
Abstract
Needle vibration tissue cutting is a method that has been shown to reduce tissue cutting force and thereby improve needle position accuracy inside the body. Needle accuracy is crucial for minimally invasive needle operations such as the radiation cancer treatment of brachytherapy. This article uniquely determines the importance of needle geometry in minimizing cutting force in needle vibration tissue cutting. This article also determines how vibration specifically affects cutting force. This new information was found by performing needle cutting experiments with five varying conical tipped needles being inserted into ex vivo bovine liver as well as a polyurethane sheet at varying vibratory amplitudes and frequencies. Results show that applying vibration to sharper needles greatly reduced the insertion force by up to 67%, where the blunter needles saw diminishing benefits. The tissue phantom experiments showed that vibration reduced the force needed to propagate the created crack but showed no improvement over the initial puncture force. This greater understanding of needle vibration tissue cutting can lead to improved needle geometry designs that work with vibration to reduce tissue cutting force.
Introduction
Needles are very commonly used in medical procedures as a minimally invasive medical device. They are used in drug delivery, tissue biopsy, blood drawing, brachytherapy, and many other procedures. 1 Many procedures rely on high needle accuracy to be effective. For example, brachytherapy is a procedure where precise needle accuracy is required for placing permanent radioactive seeds inside the body to kill cancerous cells. Inaccurate placement of the seeds can lead to the procedure being ineffective as well as further complications in the patient. 2 In addition, false diagnoses can occur when the needle tip is not located precisely inside the body while performing biopsies. When the needle used in the procedure is inserted as shown in Figure 1(a), the forces acting on the needle cause the needle to bend and deflect away from the desired path, as can be seen in Figure 1(b). In addition, unlike traditional manufacturing where the workpiece is rigidly fixed, the tissue is free to move, as can be seen in Figure 1(c). The combination of needle and tissue deflection causes the needle tip to miss the intended target. Lower insertion forces and more efficient cutting geometries have shown to reduce tissue and needle deflections.3,4
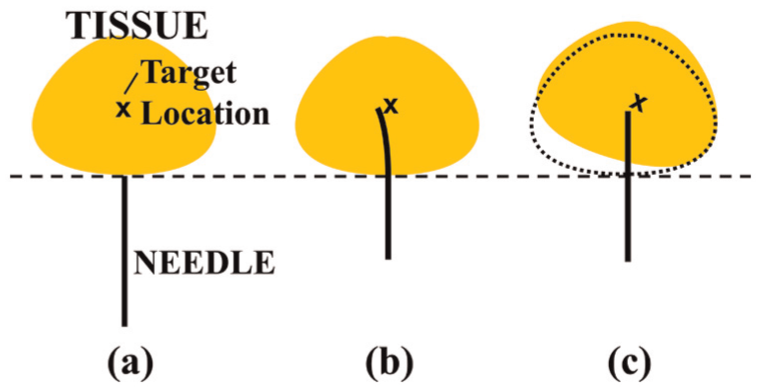
Needle shown (a) before tissue insertion, (b) bending as a result of insertion forces, and (c) deflecting tissue as a result of insertion forces.
Previous work by other researchers has been performed to reduce the insertion force of needles. This includes creating microneedles,5–7 increasing the insertion speed,8–12 and altering tip geometries.13–15 Researchers have explored how the rake and inclination angles of the medical tool geometry can be measured16–18 and how this geometry affects needle insertion force. 16 Han et al. 19 further modeled the geometries of various needle tips to improve needle design. Wang et al. 20 investigated the effects of grind angles of lancet point needles on insertion forces. In addition, the application of an axial vibration has been shown to reduce the insertion force.
Vibration cutting has been utilized in traditional manufacturing processes with multiple benefits. Ultrasonic vibration has shown to reduce burr formation,21,22 create smoother finishes,23–26 and reduce cutting force.24,27,28 With vibration cutting being used in traditional manufacturing for decades, there has been optimization of vibratory parameters to achieve the best machining results for different workpiece materials and cutting processes.29–31
Applied axial vibration has shown to reduce the insertion force in tissue by several researchers. The addition of vibration can reduce the force needed to insert microneedles (needles that are 100 µm in diameter or less) by up to 70%.32,33 Huang et al. 34 have shown that ultrasonic vibration can reduce the insertion force of 27-gauge hypodermic needles. The optimization of vibratory parameters has only been briefly explored. Barnett et al. 35 tested a wide range of vibratory parameters to determine their effect on the insertion force of various sized hypodermic needles. Begg and Slocum 36 similarly tested the insertion force of lancet needles at varying frequencies and amplitudes. However, the effects of vibration and cutting geometry of the needle together are yet to be explored: the focus of this article. This article uniquely determines the importance of needle geometry in minimizing cutting force in needle vibration cutting. This article also determines how vibration specifically affects cutting force.
This article focuses on investigating the effects of vibration and needle geometry together on insertion force. Experiments are performed to insert conical tipped needles of different grind angles into ex vivo bovine tissue at a wide variety of vibratory parameters (amplitude and frequency). In addition, phantom tissue is utilized to verify results. This article describes the geometry utilized in the study, the experimental procedure of testing the effect of geometry on vibration tissue cutting, the results from the experiments, and conclusions drawn.
Needle geometry
To determine how geometry and vibratory parameters are related, the geometry of the needle must be quantified. For this study, the volume of the needle from the tip of the needle was considered. Five conical tipped needles were used in this study as shown in Figure 2 to isolate the effects of one geometric feature: the grind angle ξ. Needles such as lancet point needles have complex cutting faces and angles, making it difficult to fully understand the relationship between geometry and vibration. 16 The symmetric nature of the conical tip does not instill transverse forces on the needle which can cause the needle to deflect. 37 Blunter geometry needles are being utilized in medical procedures to reduce accidental punctures.38–41 However, the blunt cutting geometry requires greater insertion force to puncture tissue. 42
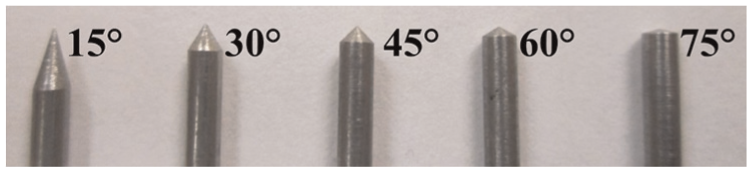
Conical tipped needles with varying grind angles, ξ.
The volume for the conical tipped geometry can be expressed in terms of the grind angle ξ and the outer radius ro, as can be seen in Figure 3. The volume of the conical needle for a given depth z is shown in equation (1). This equation was developed based on Eudoxus’ method for calculating the volume of a cone

where the length of the needle tip zl, as seen in Figure 3, is given by

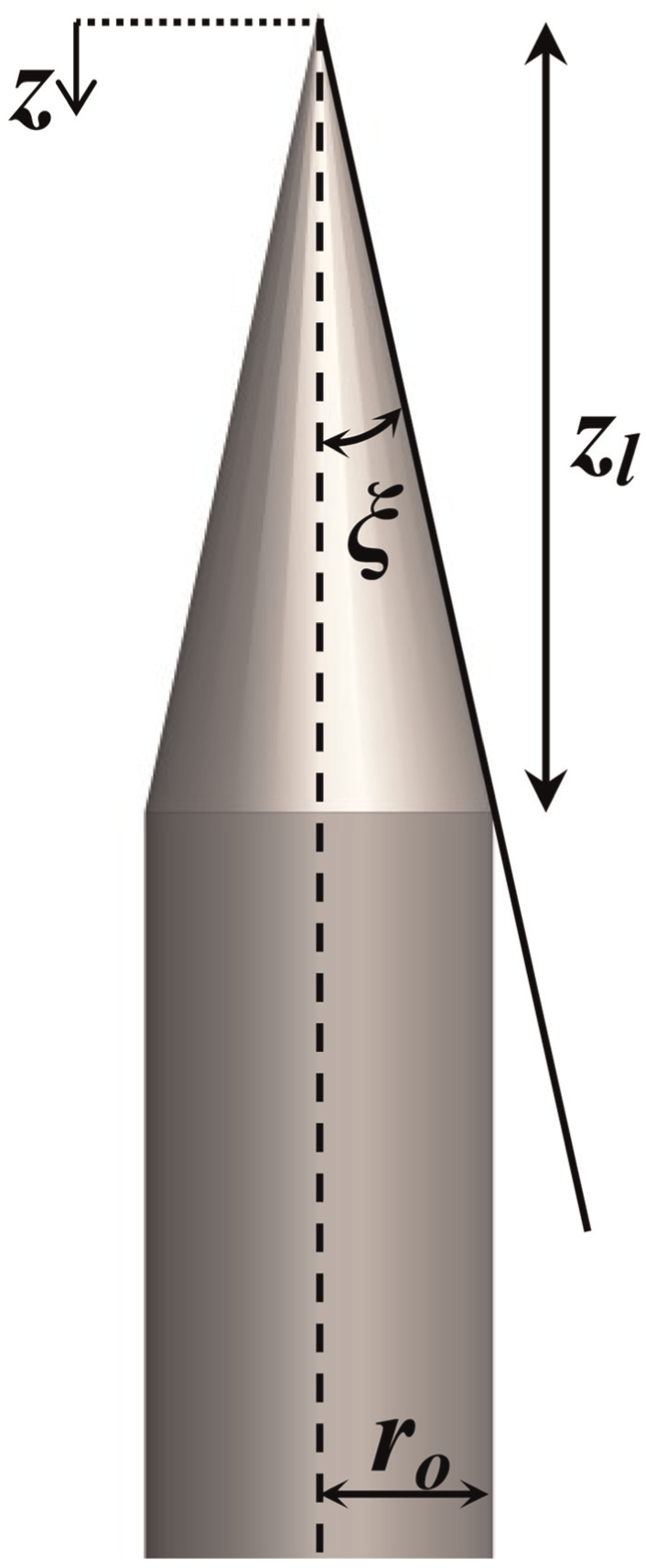
Geometry of conical needle tip.
Five conical tipped needles made of 304 stainless steel were considered with varying grind angle ξ. The grind angles utilized were 15°, 30°, 45°, 60°, and 75°. The grind angles were verified by measuring the angles with a stereomicroscope (Zeiss, Oberkochen, Germany). Digital pictures of the needle tips were taken, and the grind angles were measured using Axiovision software (Zeiss). The 304 stainless steel was utilized because it is the most commonly used needle material. This material is biocompatible, has good corrosion resistance, and is inexpensive for its high tensile strength and high modulus of elasticity. All needles had an outer diameter of 1.6 mm, equal to that of a 16-gauge needle.
Figure 4 shows the volume of the needle tip at varying depths for the five different grind angles. As can be seen, the steeper the grind angle (lower ξ), the lower the rate of volume change. The lower volume change rate allows the needle to fracture the tissue with less force. 43
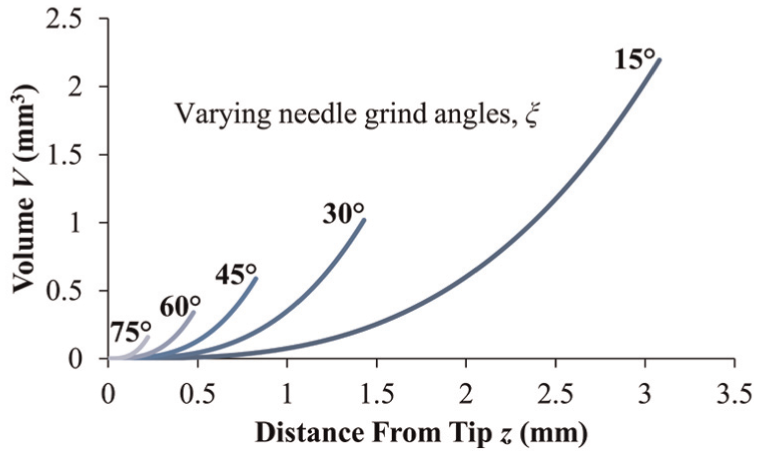
Volume of needle tip at a given distance from the tip for each given grind angle.
Experimental procedure
To determine the effects of vibration and geometry on insertion force, two experiments were conducted as outlined in Table 1. First, the needles were inserted into ex vivo bovine liver. Bovine liver was used in this study due to its consistency throughout the portion being tested. Bovine liver has been used in previous tissue cutting studies.16,44,45 However, tissue cutting experiments in ex vivo tissue have been shown to have standard deviations of up to 25%. 46 To verify the ex vivo tissue results, a second experiment was conducted. The needles were inserted into phantom tissue made from a 1.6-mm-thick polyurethane sheet of Shore hardness 40A. Polyurethane sheets have been used in other studies to simulate skin dermis.47,48 The phantom material does not produce as accurate of force profiles as ex vivo tissue but yields more consistent results.
Outline of experiment procedures.

Ex vivo tissue procedure
Needle insertion testing apparatus
This study utilized the experimental setup shown in Figure 5. It utilizes a linear motor (Dunkermotoren, Bonndorf, Germany) to insert the needle into the bovine liver at a constant rate. Mounted to the slide is a piezoelectric actuator (Physik Instrumente, Karlsruhe, Germany) which provided the vibration during the tests. The force was measured with a six-axis force sensor (ATI Industrial Automation, Apex, NC, USA) mounted on an adjacent table to isolate it from the vibrations. The force sensor was mounted underneath the tissue box. Force and position data were collected for each trial. The data were sampled at four times the vibration frequency to accurately measure the force.
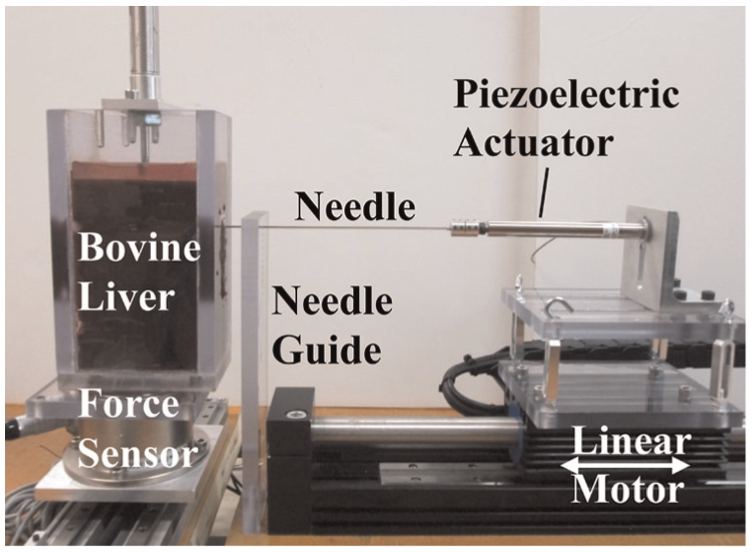
Force measurement setup for ex vivo tissue experiment.
Because workpiece holding is important in consistently cutting soft materials as shown by the study done by Shih et al. 49 on cutting elastomers, the bovine liver was held in a box, and a slight pressure of 11.65 kPa was applied to the liver. The box had a slot on the front to allow the needle to pass into the tissue. The needle was passed through the middle of the tissue to eliminate the effects of boundary conditions.
Tissue damage caused by the insertion of these needles was a factor that was not directly measured in these experiments. However, the needle force does give some indication as to the amount of damage that would be seen on the tissue. Lower force will create less pressure and bruising on the tissue. Needles with sharper geometry will produce less tissue damage by creating less tissue fracture. To more precisely quantify tissue damage, future studies will perform histological evaluations.
Experimental design
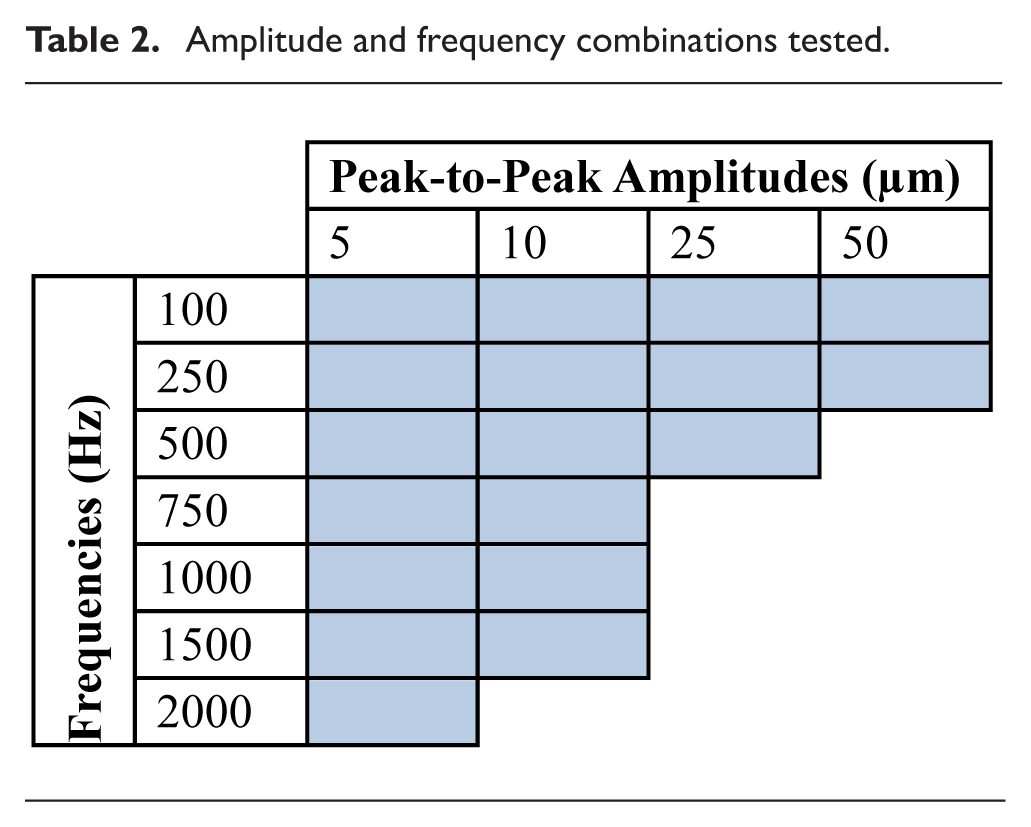
An experiment was designed to test the insertion force of different angled conical needles through bovine liver at various vibration frequencies and amplitudes. The steady insertion speed was kept at a constant of 1 mm/s, supplied by the linear slide, for all trials. This is to isolate the effects of the vibration as well as the geometry of the needle. The experiment utilized the five different conical tipped needles as described in section “Needle geometry.” Each of the needles was tested at 18 different combinations of amplitude and auditory frequency as listed in Table 2. Each needle was also inserted with no vibration as a control. The combinations test a broad range of frequencies and amplitudes to determine the effects of the vibratory parameters and how they relate to the needle geometry. The limits of frequency and amplitude tested were determined by the amount of power that could be safely put into the piezoelectric actuator. Having both high frequency and high amplitude requires a large amount of power be applied to the piezoelectric actuator. Excessively high electrical power will cause the actuator to generate large amounts of heat and break the piezoelectric ceramic. The needle was inserted five times at each parameter combination including the control. Each trial was inserted into a new location in the tissue to avoid inserting into the same hole as a previous trial.
Amplitude and frequency combinations tested.
Phantom tissue procedure
Needle insertion testing apparatus
The test setup shown in Figure 6 was utilized to insert the needles into a polyurethane sheet to verify the ex vivo results. This setup utilized the same needles, linear motor, piezoelectric actuator, and six-axis force sensor as the previous setup. The polyurethane sheet was held between two plates to ensure consistent boundary conditions between trials. The needle was able to pass completely through the sheet unless it bent under excessive force.
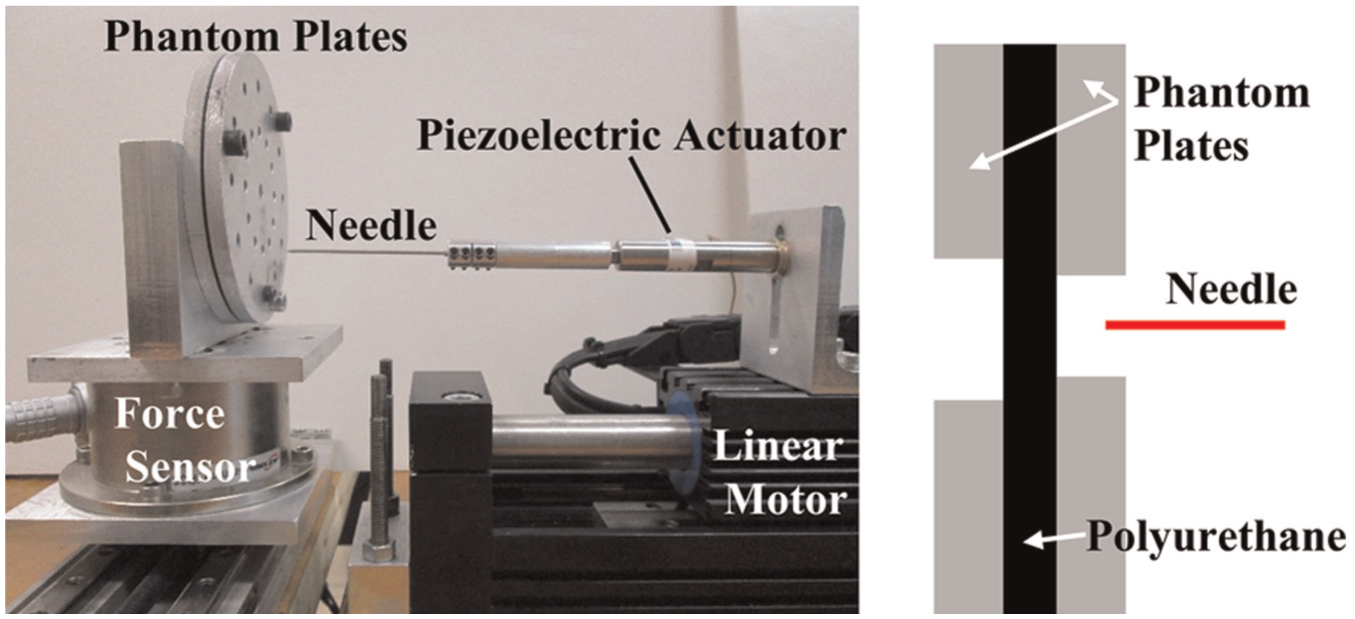
Force measurement setup for phantom tissue study.
Experimental design
The 15°, 30°, 45°, 60°, and 75° grind angle needles were inserted through the polyurethane sheets. For this study, only two vibratory combinations were utilized in addition to the control insertion, as can be seen in Table 3. These parameters were chosen based on the results from the ex vivo tissue study, as well as their locations at the extremes of the combinations tested in the ex vivo tissue study. Each needle was inserted six times for each vibratory parameter. The 60° and 75° grind angle needles were inserted until they started to bend, which occurred near 25 N. The other needles were successfully inserted all the way through the phantom material.
Phantom vibratory experimental space.

Results and discussion
Ex vivo tissue results
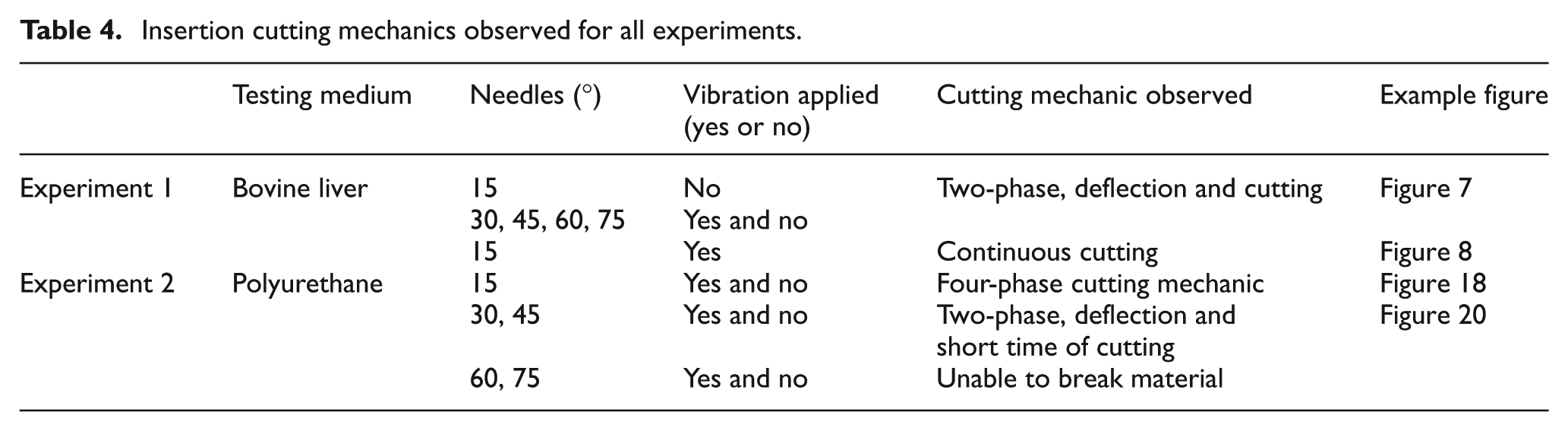
Different cutting mechanics were observed based on the different experimental parameters as summarized in Table 4. For the ex vivo tissue experiments, it was shown that for 30°, 45°, 60°, and 75° needles with and without vibration had a typical two-phase cutting mechanic, as shown in Figure 7. This two-phase cutting mechanic was also shown in 15° needles without vibration. In phase I, the tissue deflects and the force gradually rises. In phase II, the tissue is cut by the needle. There can be many rises and falls of the force as the needle penetrates further into the tissue, repeating many cycles of phase I and phase II. The steady increase in force is due to more of the needle being inside the tissue, which increases the friction force. The insertion force is the puncture force that occurs at the first transition between phase I and phase II as illustrated in Figure 7.
Insertion cutting mechanics observed for all experiments.
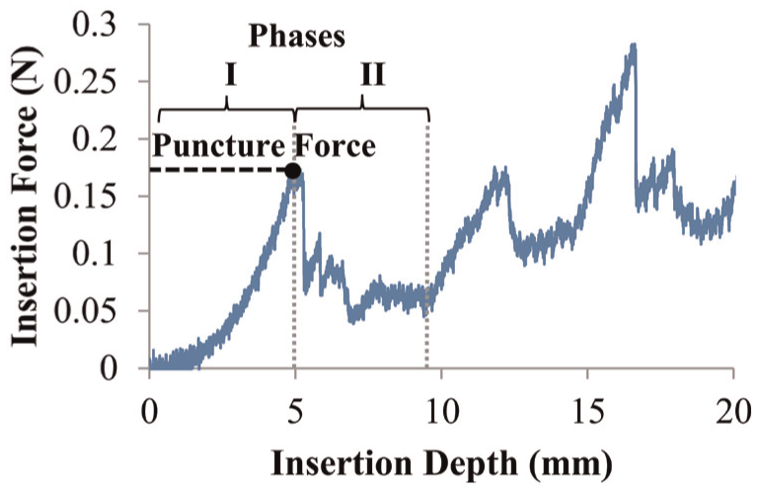
Cutting mechanic of deflection and then cutting shown in insertion force for 45° grind angle needle going into bovine liver without applied vibration.
The insertion force for the 15° grind angle displayed a different cutting mechanic with the vibration applied, as shown in Figure 8. Without applied vibration, the needle cutting mechanic was the same as in Figure 7, with phase I and phase II distinctly present. With the vibration applied, the needle geometry in conjunction with vibration was sharp enough to cut without phase I and phase II being easily distinguishable from each other. This is evident by the constant increase in force as the needle is inserted deeper. This was true for all vibratory combinations tested. This cutting mechanic is important because the needle inserts into the tissue without large deflections, which can lead to better needle placement accuracy, important for many medical procedures. For the 15° grind angle trials with vibration applied, the insertion force was determined as the force at 7.5 mm insertion depth for all trials. This depth was chosen because it is the average insertion depth of the puncture force of the 15° grind angle control insertions. A 7.5 mm is also twice the tip length for the 15° grind angle needle, allowing for the complete outer radius of the needle to enter the tissue.
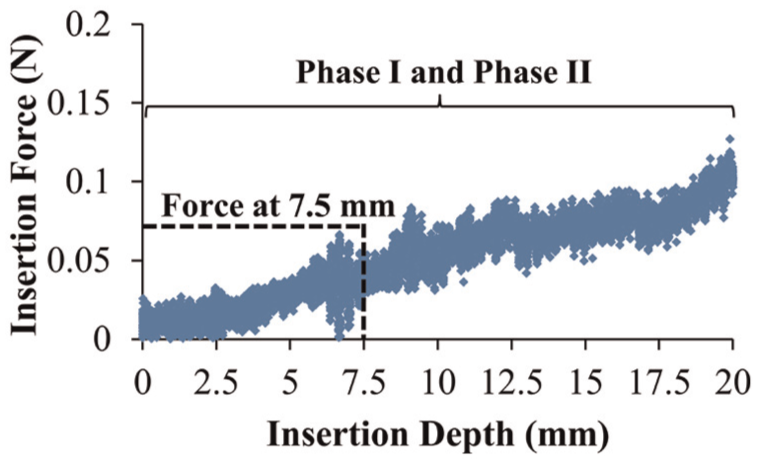
Cutting mechanic of continuous cutting shown in insertion force for 15° grind angle with vibration into bovine liver.
The needles tested in bovine liver showed oscillations in the force graphs as illustrated in Figures 7 and 8. This is a result of the tissue moving in response to the needle insertion. Tissue deflection and tissue cutting create oscillating forces which are detected by the force sensor. This oscillation in force is greater when vibration is applied to the needle.
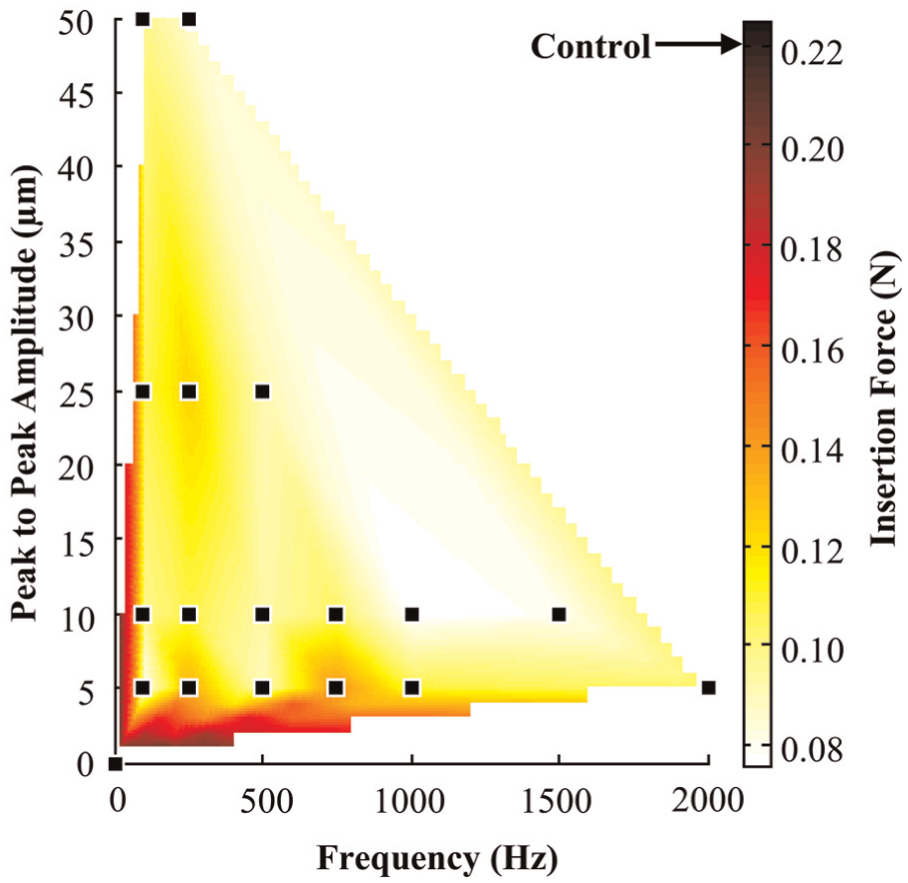
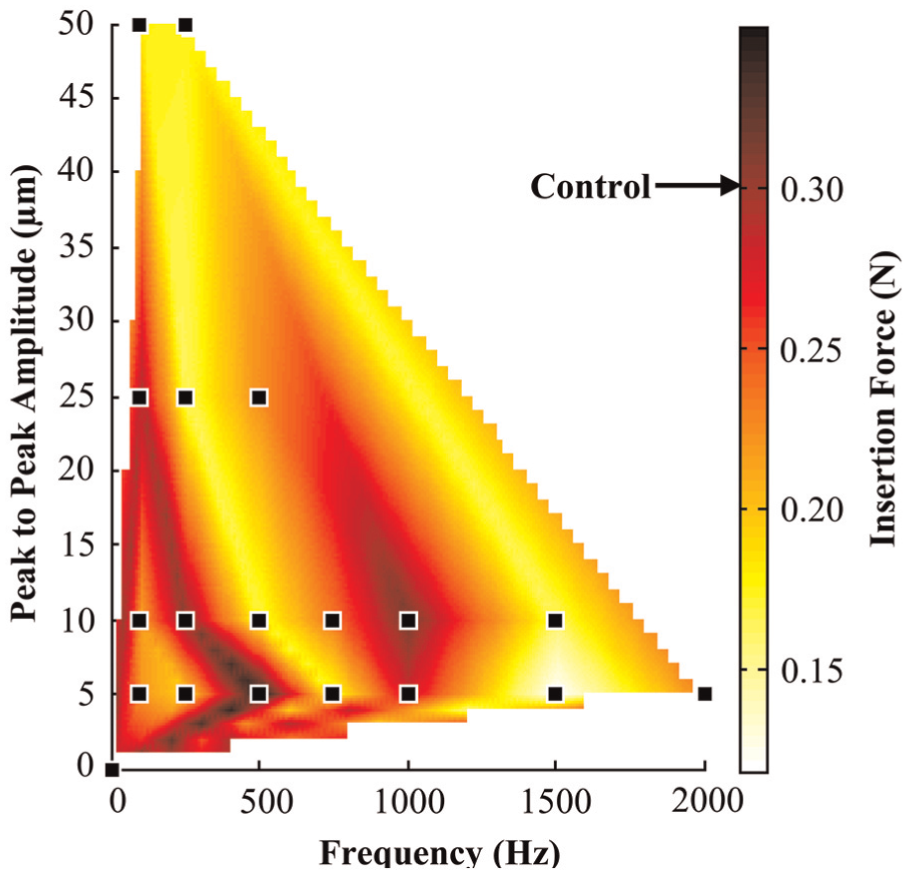
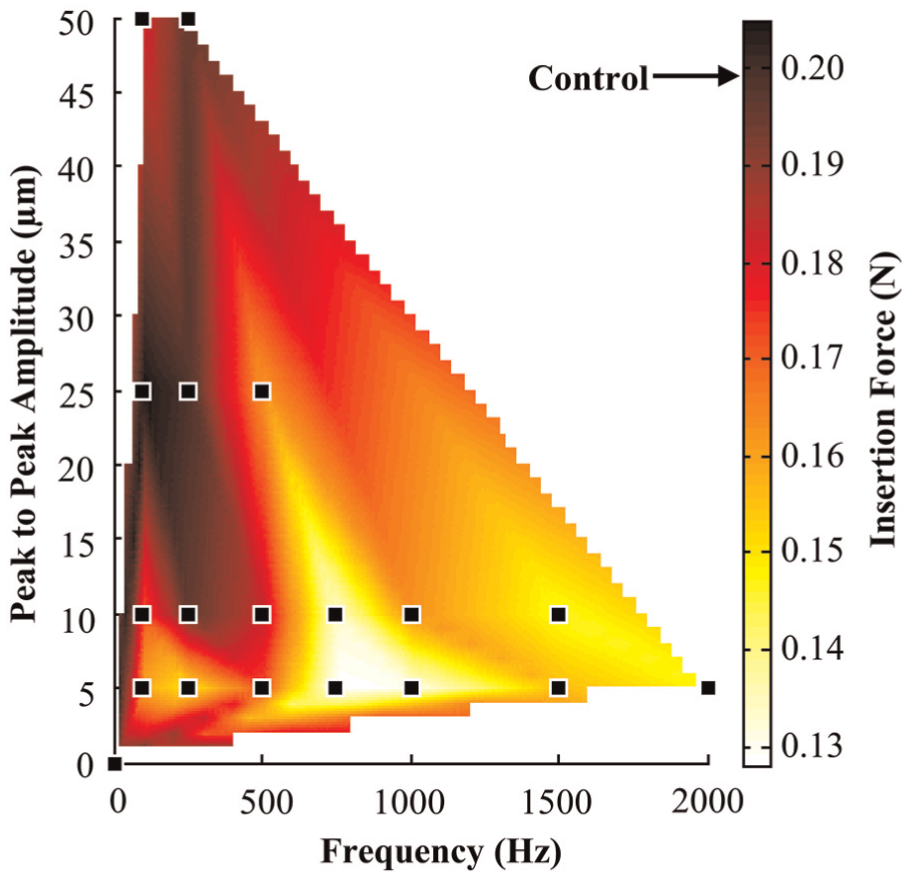
The results for the insertion force trials were averaged across the five trials at each set of parameters. The results were then plotted against the amplitude and frequency of the vibration. A linear interpolation was conducted to map out the insertion force between tested parameters. This was done for the five different needles separately. The average standard deviation at each data point was 32.5%. This is due to the inherent variability in the liver tissue being tested. The results for the 15°, 30°, 45°, 60°, and 75° grind angle needles are shown in Figures 9–13, respectively.
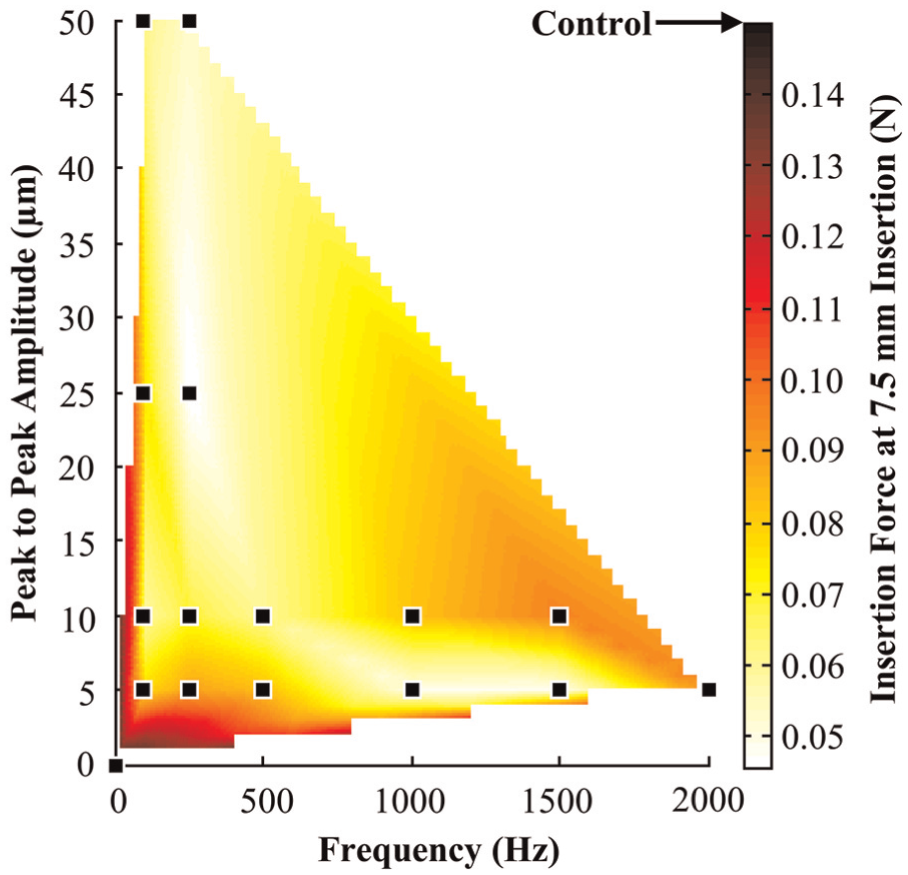
Insertion force map for 15° grind angle into bovine liver.
Insertion force map for 30° grind angle into bovine liver.
Insertion force map for 45° grind angle into bovine liver.
Insertion force map for 60° grind angle into bovine liver.
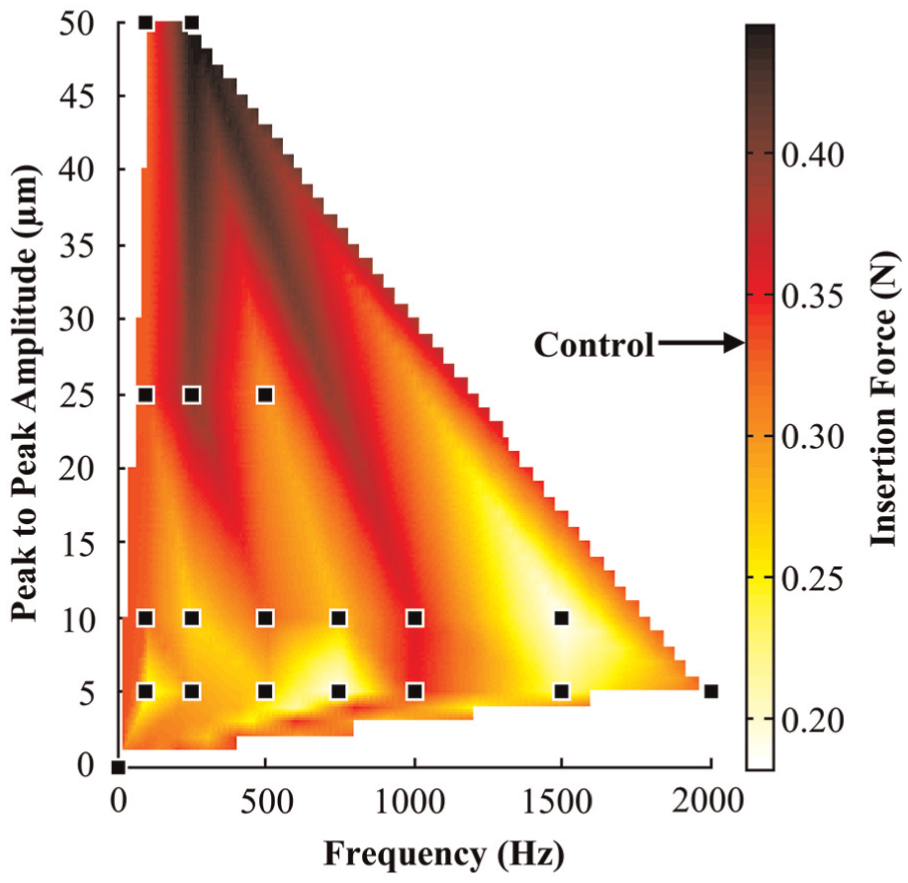
Insertion force map for 75° grind angle into bovine liver.
As the force maps in Figures 9–13 show, there are regions of high and low forces in the plots. All needles show a reduction in force due to applied vibration. To quantify the reduction, the highest force and lowest force were determined for each needle. These maximums and minimums were compared to the control insertion for each needle, and the percent difference from the control insertion is plotted in Figure 14. As can be seen in Figure 14, for the two sharpest needles, the 15° and 30° grind angles, the highest insertion force was the control insertion. The three blunter needles had the highest recorded insertion force occur at one of the vibratory parameter combinations. Figure 14 also shows the greatest reduction in cutting force for each needle. The maximum percent reduction and the vibratory parameters where the minimum occurred are shown in Table 5. As shown, there was not one combination that lowered the insertion force the most for every needle; however, the results show that vibration can be utilized to reduce the insertion force of needle penetration, by up to 67.7%.
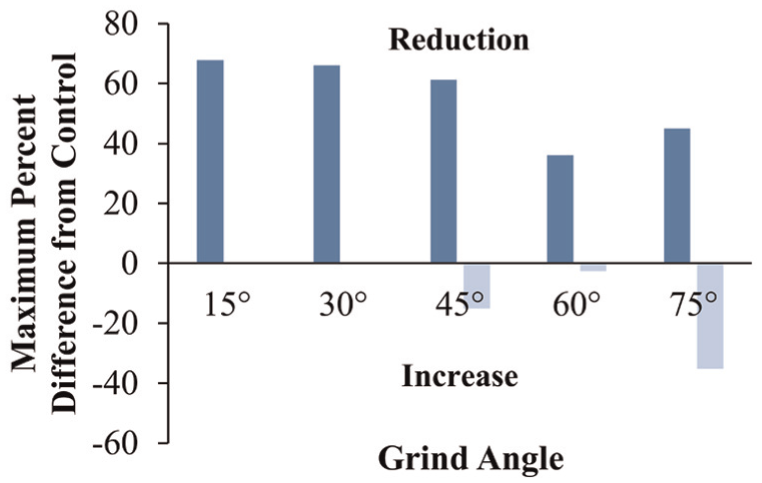
Maximum reduction and increase in insertion force from the control insertion due to applied vibration.
Maximum insertion force reduction for each grind angle and the frequency and peak-to-peak amplitude at which it occurred.

The maximum percent force reduction decreases with the blunter needles. This would imply that geometry has a role in the effectiveness of the vibration in reducing the insertion force. To determine the effect of geometry on vibration tissue cutting, all the vibration trials were averaged together and compared to the control insertion. The results are seen in Figure 15. The results show that for the sharper needles, any applied vibration is beneficial and will reduce the insertion force. However, as the needles become blunter, the overall benefit of vibration begins to decrease and its ability to reduce the insertion force is lost. This implies that the vibration cannot overcome the inefficient cutting geometry of the blunt needles.
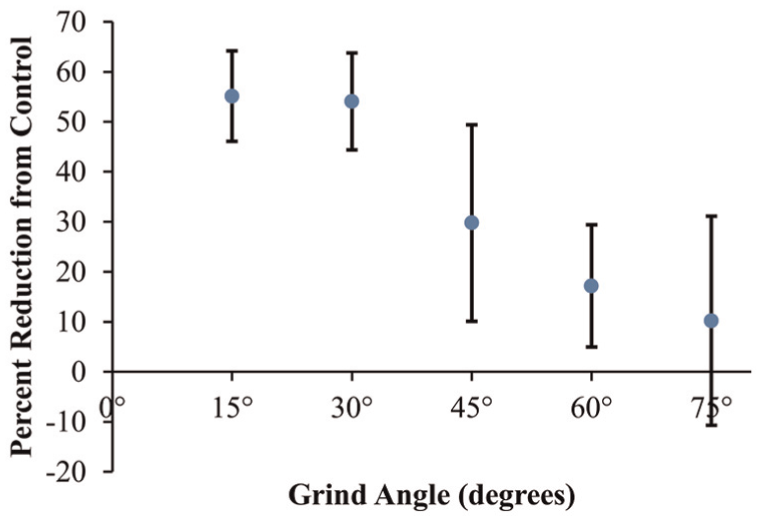
Average reduction in insertion force from the control insertion due to applied vibration.
The force map in Figure 13 for the bluntest needle (75° grind angle) shows that the regions of high insertion force are located at higher amplitudes. This would imply that for blunter geometries, amplitude emerges as a factor for determining the insertion force. To determine the dependence of the amplitude of vibration on insertion force, the insertion forces were averaged at all frequencies at each amplitude. The 75° grind angle needle has greater insertion force at the higher amplitudes as illustrated in Figure 16. The 60° grind angle needle showed an increase in insertion force as the amplitude increased but not as direct as the 75° needle. The 15°, 30°, and 45° grind angle needles did not show general trends with respect to the amplitude of vibration. Linear fits were applied to the data to quantify the relationship between insertion force and amplitude. The rate of increase in the insertion force with respect to amplitude as well as the R2 value for the fit can be seen in Figure 16. The 15° grind angle needle was omitted on the graph for ease of viewing and had a rate of −0.198 mN/µm and R2 value of 0.61. The increase in insertion force with higher amplitude of vibration for the 75° grind angle needle could be due to the blunter geometry not being able to cut the tissue and thus the higher amplitude deflecting the tissue more, increasing the insertion force.
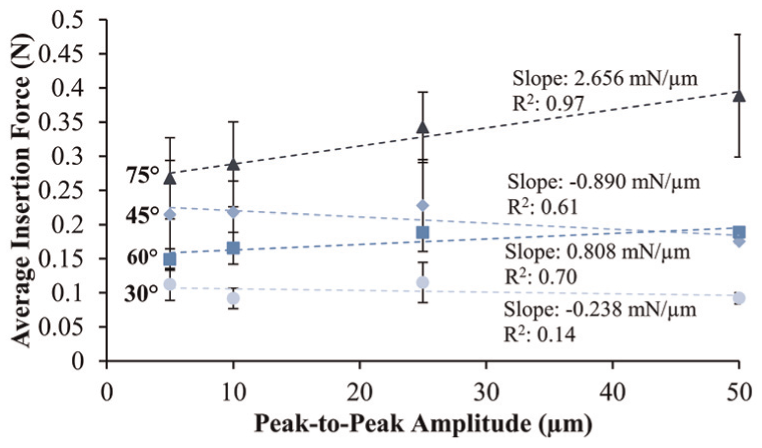
Average insertion forces for 30°, 45°, 60°, and 75° grind angle needles versus amplitude with linear trendlines.
Researchers have shown that by increasing the insertion speed of the needle, the insertion force of the needle through soft tissue is reduced.8,10–12 To determine if the benefit of the application of vibration is due to the increased speed of the needle, the maximum vibratory insertion speed was calculated for each vibratory parameter combination. The maximum vibratory insertion speed was determined by converting the frequency and amplitude to speed by the following equation

where Ai is the amplitude of vibration, fi is the frequency of vibration, and vo is the steady insertion speed. The maximum vibratory insertion speed is plotted for each vibratory parameter combination in Figure 17 as well as a linear interpolation between the parameters. When the insertion forces for each grind angle were plotted against the maximum vibratory insertion speed, no correlation was present (R2 values less than 0.19). This implies that the reduction of force due to vibration is not directly related to the relative increase in the speed of the needle.
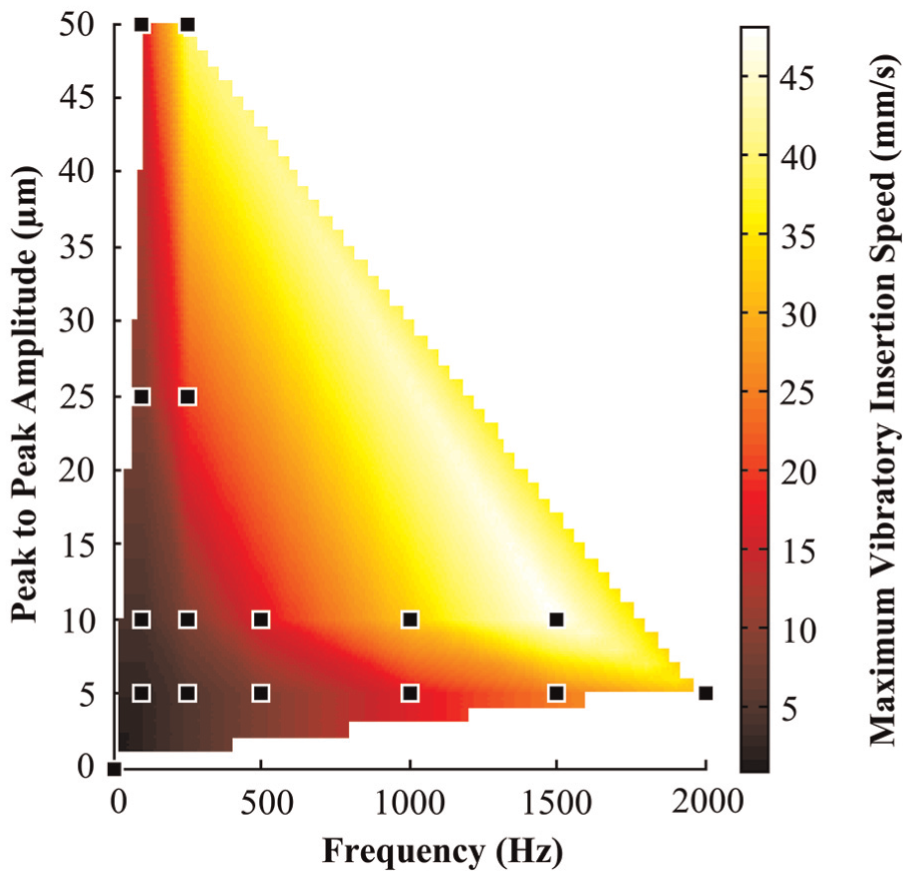
Maximum vibratory insertion speed at vibration parameter combinations.
Phantom tissue results
Different cutting mechanics were observed during the phantom tissue experiments based on the different experimental parameters as summarized in Table 4. A unique four-phase cutting mechanic was found for the 15° needle with and without vibration as shown in Figure 18. In phase I, the phantom tissue deflects without being cut. Phase II is when the needle first punctures the phantom tissue. Phase III is the spreading of the crack to accommodate the increased diameter of the needle as insertion progress. Phase IV is where the needle tip exits the phantom tissue and only friction remains. As shown in Figure 18, the vibration decreases the force needed to extend the crack in the phantom tissue and the friction force between the needle and the phantom. To determine the effect of vibration, the force at the first peak (end of phase I) and the peak force in phase III were recorded and plotted in Figure 19. The vibration decreases the force needed to extend the crack in phase III; however, the puncture force is the same for both no applied vibration and applied vibration. Figures 18 and 19 show a benefit to using vibration, as the ex vivo tissue result suggested.
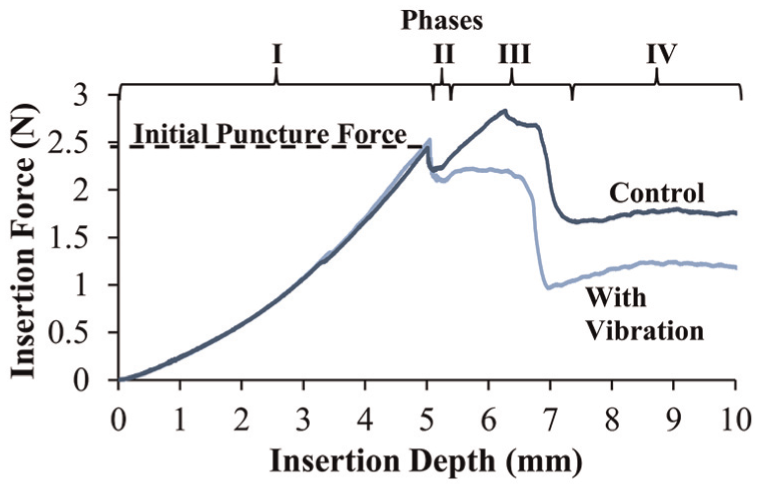
Cutting mechanic of 15° grind angle needle into phantom tissue.
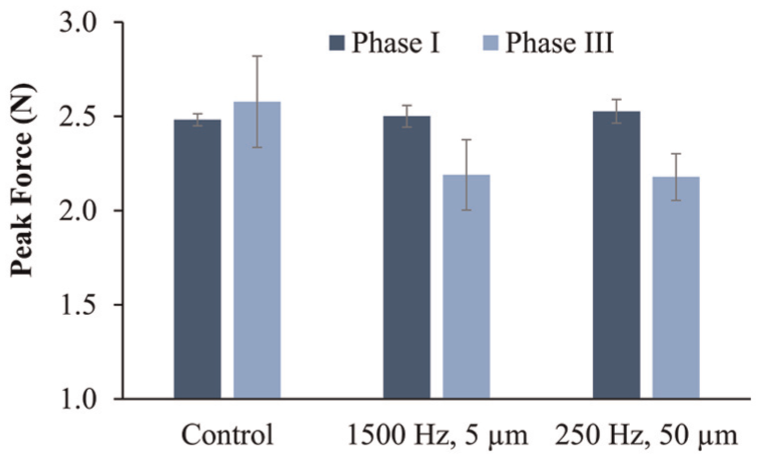
Peak forces for phase I and phase III for 15° grind angle needle with and without applied vibration.
A two-phase cutting mechanic was found for the insertion of the 30° and 45° grind angle needles as shown in Figure 20. Figure 20 shows a 45° grind angle needle with a control insertion and an insertion with vibration combination 2 (250 Hz, 50 µm) as described in Table 3. For the 30° and 45° needles, there is not an initial puncture and an extension of a crack. The entire cutting occurs over a short period of time, as the force sharply drops after the puncture. The sudden release of force when the polyurethane is fractured creates vibrations in the experimental setup which causes oscillations in the force after the initial puncture force. The results of the 30° and 45° grind angle needles for the control and two vibratory combinations show no change in the initial puncture force across the three vibratory parameters.
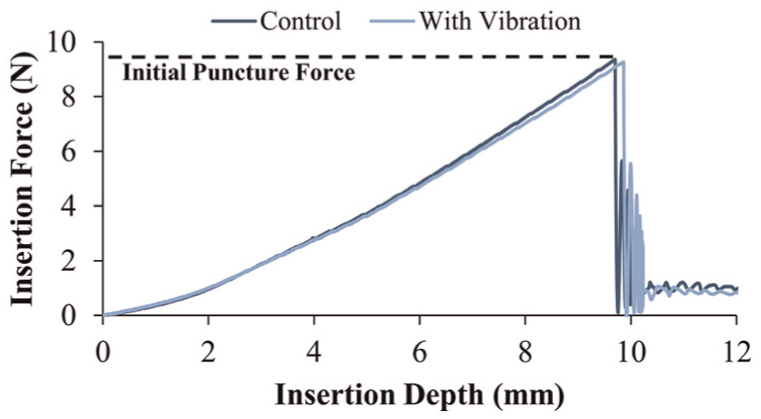
Cutting mechanic of 45° grind angle needle into phantom tissue.
The bluntest needles that have 60° and 75° grind angles were unable to puncture the synthetic material. In these experiments, the needle begins to bend around 25 N, forcing the test to be stopped. This occurred for both with and without vibration. This exceptionally high force is a result of the needle tip geometry being unable to initiate a crack in the material.
The phantom results using conical needles show that the force needed to initiate puncture was the same for a given needle regardless of whether there is applied vibration or not. This is occurring because the phantom tissue is being stretched and absorbs the small amplitudes of the needles motion. In the sharpest needle (15° grind angle) after the initial puncture of the phantom tissue, the vibration reduced the friction between the needle and the phantom and lowered the force needed to extend the crack (phase III). The duller needles tested created so much force before puncture that the needle broke through the phantom in an extremely short time period. This high force and short cutting phase caused the vibration to not have a noticeable effect after fracture.
Conclusion
It was concluded that sharp needle cutting geometry is critical for vibrational cutting to be most effective at minimizing the cutting force. Vibration did not reduce the needle insertion force in blunt needles as much as with sharper needles. The average percent reduction in insertion force from the control was 55%, 54%, 30%, 17%, and 10% for the needles with a grind angle of 15°, 30°, 45°, 60°, and 75°, respectively. This diminishing benefit of vibration for duller needles was also shown in phantom experiments, where the vibration reduced the maximum cutting force of the sharper 15° grind angle needle but did not affect the cutting force of the duller needles.
It was concluded that vibration creates different cutting mechanics in different materials with different needle geometries. The 15° grind angle needle vibrating in bovine liver allowed for continuous cutting without any noticeable tissue deflection. The other needles tested in bovine liver with vibration simply had a two-phase (deflection and cutting) cutting mechanic. The vibration applied to the 15° grind angle needle cutting through polyurethane created a four-phase cutting mechanic. In these four phases, the vibration only helped to reduce the friction and the force needed to extend the crack. For a given needle, the force to initiate the crack was the same in all the polyurethane experiments.
Having a greater understanding of how vibration and geometry together help to reduce cutting force can lead to improved needle geometry designs that work with vibration to reduce tissue cutting force. Lower cutting force needles can allow for greater placement accuracy that can greatly benefit the efficacy of numerous needle-based procedures.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science Foundation under Grant No. CMMI-1404916.