
Abstract
Fentanyl transdermal patches have long been used in the palliative care of patients with chronic pain with a favorable safety profile. However, intoxications secondary to intentional and unintentional misuse have been widely reported. In this study, we report an otherwise healthy woman presented to emergency department who used three patches of fentanyl to alleviate her knee pain and with a picture mimicking acute coronary syndrome.
Introduction
Fentanyl transdermal patches have been widely used in the palliative care of patients with chronic pain since 1991, where prolonged opioid use is warranted. Transdermal drug delivery is favored due to the advantages of delivering a steady dose and improving patient compliance with the ease of use besides its favorable safety profile. However, intoxications secondary to intentional and unintentional misuse and abuse have been widely reported in the literature. Here, we report the case of fentanyl overdose due to misuse, mimicking acute coronary syndrome (ACS).
Case
A 32-year-old otherwise healthy woman was presented to the emergency department with syncope. Upon questioning, she complained of chest tightness for 1 h. On physical examination her blood pressure was 100/60 mmHg, pulse rate was 55 beats/min, and respiration rate was 14 per min. Her past medical history was unremarkable. Electrocardiogram (ECG) revealed sinus rhythm with nonspecific T wave alterations (Figure 1). Her blood chemistry and blood gas analyses were within normal limits except a slightly elevated troponin level, that is, 0.011 µg/l. During her follow-up, she persistently complained of chest tightness, nausea, and sweating. The ECG revealed minor T wave flattening and inversion on precordial leads and the troponin level was slightly elevated to 0.013 µg/l. In order to rule out acute pulmonary embolism or myopericarditis, transthoracic echocardiographic examination was performed which was within normal limits. The patient was taken to the catheterization laboratory with suspicion of an ongoing ischemia. In the catheterization laboratory, respiratory depression ensued resulting in sudden cardiopulmonary arrest before introduction of femoral access. Following a 5-min-long cardiopulmonary resuscitation, cardiopulmonary circulation was secured. Catheterization was carried out on revealing completely normal coronary anatomy (Figure 2). During her transport to the intensive care unit, three patches of fentanyl 75 µ/h were detected over the inner aspect of her medial thigh. After an 8-h follow-up period, she regained consciousness and was weaned from respiratory support. When further questioned, it became clear that she used her mother’s patch, who died of breast cancer, in order to overcome her troubling knee pain. Due to the lack of efficiency, she plastered one after another and soon lost consciousness following a period of dizziness.
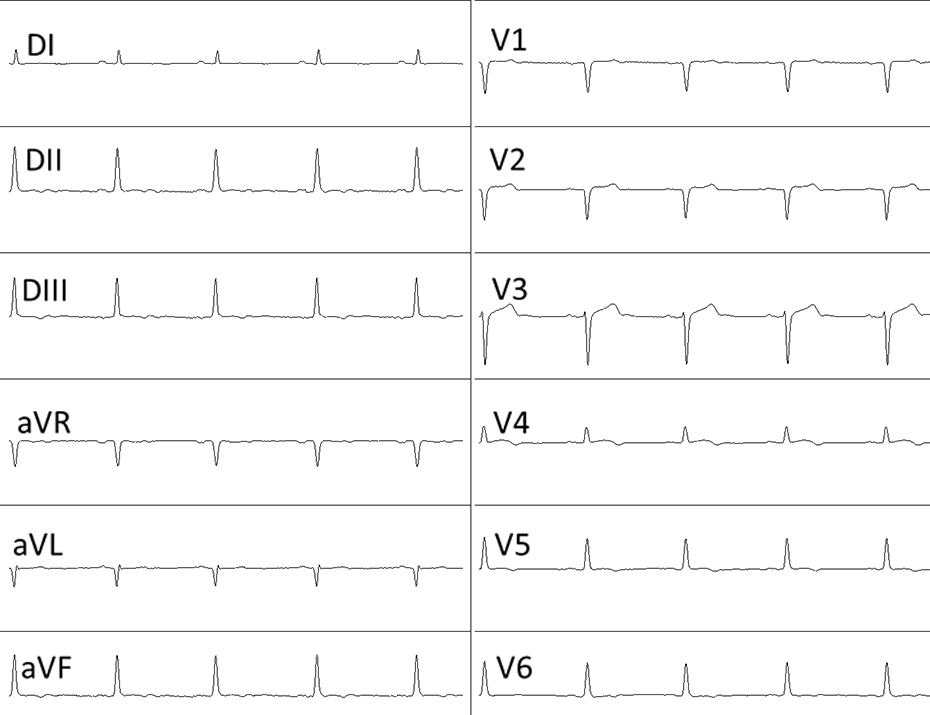
Electrocardiogram of the patient with nonspecific T wave alterations.

Coronary angiography of the patient with completely normal coronary anatomy.
Discussion
Fentanyl is a pure selective opioid receptor agonist, which is 80–100 times more potent than morphine. 1 It can be administered via intravenous, epidural, transmucosal, and transdermal routes. Transdermal route provides sustained analgesia for 72 h and long-term treatment with transdermal fentanyl is generally well tolerated, with a favorable safety profile. It produces typical adverse effects of opioids such as central nervous system depression, hypotension, bradycardia, respiratory depression, cold and clammy skin, and flaccid skeletal muscle. 1 Respiratory arrest is the most common cause of death due to fentanyl intoxication. 2 Cardiovascular side effects listed in the product monograph for transdermal fentanyl includes hypotension, bradycardia, and rarely arrhythmias. One report has suggested a possible prolongation in corrected QT interval due to related narcotic sufentanil administration. 3 Another report has implicated fentanyl as a potential cause of pulsus alternans in a patient with aortic stenosis and congestive heart failure. 4 Although fentanyl has been advocated by some as a satisfactory agent even for coronary artery surgery, there are reports suggesting that epidural fentanyl may mask the pain of myocardial ischemia. 5
In this case, accidental overdose had probably led to bradycardia and dizziness resulting in syncope rather than an ongoing ischemia. Slightly elevated troponin level was also possibly secondary to bradycardia, hypotension, or respiratory depression. Sick appearance of the patient and persistence of a nonspecific chest tightness further supported the suspicion of an ACS leading to coronary artery imagining.
There is a list of accidental fentanyl intoxications due to abuse or misuse in the literature, some even resulted in fatalities. Although it is deemed safe, patients who are using fentanyl patches and their relatives should be educated about the use, indications, and possible side effects of the patch.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.