
Abstract
Objectives:
This study examines the relationship between toner exposure and its health effects in terms of biomarkers which are known to assess the damages to humans caused by toxic material exposure.
Methods:
The subjects were 1504 male workers aged below 50 in 2003 in a Japanese toner and photocopier manufacturing company. Personal exposure measurements, pulmonary function tests, chest X-ray examinations, biomarker measurement, and a questionnaire about respiratory symptoms were conducted. We will report about biomarker measurement in this study. Cross-sectional survey studies and a longitudinal study from 2003 to 2008 were conducted.
Results:
Few significant findings were associated with the toner exposure in both the cross-sectional and the longitudinal studies. The higher toner exposure concentrations did not induce effects on increasing biomarkers.
Conclusion:
There was no evidence of excessive inflammatory, allergic, or oxidative stress reaction in toner-handling workers as compared to non-handling workers, despite some sporadically significant findings. There are no other reports of a longitudinal epidemiological study with regard to toner exposure; this report significantly contributes to toner exposure literature. Although in the current well-controlled working environment, the toner exposure concentrations are quite low; further studies are needed to completely understand the health effects toner may have, however small they may be.
Introduction
In 1994, a case of siderosilicosis caused by toner exposure was reported for the first time in the journal The Lancet 1 ; since then there have been several reports on pneumoconiosis associated with toner exposure. 2,3 In 1996, the International Agency for Research on Cancer (IARC) reevaluated carbon black, which is a toner component, as belonging to Group 2B, which is possibly carcinogenic to humans, based on experiments on rats. 4 As most reports were case reports of specific diseases, the acute effects of uncontrolled exposure and animal experiments with artificially extremely high exposure concentrations, the information in these studies was insufficient to verify the actual risk of carbon black and toner. Recently, concerns about indoor air pollution in offices from exposure to particulate matter, ozone, and volatile organic compounds emitted from printers have been raised. Some studies have been conducted to examine the relationship between office machines such as printers and photocopiers and indoor environments 5,6 to identify the chemical composition of emissions from different types of printers 7,8 and to measure the emitted particulate matter from printing a sheet of paper for over a period of time. 9 –11 In vitro 12 and in vivo 13 –15 experiments had been performed in order to assess the cytotoxicity of toner and emissions from printers. Concerns also exist about the allergic effects on office workers working near printers. The Federal Institute for Risk Assessment in the Federal Republic of Germany conducted a health assessment of potential risks from printer emissions and issued its final report 16 about a toner study in 2008. A study on respiratory symptoms in copy center workers in Taiwan 17 was also reported. As the past reports were cross-sectional studies and in vitro or in vivo experiments, the scientific evidence to evaluate the magnitude of health effects on humans from the toner exposure and emissions was insufficient. An epidemiological well-designed study on humans was needed; we started a 10-year cohort study to investigate the relationship between toner exposure and its health effects on toner-handling workers. We will report the results of a 5-year follow-up from 2003 to 2008. We conducted a cross-sectional analysis and a longitudinal analysis, significantly contributing to toner exposure research. This study examines the health effects due to toner exposure in terms of inflammatory, allergic, and oxidative stress markers.
Subjects and methods
This study was conducted in accordance with the survey guideline 18 proposed by the scientific advisory group organized for the Japan Business Machine and Information System Industries Association (JBMIA), which was drawn up to validate the survey methods.
Subjects
The subjects were 1504 male workers aged below 50 on 1 April 2003 in a Japanese toner and photocopier manufacturing company. At the start of this study, the subjects consisted of 768 toner-handling workers and 736 non-handling workers as the controls. The occupational hygienists at each plant were asked to select workers to participate in the study according to the JBMIA guideline because of their understanding of occupational histories, work situations, and work content. The toner-handling and the non-handling groups were categorized depending on their work at the start of this study. The toner-handling workers were engaged in the five work categories of toner development, toner manufacturing, photocopier development, toner and photocopier recycling, and customer service, and the non-handling workers were engaged in desk work in the offices. The controls were selected from the same plants to eliminate the differences of potential confounding factors such as living conditions, environmental factors, and socioeconomic status as much as possible.
Measurement of toner exposure level
Several workers in each work category were randomly selected and personal exposure measurements were conducted based on the Working Environment Measurement Standards. In Japan, the definition of respirable dust in this standard was revised from ≤7 to 4.5 µm in 2004. 19 Along with this revision, the personal dust sampler was changed from 2005, which was when the third survey was conducted. Each subject wore the data recorder of the personal dust sampler on their waist to the left and the detector around their neck. Respirable dust trapped on the filter was measured with an electric balance; the measured quantity was divided by the total aspirated air volume to calculate the respirable dust concentration. In order to compare with the threshold limit value as defined by the American Conference of Governmental Industrial Hygienists, which is based on an allowable exposure averaged over a normal 8-h workday or 40-h workweek, an 8-h time weighted average (TWA8h) was calculated by the formula described in the guidelines for evaluating worker exposure to hazardous substances. 20
Inflammatory, allergic, and oxidative stress markers
The following seven biomarkers were measured in this study: C-reactive protein (CRP), immunoglobulin E (IgE), interleukin-4 (IL-4), interleukin-6 (IL-6), interleukin-8 (IL-8), and interferon-γ (IFN-γ) in serum and 8-hydroxy-2′-deoxyguanosine (8-OHdG) in urine. To have an adequate quality of data of biological indices throughout the 10-year cohort study, we selected two institutions, SRL Inc. (Japan) and OHG Institute Co. Ltd (Kitakyushu, Fukuoka, Japan), based on quality management standards and entrusted the work to them. CRP, IgE, IL-4, IL-6, IL-8, IFN-γ, and 8-OHdG were examined using latex immunoagglutination assay, fluorescence enzyme immunoassay, chemiluminescent enzyme immunoassay, chemiluminescent enzyme immunoassay, enzyme-linked immunosorbent assay, enzyme immunoassay, and high-performance liquid chromatography in order. Limits of detection (LOD) of SRL Inc. were 0.02 mg/dl in CRP, 5.00 IU/ml in IgE, 2.00 pg/mL in IL-4, 0.20 pg/mL in IL-6, 2.00 pg/mL in IL-8, and 0.10 IU/mL in IFN-γ. The 8-OHdG concentration in spot urine was unstable, even for individuals, depending on the activity in day time, the time to sample the urine and other factors. Although 24 h urine collection analysis was considered the most appropriate, the method was impractical for this study. We selected assessing 8-OHdG with creatinine correction (8-OHdG/Cre) which is considered a good method to obtain stable data.
Statistical analysis method
Data were analyzed focusing on the relationship between toner exposure and its health effects. The undetectable value in each marker was assigned to the LOD/2 value to analyze. The distribution of the values of each marker showed skewness and high kurtosis. The p-values of Shapiro–Wilk normality analysis of each biomarker were <0.05, with 0.05 considered statistically significant, and the Kruskal–Wallis test was used in the cross-sectional analysis. In this study, the biomarkers of each subject were examined annually. A correlation in repeated measures data for each subject was a concern in the cohort study, so generalized estimating equations (GEE) 21 were applied in the longitudinal analysis. Each biomarker was used as a dependent variable, and the exposure concentration categories of high exposure group, low exposure group and non-toner handling group, current smokers, former smokers, and never smokers, with or without asthma, with or without allergic rhinitis, with or without atopic dermatitis, and age were used as independent variables. The hypothesis of this analysis was that the higher the exposure concentration, the greater the each biomarker would be. All analyses were performed with SPSS20.0J (IBM) for Windows.
Ethical approval
This study was conducted with the approval of the ethics committee of University of Occupational and Environmental Health, Japan (No.03-32 10 December 2003). Written informed consent was obtained from each individual in the study.
Results
Among 1504 subjects, we were able to follow the inflammatory, allergic, and oxidative stress markers of 1212 workers over 5 years. The follow-up rates of the toner-handling and the non-handling groups were 83.3% (640/768 subjects) and 77.7% (572/736 subjects), respectively. We obtained documentation when subjects left the study and confirmed that no subjects left the study due to specific respiratory diseases such as pneumoconiosis, chronic obstructive pulmonary disease, or lung cancer. However, five toner-handling workers and one non-handling worker died of cerebrovascular attack, ischemic heart disease, and other illnesses during the follow-up period. The characteristics of the subjects in the first survey are shown in Table 1. The mean age was 38.2 years in the toner-handling group and 39.1 years in the non-handling group. There were no significant differences in the morbidity of asthma, allergic rhinitis, and atopic dermatitis between the two groups. With regard to smoking, the smoking rate tended to be higher in the toner-handling group than in the non-handling group.
Characteristics of subjects in the first survey.a

a12 subjects were excluded from the comparison of smoking habit because they did not examine the questionnaire or forget to fill in the smoking habit.
b p Value of Student’s t test and χ2 test.
c p < 0.05.
Measurement of toner exposure level
There was a wide spread in the mean TWA8 h in the first survey shown in Figure 1. There was a wide spread in the results of the first survey from 0.019 mg/m3 in photocopier development to 0.989 mg/m3 in toner and photocopier recycling. As the survey proceeded, the differences among the toner-handling work categories decreased. Based on the results of personal exposure measurements, we classified the toner-handling workers into two groups by exposure concentrations. The high exposure group included toner manufacturing and toner and photocopier recycling; the low exposure group included toner development, photocopier development, and customer service.

Personal exposure measurement in each toner-handling work category.
Inflammatory and allergic markers
Cross-sectional study
In the 1st survey, 189 samples inappropriately handled or transported were eliminated from the analysis because of unreliability. Table 2 shows the median of inflammatory, allergic, and oxidative stress markers. While statistically significant differences among the high exposure group, low exposure group, and non-handling group were observed in CRP in the 5th survey, IL-4 in the 1st, 3rd, and 4th surveys, IL-6 in the 1st survey, IL-8 in the 5th survey, IFN-γ in the 1st and 3rd surveys, and 8-OHdG/Cre in the 3rd survey, no consistent tendencies related to the toner exposure concentrations were observed.
Comparison of inflammatory, allergic, and oxidative stress markers among the high-exposed group, the low-exposed group, and the non-exposed workers.

CRP: C-reactive protein; IgE: immunoglobulin E; IL: interleukin; IFN: interferon; 8-OHdG/Cre: 8-hydroxy-2′-deoxyguanosine with creatinine correction.
a p Value of Kruskal–Wallis test.
b p < 0.05.
c p < 0.01.
Longitudinal study
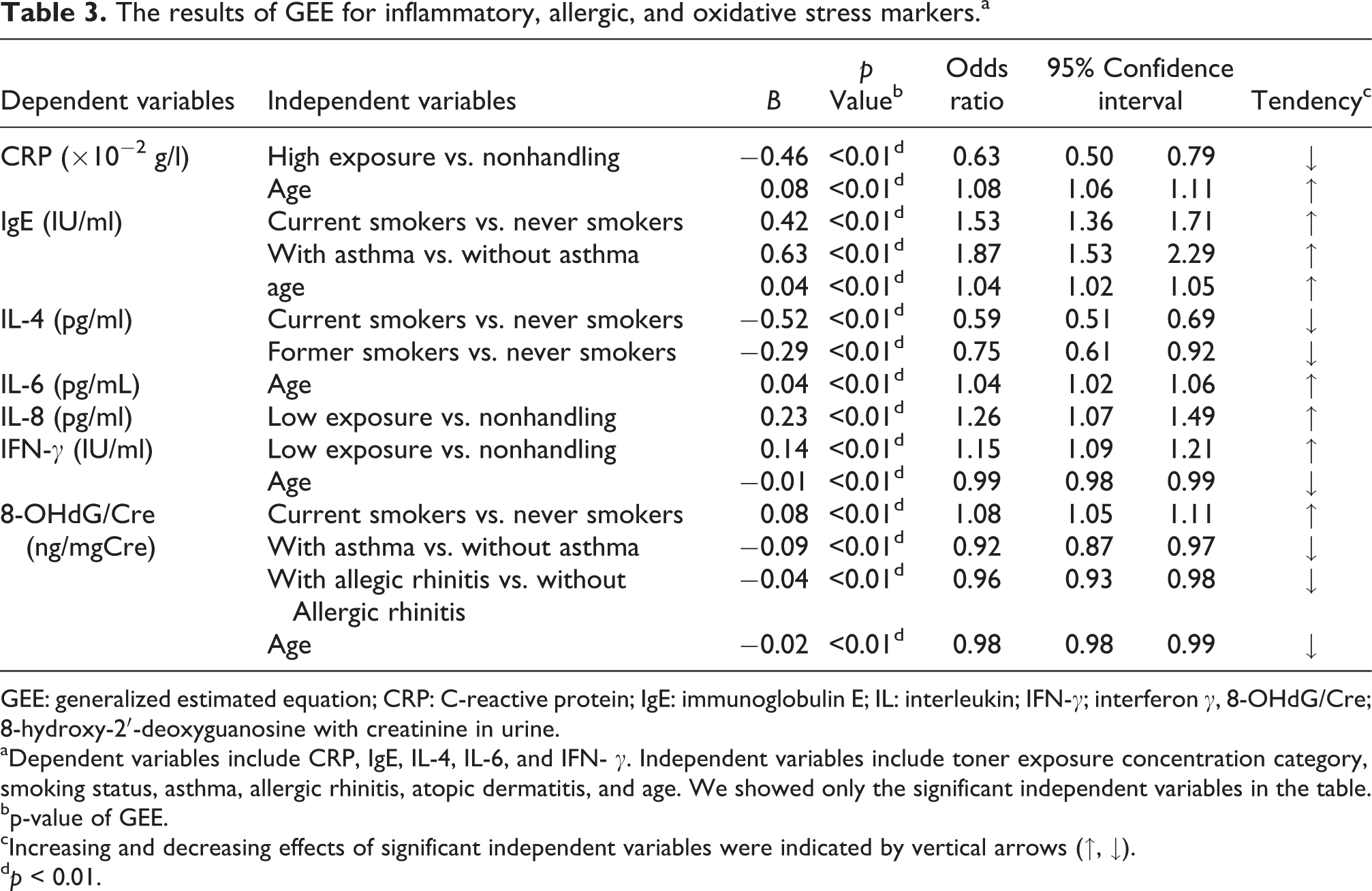
We applied GEE to examine the factors affecting inflammatory, allergic, and oxidative stress markers. We showed only the significant independent variables in Table 3. If the odds ratio was >1.0, the independent variable had the effect of increasing biomarkers, while if the odds ratio was <1.0, the independent variables had the effect of decreasing biomarkers. The effects of increasing and decreasing are indicated in the table by vertical arrows (↑, ↓). Biomarkers examined in this study are known to assess the damages on humans caused by exposure to toxic materials. Focusing on toner exposure, the low exposure group had the effect on IL-8 and IFN-γ increasing. Current smoking significantly affected IgE and 8-OHdG/Cre increasing. The effect on increasing IgE and CRP due to asthma and the effect on increasing IgE and IL-6 due to age were also observed.
The results of GEE for inflammatory, allergic, and oxidative stress markers.a
GEE: generalized estimated equation; CRP: C-reactive protein; IgE: immunoglobulin E; IL: interleukin; IFN-γ; interferon γ, 8-OHdG/Cre; 8-hydroxy-2′-deoxyguanosine with creatinine in urine.
aDependent variables include CRP, IgE, IL-4, IL-6, and IFN- γ. Independent variables include toner exposure concentration category, smoking status, asthma, allergic rhinitis, atopic dermatitis, and age. We showed only the significant independent variables in the table.
bp-value of GEE.
cIncreasing and decreasing effects of significant independent variables were indicated by vertical arrows (↑, ↓).
d p < 0.01.
Discussion
To test the hypothesis that a dose-dependent relationship existed between inhaled toner particles and health effects, we classified toner-handling workers into the high and low exposure groups. We did not find sufficient evidence to prove our hypothesis. Some sporadic findings suggested a relationship to toner exposure in both the cross-sectional and longitudinal studies, but consistent reasonable health effects associated with the toner exposure concentrations were not demonstrated.
Although toner was suspected to cause asthma and allergic rhinitis, 22 there were no significant differences in IgE among the high exposure, low exposure, and non-handling groups in this study. The values of IgE in each exposure concentration category were completely within the normal value of Japanese adult males 23 throughout the follow-up period.
Cytokines such as ILs and IFN in serum are known to be elevated in allergic reactions, immunoreactions, and inflammatory reactions. In this study, there were almost no differences in IL-6, IL-8, and IFN-γ among the high exposure, low exposure, and the non-handling groups. If the toner exposure concentration is as much or less than that in this study, the risk of the toner exposure causing allergic, immune, and inflammatory reactions is almost the same as that of the controls. However, in many cases, the values were below LOD, especially in IL-8 and IFN-γ, and are described in Table 4. The possibility that undetectable cases may lead to underestimating toner exposure must be considered. We considered that IL-8 and IFN-γ were inappropriate biomarkers in such prospective cohort studies for checking whether the health effects would occur.
The comparison of undetectable cases among the exposure to toner.

CRP: C-reactive protein; IgE: immunoglobulin E; IL: interleukin; IFN-γ; interferon γ, 8-OHdG/Cre; 8-hydroxy-2′-deoxyguanosine with creatinine in urine; LOD: limits of detection.
aLOD of each biomarkers show CRP: 0.02 × 10−2g/l, IgE: 5.00 IU/ml, IL-4: 2.00 pg/ml, IL-6: 0.20 pg/ml, IL-8: 2.00 pg/ml, IFN-γ: 0.10 IU/ml.
bUndetectable case means the value was below LOD.
8-OHdG in urine is known as an oxidative stress marker and is also affected by personal factors such as smoking, hard exercise, and food habits. 24,25 The only significant difference was shown in the fourth survey, and this finding may have been caused by personal factors rather than toner exposure.
Conclusion
In conclusion, there was no evidence of excessive allergic, inflammatory, and oxidative stress reaction in the toner-handling workers regardless of the toner exposure concentration, as compared to the nonspecifically exposed workers, despite some sporadically significant differences. There are no previous reports of a longitudinal epidemiological study focusing on toner. This study presents the first half of a 10-year cohort study that started in 2003. In the current well-controlled working environment, the exposure concentrations of toner were quite low even if the subjects were engaged in toner-handling work. Nevertheless, further studies are needed to completely understand the health effects toner may have, however small they may be.
Footnotes
Acknowledgments
The authors wish to acknowledge occupational physician Dr K Kohno and occupational nurse Y Matsuda of Fuji Xerox Co. Ltd, Tokyo, Japan, for their assistance during this study. We would also like to express our appreciation to Kanagawa Health Service Association, SRL Inc. and OHG Institute Co. Ltd for their laboratory assistance.
Conflicts of interest
In order to avoid any bias in the results, this study was based on the Japan Business Machine and Information System Industries Association guide and was undertaken according to the requirements of the ethical committee of University of Occupational and Environmental Health (UOEH), and the fairness of the study was clearly stated in the contract between Fuji Xerox Co Ltd and UOEH.
Funding
Fuji Xerox Co Ltd provided the funds for the present study to University of Occupational and Environmental Health, Japan, according to the research contract.