
Abstract
Active Labour Market Programmes (ALMPs), which form important components of employment support policies around the world, have been found to improve mental health and wellbeing of participants. However, it remains unclear how these health effects compare with the effects of different types of employment for men and women. Using 1991–2019 panel data in the UK, we find that unemployed women derive similar mental health benefits from ALMPs compared with employment. Unemployed men also benefit from ALMPs but obtain significantly more health benefits from formal employment. Such benefits are particularly pronounced in full-time, permanent and upper/middle-status jobs. Further analyses reveal that programmes that deliver human capital training have larger mental health benefits than employment assistance ALMPs. These findings provide a more nuanced understanding of the mental health impacts of ALMPs compared with different types of employment, and highlight the need for a more gender-sensitive design in labour market interventions.
Introduction
The impact of unemployment on individual mental health and wellbeing has received extensive academic and policy attention. It is well established that in contemporary Western societies paid work plays a fundamental role in individual identity, mental health and wellbeing by providing material and psychosocial benefits such as income, time structure, enforced activity, social contact, collective purpose and status (Fryer, 1986; Jahoda, 1982; Wood and Burchell, 2018). It has been shown that unemployed people who are deprived of these psychosocial benefits are more likely to experience mental illness, anxiety and lower levels of happiness and life satisfaction (Coutts et al., 2014; Kamerāde et al., 2019). Given the potential adverse health impact of unemployment, policy interventions to improve mental health and help the unemployed return to work are high on the political agenda of many countries.
One of the most important approaches used to address unemployment are Active Labour Market Programmes (ALMPs), which are delivered in the form of various types of employability provision and welfare-to-work policies. Although ALMPs have been commonly adopted in Scandinavian countries, they have gained popularity in the UK since the New Deal, a large-scale workfare programme introduced by the New Labour government in 1998. Under workfare and the move toward activation, job seekers became increasingly compelled to undertake work or ALMPs in order to receive state benefits. The New Deal became the dominant labour market policy for tackling unemployment from 1998 to 2010, introducing various ALMPs which targeted diverse population groups such as youth and lone parents. The New Deal was replaced in 2010 by the Work Programme under the Coalition government and later the Conservative party (Orton and Green, 2019). Compared with ALMPs in continental Europe and Scandinavian countries, which tend to include more human capital development aspects, ALMPs in the UK have tended to focus more on providing job search skills and career counselling. However, in recent years, there has been a convergence in ALMPs in different countries, with the overall aim to improve participants’ employability by providing a wide range of services such as job search assistance, human capital training and wage and employment subsidies (Coutts et al., 2014).
Whereas the economic evidence on the effectiveness of ALMPs is mixed in terms of generating employment outcomes (Card et al., 2018; Coutts et al., 2014), such programmes have been found to mitigate the health-damaging effects of unemployment in the United States and Europe (Ayala and Rodríguez, 2013; Sage, 2015b; Stuckler et al., 2009; Wulfgramm, 2014). The underpinning framework proposed by Coutts (2005, 2009), suggests that ALMPs can imitate some of the psychosocial attributes or non-pecuniary aspects of the employment experience, particularly time structure, meaningful activities (e.g. learning job search skills), social contact with fellow participants and social support provided by the work coaches, that are widely reported to be missing during spells of unemployment (Coutts, 2005, 2009). These psychosocial features are regarded as active elements embedded in the operation of ALMPs that could produce a more salutogenic or health-beneficial psychosocial environment compared to open unemployment, and therefore mediate the negative health effects of unemployment (Coutts, 2009).
However, there are several important gaps in understanding the mental health impacts of ALMPs. Firstly, Coutts (2009) argues that in ALMPs people are neither unemployed nor employed, but occupy an intermediate stage in terms of labour market status with access to some psychosocial benefits of regular employment. However, to what extent ALMPs can emulate the psychosocial experience of regular employment and provide mental health benefits remains largely theoretical and unclear given the limited evidence. This is further complicated by the fact that the effects of employment on mental health are not always positive, varying significantly with job quality. Thus, the first objective of this study is to compare the effects of ALMPs on individuals’ mental health with the effects of paid working, with various job qualities defined by working time, occupational status and precariousness. We also conduct additional analyses to consider diverse types of ALMPs, which may have different effects on participants’ mental health. Secondly, the existing evidence on ALMPs and health assumes that the extent to which people in ALMPs can access the same health benefits of employment is homogeneous across population groups. However, given the widely reported gender differences in cultural norms, work centrality and labour market experiences (Hochschild, 1989), the degree to which ALMPs simulate the employment experience in terms of providing mental health benefits may also vary with gender. Thus, the second objective is to explore whether the health effects of ALMPs relative to paid work vary by gender.
By achieving both objectives, this article provides important insights into the mental health benefits of ALMPs and how they compare to various types of employment with different job quality characteristics. Given the predicted rapid rise in global unemployment due to Covid-19 and high levels of precarious employment, this article suggests that the design of ALMPs should not just focus on short-term employment outcomes, but must pay attention to the health and wellbeing benefits of participation and the long-term effects on participants’ employment and job quality. Moreover, by analysing gender differences, this article provides a more nuanced understanding of the differential effects of labour market policies on mental health, highlighting the need for policy-makers to adopt a more gender-specific approach when designing policies for the unemployed.
Background literature
Employment, unemployment and mental health
Employment plays a pivotal role in individual identity formation, mental health and wellbeing (Wood and Burchell, 2018). Jahoda’s (1982) Latent Deprivation Theory is the first systematic explanation about the importance of employment in people’s mental health. Jahoda argued that paid employment, acting as a dominant social institution in contemporary societies, is more than a source of income (the manifest function) – it also provides a number of latent functions (i.e. time structure, enforced activity, social contact, collective purpose, social status and identity) to fulfil people’s psychosocial needs. Fryer (1986) further develops this theory with the Agency Restriction Theory, which argues that in addition to the withdrawal of psychosocial benefits, the loss of income and the consequent financial strain and lack of ability to control one’s life during spells of unemployment also lead to a deterioration of mental health (Fryer, 1986). A large number of studies demonstrate that unemployed people who are deprived of these psychosocial and material benefits from employment have an increased risk of a range of mental health problems (e.g. depression and anxiety), and on average have lower levels of wellbeing, self-efficacy and higher levels of social isolation than employed people (Kamerāde et al., 2019; Wood and Burchell, 2018).
ALMPs and mental health: A theory of change
Given the negative impacts of unemployment on a wide range of mental health and wellbeing outcomes, ALMPs that are found to mitigate the damaging effects of unemployment have received much scholarly and policy attention. Coutts (2005, 2009) proposes that the impacts of ALMPs on mental health can be understood by bringing together Jahoda’s (1982) latent and manifest benefits of employment and various sociological and psychological approaches concerning the salutogenic effects of self-efficacy (Bandura, 1986), social support (Berkman and Syme, 1979) and social networks (Cacioppo et al., 2011). Coutts (2005, 2009) has demonstrated how ALMP participants are neither employed nor unemployed but occupy a state of ‘labour market limbo’ and could have access to some active elements within the interventions that cause changes in their mental health, wellbeing and behaviour.
It is suggested that the psychosocial environment unintentionally created by ALMPs can emulate many attributes of employment and generate positive mental health impacts through at least three types of active elements embedded in the interventions: (1) social contact and social support from course leader and fellow participants; (2) time structure and routine of employment; (3) human capital training and employment assistance. Firstly, existing evidence from sociology and social epidemiology demonstrates that the unemployed are more likely to report feelings of loneliness and social isolation linked to a range of negative mental health problems (Berkman and Syme, 1979; Cacioppo et al., 2011; Coutts, 2009). Participation within an ALMP can help to offset these feelings as the intervention involves interacting within a group environment, providing participants with social support and social contact, thereby reducing feelings of social isolation (Coutts et al., 2014; Sage, 2015a). Secondly, as previous research shows that unemployed people are deprived of time structure and enforced activity, conditions associated with poor mental health, ALMPs requiring participants to attend the course at certain times per day or per week could provide a constructive daily routine rather than a monotonous one they experienced while being out of work (Card et al., 2018; Jahoda, 1982; Sage, 2015b). Finally, by providing a wide range of employability provision services, such as human capital and vocational training, job search and networking skills, ALMPs could provide participants with skills and knowledge that familiarise them with the current labour market situations and employer demands, enhance their employability, and build their self-esteem and self-efficacy. This may in turn improve their mental health and wellbeing (Bandura, 1986; Coutts et al., 2014). Nevertheless, the ALMP participants who are in ‘labour market limbo’ between unemployment and employment may still not access some benefits of formal employment, such as income and social status (Sage, 2015b).
Overall, these active elements embedded within ALMPs could replicate some psychosocial benefits of employment and facilitate health, wellbeing and behaviour changes among participants. However, another stream of research reveals the compulsory nature of some ALMPs that may undermine participants’ mental health. For example, in order to receive work-related benefits, many ALMP participants are compelled to conduct the required job searches and training activities, which could inhibit the possibility of developing positive relationships with their work coaches (Dwyer et al., 2020).
ALMPs and mental health: Empirical evidence
So far, there is a series of empirical studies which have investigated the impacts of ALMPs on mental health and wellbeing. At the individual level, research using experimental or quasi-experimental methods from the UK (Sage, 2015a, 2015b), Germany (Crost, 2016; Wulfgramm, 2014), Spain (Ayala and Rodríguez, 2013), Serbia (Bonin and Rinne, 2014), the USA (Vinokur et al., 2000) and Finland (Vuori and Vinokur, 2005) lends support to the positive effects of ALMPs and back-to-work interventions on physical and mental health as well as subjective wellbeing. At the national or regional level, a number of studies show that higher levels of government expenditure on ALMPs, as well as other social protection policies, can significantly reduce suicide rates caused by unemployment (Niedzwiedz et al., 2016; Stuckler et al., 2009).
However, only a small number of studies from Germany and the UK provide a limited understanding of how ALMPs may emulate the mental health and wellbeing benefits of paid employment. Wulfgramm (2014) shows that people in formal paid work have significantly higher levels of life satisfaction than those in ALMPs. This suggests that ALMPs for the unemployed could not fully replicate the wellbeing benefits of regular employment in promoting individual life satisfaction. Similarly, Sage (2015b) uses the British Household Panel Survey and the Understanding Society datasets to compare the difference in several health outcomes between people in paid work and ALMPs, and finds significant difference in life satisfaction, but not mental health. Taken together, these studies suggest that although ALMPs could improve participants’ mental health and wellbeing, they are not able to fully emulate the psychosocial attributes of formal employment.
Differences in types of employment
Previous research on ALMPs provides a limited understanding of whether they can have the equivalent mental health effects to formal paid employment. An important limitation of these studies lies in conceptualising employment as a homogeneous category, and ignoring the role of various types of employment status with different job quality characteristics that can have heterogeneous effects on mental health and wellbeing.
In fact, there is rich literature from various social science disciplines that highlights the importance of job quality in workers’ mental health and wellbeing. From the perspective of occupational psychology, Peter Warr’s (1999) ‘vitamin’ model shows how specific job characteristics could influence employees’ mental health and proposes 12 important job characteristics, which are analogous to vitamins (e.g. money, social contact, status, opportunity of skill use and control) (Warr, 1999). Importantly, Warr highlights that the effects of employment on health are not always positive but depend on the availability of and length of exposure to these beneficial job characteristics or ‘vitamins’ in the workplace. For example, when people are deprived of these ‘vitamins’, intake of any of them is beneficial for mental health. However, after an optimum level is reached, further intake of some ‘vitamins’ (e.g. money, physical security and valued social status) has no further effect, whereas for other vitamins further intake may actually undermine health (Warr, 1999).
Consistent with Warr’s vitamin model, substantial research from other social science disciplines highlights a number of important dimensions of job quality for employees’ health and wellbeing, including earnings (orthodox economics), skill use and meaningfulness (sociology), employment prospects and security (institutional economics), physical and social environment (occupational health), as well as work–life balance (management) (Muñoz de Bustillo et al., 2011). In recent years, as jobs become increasingly polarised across these job quality dimensions (Kalleberg, 2011), the extent to which employment could bring mental health benefits essentially depends on whether people work in ‘good’ or ‘bad’ jobs. In particular, research shows that transitions into ‘bad’ jobs characterised by low pay, lack of control over work and high job insecurity could undermine mental health and wellbeing (Butterworth et al., 2012; Chandola and Zhang, 2018). This may be particularly relevant for ALMP participants because of the mandatory nature of some ALMPs, which suggests that participants under the constant pressures of work coaches are compelled to find a job more quickly and are likely to end up transitioning into low quality jobs (Dwyer et al., 2020).
Thus, given the increasing heterogeneity within employment, to what extent ALMPs could replicate the mental health benefits of regular employment may depend on the types of employment embodied with different job quality characteristics. In this study, we focus on working time, occupational status and type of contract, aspects that have been found to influence mental health. Firstly, research on under- and over-employment highlights the effects of working time on health because it determines employees’ length of exposure to various positive or negative job characteristics (Kamerāde et al., 2019). Secondly, occupational status is widely regarded as a combined measure of both materialistic and social influence of a job that defines individuals’ position in the social structure and their different work-related health exposures (Eyles et al., 2019). Finally, the type of contract is used to measure precariousness because research shows that compared with those on temporary contracts, employees with permanent contracts tend to have higher job security and more control over their work, which is associated with better health (Chandola and Zhang, 2018).
Gender differences
Drawing on wider sociological and economic evidence, it can be argued that the effects of ALMPs on mental health may vary with gender due to societal norms surrounding the gendered division of labour, and gender differences in labour market experiences. From the perspective of traditional gender role norms, the male breadwinner hypothesis assumes that women are expected to take the main responsibility for childcare, household duties and care of ageing parents, whereas men are expected to work in the labour market (Hochschild, 1989). The gendered labour division is not only shaped by men and women’s different comparative advantages in the labour market and domestic work (Becker, 1991), and different negotiating power and resources (Lundberg and Pollak, 1996), but may also reflect differing performances of gender identities. While men may display their masculine identity through employment, women are more limited by their relative economic dependence on men and instead perform gender through some forms of domestic servitude (Fensternmaker and West, 2002). The male breadwinner hypothesis also suggests that men gain their social identity and approval from work, whereas women may be more flexible and able to generate social approval and identity from participation in other roles, such as being a mother and wife (Hoherz and Bryan, 2020; McMunn et al., 2020; Wang and Coulter, 2019). Thus, the higher work centrality among men suggests that men may be more likely to obtain mental health benefits from employment than women. However, in recent decades the gradual decline of traditional gender role norms brings into question whether men can obtain more mental health benefits from employment and other labour market statuses, such as ALMPs, than women.
In addition to different cultural values, men and women also have different labour market experiences and statuses, which may determine the extent to which they can obtain mental health benefits from employment and ALMPs. For example, existing evidence from the sociology of work shows that, compared with men, women are more likely to suffer discrimination in terms of pay, promotion and job security, and also more likely to experience sexual harassment in the workplace, situations that are closely linked to poor mental health (Hoherz and Bryan, 2020; McMunn et al., 2020; Wang, 2019). Moreover, compared with male workers, women working in full-time jobs are more likely to encounter work–life conflicts, and demands of multiple conflicting roles could undermine their mental health and wellbeing (Scott et al., 2010). Taken together, women’s negative labour market experiences may offset the mental health benefits they derive from employment, suggesting that women’s mental health may benefit less from employment than men’s.
Research questions and hypotheses
In order to address these evidence gaps, we propose two research questions:
1. How do the effects of ALMPs on mental health compare to various types of employment with different job quality characteristics defined by working time, occupational status and precariousness?
We hypothesise that people working in full-time, upper/middle-status jobs with permanent contracts could obtain more mental health benefits from employment compared to ALMPs, whereas people working in part-time, low-status and temporary jobs do not obtain more mental health benefits from employment than from ALMPs. This is because people working in high quality jobs have more exposure to various positive psychosocial benefits of employment than those in low quality jobs and ALMPs. We also conduct additional analyses to consider diverse types of ALMPs, which may have different effects on participants’ mental health.
2. To what extent do the effects of employment on mental health compared with ALMPs differ between genders?
Owing to men’s higher work centrality and women’s negative labour market experiences (e.g. gender discrimination and sexual harassment), we hypothesise that the mental health benefits of employment, especially in high quality jobs, over ALMPs are more pronounced for men than for women.
Method
Data and sample
The data used in this study are from 18 waves (1991–2009) of the British Household Panel Study (BHPS) and nine waves (2009–2019) of its successor Understanding Society: United Kingdom Household Longitudinal Study (UKHLS). In its first wave, in 1991, the BHPS conducted a nationally representative survey of over 10,000 individuals from 5500 British households using a stratified and clustered sampling design, interviewing the same households in each subsequent year. In 2009, the BHPS had 18 consecutive waves and was replaced by UKHLS, which sampled over 50,000 individuals from 30,000 households in its first wave and by 2019 had nine completed waves. This study has combined data from both BHPS and UKHLS to create long-term panel data including 27 waves from 1991 to 2019. After excluding full-time students and retired individuals due to their loose attachment to the labour market, the final analytical sample was 380,748 person-wave observations from 70,593 respondents. The UKHLS longitudinal weights were used to adjust for the complex survey design, non-response and attrition rates.
Measurements
The dependent variable is the 12-item General Health Questionnaire (GHQ), which is a widely used reliable mental health measurement (Golderberg and Williams, 1988). The questionnaire asked respondents 12 questions about their mental health and wellbeing on a four-point scale ranging from 0 (better than usual) to 3 (much less than usual) (Golderberg and Williams, 1988). Following previous research, the answers to GHQ-12 questions were reversed and summated to construct a metrical scale ranging from 0 (worst mental health) to 36 (best mental health) (Kamerāde et al., 2019).
The key independent variable was labour market status. We first distinguished four main categories of labour market status: employed, unemployed, inactive and those reporting on a government training scheme. Most previous research has used government training schemes to measure ALMPs because ALMPs are defined as a series of government programmes and social expenditure that aim to improve overall employment rates in a society (Sage, 2015a, 2015b; Wulfgramm, 2014). We followed this method used in previous research, although it is important to note that both concepts are not identical and the government training schemes may contain some other programmes not related to employment. We further analysed Annual Population Surveys with more detailed measures of various types of ALMPs (see Further Analysis 4, pp. 14–15). Reassuringly, the results are consistent with our main analyses but provide more nuanced insights into how different types of ALMPs affect respondents’ mental health.
Given the heterogeneity of employment, we compared ALMPs with various types of employment and different job quality characteristics defined by working time, occupational status and type of contract. In terms of working time, we divided the employed people into full-time (35 hours per week or more) and part-time (less than 35 hours per week) employees. Occupational status is defined by the National Statistics Socio-economic Classification (NS-SEC) including three categories: high occupational status (managerial and professional jobs), middle occupational status (intermediate occupations such as clerical, sales, service, and small employers and own account workers), low occupational status (semi-routine and routine jobs). The type of contract was used to measure the precariousness of a job, consisting of permanent and temporary employment contracts.
Several individual and household characteristics that influence employment status, working hours and mental wellbeing were controlled for. They included age (grand mean centred), age squared to capture the potential curvilinear relationship, marital status, presence of children, longstanding illness and household income. Overall, ALMP participants were younger and more likely to be single than any other groups. Also, people who were employed and participated in ALMPs had lower levels of mental distress and higher household income than those who were unemployed and inactive (for more details, see Table A1 in the online supplementary material).
Analytic approach
This study used fixed effects (FE) regression models, which have at least two important advantages over cross-sectional analysis. Firstly, by using only ‘within-individual’ variation (i.e. how changes in labour market status are linked to changes in mental health within each individual over time), FE regression eliminated the unobserved heterogeneity, confounding effects from all time-constant variables, and enabled a more accurate estimate of the causal relationship between work and mental health (Allison, 2009). Secondly, FE models could help understand the dynamic effects of ALMPs on mental health by using lagged independent variables in panel data (Allison, 2009). Given the widely acknowledged difference between men and women’s work orientations, employment trajectories and experiences, FE models were fitted separately by gender, controlling for other socio-demographic characteristics.
Results
Fixed effects models
Table 1 reports a series of fixed effects models to predict effects of ALMPs and types of employment on mental health for men and women. Overall, in all models we found that people who became unemployed and economically inactive had significantly worse mental health compared with those who participated in ALMPs. This pattern remained similar across genders. Comparing ALMP participation with various types of employment, Model 1 shows that, for men, employment in full-time jobs with either permanent or temporary contracts and part-time jobs with permanent contracts was associated with significantly better mental health than ALMP participation, whereas employment in part-time jobs with temporary contracts was not significantly different from ALMP participation in terms of mental health. However, for women (Model 2), ALMP participation was not significantly different from paid employment regardless of working hours and type of contract. Figure 1 predicted mental health scores calculated using estimates from Models 1 and 2 in Table 1 and enabled a visual comparison between genders. Overall, economically inactive and unemployed men and women had the lowest levels of mental health, which was significantly improved when they participated in ALMPs. However, once they became employed, regardless of working hours and type of contract, the level of mental health further increased for men (non-significant in part-time jobs with a temporary contract), but remained similar for women.
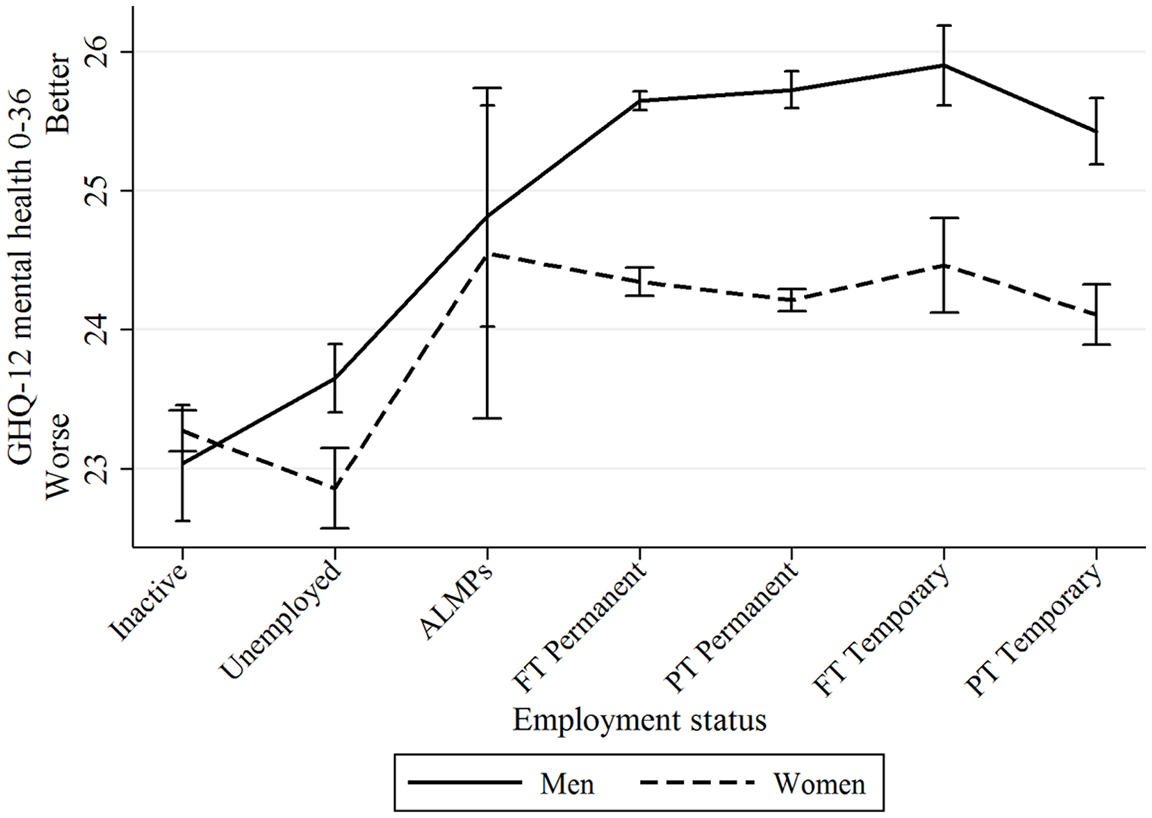
Differences in mental health between ALMPs and employment types differentiated by contract and working hours with 95% confidence intervals.
Two-way fixed effects models predicting effects of ALMPs and types of employment on GHQ-12 mental health for men and women (BHPS/UKHLS 1991–2019).
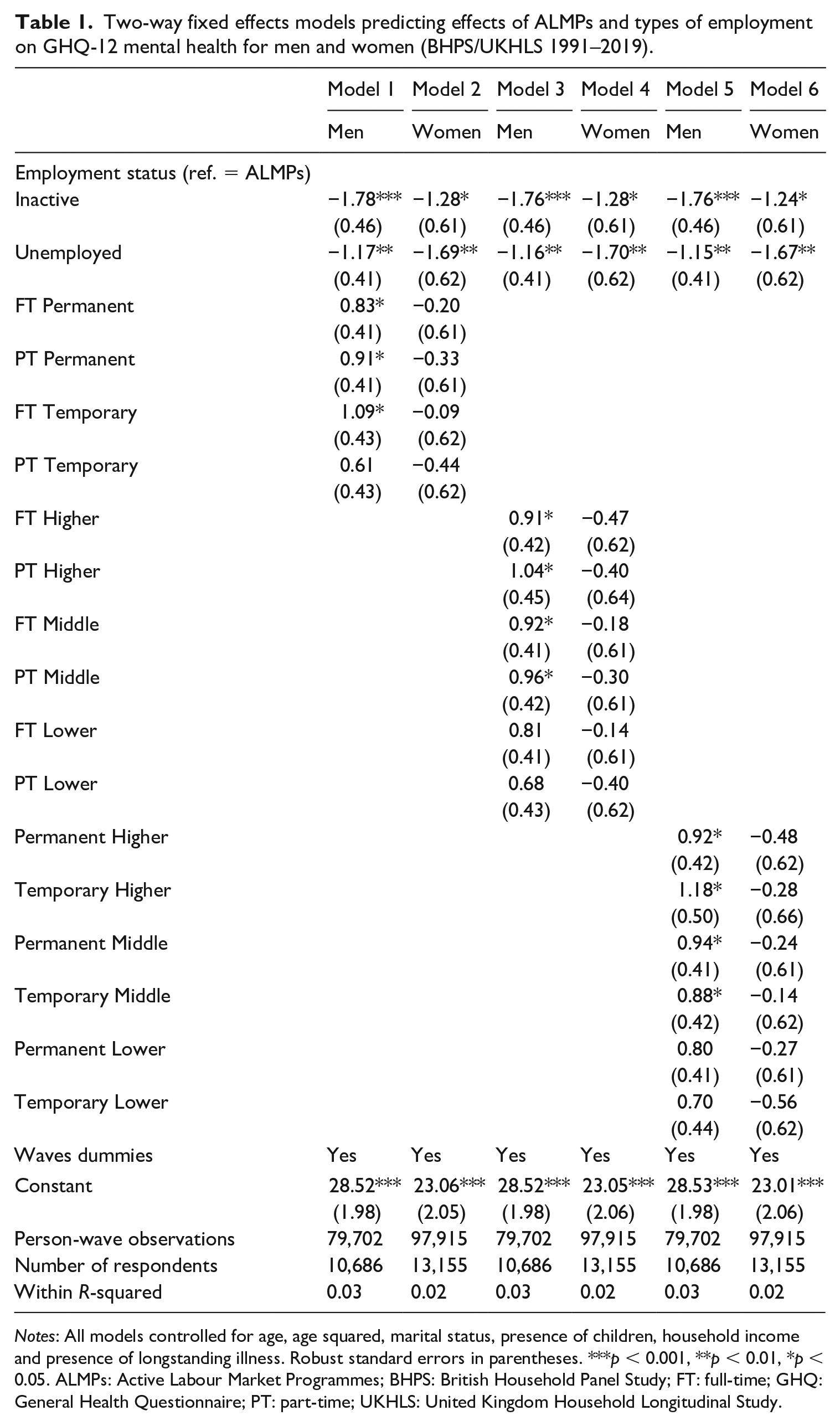
Notes: All models controlled for age, age squared, marital status, presence of children, household income and presence of longstanding illness. Robust standard errors in parentheses. ***p < 0.001, **p < 0.01, *p < 0.05. ALMPs: Active Labour Market Programmes; BHPS: British Household Panel Study; FT: full-time; GHQ: General Health Questionnaire; PT: part-time; UKHLS: United Kingdom Household Longitudinal Study.
Next, Models 3 and 4 in Table 1 compared ALMP participation with types of employment, differentiated by working hours and occupational status. Similarly, we found that for men, employment in either full-time or part-time higher and middle-status jobs led to significantly better mental health compared with ALMP participation, whereas employment in either full-time or part-time low-status jobs was not significantly different from ALMP participation. Again, for women, ALMP participation was not significantly different from any types of employment in terms of mental health. These patterns were well demonstrated in Figure 2, which shows that compared with ALMP participation, paid employment could greatly improve mental health for men (albeit non-significant in full-time or part-time lower class jobs), but could not further improve mental health for women.
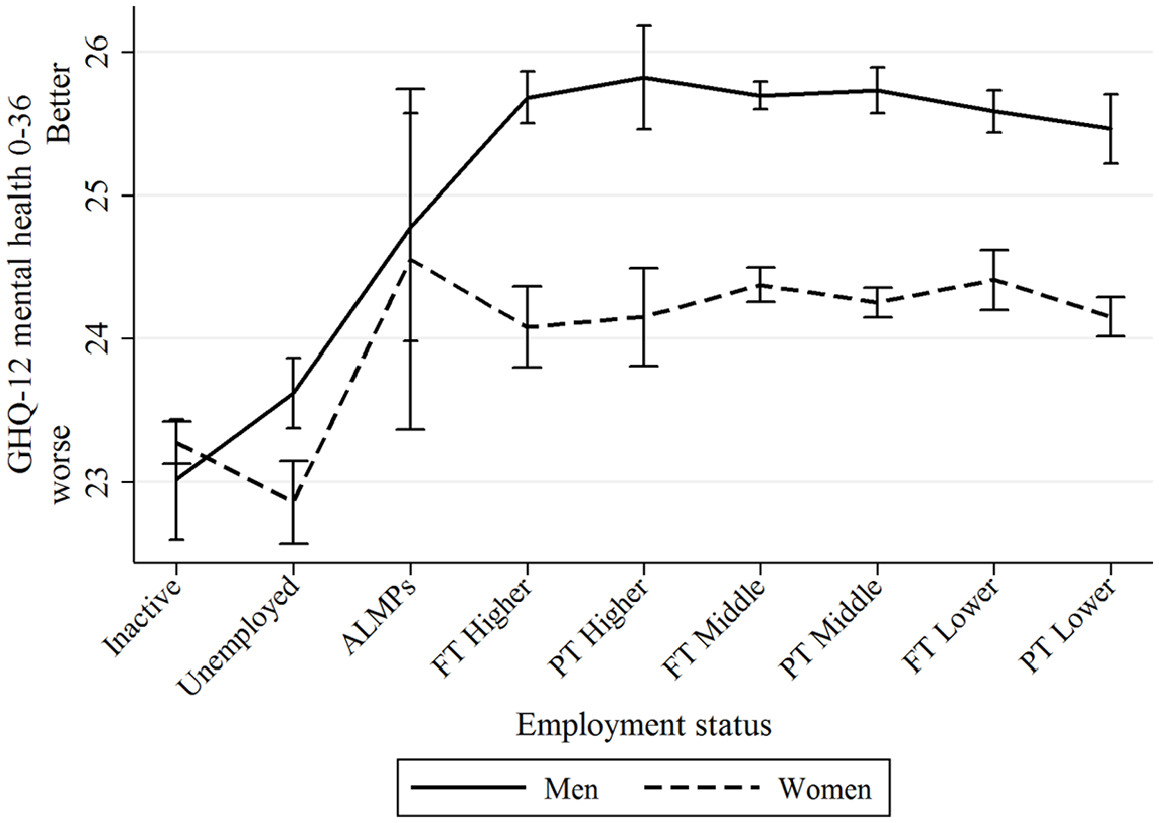
Differences in mental health between ALMPs and employment types differentiated by occupational status and working hours with 95% confidence intervals.
Finally, Models 5 and 6 in Table 1 compared ALMP participation with types of employment differentiated by type of contract and occupational status. Consistent with previous findings, we found that for men, employment in higher and middle-status jobs with either permanent or temporary contracts led to significantly better mental health compared with ALMP participation, whereas employment in low-status jobs with permanent or temporary contracts was not significantly different from ALMP participation. Again, for women, ALMP participation was not significantly different from any types of employment in terms of mental health. The patterns were consistent with Figure 3, which shows that compared with ALMP participation, paid employment could greatly improve mental health for men (albeit non-significant in permanent or temporary low-status jobs), but not for women.
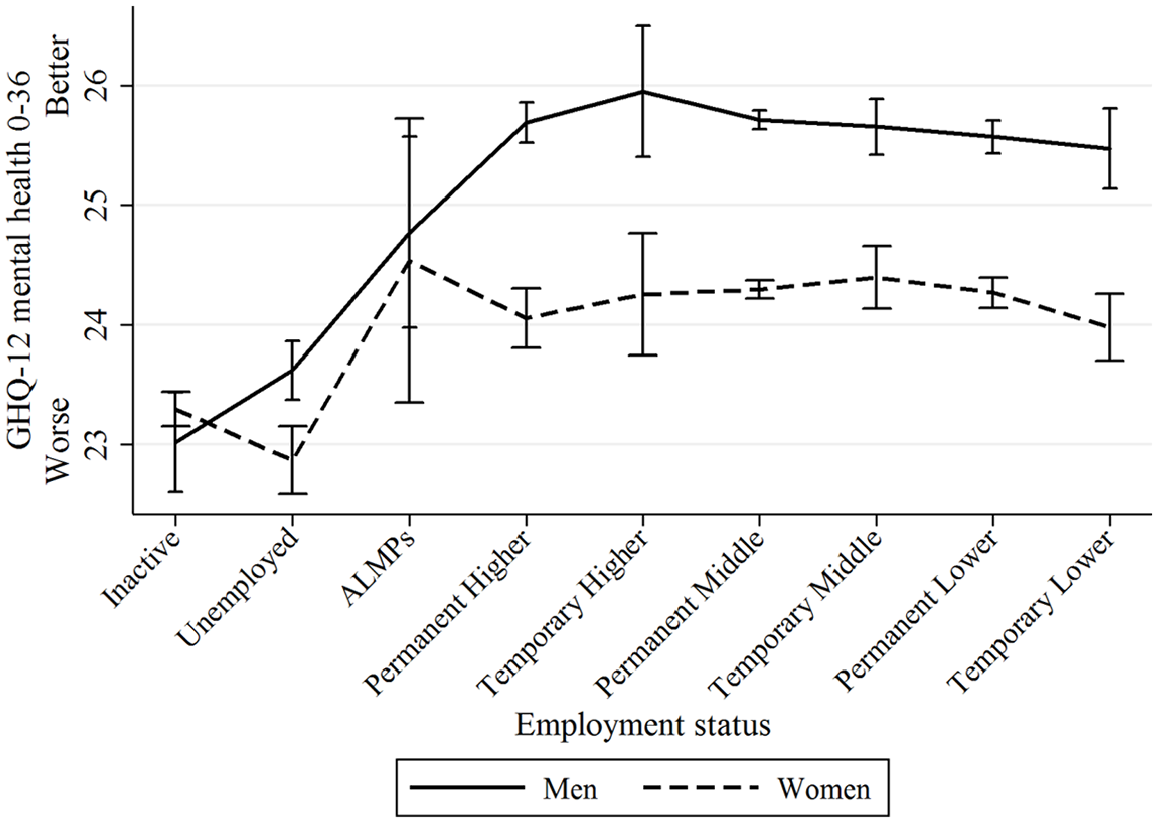
Differences in mental health between ALMPs and employment types differentiated by occupational status and contract with 95% confidence intervals.
Taken together, we found that, for both genders, ALMPs led to significantly better mental health than unemployment and economic inactivity. For men, once in paid employment they could further obtain significantly more mental health benefits from formal work than from ALMPs, but in precarious and low-status jobs they could only obtain similar mental health benefits as through ALMPs. In contrast, for women, ALMP participation was not significantly different from any types of paid employment in terms of mental health. Additional analyses suggest that the gender differences were significant especially among permanent and high-status jobs.
Further analyses
We conducted four additional analyses to extend our results in the main analysis as well as check their robustness. The details of these analyses, including five tables (Tables A2–A6), can be found in the online supplementary material.
1. Lagged effects of ALMPs and types of employment on mental health
Firstly, we analysed whether the mental health benefits of ALMPs and employment (mainly in high quality jobs for men) could last for more than one year by examining whether lagged ALMPs and various types of employment (at time point t–1) could still influence respondents’ mental health (at time point t) in Table A2. However, we found that after using lagged independent variables, the mental health benefits of ALMPs (relative to unemployment/inactivity) and employment (relative to ALMPs, mainly for men) disappeared. In other words, the positive effects on mental health could not last for more than one year.
2. Using GHQ-12 mental health constructed by factor analysis
In the main analysis, GHQ-12 mental health was constructed by summating the reversed answers of the 12 items. This approach assumes that each component item has an equal weight to the summated GHQ-12 score. We conducted principal component factor analysis (based on polychoric correlation) to explore the structure of GHQ-12. After the analysis in Table A3, we obtained one factor score from the 12 items (eigenvalue = 6.37, variance explained % = 89.58, alpha = 0.89), which was standardised to range from 0 to 10, with a higher score indicating better mental health. In Table A4, we found that by using factor score GHQ-12 as the dependent variable we generally replicated the results in Table 1. This suggests that our main findings are robust to alternative variable specification.
3. Effects of ALMPs before and after the New Deal
Because the social expenditure on labour market programmes greatly increased after the New Deal 1998, the effects of ALMPs on mental health might have also changed over time. We fitted several interaction terms to examine whether the effects of ALMPs on mental health changed before and after the New Deal in Table A5. Overall, none of the interaction terms were significant, suggesting that the mental health effects of ALMPs remained similar before and after the New Deal. However, the results should be interpreted with caution due to the small sample size of ALMP participants.
4. Effects of different types of ALMPs
Because BHPS/UKHLS did not distinguish between different types of ALMPs, we used pooled 2012–2018 Annual Population Survey (APS) data to explore how participation in different types of ALMPs affects participants’ mental health. The APS is a large-scale annual cross-sectional survey, which combines data from quarterly annual waves of the Labour Force Survey in the UK and consists of around 150,000 households and 300,000 individual respondents. This analysis used data from wave 2012 to wave 2018 because these waves contain consistent measures of mental health and ALMP participation.
Owing to data limitations, there are several differences in the selection of variables between the main analysis and the further analysis. Firstly, mental health (the dependent variable) was measured by three questions asking respondents about the extent to which they were happy, satisfied with their lives and thought their lives were worthwhile on a scale ranging from 0 to 10. Given the three items had high internal consistency (alpha = 0.80), a summated score of these items (0–30) was calculated, with a higher score indicating better mental health. Secondly, following previous research in the UK (Sage, 2015a), we identified three types of ALMPs: human capital ALMPs (providing education and vocational training to improve the human capital of jobless people, including Work Experience, Work Trial, Training for Success, Training for Work, Get Ready for Work, 18.8%), employment assistance ALMPs (providing job subsidies, job search skills and counselling including Work Club or Enterprise Club, New Enterprise Allowance, Work Programme, Steps to Work/Steps 2 Success, 44.9%) and other ALMPs (types unspecified, 36.3%). Thirdly, our control variables included age, age squared, marital status, ethnicity and education levels, which were slightly different from the main analysis.
Ordinary least squares (OLS) regression models in Table A6 show that, for both men and women, those who participated in human capital ALMPs had significantly better mental health than unemployed or inactive individuals. Moreover, compared with those in human capital ALMPs, those who participated in employment assistance ALMPs had significantly worse mental health for both genders, although the difference is more pronounced for women than for men. Finally, comparing ALMPs with different types of employment, we find that, for both genders, paid employment of any type was associated with significantly better mental health than in ALMP participation, and the effects were more pronounced in full-time, upper/middle-status and permanent jobs, and for men. However, it should be noted that the significant effects of ALMPs and paid employment were likely to be over-estimated because OLS regression models often suffer omitted variable bias. Although the results from UKHLS and APS were not directly comparable due to different research design, the results based on APS are consistent with our main findings and provide more nuanced insights into understanding the health effects of various types of ALMPs.
Discussion and conclusions
In recent years, the effects of ALMPs on participants’ mental health have received much scholarly and policy attention. Although ALMPs are thought to mitigate the health-damaging effects of unemployment by providing participants with psychosocial attributes of the employment experience (Coutts et al., 2014), little is known about the extent to which ALMPs can replicate different types of paid employment in terms of psychosocial attributes for men and women.
This research has three key findings. Firstly, we find that the extent to which ALMPs emulate the mental health benefits of employment varies significantly by gender. For men, participation in the ALMPs does not appear to provide them with mental health benefits equivalent to those they gain from employment, especially in high quality jobs. This is possibly because ALMPs are regarded as a temporary and transitional process before they find formal paid employment. However, women appear to be more responsive in terms of mental health and wellbeing, given that participation in ALMPs was found to have similar health benefits to regular employment regardless of job quality. This is consistent with Coutts’ suggestion that ALMPs can emulate the psychosocial experience of regular employment via their active elements, such as social contact and support, time structure and routine, human capital training and employment assistance, which could in turn improve participants’ self-efficacy and generate the associated mental health and wellbeing benefits (Coutts et al., 2014).
The observed gender health difference may be explained by the male breadwinner hypothesis in that paid work appears to have larger impacts on men’s social status, identity and mental health compared to women (Hochschild, 1989). Alternatively, this could also be due to women’s negative labour market experiences (e.g. discrimination, harassment or work–life conflicts) that may offset mental health benefits from employment (Scott et al., 2010), or due to gender differences in more nuanced types of ALMP participation. These explanations help us understand why women benefit equally from participation in ALMPs and employment, whereas for men these benefits are derived from engaging in formal employment rather than the quasi-transitional status embodied in ALMPs. In policy terms, providers of employability interventions should be aware of the differential responsiveness in terms of health and wellbeing benefits between male and female participants, highlighting the need of a more gender-sensitive policy design. However, this does not mean that ALMPs should entirely focus on women as ALMPs may act as interventions which help men into work and brings about subsequent health improvements.
Secondly, while men may obtain more mental health benefits from formal employment than participation in ALMPs, such benefits were more pronounced when they worked in full-time, permanent, high-status jobs, and these effects did not last more than a year. This result suggests that, for men, ALMPs can only provide a limited number of health and wellbeing benefits within a short period of time and are far from being as salutogenic as when they are fully employed in high quality jobs. Previous research comparing the health and wellbeing effects of ALMPs with employment may have overlooked important nuances and details within the employed samples (Sage, 2015b; Wulfgramm, 2014). Given that the aim of ALMPs is to provide a temporary and supportive transition to employment, many distinct benefits that can be derived from high-status jobs, such as income and social status, cannot be readily imitated by ALMPs. The recent Marmot Review 2020 recommended that ‘good quality’ ALMPs can be used to help protect the health of the unemployed and return people to work (Marmot et al., 2020). However, it is unclear from the existing evidence as to what constitutes a good quality ALMP. Our results offer further insights into how good quality ALMPs can be designed. Given the rapid increase in Covid-19-related job loss and the rise of precarious employment, it suggests that more policy attention should be focused on the post-ALMP experiences and whether there are good quality jobs that participants can take up because our results show that high quality jobs are likely to benefit mental health and wellbeing.
Thirdly, we find that different types of ALMPs and employability provision have heterogeneous effects on participants’ mental health and wellbeing. ALMPs focusing on human capital, education and skills development were found to have greater mental health and wellbeing benefits than the traditional employment assistance ALMPs, which focus on job search skills and employment subsidies. This could be explained by the fact that the education and vocational training involved in human capital ALMPs are better able, following Jahoda (1982), to satisfy participants’ latent psychosocial needs, such as identity, activity, bolstering social support and social networks, which improves individuals’ self-efficacy, motivation and confidence in finding a job. In contrast, ALMPs and employability provision that offer the more basic job search skills are less able to replicate the psychosocial experience of employment and associated latent benefits. This finding lends further insights into the framework proposed by Coutts (2009) in terms of the diverse effects of ALMPs on mental health and wellbeing and the nature of the active elements and mechanisms embodied in ALMPs which help to generate changes in mental health, wellbeing and behaviour.
There are a number of limitations with our study, which can guide the focus of future research. Firstly, although we have used longitudinal data and fixed effects models, readers should be cautious in interpreting our results as causal relationships due to potentially omitted time varying variables such as changing labour market situations. Secondly, although we have identified a number of active elements within ALMPs that could improve participants’ mental health, it is unclear how these active elements work jointly to change participants’ behaviour and which one is the most important. This requires future research using qualitative methods (e.g. ethnography and participant observation) to understand the intervention processes and active elements used in ALMPs, why they work and how. Thirdly, we have proposed that gender differences in the health effects of ALMPs and employment could be explained by the male breadwinner hypothesis and women’s negative labour market experiences. However, due to data limitations, we have not tested either explanation, and there may be other reasons that may explain the gender differences. Future research using more comprehensive data could profitably explore why there is a gender difference in the mental health benefits from the transition between ALMPs and employment.
Despite these limitations, this study suggests that the design of ALMPs and employability provision should not just focus on short-term employment outcomes as indicators of effectiveness, but need to pay attention to the health and wellbeing benefits of participation and the long-term effects on participants’ employment and job quality. As Coutts (2009) suggests, improvements in mental health and wellbeing may help to enhance the employability of participants and move them closer to labour market entry. Currently, in the UK, there are policy efforts to focus on the ‘distance travelled’ (i.e. progress achieved) by ALMP participants in terms of employment outcomes. The inclusion of mental health and wellbeing as outcomes provides potential indicators for measuring ‘distance travelled’. Given the upcoming economic recession and high unemployment rates due to Covid-19, ALMPs will become even more crucial to policy. Our study offers important insights into policy understanding of the impacts of ALMPs and how they can be designed to help reduce the mental health burden of unemployment.
Supplemental Material
Online_supplementary_material_20200629 – Supplemental material for Can Active Labour Market Programmes Emulate the Mental Health Benefits of Regular Paid Employment? Longitudinal Evidence from the United Kingdom
Supplemental material, Online_supplementary_material_20200629 for Can Active Labour Market Programmes Emulate the Mental Health Benefits of Regular Paid Employment? Longitudinal Evidence from the United Kingdom by Senhu Wang, Adam Coutts, Brendan Burchell, Daiga Kamerāde and Ursula Balderson in Work, Employment and Society
Footnotes
Acknowledgements
This study was part of the project ‘The Employment Dosage: How Much Work is Needed for Health and Wellbeing?’ at the Centre for Business Research, University of Cambridge. We would like to thank the editor and three anonymous reviewers for their highly constructive comments. We also would like to thank Niamh Bridson Hubbard for her careful proofreading. Understanding Society and BHPS are funded by the Economic and Social Research Council and various government departments, with scientific leadership by the Institute for Social and Economic Research, University of Essex, and survey delivery by NatCen Social Research and Kantar Public. The research data are distributed by the UK Data Service.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research grant from the Cambridge Political Economy Society Trust. Dr Adam Coutts is funded by the Health Foundation’s Health and Care Sustainability programme (Grant ID: 1273834). The Health Foundation is an independent charity committed to bringing about better health and health care for people in the UK. Dr Senhu Wang received funding from the Major Project of the National Social Science Fund of China (No. 19ZDA149) at Nanjing University, China.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.