
Abstract
Hygiene plays a key role in tipping the balance towards reduction of diarrhoeal and other infectious diseases. Yet it has often been overlooked, positioned as a “supporting rider” of water supply and sanitation services, or narrowly understood as handwashing. By focusing on handwashing infrastructure as proposed for the monitoring of Sustainable Development Goal (SDG) 6, development actors might miss the opportunity of capturing hygiene practices that are socially embedded and can act as a catalyst for change and risk reduction. We develop this argument by presenting an in-depth examination of hygiene practices in a low-income neighbourhood of Lilongwe, Malawi. Despite the high poverty levels and the constant water shortages in the area, a number of water-intensive hygiene practices are consistently carried out, proving that hygiene is central to residents’ everyday lives. Development projects should start by identifying these practices and by reflecting on the extent that these already work or can be made to work for reducing health-related risks.
Keywords

I. Introduction
Sub-Saharan Africa is rapidly urbanizing and is expected to be the region with the highest urban population growth to the 2020s.(1) Most of this growth takes place informally and is concentrated in high-density, low-income urban areas.(2) The nature and scale of this growth have significant implications for risk distribution and accumulation in cities, where greater levels of social exclusion often lead to greater risk accumulation in marginalized areas.(3) High-density low-income areas are often located at the urban fringes, characterized by the largest deficits in infrastructure and services.(4) Many of these settlements are located in hazardous areas, often exposed to both localized floods caused by the inadequacy of the drainage system and large-scale, seasonal flooding.(5) As these risks accumulate and become more pressing, urban development and disaster risk management professionals urge the acknowledgement and examination of everyday risks faced by urban dwellers at home and in their neighbourhoods as a key strategy for both development and disaster risk reduction.(6) Similarly, recent studies have argued that cumulative exposure to everyday hazards – waterborne diseases associated with inadequate water, sanitation and drainage provision, for example – have greater impact on urban dwellers than large disasters.(7) From this perspective, an examination of sub-Saharan urbanism through the lens of everyday urban risk becomes more urgent also in terms of rethinking development planning and practices, and the underlying priorities.(8)
Adequate access to water, hygiene and sanitation plays a key role in tipping the balance towards reduction of everyday health risks of urban dwellers living in high-density, low-income areas.(9) Diarrhoeal (e.g. cholera) and parasitic (e.g. trachoma, scabies, malaria) diseases related to water, sanitation and hygiene (WASH) are caused by consumption of and contact with contaminated water, insufficient water to properly practise hygiene, poor hygiene, or insects breeding in water.(10) A 2016 study estimates 842,000 deaths caused by diarrhoeal diseases in 2012, of which 502,000 are attributed to poor drinking water, 280,000 to inadequate sanitation, and 297,000 to inadequate handwashing hygiene.(11) Hygiene is seen as a cost-effective approach to risk reduction, compared to infrastructural investments in water supply or sanitation infrastructure.(12) A review of the impact of handwashing on disease control, for instance, suggests that this practice could reduce diarrhoeal diseases by approximately 47 per cent,(13) as well as play a key role in prevention of other infectious diseases such as influenza, pneumonia, HIV and neonatal infections.(14)
These studies, however, are based on a very narrow understanding of hygiene, which many programmes position as a “supporting rider” of water supply and sanitation services.(15) The most staggering example is the omission of a hygiene indicator in the Millennium Development Goals monitoring programme. As a consequence, today very few data are available on the status of hygiene and the effectiveness of hygiene interventions.(16) These omissions are partly reproduced by the Sustainable Development Goals, which define hygiene as a sub-component of sanitation (i.e. the percentage of the population not practising open defecation and the percentage of the population with access to basic and private sanitation facilities), or quite narrowly in relation to handwashing infrastructure (i.e. the percentage of the population with handwashing facilities with soap and water at home).(17) This understanding of hygiene is reflected in interventions in the urban global South, which mostly consist of hygiene education that targets behaviour change and handwashing with soap at critical moments, such as after defecation or before touching food.(18)
Our own study was, therefore, motivated by the suspicion that such widely spread assumptions and definitions of hygiene might help explain the limited effectiveness of hygiene programmes.(19) Without denying the importance of handwashing in disease control, we argue that this narrow understanding of hygiene poses two main problems. First, it overlooks other important hygiene practices related to personal hygiene, food hygiene, medical care hygiene, and keeping the home and surroundings clean.(20) Second, behaviour change and, in particular, the adoption of handwashing have proven to be complex to achieve. In a number of places, even where people are made aware of the health implications of handwashing, the actual practice is scarcely implemented.(21) Actually, the evidence indicates that hygiene practices are often motivated by desires for “order and control”,(22) meanings of cleanliness and dirtiness, and the wish to feel clean or free of bad odours, rather than disease prevention.(23) Authors have, therefore, questioned the effectiveness of hygiene interventions that ignore the socially embedded hygiene practices and the motivations and logics behind those practices.(24) These authors highlight the importance of the emotional dimensions of sanitation and hygiene, including safety, dignity and the role played by interpersonal relationships.(25) Joshi et al.,(26) for instance, document the frustrations low-income dwellers have with top-down hygiene programmes demanding the incorporation of hygiene practices that are not context specific and do not recognize the barriers to implementing such practices. The challenge of keeping the hands clean, for instance, is particularly arduous with small children living and playing in contaminated environments. For this to be effective it would require constant vigilance, severe and unrealistic restrictions on children’s play, and repeated handwashing through the day.(27)
We argue that understanding which hygiene practices are prioritized and why, as well as the role of social relations in shaping them, can contribute to risk reduction. In the remaining sections of this paper, we explore these questions through an in-depth examination of everyday hygiene practices and experiences in a low-income area of Lilongwe, Malawi (Section II) and reflect on the potential co-benefits of these practices for risk reduction (Section III). We conclude in Section IV that socio-cultural and psychological dimensions are key motivations for practising hygiene. More attention should be given to locally embedded hygiene practices that are, potentially, a key resource for reducing health risk in low-income urban areas.
II. Research Study
a. Methodology
Central to this study are questions related to residents’ preferences and motivations around hygiene, and the barriers to practising hygiene in their everyday lives. In the design of our methodology we were thus confronted with three main concerns. First, some hygiene practices as “use of the toilet” or “handwashing” can be a sensitive, if not a taboo, topic, with a high risk of getting socially desirable answers. Second, the actions of residents may not be consistent with their intentions because of contextual factors constraining their ability to exercise their preferred hygiene practices.(28) These factors, in turn, may influence residents’ multiple and at times differing perceptions of both current and aspired-to hygiene practices.(29)
We therefore selected a mixed-methods approach to reflect on the multiple dimensions of our research problem and triangulate our findings, drawing on in-depth interviews, focus groups and a survey. An ethnographic approach was taken to capture the complexity of practices and identify the motivations and influence of culture and place on these practices. In-depth semi-structured interviews (in English and in Chichewa) were carried out with 75 residents (65 women and 10 men). More women were interviewed because they happened to be more frequently at home during daytime and because they play a key role in ensuring household hygiene. Interviews were conducted with the help of a local research assistant, who was familiar with the area and able to communicate in the local language in an open, friendly and respectful way. The situatedness of the foreign researcher and her local assistant as young female students, showing interest in a non-judgemental way, was also crucial. Starting conversations with topics respondents were more comfortable with, such as the best way of cleaning their homes, encouraged them gradually to open up about more private aspects of their hygiene practices. Observations took place in the morning, when the majority of the hygiene practices take place, and entailed following residents as they performed their hygiene routines.
Additionally, three focus group discussions were held with 10 to 15 women each to triangulate our data and create a safe space for discussion. To complete our understanding of the broader political hygiene landscape, 15 members of NGOs and government organizations were interviewed.
Last, a household survey (the survey of Uncovering Hidden Dynamics in Slum Environments [UNHIDE] and Investigating Natural, Historical and Institutional Transformations in Cities [INHAbIT Cities]),(30) focused on urban risks and sanitation, was done with the aim of quantifying access to basic services and risk perception in the area. The 84 respondents, selected through convenience sampling, were surveyed in the local language by three research assistants over a period of two weeks.
Fieldwork was undertaken between January and March 2016, between the wet and dry seasons. Seasonal variations have implications for the ability of residents to engage in water-dependent hygiene practices. During the dry season, the overall water availability is significantly reduced, water shortages are more frequent and extended, and alternative sources like shallow wells and river streams may dry up. Further, with higher temperatures residents might feel the need to bathe and wash more frequently to avoid feeling sweaty and dirty.
Undertaking the study during this time of the year allowed us to observe the “habitual” hygiene practices (i.e. when water shortages are less frequent, and temperatures more moderate).
b. Research location and background
Lilongwe’s population has reached approximately 1 million inhabitants, living in 58 administrative units, called areas.(31) Area 56, which housed a population of 36,642 in 2007,(32) is located at the western confines of the city and is classified as a low-income and high-density area (LIA).(33) Residents’ incomes in the area range between 36,000 and 45,000 a month Malawian kwacha (MWK) (i.e. US$ 55–70), for a household of, on average, six people.(34) Water supply and sanitation, as well as urban infrastructure in general, are very precarious. Since 2006 the area has been served by the formal water utility through a system of water kiosks, which are managed by water user associations and open every day from 6–10am and 4–6pm. Residents, however, tend to combine water from kiosks, wells, individual connections of neighbours living in nearby higher-income areas, boreholes and rainwater for their everyday consumption and hygiene practices.(35) Underlying this strategy is the need to cope with both affordability concerns and the frequent periods when water supplies are irregular, which may last up to three or four consecutive days.(36) Very few households have in-house connections. Although the price per m3 for in-house connections is substantially lower than that paid at kiosks, most cannot afford the initial cost of connecting (Table 1). When water is short at the kiosks, residents see no other option than walking the long way to the high-income Area 47, where water supply is more reliable and the majority of households have in-house connections and a septic tank. Here they negotiate access through the solidarity of doormen and domestic workers.
Strategies for accessing water in Area 56, Lilongwe
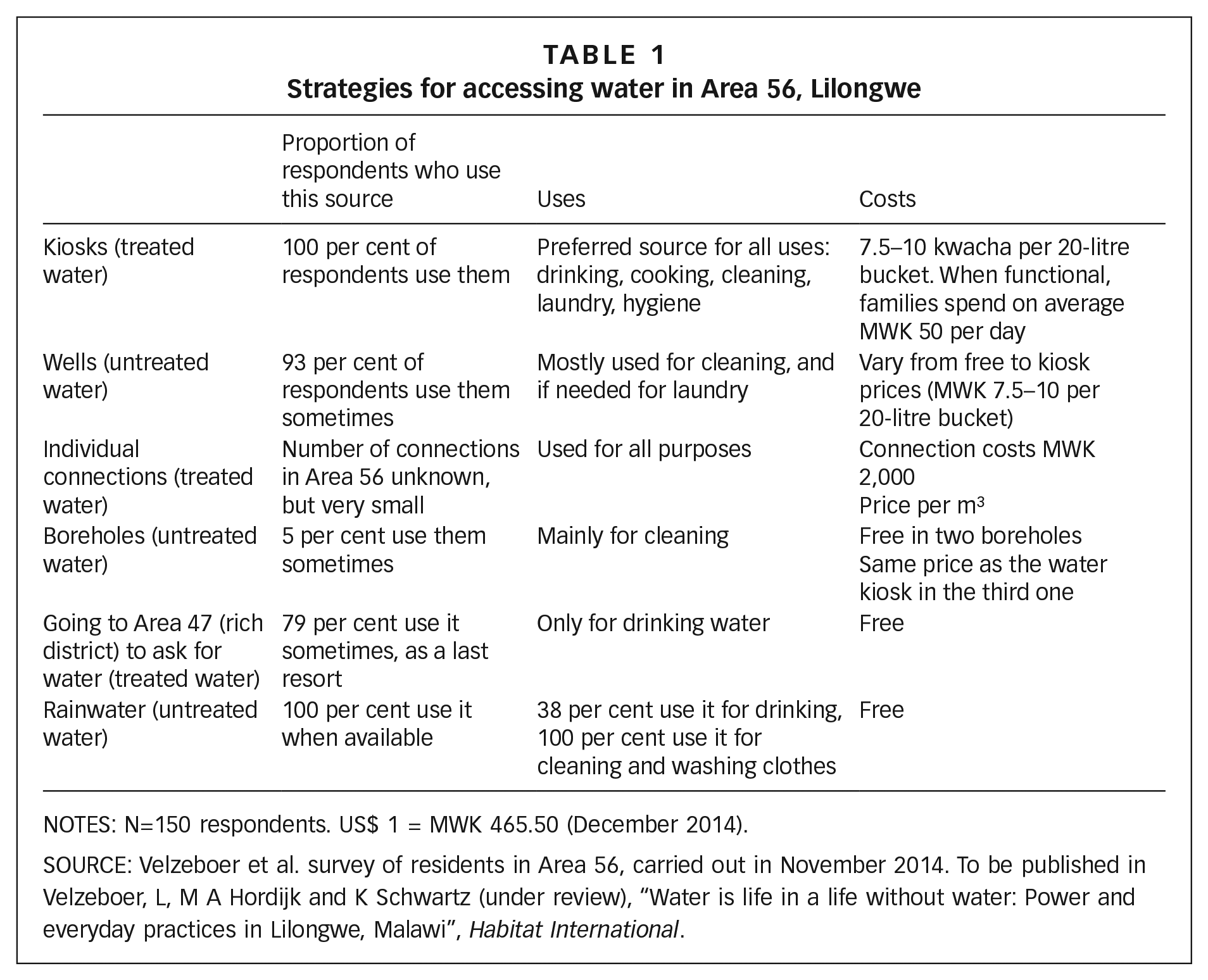
NOTES: N=150 respondents. US$ 1 = MWK 465.50 (December 2014).
SOURCE: Velzeboer et al. survey of residents in Area 56, carried out in November 2014. To be published in Velzeboer, L, M A Hordijk and K Schwartz (under review), “Water is life in a life without water: Power and everyday practices in Lilongwe, Malawi”, Habitat International.
Sanitation arrangements contribute to increased health risks, which are more or less directly associated with hygiene: 87.9 per cent of the residents share a latrine with neighbouring families or landlords, and 55.4 per cent with more than four families. A quarter of the latrines do not even have a roof. This is particularly risky during the rainy season, when sludge from the toilet is washed out, exposing residents to additional health risks associated with faecal contamination. Very few residents can afford more advanced technologies such as ventilated improved pit (VIP) latrines and flush latrines, although some are present in the area (Table 2).
Sanitation infrastructure in Area 56, Lilongwe
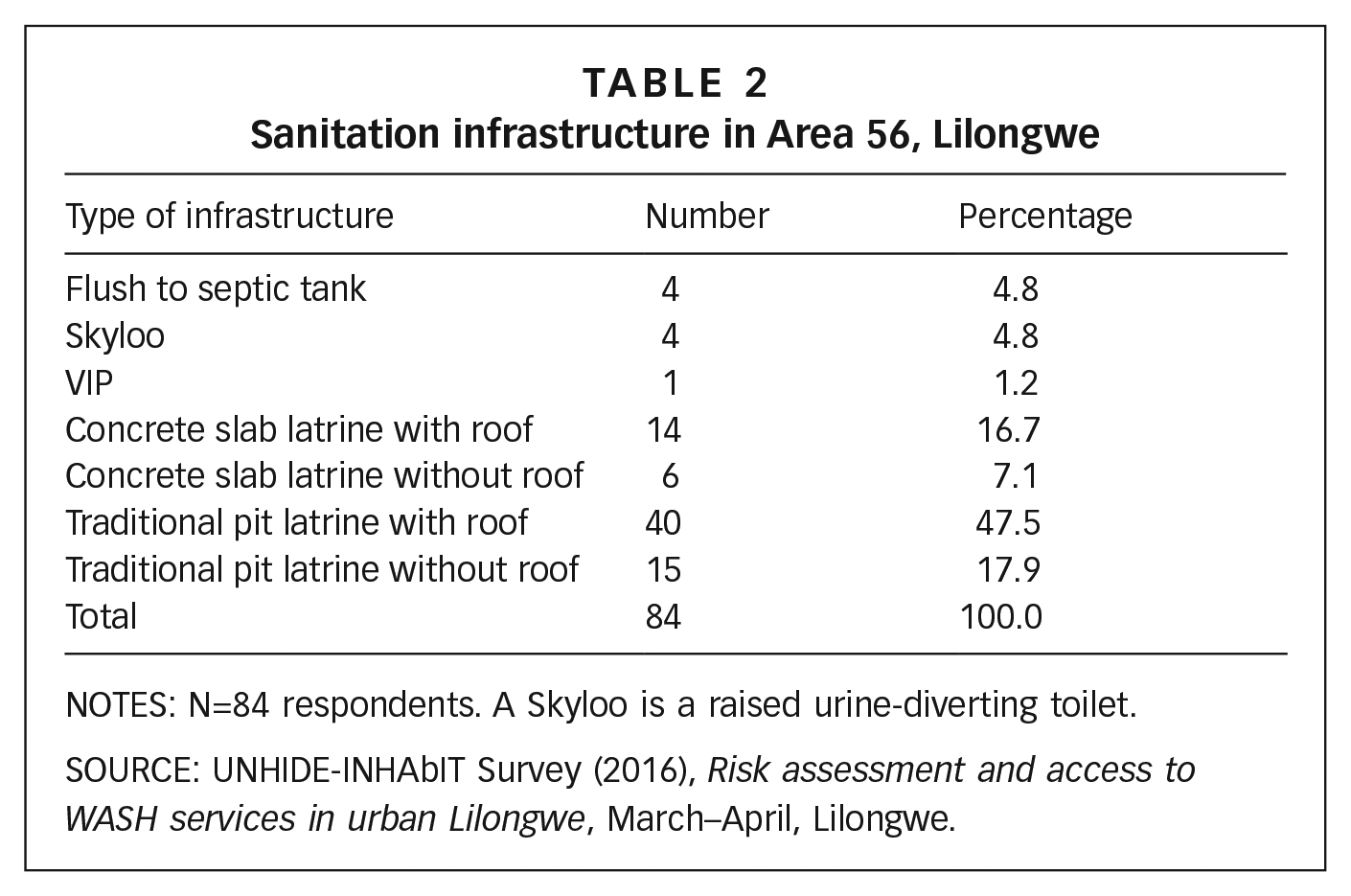
NOTES: N=84 respondents. A Skyloo is a raised urine-diverting toilet.
SOURCE: UNHIDE-INHAbIT Survey (2016), Risk assessment and access to WASH services in urban Lilongwe, March–April, Lilongwe.
Because pit-emptying costs are too high for the majority of the residents, many opt for closing a full pit latrine and building a new one next to it. Water wells, which are used for consumption and hygiene practices, are often placed near these facilities, increasing risks of water contamination. Support for improving sanitation in the area is fairly limited. Connection to the piped sewerage system was originally not foreseen for this area,(37) and even in the most recent Urban Development Plan, piped infrastructure is projected to be constructed only in 2030 or beyond.(38) Most WASH activities in Lilongwe focus on water provision, and only in 2008 did WaterAid start its first sanitation and hygiene programme. The very few sanitation programmes focus on demand creation, with the idea that “if people do not feel the need for proper sanitation, giving them the materials to build a latrine does not work. First there must be a demand from the communities” (CSO representative).(39)
These programmes have a narrow perspective on what hygiene is and what is needed to practise it effectively: “Our focus on hygiene is with door-to-door campaigns…to promote handwashing at a household level. So first with the household members…with this we are trying to raise awareness in handwashing practices” (NGO representative).
The living conditions experienced in Area 56 are similar to those of other low-income areas in Lilongwe, as well as those of other urban low-income areas in sub-Saharan Africa. Dense populations and scarce and precarious services often characterize these areas. To meet their water and sanitation needs, urban dwellers are forced to make use of both formal and informal infrastructure, a range of water sources, and practices with different degrees of quality and reliability.(40) The discussion of everyday hygiene risks in Area 56 associated with inadequate access to basic services thus has much wider relevance. Further, this area was selected as our research location because we could build on earlier research on provision and use of drinking water, carried out in the context of two research projects.(41)
III. Everyday Risk and Hygiene Practices in Area 56
a. Experiences of everyday health risk and the role of hygiene for disease control
Residents of Area 56 are well aware of the health risks they experience on an everyday basis and of how hygiene practices can mitigate these risks. Data from the survey show that inadequate access to health care is one of the greater concerns of people living in the area (Table 3). There is no hospital or clinic in the area and no ambulance service available. Concerns about the inadequacy of the health care system are intensified by residents’ awareness that the poor quality of the water they drink and use for their hygiene practices may cause conditions like cholera, diarrhoea, and skin infections or rashes. It is evident that residents see inadequate water supply, whether the lack of access or water shortages, as the most important cause of disease and, potentially, the most important resource to reduce everyday health risks. Despite this awareness, water shortages and affordability constraints force households to turn to other water sources (Table 1), which they consider harmful for their health. “Water from the kiosk is good water, because sometimes the Water Board is using medicine [chlorine], while water from the river is not good for hygiene because people wash their dirty, very dirty clothes there. And water from the well is also not good for hygiene, because some of the wells are not covered or don’t use the Waterguard [chlorine]” (Micha, resident).
Main risks in Area 56 according to respondents
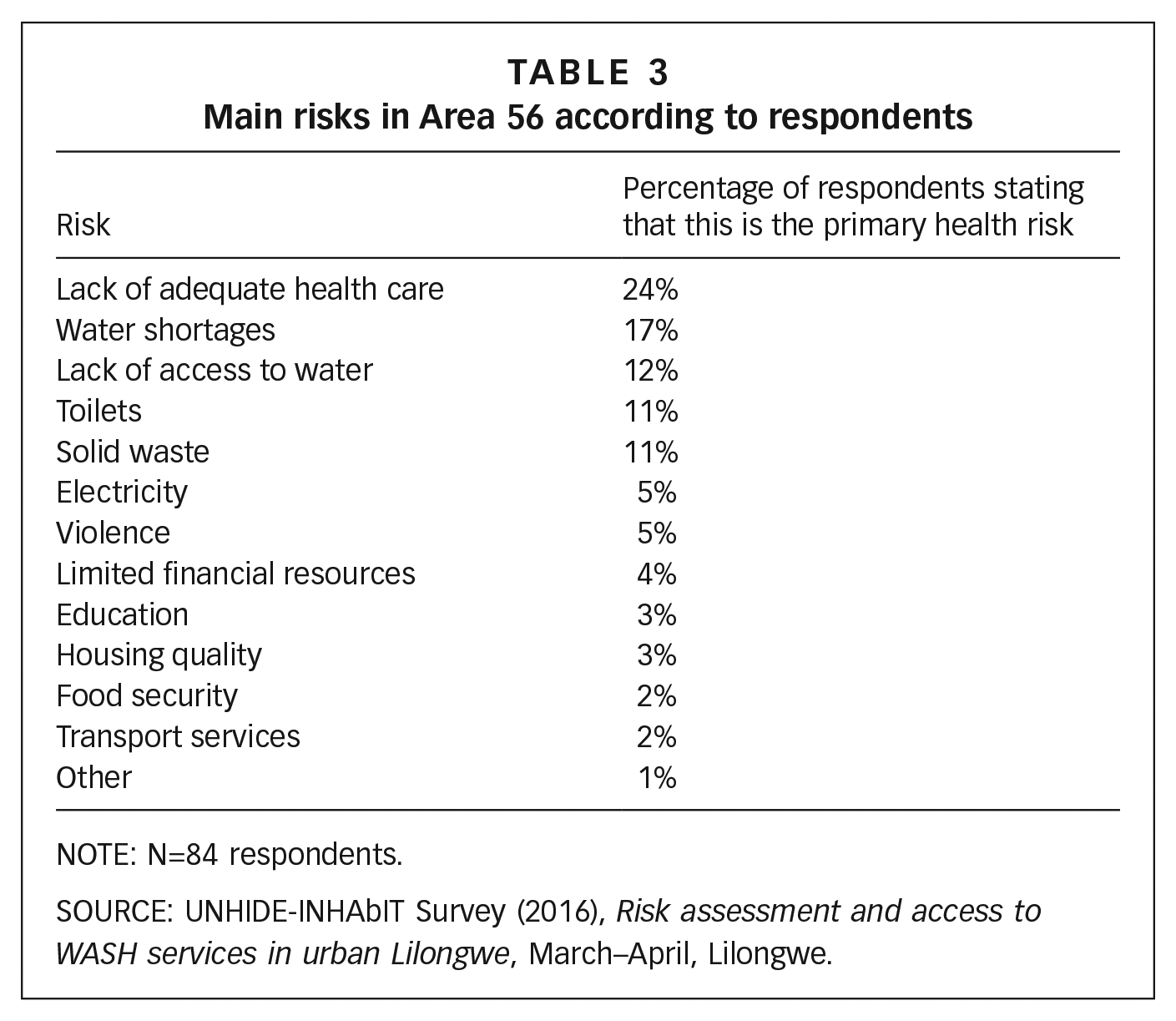
NOTE: N=84 respondents.
SOURCE: UNHIDE-INHAbIT Survey (2016), Risk assessment and access to WASH services in urban Lilongwe, March–April, Lilongwe.
In general, residents know which hygiene practices are important to reduce their health risks (Table 3). For example, they often explain that “covering [water] buckets is very important to do, because this will prevent you from getting diseases” and “having a dustbin or a dump is very important to avoid flies and diseases”. Similarly, wearing shoes is very important when going to the toilet because “when you do not do this, you can easily get sick because the floor is dirty and you can get contaminated”. Bathing frequently with treated water (i.e. water from the water utility, supplied through both kiosks and in-house connections) is perceived as being good for health too. Perceptions of healthiness and cleanliness are, thus, clearly and directly connected in resident’s accounts. Clean kids, for example, are labelled as healthy. As they go on describing their hygiene routine, residents also express their concerns about the greater vulnerability of children to WASH-related diseases: “doing the dishes is important for health reasons because unclean dishes will attract flies and especially children get sick easily”. Women also feel that they and their children face higher risks than men. As they explain, women and their children spend most of their time at home, while men often work as gardeners or night guards and at times reside in the higher-income Area 47, where they have access to better water and sanitation services.
Awareness of health risks, however, does not always work to shape hygiene practices. The most remarkable case is handwashing facilities, largely promoted by NGOs and health workers, but rarely reported as a priority by residents. As we walked through the area we rarely saw the extensively promoted handwashing facilities near the toilet, and the few that were there often lacked both soap and water. Thus, while households seem to be aware that handwashing is good for their health, most of them do not consider this practice a priority. As the urban programme coordinator of an international NGO working in the area puts it, “people do not see the point of washing hands because their parents also did not do it frequently and they did not die because they did not wash their hands”. Although residents are aware of health risks, they are often unable to carry out practices that would mitigate those risks. When it is less time consuming and the costs are lower, households may consider using untreated water, even though they are aware of the risk this poses for their health. Further, as water shortages at the kiosks are very frequent in the area, residents are forced to select which practices they want to undertake with treated water and which can reasonably be done with lower-quality water sources.
b. The psychological dimension of hygiene: stigma and self-image
While the health benefits of personal and household hygiene seem to be generally known, the motivations underlying the performance of hygiene practices are more often related to psychological and socio-cultural benefits. The first of these is considered here, the second in Section IIIc.
In Area 56, everyday hygiene practices are pursued more often as a means to project an image of cleanliness and care of bodies, clothes and houses than out of concern about the health implications. According to interviewees, people should make sure that their clothes are clean, as this is what others see, and residents are concerned with eliminating bad odours (“bad hygiene is when you have smelly babies” – Eve, resident) and projecting a clean image (the “dirtiest practice…is dirty clothes” – Vanessa, resident). A clean house is an important part of this. If the floor around the house is not swept, the neighbours may label people of that household as dirty and say they are unable to take care of their own space: “Good hygiene means that you clean the surrounding around the house because you do not want to look shabby” (Derita, resident).
Hygiene is perceived as key to self-esteem and those who do not comply with local hygiene standards face the social risk of exclusion and stigmatization. Vanessa, for instance, explains that when people are wearing dirty clothes, others think that they are not able to take care of themselves. Since the care and cleanliness of children is generally considered a priority, when limited amounts of water are available, children’s bathing and laundry take precedence. Those who do not provide for good hygiene conditions for the elderly and for children are most likely to be stigmatized: “Dirty children are disgusting and also bad because other people are going to talk about you” (Vanessa, resident).
Residents explain that certain hygiene practices are especially undertaken to avoid stigma and exclusion. Brushing teeth, for instance, has a strong psychological impact: Those who do not brush their teeth do not feel confident in talking to other people and feel unattractive. Similarly, the use of the soap is considered very important because it “kills bad smell. Soap also makes you look smart and you smell good because of soap” (Anna, resident). Sweeping the floor is important because no one wants visitors to find the house dirty or think they are lazy. One of the reasons for exercising social pressure on those who do not follow the local hygiene standards is the fear that the bad hygiene of their neighbours might reflect poorly on them and on the whole area. “When you find someone who is practising a bad hygiene, this means your area is very dirty” (Eve, resident).
The motivations for low-income dwellers to practise hygiene and prioritize certain practices are, thus, socially grounded and deeply embedded in emotions, norms, culture and lifestyles. Everyday hygiene practices are pursued as means to project an image that is often equated with dignity and considered part of good citizenship. The fear of appearing poor, dirty or unclean is a strong motivation for households to prioritize certain practices over others. This is particularly evident for brushing teeth, doing laundry, cleaning the surroundings of the house, and bathing.
c. Socio-cultural dimensions of hygiene: embedded practices
Residents’ hygiene priorities and the way these are undertaken may be determined by self-image and the fear of stigma, but these priorities are socially constructed and are the product of embedded practices. The more consistently practised hygiene behaviours in the neighbourhood are those that have been passed on by family members, mostly mothers, or that are institutionalized in religious practices (Table 4).
Hygiene practices in order of importance, with the most used water source
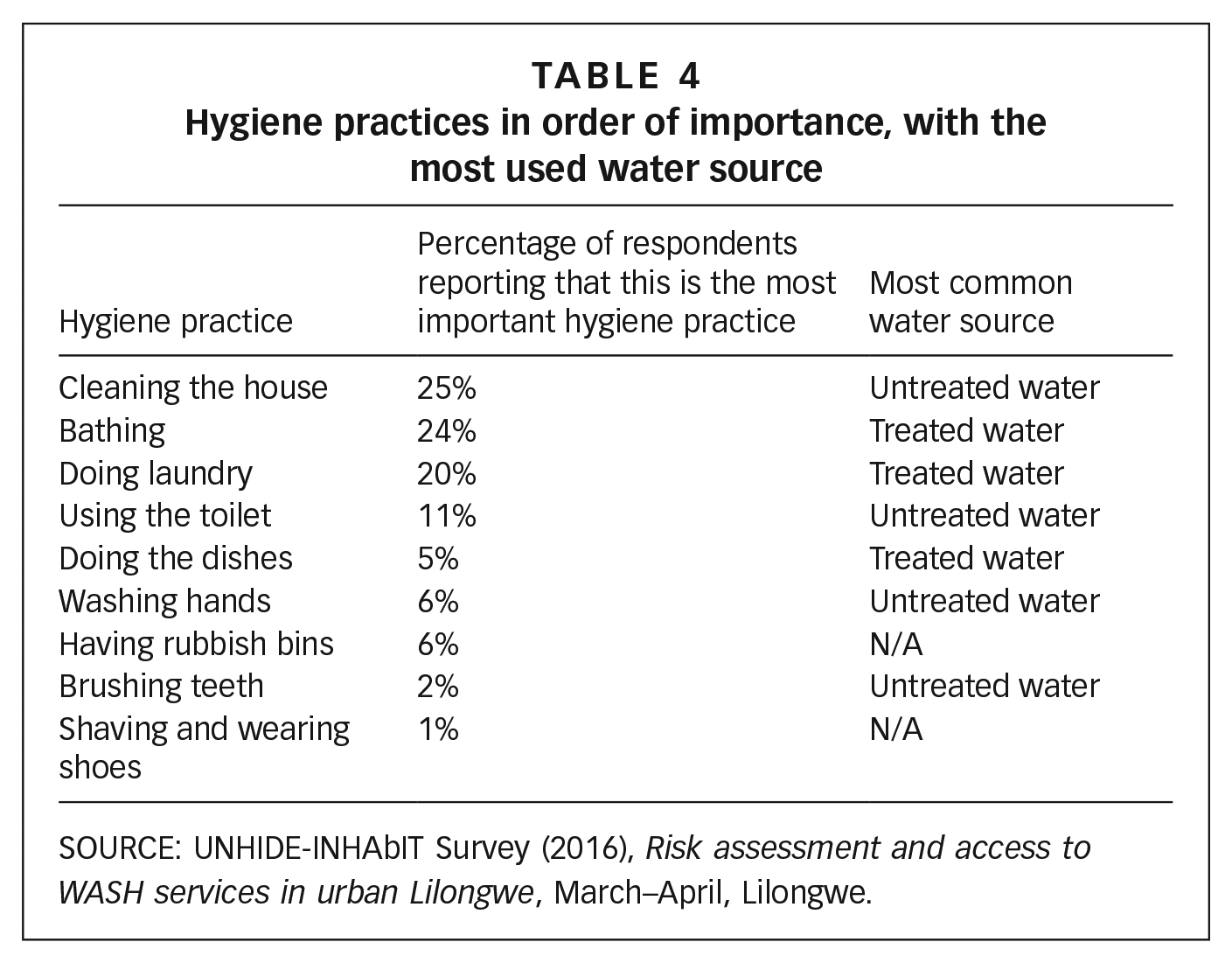
SOURCE: UNHIDE-INHAbIT Survey (2016), Risk assessment and access to WASH services in urban Lilongwe, March–April, Lilongwe.
Bathing is one of these embedded practices: “it is from our mothers that we know how to bathe, you see what they are doing and that you can copy what they are doing” (Monica, resident). Where possible, residents will bathe two–three times per day. Derita, a resident from Area 56, explains that for her, “bathing is important for good hygiene. The elderly here they take a bath in the morning and in the evening, but for the kids it is in the morning, in the afternoon and in the evening”.
In most households, the bathroom is adjacent to the toilet, though the preference would be to bathe farther away from it, because it is perceived as unclean and smelly. If the (often shared) toilet is not clean, residents may opt to wash themselves outside, as this is considered healthier than bathing in a dirty bathroom. Their bathing ritual entails the use of special “bathing” buckets, which people fill with 15 litres for adults and 5 litres for kids.
Doing laundry is time consuming and physically exhausting. It requires fetching large quantities of water – one 40-litre bucket for washing, another for rinsing, and a third bucket for storing clean clothes. The process of hand washing clothes in the hot sun is energy draining. Despite this, it is evident from walking through the area that this is an embedded practice and a common routine. In the morning, women fetch water and wash their clothes, and for the rest of the day, clothes and shoes hang from ropes in front of their houses to dry in the sun (Photo 1).

A typical laundry-hanging scene in Area 56
The ritual of laundry is complex, but as a resident named Megga explains, “I cannot imagine doing it another way”. For this practice women prefer to use treated water. Untreated water is dirty and salty, and produces skin problems such as rashes. It also requires the use of more soap, making this practice more expensive. “Water from the well is very salty. You cannot be comfortable in washing clothes. You cannot use the soap, because this doesn’t go well with that water” (Elbert and Mice, residents).
The way laundry is done and the standards associated with it are passed on by mothers, whose knowledge is accepted with confidence. “The way we do the laundry is a tradition, I learned it from my mother, so that is why I am doing the laundry like this…If I would get a washing machine, then everybody will suppose that I am arrogant. The laundry should be like this because this is the way it goes” (Brenda, resident).
Although generally less crucial than the influence of mothers, religious beliefs also influence notions of appropriate hygiene practices. While health workers “only come once a year and don’t teach anything” (Eve, resident), residents feel that the church has a more regular influence on hygiene practices. Both Muslim and Christian residents explain that their religious institutions also provide the space and the opportunity to discuss hygiene concerns within their community. As a church member explains, “everyone at the church is free to say today I want to teach my fellow Christians about sanitation”.
In our study area, this religious influence is more deeply embedded with Muslims. Handwashing, for example, is promoted in both churches and mosques, but Muslims take it more seriously. Our observations show that latrines of Muslim households are more likely to have handwashing facilities than those of Christians. As a Muslim woman explains, their religious norms prescribe handwashing and anal cleansing with water, rather than the use of paper. Having a good toilet, therefore, is strongly related to the handwashing facility. “Our religion does encourage us to be hygienic. The mosque reminds us every time that when I want to use a toilet I should have a bucket of water in the toilet to wash my hands with after using the toilet” (Melandi, resident).
For Christians in Area 56, handwashing is not an embedded religious norm, and the influence of the church in promoting this practice appears limited. Handwashing facilities are less common in Christian households and, where available, they are often placed far from the toilet (Photo 2).

Handwashing buckets in front of a house
Prescriptions on handwashing might also conflict with more socially embedded practices, according to which, for instance, “it is more dirty not to wash yourself for days than to not wash your hands”. Certainly, the resistance to practising handwashing at the toilet might also be related to external factors. Having the handwashing facilities near the latrine, for example, is considered problematic, especially because the water or even the bottle may be stolen. “I have some troubles with the kids. They are always playing with that bottle. I decided to have a bucket. So if someone will use a toilet, there is a bucket and a cup” (Vanessa, resident).
These everyday hygiene experiences show that when water is scarce and costs are high, residents are forced to make trade-offs. They are likely to prioritize a clean appearance over the less visible effects of handwashing, following the locally embedded hygiene norm with its clearly established priorities. The emotions that motivate and prioritize certain practices are both relationally produced between community members and locally embedded through mothers and institutions, such as religious organizations, that are locally legitimated to take up the roles of hygiene promoter and educator.
d. Preferences versus everyday practices: “what we want and what we can do”
Hygiene preferences in Area 56 are based on a shared morality around cleanliness and what constitutes good and hygienic behaviour for individuals and households. Women are at the same time the ones who pass on hygiene norms and the ones most burdened by the social pressures surrounding these norms. Prescriptions on hygiene requirements are quite specific and there is often a time, an order, and a series of objects attached to these practices. What is actually practised on a daily basis, however, often differs from the socially structured norms. Government and development workers in Lilongwe often point to the need to address behavioural issues through development initiatives, aiming to monitor and enforce the presence of toilets and handwashing facilities and to change behaviour. By residents’ own admission, there are households in the area that have poor hygiene practices: “You find someone who is doing a bad hygiene, you find the dishes are not clean, the area is very dirty, maybe they have smelly babies, and the laundry is not done” (Eve, resident).
Residents attribute these failures to both culture and circumstances. On the one hand, echoing NGOs and health workers, bad hygiene practices are perceived as the result of bad habits of certain individuals: “this is just the way they live. This is the way they are born” (Brenda, resident). On the other hand, residents point to the challenges of implementing these practices in a context of poverty and limited access to basic services. For many urban dwellers, practising hygiene is expensive. To fulfil their preferences, and for each family member to bathe two or three times a day, as well as do laundry and the dishes, each household would need to buy large quantities of clean water from kiosks. This is not only unaffordable for most households, but would also be physically exhausting and heavily time consuming for the women who are responsible for fetching water from the kiosks. Similarly, for most households, soap, although fundamental to ensuring good sanitation, is unaffordable.(42) Further, as mentioned, water provision in Area 56 is very unreliable: “Sometimes we have kiosk water; sometimes we don’t have kiosk water. Without water we have to go and fetch it somewhere else, which takes time and a lot of effort” (Lucia, resident).
Given these conditions, households close to a well may benefit from the easy access to untreated water. This may work to improve some hygiene practices and thus reduce everyday health risks. These households, for instance, tend to clean their houses significantly more than those living further away, as is shown in Map 1. The clusters of houses shown on the map (green, yellow, red) correspond to the frequency of cleaning the surroundings of the houses. These may suggest that not only the distance, but also practices within the neighbourhood, may influence the degree of cleanliness of each household.

Cleaning frequency reported by Area 56 households, indicating that the distance to the well influences the cleaning of the surroundings
Another resident reminds us of the costs of the irregularity of the service and how this frustrates people living in this area: “the bucket is not something cultural, it is everyday life…if we have water the whole day we would not need to have buckets, then we could go straight to the source”. Residents claim that if they had the same quality of service as Area 47, practising hygiene would be much easier and more common. For instance: “You have a better life with your own tap because you can only use the water right there. For kiosk water, when you have for example three buckets you have water but you cannot cover it. Flies can come. And that is something I find bad hygiene” (Monica, resident).
Sometimes treated water is only available at night, and women have to wake up and walk to the kiosk in the dark, with significant risks to personal safety, including physical violence and robberies: “customers get robbed, they run away and sometimes they break their buckets. This is what happens during shortages” (Grace, resident and kiosk attendant). The trade-offs between personal security and securing water for drinking and hygiene practices are experienced by women in the area on a daily basis. The reliability and continuity of water supply, the distance to the water point, and the price of the water and soap all shape residents’ hygiene strategies. Households have to ask themselves “what is needed?”, “what is affordable?” and “which water sources are accessible today?” Households have to define their priorities (i.e. what they can do, what has to be sacrificed), rather than realizing all their preferences. They may have to choose among having soap or an additional bucket of water, settling for doing laundry with untreated water, and being unable to buy toothpaste. Most households opt for bathing and doing laundry with treated water, while they clean their surroundings with untreated water. People would prefer to use treated water for brushing their teeth, but will use untreated water when necessary. Using toothpaste is preferred, but as this is an expensive product, many households cannot afford it. “Sometimes we use [toothpaste], but it is not frequently because of income and then we use ash and sometimes when we don’t have a toothbrush, we use our hand, so that is how we clean our teeth” (Vanessa, resident).
For many households, even toilet paper is unaffordable. Many have to use leaves or newspapers, or when these are not available, they scratch their buttocks against the wall to clean themselves: “Leaves are not good, only people with low income are using these. Using the wall we find really dirty, but what can we do if you don’t have the money” (Resident during focus group discussion).
Hygiene is not only about having access to treated water. Most of the narratives on fetching water are associated with water consumption, while everyday hygiene involves many kinds of water use. This means not only that larger quantities of water are needed but also, where possible, more buckets to separate water used for different tasks (Photo 3). Steve, a resident, explains what is called for to properly carry out locally preferred hygiene practices. “The way I understand hygiene, is, if you have buckets, you should have one for laundry and one for bathing, buckets for keeping your water, like drinking water, then you have a special bucket for that, if you want to have a bucket for cooking, you should have a bucket for that. And a mopping bucket, they should only be used for mopping.”

Different buckets for each hygiene practice
This further increases the costs of practising hygiene. A resident named Anna expressed a common sentiment when she said, “the difference in hygiene between households is because some cannot afford so many buckets or can’t go to the shop to buy soap”. All the preferred hygiene practices are, thus, rarely implemented in this area. Residents are forced to prioritize, as already described, trading off between what they want to do and what they can afford to do, with clear implications for the risks incurred. As further discussed in the conclusions, this entails rethinking hygiene programmes and the water demands associated with these interventions.
IV. Conclusions: Co-Benefits, Trade-Offs and Emotive Realities of Hygiene Practices
Despite the high poverty levels and the constant water shortages in the area, a number of water-intensive hygiene practices are consistently undertaken by residents. While handwashing is not as regular as health workers and NGOs advise, residents and women in particular do a lot to keep themselves, their families and households clean under adverse conditions. Although this might be for socio-cultural reasons, their priorities also bring important co-benefits for health and would be much more effective with improved access to clean water and soap. Doing laundry and bathing, for instance, may be seen as means of “handwashing by proxy”, especially if households have access to sufficient water and soap to do this as often as they would like. As both treated water and soap are expensive and the supply from the kiosks is highly irregular, many of the potential co-benefits are lost. Residents are forced to trade off between the different hygiene practices they would want to carry out and, in doing so, their risks increase. Residents may opt to bathe or do laundry less frequently during water shortages or to bathe without soap, thus reducing the impact of handwashing by proxy.
Focusing on socially embedded practices would have strong implications for the design of hygiene programmes and, more broadly, for WASH programming. Hygiene is often described as a cost-effective health intervention,(43) based on the assumption that much of the disease control can be done through handwashing, requiring minimal amounts of water and a relatively small amount of soap. Some even argue that the promotion of handwashing is a more cost-effective health solution than any other investment in water supply or sanitation infrastructure.(44) Our findings, however, show that locally embedded practices, such as doing laundry and bathing multiple times a day, are water- and soap-intensive. Working with local “hygiene hierarchies” and socially embedded practices would, thus, require rethinking the quantity of water needed for proper hygiene and the implications for residents in terms of the affordability of and access to increased water quantities. Hygiene programmes should therefore entail both creating the infrastructural conditions for residents of low-income areas to be able to perform their preferred and locally embedded hygiene routines (e.g. improving access to reliable sources of water) and undertaking locally attuned endeavours to expand the range and quality of hygiene practices implemented.
Our findings also give reasons to question behavioural approaches to hygiene education. Many of these approaches are based on the assumption that actors make rational choices once properly informed, even in conditions of scarcity. But emotive realities have a direct bearing on how and why water, soap, buckets and other resources are used.(45) The women cited in this article express strong emotions concerning “cleanliness” and “shabbiness”, and describe the shame they experience when scarcity impedes their preferred hygiene practices. We argue that these strong emotions, relationally produced between community members, along with the harsh conditions of the sites they inhabit, are also significantly shaped by traditions and culture, and passed on from mother to children. Understanding the choices people make in relation to sanitation and hygiene requires a respectful consideration of this rootedness.
That hygiene needs, practices and responsibilities are deeply gendered is widely acknowledged.(46) This study foregrounds the decisive importance of women in shaping what is valued, practised and prioritized in enacting daily hygiene practices. Gendered social norms place women in charge of ensuring the family’s and household’s hygiene and of passing on hygiene norms to their children, who regard them as role models. As women contribute to reducing the health risks of their families with their situated knowledge and unpaid work, they might understandably be seen as an entry point for development interventions to comprehend locally embedded practices. Interventions should, however, strike a careful balance in acknowledging and building on women’s knowledge and roles in shaping hygiene practices without increasing the gendered burden of performing these practices.(47)
Last, reframing urban risks to include hygiene as a “standalone” goal, encompassing a wider spectrum of locally embedded practices, also means rethinking what should be measured and targeted in hygiene programmes. Global monitoring processes tend to use narrow definitions of hygiene and overlook the complexities and trade-offs experienced by residents of low-income urban settlements. To illustrate, the currently proposed indicator for SDG 6.2, “access to adequate and equitable hygiene”, is the “percentage of households with soap and water at a hand washing facility commonly used by family members”.(48) Whilst disaggregated quantitative data are an important resource for global monitoring, these do not capture the complexities of practising hygiene. They should be coupled with case-based and context-specific qualitative studies in order to broaden understanding of hygiene and to monitor what matters locally.
Footnotes
Funding
This research has been undertaken in the framework of the collaboration between INHAbIT Cities (Investigating Natural, Historical and Institutional Transformations in Cities) and UNHIDE (Uncovering Hidden Dynamics in Slum Environments). INHAbIT Cities is sponsored by the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 656738 and is implemented by King’s College London. UNHIDE is sponsored by the Dutch Ministry of Development Cooperation (DGIS) and is implemented under the memorandum of understanding between the University of Amsterdam and the UNESCO-IHE Institute for Water Education.
1.
United Nations (2015), World Urbanization Prospects: The 2014 Revision, Department of Economic and Social Affairs, Population Division; also Angel, S, J Parent, D L Civco, A M Blei and D Potere (2011), “The dimensions of global urban expansion: Estimates and projections for all countries, 2000–2050”, Progress in Planning Vol 75, No 2, pages 53–107.
2.
UN-Habitat (2016), Urbanization and Development: Emerging Futures, World Cities Report 2016, United Nations Human Settlements Programme, Nairobi; also Tatem, A J, A M Noor, C von Hagen, A Di Gregorio and S I Hay (2007), “High Resolution Population Maps for Low Income Nations: Combining Land Cover and Census in East Africa”, PLoS ONE Vol 2, No 12, e1298.
3.
4.
Boakye-Ansah, A S, G Ferrero, M Rusca and P van der Zaag (2016), “Inequalities in microbial contamination of drinking water supplies in urban areas: the case of Lilongwe, Malawi”, Journal of Water and Health Vol 14, No 4, pages 851–863; also Dodman, D, H Leck, M Rusca and S Colenbrander (2016), “African Urbanisation and Urbanism: Implications for risk accumulation and reduction”, Working Paper 10, Urban ARK; Ahlers, R, F Cleaver, M Rusca and K Schwartz (2014), “Informal space in the urban waterscape: Disaggregation and co-production of water services”, Water Alternatives Vol 7, No 1, pages 1–14; and Parnell, S, E Pieterse, V Watson (2009), “Planning for cities in the global South: an African research agenda for sustainable human settlements”, Progress in Planning Vol 72, No 2, pages 195–250.
5.
Adelekan, I (2010), “Vulnerability of poor urban coastal communities to flooding in Lagos, Nigeria”, Environment and Urbanization Vol 22, No 2, pages 433–450; also ActionAid (2006), Unjust waters: Climate change, flooding and the protection of poor urban communities: experiences from six African cities, London, accessed 14 March 2016 at ![]() .
.
6.
See reference 3; also UNISDR (2012), How to make cities more resilient – a handbook for local government leaders, United Nations Office for Disaster Risk Reduction, Geneva, 98 pages; Bull-Kamanga, L, K Diagne, A Lavell, E Leon, F Lerise, H MacGregor, A Maskrey, M Meshack, M Pelling, H Reid, D Satterthwaite, J Songsore, K Westgate and A Yitambe (2003), “From everyday hazards to disasters: the accumulation of risk in urban areas”, Environment and Urbanization Vol 15, No 1, pages 193–204; and Pelling, M (2003b), The Vulnerability of Cities: Natural Disasters and Social Resilience, Earthscan, London, 224 pages.
7.
See reference 6, UNISDR (2012); also Adelekan, I, C Johnson, M Manda, D Matyas, B Mberu, S Parnell, M Pelling, D Satterthwaite and J Vivekananda (2015), “Disaster risk and its reduction: an agenda for urban Africa”, International Development Planning Review Vol 37, No 1, pages 33–43.
8.
See reference 4, Dodman et al. (2016); also see reference 7, ![]() .
.
9.
Hutton, G and C Chase (2016), “The Knowledge Base for Achieving the Sustainable Development Goal Targets on Water Supply, Sanitation and Hygiene”, International Journal of Environmental Research and Public Health Vol 13, No 6, Art 536; also Johannessen, A, A Rosemarin, F Thomalla, A G Swartling, T A Stenström and G Vulturius (2014), “Strategies for building resilience to hazards in water, sanitation and hygiene (WASH) systems: The role of public private partnerships”, International Journal of Disaster Risk Reduction Vol 10, Part A, pages 102–115; UNISDR (2004), Living with Risk: A Global Review of Disaster Reduction Initiatives, United Nations International Strategy for Disaster Reduction, New York; and Prüss, A, D Kay, L Fewtrell and J Bartram (2002), “Estimating the Burden of Disease from Water, Sanitation, and Hygiene at a Global Level”, Environmental Health Perspectives Vol 110, No 5, pages 537–542.
12.
Freeman, M C, M E Stocks, O Cumming, A Jeandron, J P T Higgins, J Wolf, A Prüss-Ustün, S Bonjour, P R Hunter, L Fewtrell and V Curtis (2014), “Hygiene and health: systematic review of hand washing practices worldwide and update of health effects”, Tropical Medicine and International Health Vol 19, No 8, pages 906–916; also Cairncross, S and V Valdamis (2006), “Water supply, sanitation and hygiene promotion”, in D T Jamison, J G Breman, A R Measham, G Alleyne, M Claeson, D B Evans, P Jha, A Mills and P Musgrove (editors), Disease control priorities in developing countries, Second edition, Oxford University Press, New York, pages 771–792; and Curtis, V and S Cairncross (2003), “Effect of washing hands with soap on diarrhoea risk in the community: a systematic review”, The Lancet Infectious Diseases Vol 3, No 5, pages 275–281.
13.
Curtis and Cairncross list (at least) 20 viral, bacterial and protozoan enteric pathogens, among which Salmonella spp, Shigella spp, Vibrio cholerae and rotavirus are present in human excreta. These travel in the environment and, in turn, through faecal–oral contamination cause contamination of other individuals. See reference 12, ![]() .
.
15.
Hulland, K, N Martin, R Dreibelbis, J D Valliant and P Winch (2015), What factors affect sustained adoption of safe water, hygiene and sanitation technologies? A systematic review of literature, EPPI-Centre, Social Science Research Unit, UCL Institute of Education, University College London, London; also Cairncross, S (2003), “Editorial: Water supply and sanitation: some misconceptions”, Tropical Medicine and International Health Vol 8, No 3, pages 193–195.
16.
Moreland, L D, F M Gore, N Andre, S Cairncross and J H J Ensink (2016), “Monitoring the inputs required to extend and sustain hygiene promotion: findings from the GLAAS 2013/2014 survey”, Tropical Medicine and International Health Vol 21, No 8, pages 1029–1039.
17.
IAEG-SDGs (2016), Metadata for Goal 6, Compilation of Metadata for the Proposed Global Indicators for the Review of the 2030 Agenda for Sustainable Development, Inter-agency Expert Group on SDG Indicators, United Nations, accessed 14 September 2016 at ![]() .
.
18.
See reference 16; also Fewtrell, L, R B Kaufmann, D Kay, W Enanoria, L Haller and J M Colford Jr (2005), “Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: a systematic review and meta-analysis”, Lancet Infectious Diseases Vol 5, No 1, pages 42–52.
19.
Mech, K and J Ojah (2016), “A study on the awareness and practices of hand washing amongst mothers of under-five children in the slums of Guwahati city”, Journal of Evidence Based Medicine and Healthcare Vol 3, No 24, pages 1075–1078; also Whitby, M, C L Pessoa-Silva, M L McLaws, B Allegranzi, H Sax, E Larson, W H Seto, L Donaldson and D Pittet (2007), “Behavioural considerations for hand hygiene practices: the basic building blocks”, Journal of Hospital Infection Vol 65, No 1, pages 1–8; and Jumaa, P A (2005), “Hand hygiene: simple and complex”, International Journal of Infectious Diseases Vol 9, No 1, pages 3–14.
20.
See reference 9, Hutton and Chase (2016); also Bloomfield, S F and E A Scott (2003), “Developing an effective policy for home hygiene: a risk-based approach”, International Journal of Environmental Health Research Vol 13, Supplement 1, pages S57–66; and Bloomfield, S F (2003), “Home hygiene: a risk approach”, International Journal of Hygiene and Environmental Health Vol 206, No 1, pages 1–8.
21.
See reference 19, Mech and Ojah (2016); Whitby et al. (2007); and ![]() .
.
23.
See reference 18, Fewtrell et al. (2005); also see reference 19, Whitby et al. (2007); reference 19, Jumaa (2005); reference 20, Bloomfield and Scott (2003); and Järvelä, M and E Rinne-Koistinen (2005), “Purity and Dirt as Social Constructions: Environmental Health in an Urban Shantytown of Lagos”, International Journal of Urban and Regional Research Vol 29, No 2, pages 375–388.
24.
See reference 18, Fewtrell et al. (2005); also see reference 19, Whitby et al. (2007); reference 19, Jumaa (2005); reference 20, Bloomfield and Scott (2003); and reference 23, ![]() .
.
25.
Rusca, M, C Alda-Vidal and M Kooy (in press), “Sanitation Justice? The multiple dimensions of urban sanitation inequalities”, in R Boelens, T Perreault and J Vos (editors), Water Justice, Cambridge University Press also Joshi, D, B Fawcett and F Mannan (2011), “Health, hygiene and appropriate sanitation: experiences and perceptions of the urban poor”, Environment and Urbanization Vol 23, No 1, pages 91–111; and Morales, M, L Harris and G Aberg (2014), “Citizenshit: The right to flush and the urban sanitation imaginary”, Environment and Planning A Vol 46, No 12, 2816–2833.
27.
28.
Carroll, K (2012), “An introduction to African-Centered Sociology: Worldview, Epistemology, and Social Theory”, Critical Sociology Vol 40, No 2, pages 257–270.
29.
Cresswell, J W and V L Plano Clark (2011), “Collecting Data in Mixed Methods Research”, in J W Cresswell and V L Plano Clark (editors), Designing and Conducting Mixed Methods Research, SAGE, London, pages 171–198.
31.
UN-Habitat (2011), Malawi: Lilongwe Urban Profile, accessed 22 February 2017 at ![]() .
.
32.
33.
JICA (2010), The study on urban development master plan for Lilongwe in the Republic of Malawi, Final report, Japan International Cooperation Agency, accessed 15 September 2016 at ![]() .
.
34.
See reference 30.
35.
Velzeboer, L, M A Hordijk and K Schwartz (under review), “Water is life in a life without water: Power and everyday practices in Lilongwe, Malawi”, Habitat International.
36.
See reference 4, Boakye-Ansah et al. (2016); also see reference 35; and Alda-Vidal, C., M. Kooy, & M. Rusca (2017). Mapping operation and maintenance: an everyday urbanism analysis of inequalities within piped water supply in Lilongwe, Malawi. Urban Geography.
37.
Kalipeni, E (1999), “The Spatial Context of Lilongwe’s Growth and Development”, in E Kalipeni and T P Zeleza (editors), Sacred Spaces and Public Quarrels: African Cultural and Economic Landscapes, Africa World Press, Trenton, page 76.
38.
Langkau, T (2016), “Who pays for your toilet? A study on the distribution of costs and benefits through sanitation infrastructures in Lilongwe City”, MSc thesis, Department of Geography, Planning and International Development Studies, University of Amsterdam, accessed 17 September 2016 at ![]() .
.
39.
Maurits, F (2016), “Pursuing Partnerships: An analysis of CSO partnerships in the sanitation sector of Lilongwe, Malawi”, MSc thesis, Department of Geography, Planning and International Development Studies, University of Amsterdam, accessed 17 September 2016 at ![]() . This research is also part of the INHAbIT–UNHIDE project.
. This research is also part of the INHAbIT–UNHIDE project.
40.
Allen, A, J D Dávila, and P Hofmann, P (2006), “The peri-urban water poor: citizens or consumers?”, Environment and Urbanization Vol 18, No 2, pages 333–351.
41.
See the funding notice at the end of this paper.
42.
Baker, L (2016), “Shit stories: An analysis of responsibility for different sanitation infrastructures in Lilongwe”, MSc thesis, Department of Geography, Planning and International Development Studies, University of Amsterdam.
43.
See reference 16.
45.
Sultana, F (2011), “Suffering for water, Suffering from water: Emotional geographies of resource access, control and conflict”, Geoforum Vol 42, No 2, pages 163–172.
46.
See reference 25, Joshi et al. (2011); also IWSD (2012), Guidelines for Urban Hygiene Promotion, Institute of Water and Sanitation Development, accessed 5 January 2017 at https://www.humanitarianresponse.info/system/files/documents/files/Urban%20Hygiene%20Guidelines.pdf; and JMP (2015), Green Paper: Global monitoring of water, sanitation and hygiene post-2015, WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation, page 20, accessed 15 September 2016 at ![]() .
.