
Abstract
Objectives:
This study uses pulmonary function tests and chest x-ray examinations to examine the relationship between toner-handling work and its health effects.
Methods:
The subjects were 1504 male workers in a Japanese toner and photocopier manufacturing company, in the age range from 19 to 50 years in 2003. Personal exposure measurements, pulmonary function tests, chest x-ray examinations, biomarker measurements, and a questionnaire about respiratory symptoms were conducted. The present study reports the results of pulmonary function tests and chest x-ray examinations conducted in the subjects, which includes a cross-sectional study on the toner handling and non-handling workers and a longitudinal study from 2003 to 2008.
Results:
Few significant findings were suspected to be caused by toner exposure found in pulmonary function indices in both the cross-sectional and longitudinal studies. Any obvious fibrotic findings in chest x-ray findings related to the toner exposure could not be found out.
Conclusion:
No evidence of adverse effects on pulmonary function indices and chest x-rays was present in the toner-handling workers as compared to the nonspecifically exposed workers. Although the toner exposure concentration is quite low in the current well-controlled working environment, even among the toner-handling workers, we would like to continue this study in the future to verify the toner exposure health effects.
Keywords
Introduction
In 1994, siderosilicosis caused by toner was reported in the journal The Lancet 1 for the first time; since then there have been several reports of granulomatous pneumonia and other diseases associated with toner exposure. 2,3 Carbon black, one toner component, was reevaluated as a Group 2B carcinogen in 1996 by the International Agency for Research on Cancer based on an experiment on rodents. 4 However, most studies were case reports of specific diseases, the acute effects of uncontrolled exposure and animal experiments with artificial and extremely high exposure concentrations, rendering the information in these studies insufficient to verify the actual risk of carbon black or toner. Recently, concerns have been raised about indoor air pollution in offices associated with particulate matter (PM), ozone, and volatile organic compounds emitted from printers. Studies have been conducted to clarify the relationship between office machines such as printers and photocopiers and indoor environments 5,6 to identify the chemical composition of printer emissions 7,8 and to measure the emitted PM while printing a sheet of paper or over a period of time. 9 –11 In vitro 12 and in vivo 13 –15 experiments have been performed to extrapolate emission effects from printers on humans. Concerns also exist about the health effects on office workers in association with emissions generated from printers and photocopiers. The Federal Institute for Risk Assessment in the Federal Republic of Germany conducted a health assessment of potential risks from printer emissions and issued its final report 16 on a toner study in 2008. A study on respiratory symptoms in copy center workers in Taiwan 17 was also reported. An association between PM and respiratory effect in healthy subjects has not been clearly established in epidemiological studies. Recently, some studies such as “a study on pulmonary deposition and retention of ultrafine carbon particles 18 and a study on acute change in respiratory function” were carried out. 19 However, these reports were cross-sectional studies and lacked sufficient objective measures to evaluate the health impact of toner on humans; hence, a well-designed epidemiological study was needed. We started a 10-year prospective cohort study to investigate the relationship between toner exposure and its effects on human health in a Japanese toner and photocopier manufacturing company. The results of the baseline survey have been published. 20,21 This report is the result of a 5-year follow-up from 2003 to 2008. We conducted a cross-sectional analysis and a longitudinal analysis. The results concerning biomarker measurements were reported elsewhere. This study uses pulmonary function tests and chest x-ray examinations to examine the relationship between toner dust exposure and its health effects.
Subjects and methods
The present study was conducted in accordance with the survey guidelines 22 proposed by the scientific advisory group organized for the Japan Business Machine and Information System Industries Association (JBMIA), which were drawn up to validate survey methods.
Subjects
The health supervisors at each plant were asked to select workers to participate in the survey according to the JBMIA guidelines because of their understanding of the occupational histories, work situations, and work content in their plants. They selected 1504 male workers aged from 19 to 50 years as on 1 April 2003. The subjects consisted of 768 toner-handling workers and 736 non-handling workers as controls. The toner-handling workers routinely handled toner particles at work. The categories of the toner-handling work were identified as toner development, toner manufacturing, photocopier development, toner and photocopier recycling, and customer service. The non-handling workers worked at their desk in offices. The controls were selected from the same plants as the toner-handling workers to eliminate differences of potential confounding factors such as living conditions, environmental factors, and socioeconomic status.
Measurement of toner exposure level
Several workers in each work category were randomly selected and personal exposure measurements were conducted. The Working Environment Measurement Standards in Japan were partly amended in 2004, 23 and the respirable dust definition was revised from ≤7 to 4.5 µm. Along with this change, we changed the personal dust sampler in 2005. A filter holder for a personal total and respirable dust sampler, model PS-43, Roken type (flow rate 1.5 L min−1, Sibata Scientific Technology Ltd, Nagano, Japan) with glass fiber filters, polytetrafluoroethylene (PTFE) binding, T60A20 type φ25 mm (Tokyo Dylec Corporation, Tokyo, Japan) was used until 2004, and a filter holder for a personal dust sampler, model NWPS-254 (flow rate 2.5 L min−1, Sibata Scientific Technology Ltd) with glass fiber filters, PTFE binding, T60A20 type φ25 mm (Tokyo Dylec Corporation) has been used since 2005. The subjects wore the data recorder of the personal dust sampler on the left part of their waists and the detector around their necks. Respirable dust trapped in the filter was measured with an electric balance, and the measured quantity was divided by the total aspirated air volume to calculate the respirable dust concentration.
Pulmonary function tests
The pulmonary function tests were performed with a pneumotach-type spirometry measuring unit, for example, Microspiro HI-701 and Microspiro HI-801 (Chest Corporation, Tokyo, Japan), recommended by the JBMIA survey guide which met the standards stipulated by the American Thoracic Society. 24 The following indices were measured: vital capacity (VC), forced expiratory volume in 1 s (FEV1.0), maximal expiratory flow at 25% forced VC (V 25), and peak expiratory flow rate (PEFR). Using the predicted formula for Japanese adult males described by the Japanese respiratory society, which is VC(l) = 0.045 × height (cm) − 0.023 × age − 2.258, FEV1.0(l) = 0.036 × height (cm) − 0.028 × age − 1.178, and V 25(l s−1) = 0.021 × height (cm) − 0.031 × age − 0.073, 25 we calculated predicted VC (%VC), predicted FEV1.0 (%FEV1.0), and predicted V25 (%V25). Subjects were asked to take the pulmonary function test three times and the best value was adopted for analysis. In order to obtain appropriate and consistent results, the examinations were conducted in one institution with trained examiners throughout this study.
Chest x-ray examinations
Chest x-ray examinations should be conducted under standardized procedures that would be internationally comparable; the standard method specified in the Pneumoconiosis Law 26,27 was used. Readers with sufficient experience in the radiographic diagnosis of pneumoconiosis read all x-ray films twice. Radiologic interpretations were conducted based on the International Labour Organization (ILO) international classifications of pneumoconiosis radiographs in the 2000 revised edition. 28 The obtained x-ray films were electronically stored using a film digitizer.
Statistical analysis method
For pulmonary function indices, data analyses focused on the relationship between toner-handling work and health effects. We considered smoking status, allergic diseases (asthma, allergic rhinitis, and atopic dermatitis), age, and body mass index (BMI) as confounders. In a cross-sectional study, analysis of variance (ANOVA) was used to examine the association of toner exposure with annual pulmonary function indices: %VC, %FEV1.0, and %V25. We also conducted multivariable regression analysis using toner exposure level and confounders as explanatory variables to control for the potential confounding effects, and VC, FEV1.0, V25, and PEFR as response variables. We identified the combination of explanatory variables using stepwise procedure. In the longitudinal analysis, a correlation in repeated data for each subject was a concern in the cohort study. Generalized estimating equations (GEE) 29 were applied to evaluate the magnitude of toner exposure on pulmonary function: VC, FEV1.0, V25, and PEFR. Subjects were categorized into three BMI categories: <18.5, ≥18.5 and <25.0, and ≥25.0 30 and four age categories: ≤29, 30–39, 40–49 and ≥50. Smoking status, asthma, allergic rhinitis, atopic dermatitis, age, and BMI categories were added to the model as potential confounders. The values of p < 0.05 were considered statistically significant. We conducted all analyses using SPSS20.0J (IBM) for Windows.
Ethical approval
This study was approved by the ethics committee of the University of Occupational and Environmental Health, Japan (UOEH; No.03-32 10 December 2003). Written informed consent was obtained from each individual participating in the study.
Results
Subject demographics
Among 1504 subjects, we followed up 1208 workers with pulmonary function tests and 1212 workers with chest x-ray examinations over 5 years. The follow-up rates of the toner-handling and control groups were 82.9% (637/768 subjects) and 77.6% (571/736 subjects), respectively, for pulmonary function tests and 83.3% (640/768 subjects) and 77.7% (572/736 subjects), respectively, for chest x-ray examinations. We obtained the reasons in writing when participants withdrew from the study and confirmed that no subjects withdrew due to specific respiratory diseases such as pneumoconiosis, chronic obstructive pulmonary disease, and lung cancer. During the study period, five toner-handling workers and one non-handling worker died of cerebrovascular attack, ischemic heart disease, and other diseases. The characteristics of the subjects in the first survey are shown in Table 1. In 2003, the mean age of the toner-handling group was 38.2 and that of the control group was 39.1. For physical constitution, the non-handling workers were slightly taller and heavier than the toner-handling workers. The smoking rate was higher in toner-handling workers than in non-handling workers.
Characteristics of subjects in the first survey.a

BMI: body mass index; SD: standard deviation.
aTwo subjects were excluded from the comparison of age and physical indices because they did not examine the pulmonary function tests. Also, 12 subjects were excluded from the comparison of smoking habit because they did not examine the questionnaire or forget to fill in the smoking habit.
Toner exposure measurement
To compare with the threshold limit value (TLV) as defined by the American Conference of Governmental Industrial Hygienists (ACGIH), which is based on an allowable exposure averaged over a normal 8-h workday or 40-h workweek, an 8-h time weighted average (TWA8h) was calculated with the formula described in the guidelines for evaluating worker exposure to hazardous substances. 31 Table 2 shows the mean, SD, median, quartile 1, and quartile 3 of calculated TWA8hs. There was a widespread in the means of the 1st survey from 0.019 mg m−3 in toner manufacturing to 0.989 mg m−3 in toner and photocopier recycling. Even though the highest value of 0.989 mg m−3 was well below the acceptable value of 3.0 mg m−3 recommended by the ACGIH, the TLV-TWA of particles not otherwise specified 31 was still approximately 50 times higher for the latter group. After reviewing the results of the 1st survey, the company and workers took measures to reduce exposure. The measures included tool and equipment modification, better safety rule enforcement, and changes in handling materials and work procedures. As the surveys proceeded, TWA8hs, especially in toner and photocopier recycling and toner manufacturing, were reduced: the differences among the toner-handling work categories almost disappeared. The mean of desk work measured as a control was 0.012 mg m−3 (SD: 0.002), and median of deskwork in the office was 0.012 mg m−3 (quartile 1: 0.009 mg m−3 and quartile 3: 0.013 mg m−3). Based on the results of personal exposure measurements, we classified the toner-handling workers into two groups by the exposure levels. The high exposure group included toner manufacturing and toner and photocopier recycling, while the low exposure group included toner development, photocopier development, and customer service.
Personal exposure measurement in each toner-handling work category.

Work environment measurements were also implemented in the same areas where personal exposure measurements were conducted. The dust levels throughout the follow-up period in all the areas were below the control level, which is 3.0 mg m−3 as described in the working environmental measurement standards. 32
Pulmonary function tests in the cross-sectional study
To evaluate the differences among the high exposure group, the low exposure group, and the control group, %VC, %FEV1.0, and %V\vskip-2pt\hskip -3pt \dot 25 were examined to use ANOVA. We showed the ANOVA results in Table 3. There were no pulmonary function indices decreasing due to toner exposure. The statistical significances were observed in %V25 in the third and fourth surveys; contrary to expectations, the high exposure group showed significantly greater values than the control group.
Pulmonary function indices among high exposure group, low exposure group and non-exposed workers.

VC: vital capacity; FEV1.0: forced expiratory volume in 1 s; %V25: maximal expiratory flow at 25% forced VC.
a p Value of analysis of variance.
bLow-exposure group.
cHigh-exposure group.
d p Value < 0.01.
e p Value < 0.05.
We also show the multivariable regression analysis results in Table 4; only the significant explanatory variables are shown. Both the high and low exposure levels do not show any significant effects on any pulmonary function indices decreasing. Current smokers show a consistent tendency for decreased pulmonary function indices. Age and asthma have negative effects on most of the pulmonary function indices.
The results of multiple linear regression analysis.a

VC: vital capacity; FEV1.0: forced expiratory volume in 1 s; %V25: maximal expiratory flow at 25% forced VC; PEFR: peak expiratory flow rate; BMI: body mass index; SE: standard error.
aWe used the following explanatory variables: the high exposure level, low exposure level, current smoker, former smoker, asthma, allergic rhinotos, atopic dermatitis, age and BMI and showed only variables with significant effects in the table.
bStandardized coefficient.
Pulmonary function tests in the longitudinal study
The GEE results are shown in Table 5. If the toner exposure level significantly affected pulmonary functions, the tendency to increase or decrease is indicated in the table with vertical arrows (↑, ↓). Without adjusting confounders, some pulmonary functions were affected by toner exposure increasing compared with non-handling workers. The crude odds ratio and 95% confidence intervals (CI) for the high VC exposure level was 1.20 (95% CI = 1.02–1.42); the crude odds ratio and 95% CI for the high FEV1.0 exposure level was 1.21 (95%CI = 1.07–1.38); the crude odds ratio and 95% CI for the high V\vskip-2pt\hskip -3pt \dot 25 exposure level was 1.25 (95%CI = 1.07–1.47); and for the low exposure levels the values were 1.07 (95% CI = 1.01–1.14). After adjustment for confounders, none of the pulmonary function indices were significantly affected by either the high or low exposure levels. Although inhaling fine particles causes pulmonary function decline, the GEE results did not indicate this. Among confounders, asthma, and age category were significantly associated with pulmonary function indices decreasing. Smoking status, BMI, allergic rhinitis, and atopic dermatitis were not associated with pulmonary function indices.
The results of GEE for respiratory function indices.a
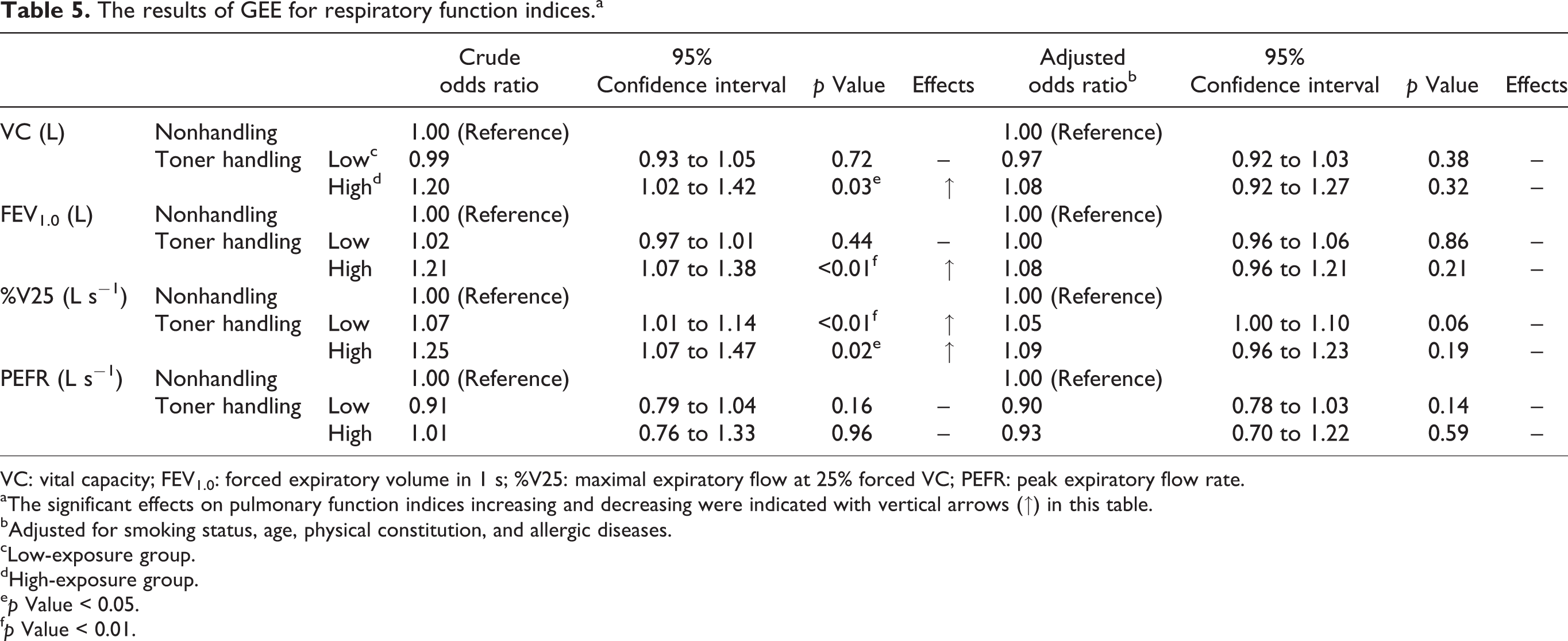
VC: vital capacity; FEV1.0: forced expiratory volume in 1 s; %V25: maximal expiratory flow at 25% forced VC; PEFR: peak expiratory flow rate.
aThe significant effects on pulmonary function indices increasing and decreasing were indicated with vertical arrows (↑) in this table.
bAdjusted for smoking status, age, physical constitution, and allergic diseases.
cLow-exposure group.
dHigh-exposure group.
e p Value < 0.05.
f p Value < 0.01.
Chest x-ray examinations
Concerning the chest x-ray examinations, a total of seven subjects had chest x-rays classified into category 1/0 according to the ILO international classification of pneumoconiosis radiographs through the follow-up period: three subjects in the low exposure group and one subject in the control group in the first survey, one subject in the low exposure group and one subject in the control group in the second survey, and one subject in the low exposure group in the fifth survey. Klepczynska-Nystrom et al. 18 reported that about 95% of ultrafine carbon particles were retained in the lung 7 days after exposure. If toner particles are harmful to human lung, the higher the exposure concentrations are, the severer the effects may be on chest x-rays. However, a clear relationship was not found between the toner exposure concentrations and chest x-ray classifications.
Discussion
In this study, we examined the pulmonary functions and chest x-rays over 5 years and compared the results between toner-handling workers and non-handling workers as controls. Few significant findings suspected to be caused by toner exposure were found in the pulmonary function indices and chest x-rays. The results of this study suggest that exposure concentrations are lower in general offices than toner-handling plants, and there is little feasibility that toner exposure will reduce pulmonary functions and cause chest x-ray abnormalities, particularly related to pneumoconiosis.
Many studies on the short-term effects of PM on health have focused on mortality and hospital admissions. Some studies setting endpoints such as respiratory and cardiovascular symptoms, or changes in pulmonary function, have been conducted on healthy subjects, but few studies have investigated the relationship between the long-term effects of PM and pulmonary functions in healthy subjects as our study does.
Some in vitro and in vivo studies have reported histopathological toner effects. Konczol et al. 33 showed that exposure to toner in human epithelial A549 lung cells causes oxidative stress through inducting reactive oxygen species (ROS) and that ROS may trigger genotoxic effects and activate pro-inflammatory pathways. Morimoto et al. 34 reported that chronic effects of toner particles on rat lungs were found as the small fibrotic foci increased in a dose-dependent manner and were not associated with carcinogenesis. Konczol et al. mentioned that when considering possible effects on human health, the concentrations used in their in vitro study must be considered because those in their study were too high to reflect realistic exposure scenarios. In this study, we did not find any obstructive impairment due to lung fibrosis in pulmonary function tests, inflammation, or tumor images. Considering the results, noting the possibility of lung inflammation, fibrosis, and cancer is necessary.
The TLV of TWA8h of insoluble respirable particulates determined by the ACGIH 31 was 3.0 mg m−3 and that of carbon black was 3.5 mg m−3. The study results were remarkably low compared with the acceptable level of the ACGIH, even for the highest value in the first survey. The results of personal exposure measurements suggest that, in current work conditions with appropriate work environment control and work practice management, inhalation of a large amount of toner dust may not occur. In this study, we were unable to evaluate the health effects due to high toner exposure concentrations, such as exceeding the TLV of the ACGIH because such severe cases were not observed. We could only examine extremely low toner exposure concentrations. Under this limiting condition, we classified toner-handling group into two groups, that is, the high exposure group and the low exposure group and tried to clarify the relationship between the toner exposure concentrations and the degree of the health effect. We could not find any significant health effects from toner exposure regardless of the exposure concentrations.
As an affective factor on pulmonary functions, severe obesity causes obstructive lung disorder. 35 The control group had a greater BMI than the toner-handling group in this study, and we considered BMI as a possible confounder. However, BMI was almost the same as the mean of the national population data of the same generation in Japanese males in 2003 36 and was assessed as not being associated with pulmonary function indices in multivariable regression. We therefore considered the differences of physical indices between toner-handling and control groups as negligible.
Smoking develops obstructive pulmonary disorders and reduces pulmonary functions. 37 In our data, the effects of smoking were observed in the cross-sectional study but not in the longitudinal study. Smokers who felt uncomfortable with their respiratory symptoms such as coughing, phlegm, and breathlessness and who had difficulty with physical activity may have already quit smoking. Although decline in respiratory function was not the only reason, the current smoking rate actually decreased for both the toner-handling and control workers throughout the follow-up period: 49.1% in the 1st survey and 41.6% in the 6th survey for all subjects. We will examine the effect of smoking for much longer periods and the interaction between toner exposure and smoking in the future.
Concerning allergic diseases, pulmonary function indices significantly decreased from asthma. However, most subjects with asthma were under medical treatment or in remission; few subjects had severe wheezing and dyspnea. It was unlikely that pulmonary function indices were exacerbated by asthma symptoms; personal factors such as smoking status were suspected. Although there was a study reporting that toner exposure will cause occupational asthma, 38 no significant differences existed in point prevalence of asthma in our study in the 1st survey: 9.4% in the high exposure group, 9.8% in the low exposure group, and 9.8% in the control group (p value of χ 2 test = 0.99). Further study will be needed to validate the relationship between asthma, pulmonary function indices, toner exposure, and other personal factors.
Nakadate et al. 39 suggested that cumulative toner exposure affects pulmonary functions. Our study was limited concerning this because personal exposure measurements were not conducted before 2003 and comprehending past exposure was too difficult. We have obtained information of the cumulative work period. Using that, we would like to construct an occupation exposure matrix deduced from past work environment measurements and occupational records for further analysis.
For chest x-rays, we only read the annual films for this report; we will examine the films of each subject of the first and the last survey to compare them in a future study.
Conclusion
In conclusion, no evidence of unfavorable effects on pulmonary function indices and chest x-rays was present in the toner-handling workers as compared to the nonspecifically exposed workers, despite some sporadically significant differences. As no other reports of a longitudinal epidemiological study regarding toner dust exposure exist, this report significantly contributes to the research on this topic. Although the toner exposure concentration may be quite low, even in the toner-handling workers in the current well-controlled working environment, we would like to continue this study in the future to verify the health effects of the toner exposure.
Footnotes
Acknowledgments
The authors wish to acknowledge occupational physician Dr K Kohno, Professor of the Graduate School of University of Human Arts and Science, Ms Y Matsuda, an occupational health nurse, and Mr Y Harada, a health supervisor of Fuji Xerox Co., Ltd, Tokyo, Japan, for their valuable assistance during this study. We would also like to express our appreciation to Kanagawa Health Service Association, SRL Inc. and OHG Institute Co. Ltd for the assistance of their laboratories.
Conflict of interest
In order to avoid any bias in the results, this study was based on the Japan Business Machine and Information System Industries Association guidelines and was undertaken according to the requirements of the ethical committee of University of Occupational and Environmental Health (UOEH), Kitakyushu, Japan, and the fairness of the study was clearly stated in the contract between Fuji Xerox Co. Ltd and UOEH.
Funding
Fuji Xerox Co. Ltd provided the funds for the present study to University of Occupational and Environmental Health (UOEH), Kitakyushu, Japan, according to the research contract.