
Abstract
Public pay-per-use toilets are the only alternative to open defecation for a significant number of people in many low-income, urban neighbourhoods where insecure tenure, space constraints, and/or cost make private sanitation facilities unfeasible. This study explores public toilet use, characteristics of public toilet customers and possible improvements to public toilet facilities in four neighbourhoods in Accra, Ghana, the country with the highest reliance on shared sanitation facilities globally. Reliance on public toilets ranged considerably depending on neighbourhood affluence, but even some people living in compounds with a private toilet used a public toilet. The vast majority of users were adults. Few public toilet customers could foresee owning a household toilet in the coming year, mostly because of lack of space, and they voiced desires for more and cleaner public toilets with better provision of handwashing facilities. Improved accessibility and management of public toilets, along with facilities more suitable for children, could reduce open defecation.
I. Introduction
Inadequate sanitation infrastructure is one of the key factors that distinguish slums(1) from other urban areas. As noted by a report of the University College of London/Lancet Commission on Shaping Cities for Health, improved sanitation infrastructure is a necessary condition for realizing the “urban advantage” in low-income countries.(2) With two-thirds of urban dwellers in Africa residing in slums (twice the rate for low-income regions globally), Africa’s cities are reported by the United Nations Human Settlements Programme to have the lowest levels of infrastructure provision globally, in part because of the poor status of water and sanitation access.(3) According to the most recent estimates, 735 million residents of cities in low-income countries lack access to improved sanitation, defined by the World Health Organization (WHO) and UNICEF’s Joint Monitoring Programme (JMP) for Water Supply and Sanitation as hygienic separation of human excreta from human contact.(4) Use of shared sanitation facilities accounts for two-thirds of those who lack access to improved sanitation, as shared facilities do not qualify under the JMP definition,(5) since the likelihood of unhygienic outcomes is considered higher when anyone can use the sanitation facility.(6) Additional considerations include the distance involved in accessing shared sanitation facilities, the risk of violence against women and the lack of accommodation for children under the age of five.(7) Ghana relies more heavily on shared sanitation in urban areas than any other country, with an estimated 72 per cent of its urban population using shared facilities.(8) Political stability and a growing economy fuel steady migration into Accra, a rapidly growing city of 3.9 million.(9) This growth has resulted in the expansion of low-income neighbourhoods where an estimated 58 per cent of Accra’s residents live in crowded housing, with inadequate water supplies, poor sanitation infrastructure and sub-standard hygiene practices.(10)
In this paper, we focus on a particular type of shared sanitation facility: public toilets. As defined by Water and Sanitation for the Urban Poor (WSUP), such toilets are characterized by their location in public places, their availability to anyone, and the charge required for each use.(11) Public toilets were first constructed in Ghanaian cities by the British government in the 1930s. Their numbers continued to increase during the post-colonial era as they came to be a practical means for addressing the sanitation needs of growing urban populations and a reliable source of revenue for sub-metropolitan councils.(12) In 2012, the public health department of the Accra Metropolitan Assembly reported 340 registered public toilet facilities. In 2006, 41 per cent of the households in Accra used public toilets. Four of out five households with access to a private latrine shared it with other households and thus did not have exclusive use (or qualify as having improved provision).(13) Only 9 per cent of the city’s population have access to sewers. Most household and public toilets either discharge liquid effluents into the storm drainage system or dump them into the ocean.(14)
Despite the historical and logistical realities that make the use of public toilets commonplace in urban Ghana, this form of sanitation does not count toward the Millennium Development Goal target 7.C, which calls for “halving the proportion of people without sustainable access to safe drinking water and basic sanitation” and is monitored by the JMP, using the definition of improved sanitation given above.(15) While case studies indicate that shared facilities can be successfully maintained, their capacity to adequately serve the needs of all members in a community is debatable.(16) For instance, a recent study of determinants of communal latrine use in Bhopal, India found wide variations in latrine conditions, management and usage rates, with women using communal latrines at half the rate of men.(17) Another study of sanitation in Kampala, Uganda found that the majority of residents were dissatisfied with the high traffic and low levels of cleanliness of their shared toilet facilities.(18) A recent survey in Accra showed only 30 per cent of households that use public toilets find them satisfactory.(19) These findings, however limited, point to the frequent failure of these facilities to meet residents’ needs. However, the extent to which inconsistent use and poor conditions are problems with public toilets globally is not certain.
It is estimated that the consequences of poor sanitation cost Ghana approximately US$ 12 per person per year.(20) Diarrhoea accounts for roughly a quarter of the deaths of children under five and Accra has recorded cholera outbreaks annually for the last several years.(21) These outbreaks have largely occurred in low-income urban communities, where Ghana’s government has embarked on significant sanitation investments to improve current sanitation conditions. For example, the US$ 150 million World Bank-funded GH-GAMA Sanitation and Water Project seeks to “improve sanitation and water supply in GAMA (Greater Accra Metropolitan Area) with emphasis on low income communities”. This project includes plans to build public toilets for schools, markets and health care centres. During the project’s design phase, authorities considered assisting households that live in compound houses(22) to build better shared latrines, even though these new facilities would not have counted toward JMP targets. Such projects exemplify plans for significant investments in Accra’s sanitation with implications for public toilets and their customers. There is a paucity of published data, however, on those who use public toilets and the factors related to their use. This study aims to address this gap and inform future investment in public sanitation in Accra and other rapidly growing cities in sub-Saharan Africa.
This study is part of a larger research and stakeholder engagement project known as SaniPath, an assessment of faecal exposure pathways in low-income urban settings, funded by the Bill & Melinda Gates Foundation and conducted by researchers at Emory University, the Noguchi Memorial Institute for Medical Research, the Water Research Institute, and Training Research and Networking for Development (TREND). The goal of SaniPath is to promote strategic investments in sanitation and facilitate evidence-based sanitation interventions by expanding knowledge about faecal contamination sources and exposure pathways in low-income urban environments.
II. Methods
A mix of qualitative and quantitative methods was applied in four Accra neighbourhoods over a period of six months in 2012 to collect data on the physical conditions of public toilets, rates of use among the population as a whole, and the socio-demographic characteristics and opinions of public toilet customers.
a. Study sites
Four neighbourhoods (Alajo, Bukom, Old Fadama and Shiabu) were selected for the SaniPath study in order to capture a diverse set of conditions with regard to tenure arrangements, income, location and frequency of flooding (Table 1). Living quarters for households in these neighbourhoods generally comprise single rooms (approximately 16 m2), which collectively form compound houses made from permanent and semi-permanent materials.
Summary of study neighbourhoods
b. Data collection
Data were collected from March to September 2012 by locally recruited enumerators. These enumerators were trained in classroom-based sessions and field pilots on ethical conduct of research, structured observation and household surveys. A subset of enumerators were trained on qualitative methods. In each neighbourhood, enumerators worked under the supervision of the local research partner, TREND, and with community liaisons. All interviews and group discussions were conducted in local languages.
Household survey
The household survey was administered to 800 households (200 per neighbourhood; see Figure 1). Ten enumerators administered the survey questionnaires over a period of four days in each neighbourhood. Neighbourhoods were divided into four segments, based on Google-generated maps containing drain and neighbourhood boundary overlays, with the help of community liaisons. Enumerators worked in pairs to randomly select a compound by tossing a coin at the edge of their segment, administer the questionnaire and then move an interval of five compounds, counting both sides of the street/alley, to arrive at the next household for interview. A household was defined as a person or group of people who shared cooking and living arrangements, and a compound was defined as a collection of households under the same structure. Only one household in each compound was interviewed and in most cases the respondent was a woman. Survey questions covered socio-demographic characteristics, access to water and sanitation facilities, hygiene practices, and frequency of interaction with other domains such as schools, markets and beaches. Each survey took no more than one hour to administer.
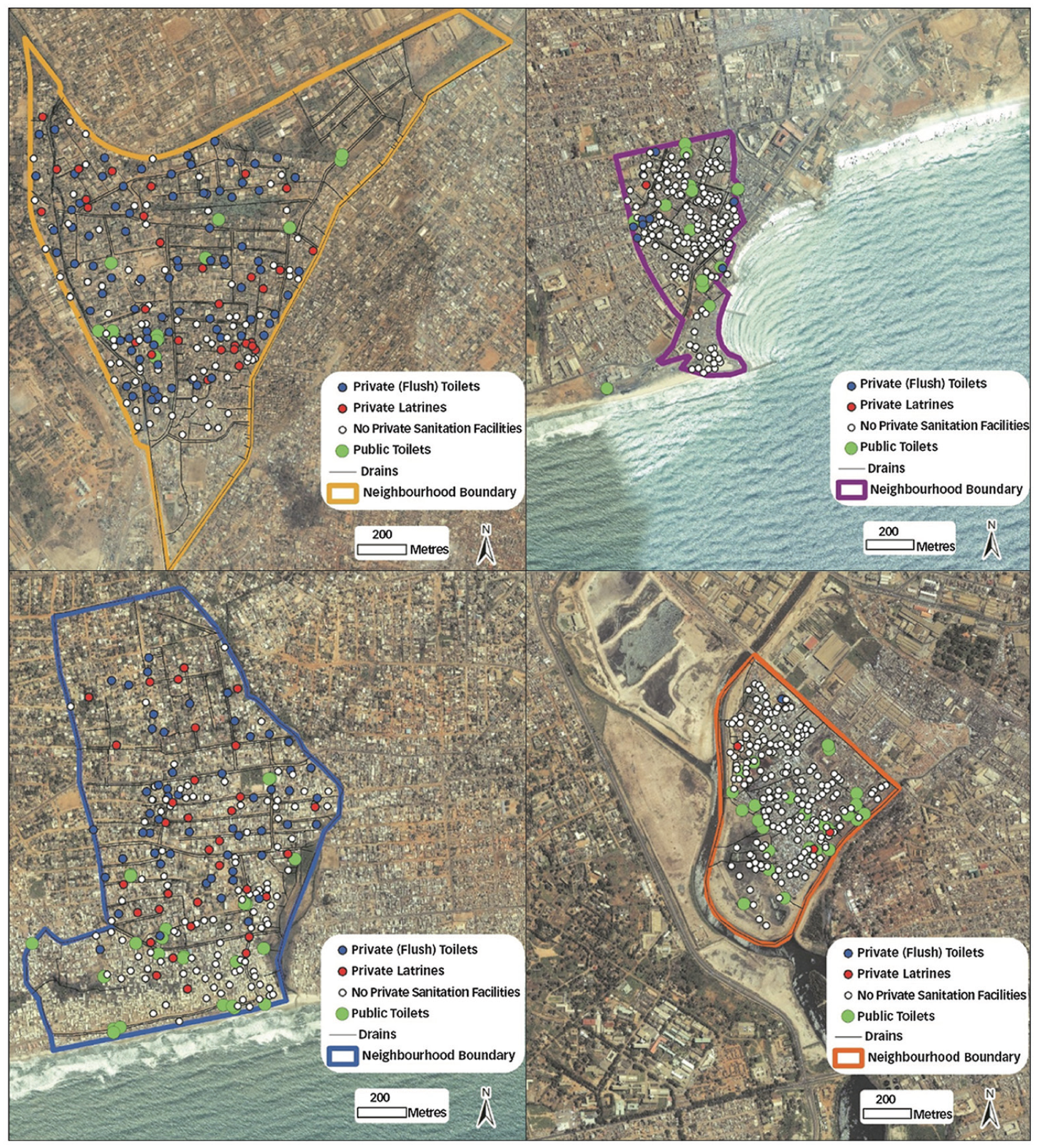
Household survey locations and types of sanitation facilities by neighbourhood
Observations at toilet facilities
Weekly observations of public toilets were conducted in each neighbourhood. Each public toilet was associated with an owner and various operators. Owners, defined as the direct beneficiaries of profits from the public toilet facility, were either private individuals or the district assembly. Operators managed the daily running of the facility. Observations took place for five hours in the morning or afternoon, from 7am until 12pm or from 1pm to 6pm. Public toilets were purposively selected according to their location within the neighbourhood. Consent for observations was obtained from the public toilet owner prior to observation. Upon arrival at the toilet, the enumerator completed a toilet description form that recorded operational characteristics and consulted with the toilet operator to determine a time for condition inspections that would not interrupt the flow of customers or compromise their privacy. The enumerator then selected a convenient vantage point from which they could tally gender and estimated age categories (5–12; 13–17; 18 and above) of all customers entering the toilet over the observation period. Enumerators recorded their independent observations of factors such as privacy, safety, odour, presence of faeces and flies for inspection of conditions.
Public toilet exit interviews
In a subset of the observed public toilets in all four neighbourhoods, enumerators also conducted public toilet exit interviews over the same five hours that the observations were conducted. Toilets for these interviews were purposively selected to represent different sections of the neighbourhood. Customers were approached by an enumerator for an interview when they exited the toilet facility. Interview questions covered socio-demographic characteristics, access to household sanitation facilities, frequency of public toilet use and likelihood of acquiring a household latrine. Interview sessions took no longer than 10 minutes and were spread across the hours of observation. Sampling intervals depended on the level of traffic at the public toilet at that time. Interviews at high-traffic toilet facilities (i.e. more than 50 customers in an hour) were spread out over observation hours by having longer intervals between interviews (i.e. interviewing every 8th customer). Interviews at low-traffic toilet facilities were conducted with each customer.
Focus group discussions
Focus group discussions were conducted with fathers and mothers of children in Bukom and Old Fadama to capture their experiences and opinions of public toilets. Themes covered by discussion questions included sanitation options in their community, accessibility of public toilets, good and bad experiences at public toilets, their plans for toilet ownership, and children’s public toilet use. Participants were purposively selected from households in different parts of the neighbourhood with the help of community liaisons. Discussion groups were comprised of six–eight participants of the same gender. All discussions were led by trained moderators and note-takers fluent in the local language. Discussions were captured with a digital recorder.
c. Data entry and analysis
Data from the household survey, public toilet observations and public toilet exit interviews were double-entered into a Microsoft Access database. The data were checked and cleaned in Access and then exported to STATA 9.0. Data from each methodological output were analysed independently in consideration of the different approaches to sampling. Neighbourhood-level descriptive analyses were performed for each dataset. Public toilet observation data were analysed by individual toilet (summary table available online as Appendix A: Public toilet observation data), and then aggregated by neighbourhood as trends emerged. Missing data were omitted from analysis.
Recordings of focus group discussions were translated and transcribed verbatim by the discussion moderators. Transcripts were read in tandem with recordings to check for accuracy. Responses were summarized and transferred into matrices that allowed for intra-case analyses of discussion themes by gender and neighbourhood. Cross-group similarities and differences were identified with illustrative quotes.
III. Results
a. Study setting and sanitation access
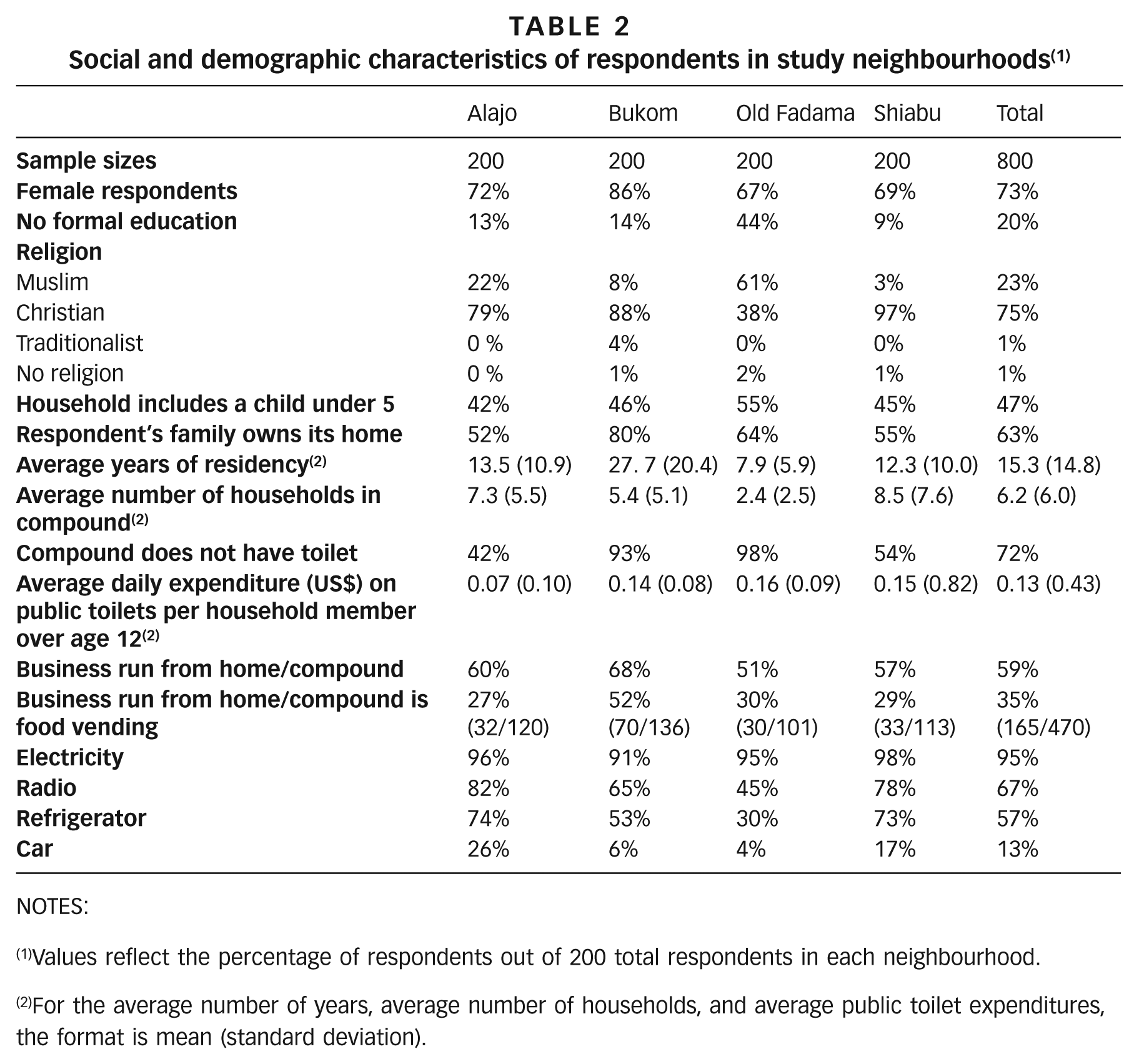
Educational attainment was found to be common in all neighbourhoods except Old Fadama, which had the greatest proportion of people with no formal education (Table 2). Neighbourhoods did not appear to differ with respect to access to electricity. However, other asset indicators, such as radios, refrigerators and cars, were consistently more common in Alajo and Shiabu and less common in Bukom and Old Fadama. In all neighbourhoods, home-based businesses were common, and 35 per cent of them involved food vending. Respondents in Bukom had lived in their neighbourhoods the longest and reported the greatest percentage of home ownership. Most compounds (72 per cent) had no toilet on site. This varied between neighbourhoods: 93 per cent and 98 per cent of homes in Bukom and Old Fadama respectively lacked sanitation facilities, as compared to 42 per cent and 54 per cent of households in Alajo and Shiabu respectively. Reported frequency of public toilet use (Figure 2) was higher in Bukom and Old Fadama, where household toilet coverage was lowest. Average per capita daily income in Old Fadama, the poorest study neighbourhood, is estimated at less than US$ 2 per day.(23) Although there are no accurate data available on per capita income for the study neighbourhoods, the best estimates suggest that residents of these neighbourhoods are not likely to earn more than US$ 5 per day. On average each household had two adults and three members in total over the age of 12. Given these parameters, public toilet expenses reported by survey respondents likely totalled at least 3 per cent of household income and afforded each household member over age 12 only one or two public toilet uses daily.
Social and demographic characteristics of respondents in study neighbourhoods (1)
NOTES:
Values reflect the percentage of respondents out of 200 total respondents in each neighbourhood.
For the average number of years, average number of households, and average public toilet expenditures, the format is mean (standard deviation).
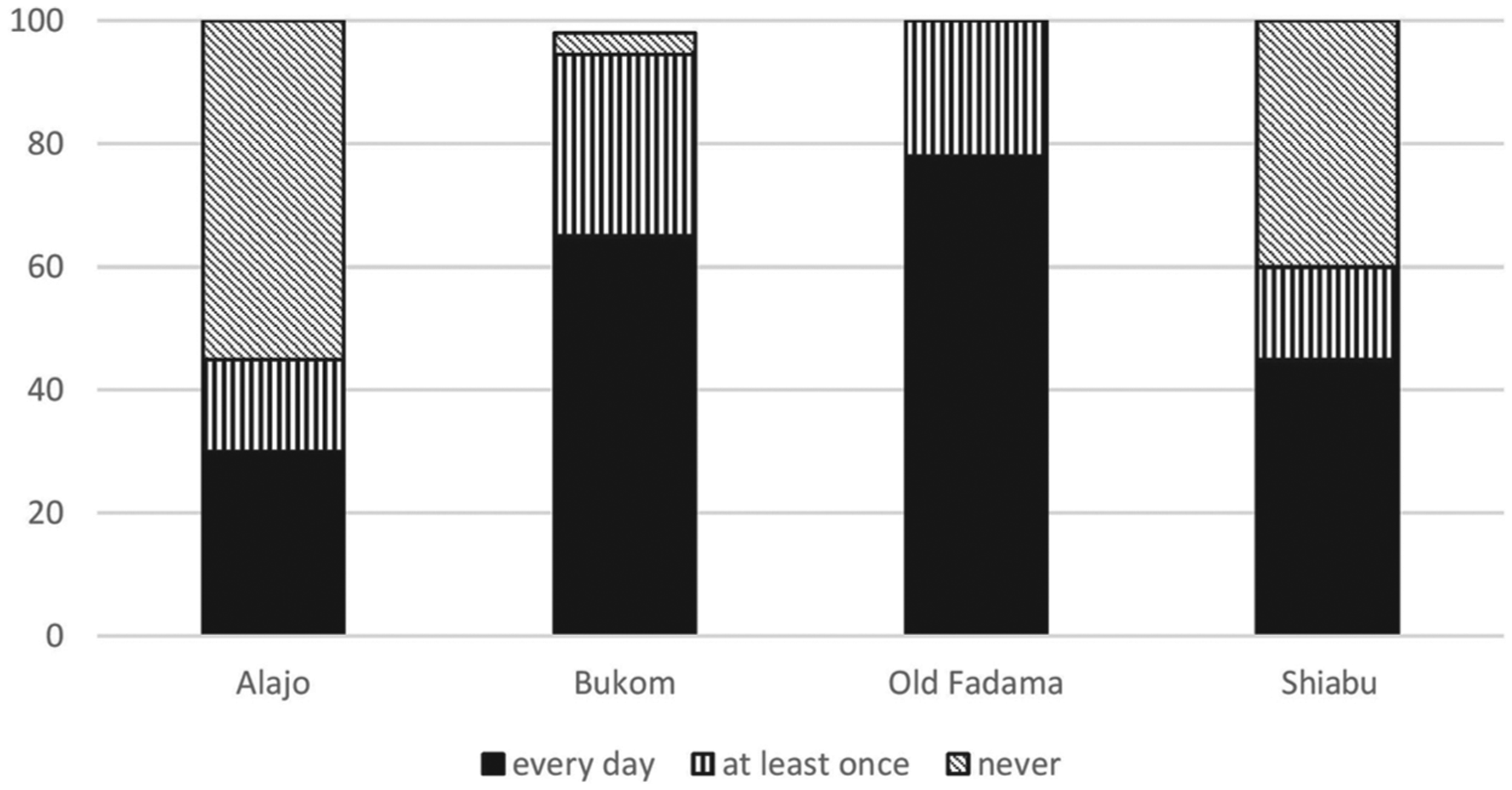
Reported weekly frequency of public toilet use by neighbourhood
b. Conditions at public toilets
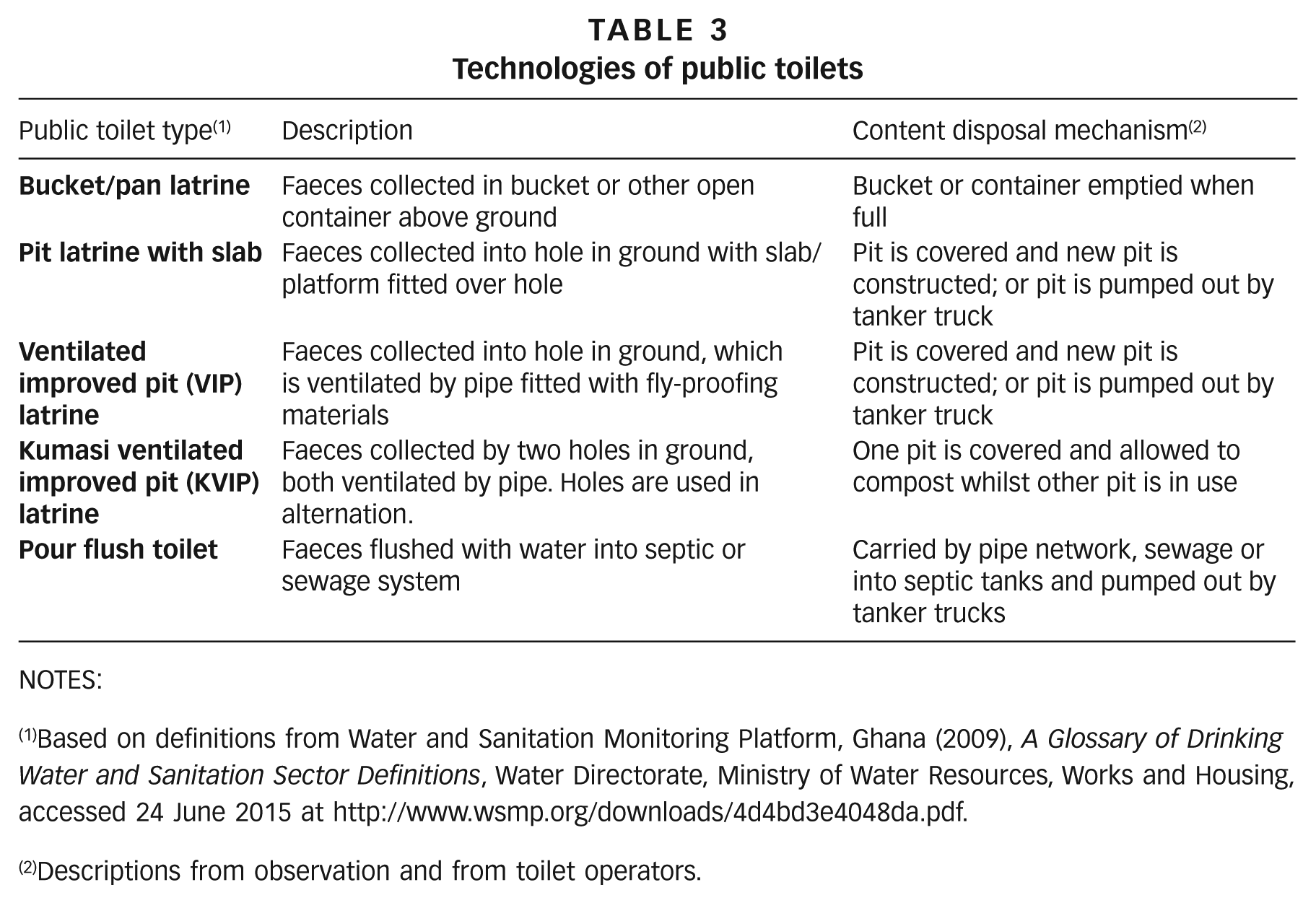
The types of toilets observed and their emptying practices are summarized in Table 3.
Technologies of public toilets
NOTES:
Based on definitions from Water and Sanitation Monitoring Platform, Ghana (2009), A Glossary of Drinking Water and Sanitation Sector Definitions, Water Directorate, Ministry of Water Resources, Works and Housing, accessed 24 June 2015 at http://www.wsmp.org/downloads/4d4bd3e4048da.pdf.
Descriptions from observation and from toilet operators.
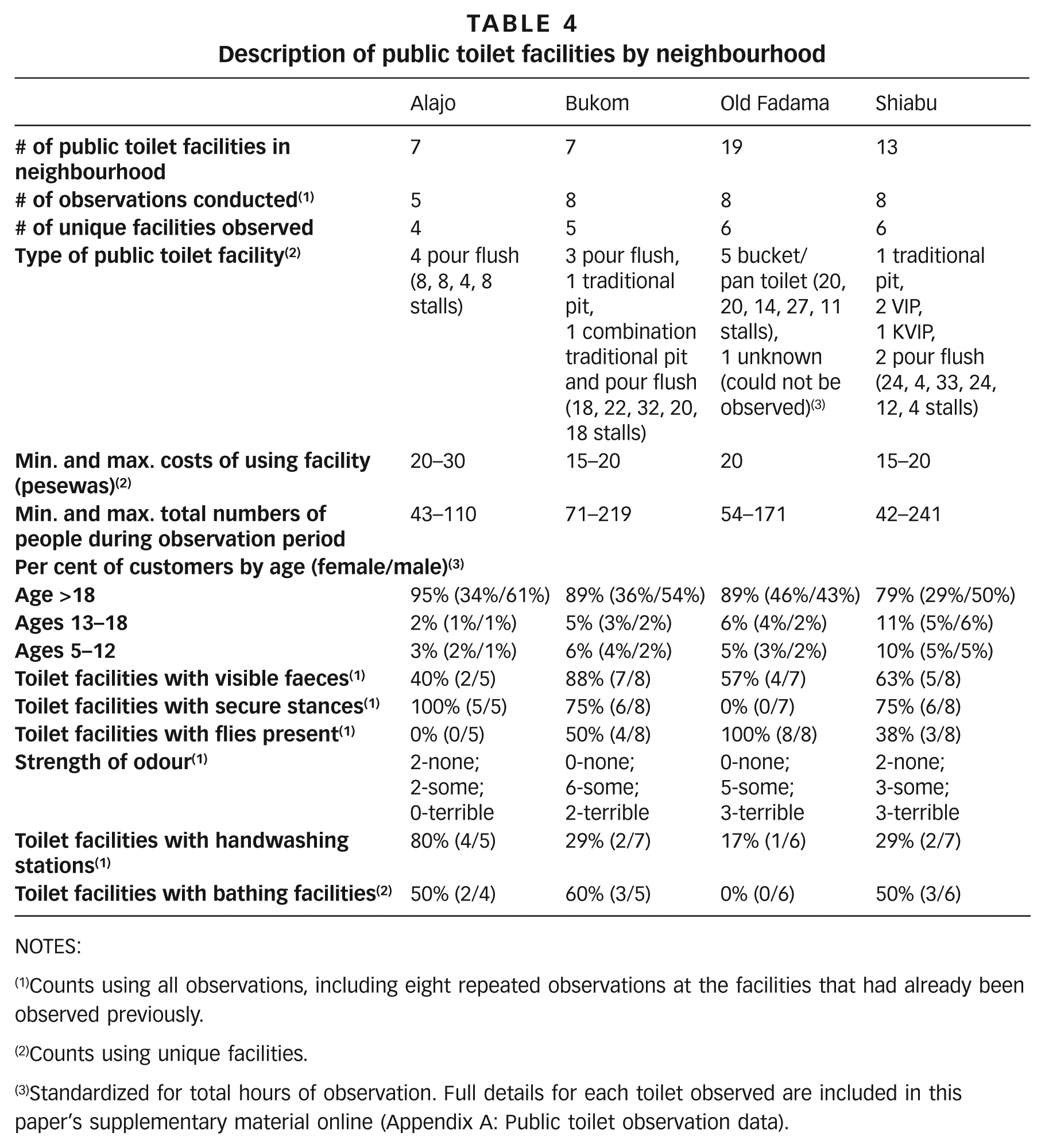
Twenty-nine public toilet observations were conducted. Public toilet facilities varied with respect to the technology involved, cost, observed number of patrons and conditions. The cost of using a toilet facility ranged from 15 to 30 pesewas per use (US$ 0.08–0.15). Such costs appeared consistent across all neighbourhoods (Table 4). The largest numbers of customers were observed in Bukom and Old Fadama. Children under 18 years of age were not typical customers, despite the fact that they accounted for 38 per cent of all members of surveyed households. Toilet conditions differed between neighbourhoods. A toilet facility was considered clean if there were no visible faeces anywhere in its stalls. The majority of facilities observed had some form of visible faeces in their stalls. A toilet facility was considered secure if none of its stalls posed a risk of falling through for the user. The majority of toilets in all neighbourhoods were observed to be secure. Insecure stances (platforms over squat holes) were mostly observed in Old Fadama, where one facility was classified as too hazardous for use. Flies were considered present if a toilet was observed to have one or more flies in any of its stalls. Flies were present in facilities in all neighbourhoods with the exception of Alajo. Some level of odour was found in all neighbourhoods. Few handwashing stations (defined as soap, water and a bucket specifically designated for customers upon exiting the toilet facility) were observed. Such stations were not found in the majority of toilet facilities observed. On the whole, toilets in Bukom and Old Fadama appeared to be less clean than those in Shiabu and Alajo. Bathing facilities were present in 38 per cent of the public toilet facilities. The cost of using a bathing facility ranged from 10 to 20 pesewas per use (US$ 0.05–0.10).
Description of public toilet facilities by neighbourhood
NOTES:
Counts using all observations, including eight repeated observations at the facilities that had already been observed previously.
Counts using unique facilities.
Standardized for total hours of observation. Full details for each toilet observed are included in this paper’s supplementary material online (Appendix A: Public toilet observation data).
c. Public toilet customers
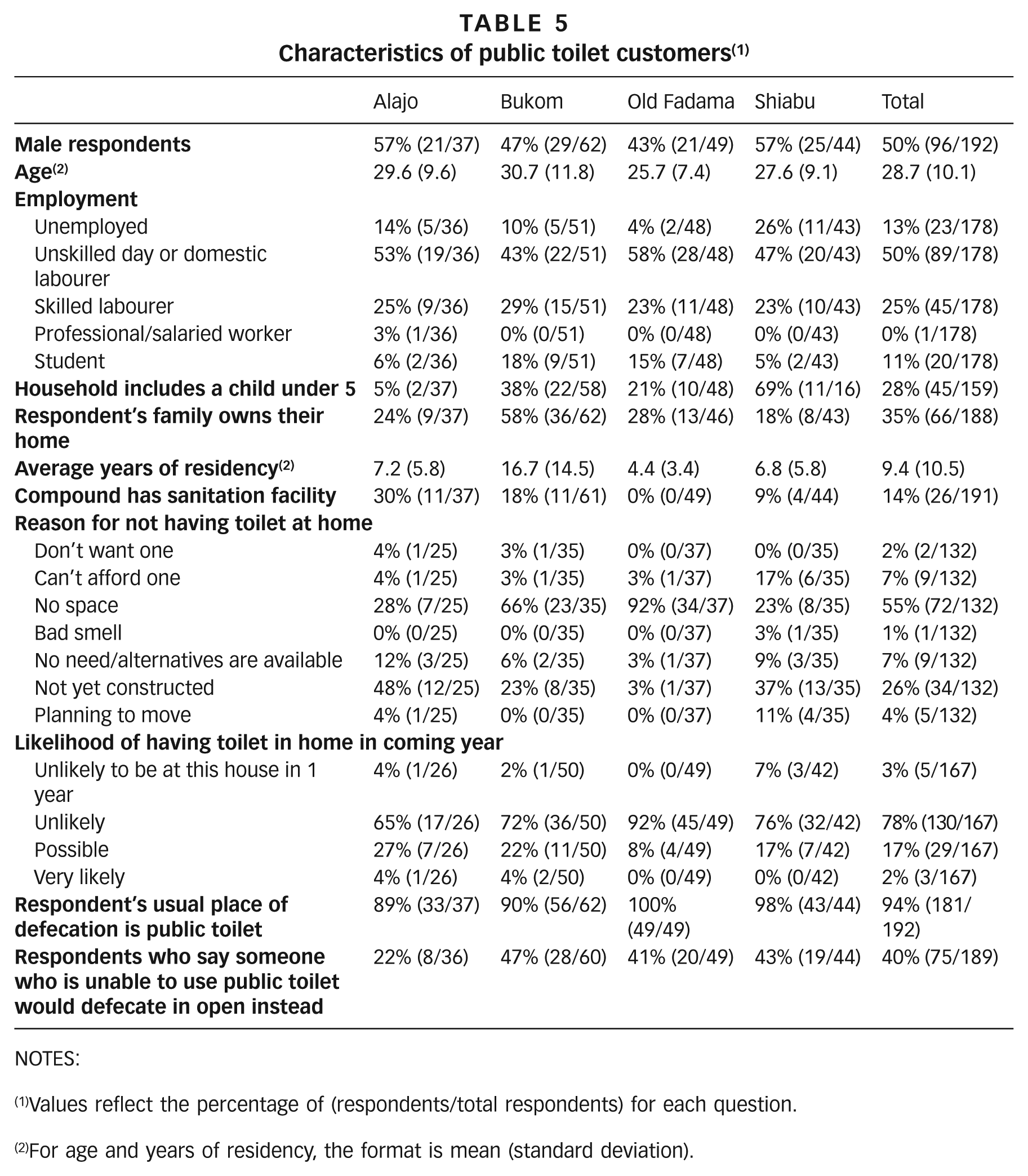
Toilet exit interviews were conducted with 192 respondents, half of them males (Table 5). The average age of respondents was 29 years. Respondents came from various employment backgrounds, although half (50 per cent) described themselves as unskilled labourers. The majority of respondents in most neighbourhoods were renters, with the exception of Bukom, where 58 per cent of respondents came from families that owned their homes. Only 14 per cent (0 per cent in Old Fadama to 30 per cent in Alajo) of respondents had a toilet in their compound. Lack of space was cited by the majority of respondents in Bukom and Old Fadama for not having a sanitation facility at home, while the most common reason in Alajo and Shiabu for not having a home sanitation facility was that respondents planned to construct a toilet but had not yet. The majority of respondents (78 per cent) thought it was unlikely that they would have a toilet in the coming year. A public toilet was the usual place of defecation for 94 per cent of respondents. Finally, when asked what others would do if public toilets were not available, 40 per cent of respondents cited open defecation as the alternative if public toilets were not available.
Characteristics of public toilet customers (1)
NOTES:
Values reflect the percentage of (respondents/total respondents) for each question.
For age and years of residency, the format is mean (standard deviation).
d. Opinions of public toilet customers
Two discussions were held in Bukom, one with a group of seven women and the other with eight men. Two other discussions were held in Old Fadama, with seven women and eight men.
Open defecation and deterrents to public toilet use
Participants in all groups (except women in Old Fadama) reported that open defecation occurred in their communities. Open defecation was described to include takeaways (defecating into a plastic bag), the use of chamber pots in homes and then dumping of contents into nearby gutters, and squatting by a beach or lagoon to defecate. In Bukom, beaches were reported to be the most common place for defecation. “So as for the beach; if anyone says he is going to defecate, it’s at the beach. The women have where they squat and the men as well.” (woman, Bukom)
The practice of open defecation was attributed to all members of the community for various reasons. For instance, children were said to defecate in the open because public toilets were designed for adults and therefore unsuited for children. The elderly were said to defecate in the open because of mobility limitations. “Like the aged, there are some old women who cannot use the public toilets so when she takes her chamber pot, she will place a bag in it and defecate into it then she dumps it into the gutters.” (woman, Bukom)
The cost of public toilets was described as the most important reason for open defecation. Public toilets were reported to cost between 10 and 30 pesewas across all neighbourhoods. This cost was generally considered burdensome. “If we have 10p and toilet attendants will not accept, our only option is to look for the gutter and do our own thing there.” (man, Bukom) This burden was exacerbated for those with many children and those with illnesses such as diarrhoea. “Also if some [one] is having a running tummy and has been to the toilet five times, he will buy the take away [rubber bag] and [defecate] inside because they can’t pay at all times.” (man, Old Fadama)
Dissatisfaction with public toilet cleanliness and service
Participants described their public toilet experiences in terms of the cleanliness of the toilet and the treatment by toilet operators. Cleanliness was reported to differ greatly between toilet facilities but was generally inadequate. “The ones for the adults are not neat and that of the children too is a problem.” (woman, Bukom)
The level of cleanliness of toilet facilities was attributed to the level of care that toilet operators showed for the toilet’s customers. “There is the need for the toilet attendant to constantly check the place but because she is fat, she is not able to do that, so the toilet owners should pay people to clean the place and remove all the cobwebs.” (woman, Bukom) “There are some people that if you tell them their toilets are not good, they will insult you.” (woman, Old Fadama)
Low likelihood of having private toilets and demand for improved public toilets
Participants cited the benefits of not having to rely on public toilets. “With your household toilet you will not use it with anybody so you will have to clean the toilet with your own hand, you will not have to hire anyone to come and clean for you. You may not have money to pay the person. This can put an end to the dirty nature of our community.” (man, Bukom)
Despite the benefits of a household toilet, the lack of space for construction was cited as the biggest barrier to household toilet ownership among discussion participants. “You see people have money to build toilet but the problem is the land and even if you have the land and money they will not be allowed you because of build ups [structures] in the community.” (man, Old Fadama) “We have that mindset [intention to build toilets] but we do not have the land to do it.” (woman, Old Fadama)
Improvements in the quantity and quality of public toilets were in high demand in all neighbourhoods, with some respondents indicating that they were willing to pay more for such improvements. “No it is not enough. The NUMBER OF toilets in the community is not enough because when you come here in the morning you find people in a long queue if you are not fortunate and IF you have running tummy you will [defecate] into your pants. I tell you all you have to do is to run to the beach.” (man, Bukom) “In my place in the morning, hey, you will find long queue, if you are not careful and you have [running] tummy you will have to run to some other place.” (man, Old Fadama) “There are some toilets which you don’t regret paying money to use. An example is the one in Kwansa; you pay 30 pesewas for a tissue and there is water and soap for handwashing so you don’t regret paying that amount and it is nice.” (woman, Bukom)
IV. Discussion
Our findings are consistent with several other recent mixed-methods investigations into the sanitation situation in dense, low-income, urban neighbourhoods.(24) In general, though, few studies specifically of public toilets and their customers have been conducted, despite heavy reliance on this form of sanitation in places such as Accra. Household sanitation coverage was found to be 28 per cent across all four neighbourhoods. This is consistent with official estimates that 72 per cent of Ghana’s urban population uses shared sanitation facilities.(25) There was great variation in household sanitation coverage between neighbourhoods, which corresponded with reliance on public toilets; greater numbers of public toilet customers were reported and observed in Bukom and Old Fadama, where household sanitation coverage was lowest. Findings from Bukom suggest that such low household sanitation coverage persists even after many years of residency in a neighbourhood. Focus group respondents and public toilet exit interviewees mostly attributed this to lack of space for toilet construction rather than insecure land tenure, although again, comparing the characteristics of respondents in our household survey to the public toilet users we surveyed, we see suggestive evidence that tenants and those who are newer to their neighbourhood are more likely to use public toilets. Most public toilet customers did not foresee acquiring a toilet in the coming year. Furthermore, this coverage issue persists even after the government’s re-energized attempt to enforce a policy that requires landlords to provide household sanitation. These findings indicate that public toilets are, and will remain, a central feature of urban sanitation in Accra.
Despite heavy reliance on public toilets, they do not appear to be used at the same rate by all members of the community. Public toilet customers were mostly adult men and women, and were less likely to be members of households with children under age five (at least during the times of day that the household surveys and interviews with public toilet customers were administered). As with the study of communal latrine use in Bophal, India, however, in three of the four study neighbourhoods we were more likely to observe men using the facilities than women, for reasons that are not clear.(26) Furthermore, children were not observed to be routine patrons of public toilets, suggesting that a large share of the population in these neighbourhoods is defecating in the open, since no other option aside from public toilets is available to those who do not have toilets at home. This observation was consistent with the statements of focus group discussion participants that children and the elderly are poorly served by public toilets because of design and mobility limitations. It is also consistent with previous research that has come to the same conclusion.(27) Young children and the elderly often struggle to maintain their balance and position themselves over squat holes designed for adults without coming in contact with soiled surfaces. More research is needed to better understand why school-aged children, who do not face these same challenges, also do not use public toilet facilities.
Factors such as cost and cleanliness were reported to deter public toilet use and contribute to the problem of open defecation in all neighbourhoods. Costs reportedly become especially burdensome for families with more children and those with diarrhoeal illnesses. In keeping with findings from the study of shared toilet users in Kampala, Uganda, public toilet users cited lack of cleanliness as a major concern.(28) Public toilet conditions varied widely within and between neighbourhoods. Observations found a mix of toilet technologies ranging from the simplest form of technology, bucket/pan toilets, which were exclusive to Old Fadama, to pour flush systems, exclusive to Alajo. Observed cleanliness followed a similar trend, with Old Fadama’s toilets having greater instances of observed flies, faeces and insecure stances and Alajo having the least, although flush technology did not preclude the possibility of poor conditions. The relationship between cleanliness and observed patronage is inconclusive, however. While on the whole more people were observed to patronize less clean toilets in Bukom and Old Fadama, this may be more a function of lower household sanitation coverage in those neighbourhoods than an indication that customers do not mind such suboptimal facilities. Cost was even cited as a fair exchange for better services. Public toilet customers recommended the construction of more toilets, improvements in cleanliness, and provision of soap and water for handwashing as key ways to improve toilets in their neighbourhoods.
Our findings suggest that the blanket categorization of public toilets as unimproved sanitation may warrant reconsideration. First, heavy reliance on public toilets means that they must be considered as part of the sanitation context in Accra’s low-income urban neighbourhoods. Second, differences in patronage, cleanliness, toilet technologies and services such as handwashing facilities indicate that public toilets are not all the same. If they are well managed and more widely available, public toilets represent a viable sanitation option for those without a household toilet and with little prospect of having one in the near future. If public toilets are accessible and well managed, they could help avert behaviours that negatively impact public health such as open defecation. Nonetheless, this study finds that children, who comprise a large share of the population of Accra, are unlikely to use public toilets, and there is suggestive evidence that members of households with young children are also less likely to use these facilities. Such considerations are key to future sanitation investments in Accra’s low-income neighbourhoods and warrant further investigation.
More generally, the current discourse on a potential re-categorization of some types of shared sanitation among improved options sanctioned by governments has been silent on the particular form of shared sanitation we describe in this paper: the pay-per-use public toilet. JMP standards fail to recognize the importance of public toilet facilities in many densely populated, low-income neighbourhoods such as those we studied in Accra. The diversity of conditions we found suggests that in practice, public toilets, like many other forms of sanitation, are not easily categorized. But the silence on this topic is also detrimental, as JMP definitions affect government priorities, and improvements in public toilet facilities would benefit many urban dwellers in low-income countries.
Footnotes
Acknowledgements
The authors wish to thank Matt Freeman and Monique Hennink of Emory University and Adam Biran, London School of Hygiene and Tropical Medicine, for suggestions during the course of the study and comments on the manuscript; we are also grateful for suggestions from two anonymous reviewers. We are deeply indebted to the residents of the study neighbourhoods for their participation in the research, and especially to our community liaisons for facilitating the data collection. Eugene Larbi, Managing Director of TREND, was a staunch supporter of the study and the TREND enumerators worked tirelessly to ensure the highest-quality data were collected.
Funding:
This study was funded by the Bill & Melinda Gates Foundation.
1.
The term “slum” usually has derogatory connotations and can suggest that a settlement needs replacement or can legitimate the eviction of its residents. However, it is a difficult term to avoid for at least three reasons. First, some networks of neighbourhood organizations choose to identify themselves with a positive use of the term, partly to neutralize these negative connotations; one of the most successful is the National Slum Dwellers Federation in India. Second, the only global estimates for housing deficiencies, collected by the United Nations, are for what they term “slums”. And third, in some nations, there are advantages for residents of informal settlements if their settlement is recognized officially as a “slum”; indeed, the residents may lobby to get their settlement classified as a “notified slum”. Where the term is used in this journal, it refers to settlements characterized by at least some of the following features: a lack of formal recognition on the part of local government of the settlement and its residents; the absence of secure tenure for residents; inadequacies in provision for infrastructure and services; overcrowded and sub-standard dwellings; and location on land less than suitable for occupation. For a discussion of more precise ways to classify the range of housing sub-markets through which those with limited incomes buy, rent or build accommodation, see Environment and Urbanization Vol 1, No 2 (1989), available at ![]() .
.
2.
Rydin, Y, A Bleahu, M Davies, J D Dávila, S Friel, G De Grandis, N Groce, P C Hallal, I Hamilton, P Howden-Chapman et al. (2012), “Shaping cities for health: complexity and the planning of urban environments in the 21st century”, The Lancet Vol 379, No 9831, pages 2079–2108.
4.
5.
7.
12.
Ayee, J and R C Crook (2003), “ ‘Toilet Wars’: Urban Sanitation Services and the Politics of Public-Private Partnerships in Ghana”, Institute of Development Studies Working Paper Series No 231.
13.
14.
16.
Wegelin-Schuringa, M and T Kodo (1997), “Tenancy and sanitation provision in informal settlements in Nairobi: revisiting the public latrine option”, Environment and Urbanization Vol 9, No 2, pages 181–190; also Burra, S, S Patel and T Kerr (2003), “Community-designed, built and managed toilet blocks in Indian cities”, Environment and Urbanization Vol 15, No 1, pages 11–32.
17.
Biran, A, M W Jenkins, P Dabrase and I Bhagwat (2011), “Patterns and determinants of communal latrine usage in urban poverty pockets in Bhopal, India”, Tropical Medicine and International Health Vol 16, No 7, pages 854–862.
18.
Tumwebaze, I K, C G Orach, C Niwagaba, C Luthi and H J Mosler (2013), “Sanitation facilities in Kampala slums, Uganda: users’ satisfaction and determinant factors”, International Journal of Environmental Health Research Vol 23, No 3, pages 191–204.
19.
City of Accra, Ghana (2010), Consultative Citizens’ Report Card.
21.
See reference 14.
22.
A compound house, consisting of multiple dwellings (often only one or two rooms) opening onto a common courtyard, is a common form of housing in Accra. Compound houses are typically occupied by extended families or tenants of a shared landlord.
23.
See Owusu, M (2013), “Community-managed reconstruction after the 2012 fire in Old Fadama, Ghana”, Environment and Urbanization Vol 25, No 1, pages 243–248. See also reference 13, page 108, Table 9.20, which reports that the average annual per capita income in the Greater Accra Metropolitan Area was 564 cedis (at an exchange rate of 0.92 cedis per dollar in 2006 at the time these data were collected, that translates to less than US$ 2 per day).
24.
See Joshi, D, B Fawcett and F Mannan (2011), “Health, hygiene and appropriate sanitation: experiences and perceptions of the urban poor”, Environment and Urbanization Vol 23, No 1, pages 91–111 for a multi-country review; Adubofour, K, K Obiri-Danso and C Quansah (2013), “Sanitation survey of two urban slum Muslim communities in the Kumasi metropolis, Ghana”, Environment and Urbanization Vol 25, pages 189–207 for conditions in Ghana’s second largest city; or Owusu, G (2010), “Social effects of poor sanitation and waste management on poor urban communities: a neighborhood-specific study of Sabon Zongo, Accra”, Journal of Urbanism: International Research on Placemaking and Urban Sustainability Vol 3, No 2, pages 145–160 for a discussion of the societal consequences of inadequate sanitation in another low-income neighbourhood in Accra.
26.
See reference 16, Wegelin-Schuringa and Kodo (1997) and ![]() .
.
27.
See Bartlett, S (2003), “Water, sanitation and urban children: the need to go beyond “improved” provision”, Environment and Urbanization Vol 15, No 2, pages 57–70.
28.
See reference 18.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.