHP – 1:5.9). 51 This difference can be explained by ethnic specificity in metabolism of DEHP.
We conclude from the current and previous biomonitoring studies 30,52,53 that the most exposed population to phthalates is in the plastic industry and next to it in the waste management occupations. In these groups, we observed higher, 50 and 95 percentile, values of volumetric urinary concentrations of MBP and MEHP, however, lower MEP in comparison with data on 12–19-year-old American general population. 54 Similarly, in the Canadian Health Measures Survey 2007–2009, 55 we observed lower volumetric urinary concentrations of MEP, MnBP, MEHP and 95 percentile of MEHHP, however, higher MEHP and MEOHP levels than in our study. For comparison, we present, in Table 7, an overview of the urinary phthalate metabolites concentration in human samples reported in various studies worldwide.
Concentration of phthalate metabolites (medians and 95 percentile, ng/mL) reported for human urine samples worldwide and in the present study.a
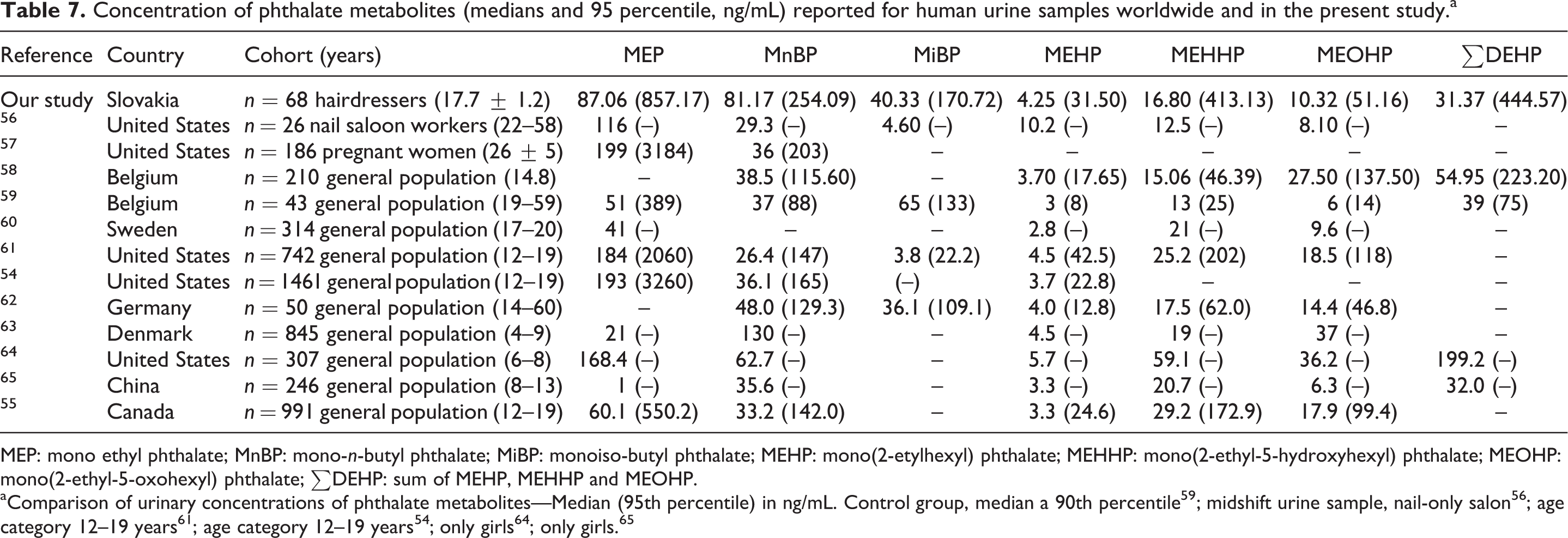
MEP: mono ethyl phthalate; MnBP: mono-n-butyl phthalate; MiBP: monoiso-butyl phthalate; MEHP: mono(2-etylhexyl) phthalate; MEHHP: mono(2-ethyl-5-hydroxyhexyl) phthalate; MEOHP: mono(2-ethyl-5-oxohexyl) phthalate; ∑DEHP: sum of MEHP, MEHHP and MEOHP.
In our study, the urinary concentration of MEHP, MEOHP, MEHHP and ∑DEHP was inversely associated with pulmonary function (%VC of PV and %FVC of PV) in agreement with questionnaires data on association of phthalate exposure from building materials or synthetic bedding with respiratory symptoms. 66 –68
Our current results differ from our previous data on waste management workers 52 where urinary concentration of MEHP was positively associated with FEV1/FVC, whereas in National Health and Nutrition Examination Survey (NHANES) III 69 MBP and MEP, but not MEHP, were associated with FVC, FEV1 and PEF in cohort of men only.
Endocrine disrupting effects of phthalates probably are related in an age/gender-specific way to endogenous hormones. Namely, it follows from our results that exposure to MnBP was associated in females on margin of statistical significance with fat distribution (BMI, WHtR), however, paradoxically also with an increase of FFMI (p = 0.006). Our findings are in contrast with data on association for boys >10 years of age only, while concentrations of MEHP, MEHHP and sum of DEHP metabolites were negatively associated with girls’ obesity. 65 Our results are also in contrast to those found in studies from the United States 70 and NHANES 71 where only MEP was associated with higher BMI and waist circumference, while MEHP was related to a decrease of BMI in females >12 years. Dose–response relationships were also seen between MEP and the sum of low molecular weight phthalates (MEP, MBP and MiBP) and waist circumference and BMI among overweight children. 64 On the other hand, partly in contrast with our results, in a study from Denmark, metabolites from DEP, DBP, DEHP and DiNP were negatively associated with absolute value of height, weight, BMI and age, while MnBP was positively associated with age. 63
It is possible that amount of adipose tissue has to be taken into account in phthalate biomonitoring because of their availability to accumulate in lipids and without apparent obesogenic effect of endocrine disruptor.
The differences in volumetric urinary concentration of phthalates reflect variability in occupational exposures where wide range in daily use of cosmetic products is common but also due to regional differences in exposure (Europe vs. United States), ethnicity, age as well as socio-economic status. The differences can also be related to the only first-morning-void urine sample, as short biological half-lives of these compounds are affecting variability in volumetric urinary concentrations during the day. Limitations of our study are related to self-reported health data and lack of environmental air data confirming exposures. As far as the authors know, this is the first occupational health study on hairdressing apprentices in Slovakia and even central Europe.
Conclusions
Because of the potential human toxicities of phthalates, internal dose measurements of phthalates are necessary for exposure and risk assessment. Our results indicate that haircare products are source of phthalate exposure and working as a hairdresser can be detrimental to health. We assume that occupational exposures to phthalates, estimated from urinary metabolites, may modify body composition and pulmonary function of hairdresser apprentices, however, the exact mechanism of these outcomes is still unclear and further study is needed. Installation of local exhaust ventilation can lead to a reduction of exposure, however, education aimed at proper use of personal protective equipment should be promoted.
Footnotes
Acknowledgement
We thank Michaela Földešiová for excellent technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the European Community under the project no. 26220220180 (Building Research Centre ‘AgroBioTech’) and (Environmental Aspects of Urban Area); supported by the Research & Development Operational Programme funded by the European Regional Development Fund and by project Vedecká grantová agentúra Ministerstva školstva, vedy, výskumu a športu Slovenskej republiky a Slovenskej akadémie vied (VEGA) no. V1/0042/12 (analysis of selected environmental factors in relation to potential health risks); and supported by Scientific Grant Agency of the Ministry of Education, Science, Research and Sport of the Slovak Republic.