
Abstract
Little is known outside of the United States about the risk of violence-related death among young people who have had contact with the youth justice system (justice-involved young people). We examined violence-related deaths among justice-involved young people in Queensland, Australia. In this study, youth justice records for 48,647 young people (10–18 years at baseline) who were charged, or experienced a community-based order or youth detention in Queensland, Australia (1993–2014) were probabilistically linked with death, coroner, and adult correctional records (1993–2016). We calculated violence-related crude mortality rates (CMRs) and age- and sex-standardized mortality ratios (SMRs). We constructed a cause-specific Cox regression model to identify predictors of violence-related deaths. Of 1,328 deaths in the cohort, 57 (4%) were from violence. The violence-related CMR was 9.5 per 100,000 person-years (95% confidence interval [95% CI] [7.4, 12.4]) and the SMR was 6.8 [5.3, 8.9]. Young Indigenous people had a greater risk of violence-related death than non-Indigenous people (cause-specific hazard ratio [csHR] 2.5; [1.5, 4.4]). Young people who experienced detention had more than twice the risk of violence-related death than those who were charged only (csHR 2.5; [1.2, 5.3]). We found that justice-involved young people have a risk of dying from violence that far exceeds that of the general population. The rate of violence-related death found in this study is lower than that in U.S.-based studies, which most likely reflects lower population level firearm violence in Australia. In Australia, young Indigenous people and those released from detention appear key groups to target for violence prevention efforts.
Introduction
Few studies have examined the risk of violence-related death among young people who have had contact with the youth justice system (justice-involved young people) (Aalsma et al., 2016; Coffey et al., 2004; Ezell & Tanner-Smith, 2009; Lindberg et al., 2017; Sailas et al., 2006; Silva et al., 2020; Teplin et al., 2014). Most of this research has been conducted in the United States (Aalsma et al., 2016; Ezell & Tanner-Smith, 2009; Silva et al., 2020; Teplin et al., 2014). These studies found that violence, particularly firearm violence, was the leading cause of death among justice-involved young people (Aalsma et al., 2016; Ezell & Tanner-Smith, 2009; Silva et al., 2020; Teplin et al., 2014). This has largely been attributed to the high availability and access to firearms, lack of adequate welfare support, and inequitable access to healthcare (Aalsma et al., 2016; Teplin et al., 2014). A prospective cohort study found that young men and women released from youth detention in Chicago, United States were two and three times more likely than the general population to die from violence, respectively (Teplin et al., 2014). Two previous U.S.-based studies have also found that young Black or Hispanic people released from youth detention had a greater risk of dying from violence than non-Hispanic white people (Ezell & Tanner-Smith, 2009; Teplin et al., 2014). These studies also found that being male (Teplin et al., 2014) and having a history of substance offenses, alcohol use disorder (Teplin et al., 2014), gang involvement (Ezell & Tanner-Smith, 2009; Teplin et al., 2014), or intergenerational criminal justice involvement (Ezell & Tanner-Smith, 2009) increased the risk of dying from violence among young people released from detention in the United States. Given the high rates of violent deaths in the general population in the United States, particularly from firearms, the findings of these studies may have limited generalizability to other high-income countries such as Australia, Canada, the United Kingdom, France, and Germany, which have lower rates of violence at the population level (Grinshteyn & Hemenway, 2016).
Beyond the Unites States, little is known on the risk of dying from violence among justice-involved young people. Similar to trends in the general population (Grinshteyn & Hemenway, 2016), studies conducted in Australia (Coffey et al., 2004) and Finland (Lindberg et al., 2017; Sailas et al., 2006) found that a lower proportion of young people released from detention died from violence (3%–16%) compared to U.S.-based studies (48%–68%) (Aalsma et al., 2016; Ezell & Tanner-Smith, 2009; Teplin et al., 2014). Our previous study found that violence-related deaths among justice-involved young people in Australia often involved a weapon, were preceded by an altercation for men and a relationship breakdown for women, and had cannabis and/or alcohol present in the toxicology reports of the death (Willoughby et al., 2021). However, these studies did not examine predictors of violence-related death or compare the risk of dying from violence in the study cohorts to that in the general population. Based on evidence from all-cause deaths in the United States (Aalsma et al., 2016), the risk of dying from violence may differ by different types of youth justice contact, with more serious youth justice contacts (e.g., detention compared to being charged) associated with an increased risk of death. No studies, in the United States or elsewhere, have examined the risk of dying from violence among young people with different levels of contact with the youth justice system (e.g., being charged, receiving a community-based order, or held in youth detention).
The patterns and circumstances of violence-related death differ between countries with high and low rates of violence (Eisner, 2013) and, as such, the optimal prevention strategies are likely to also differ between these countries. An improved understanding of violence-related death among justice-involved young people in other high-income countries outside the United States is needed to inform prevention responses for these young people. Australia is a country with a lower rate of death from violence (1.0 per 100,000 population) (Serpell et al., 2021) compared to the United States (7.5 per 100,000 population) (Centers for Disease Control and Prevention, 2021). In a large, whole-population cohort of young people who had been charged, or sentenced to a community-based order or youth detention in the state of Queensland, Australia, we examined the risk of violence-related death after contact with the youth justice system. Specifically, we aimed to: (a) calculate the rate of violence-related death, (b) compare the risk of dying from assault (a subset of violence-related death) to that in the age- and sex-matched general population, and (c) identify predictors of violence-related death.
Methods
Study Population
We conducted a retrospective data linkage study of all young people who were charged with one or more offenses, sentenced to a community-based order or experienced youth detention in Queensland, Australia between June 30, 1993 and July 1, 2014. In Australia, cases involving young people are generally dealt with separately from adults in a specialized criminal justice system, known as the youth justice system (Australian Institute of Health and Welfare [AIHW], 2020). Over the study period, young people in Queensland, Australia, who were charged with an offense while they were aged 10 to 16 years came under the responsibility of Youth Justice Queensland (O’Leary, 2014). In some circumstances, young people in youth detention or under youth justice supervision could remain in the youth justice system after the age of 16 (O’Leary, 2014). The demographic characteristics of the study cohort are shown in Table 1 and described in the cohort characteristics section below.
Characteristics of the Cohort by Cause of Death.
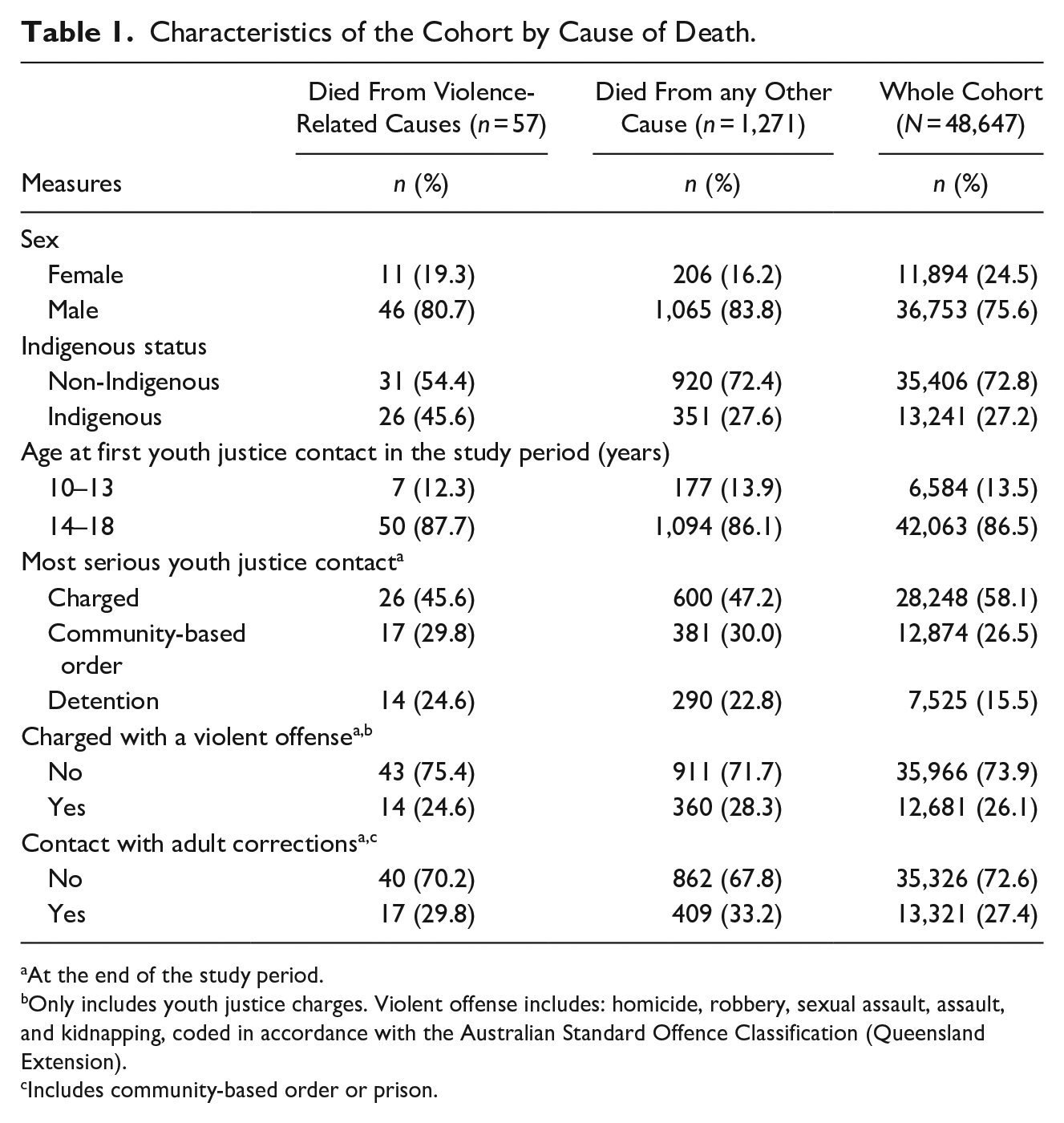
At the end of the study period.
Only includes youth justice charges. Violent offense includes: homicide, robbery, sexual assault, assault, and kidnapping, coded in accordance with the Australian Standard Offence Classification (Queensland Extension).
Includes community-based order or prison.
Linked Administrative Records
Young people (aged 10–18 years) who had contact with the Queensland youth justice system during the study period were included in the cohort. Youth justice records (June 30, 1993–July 1, 2014) were probabilistically linked to national death and coroner records, and state-based adult correctional records until June 30, 2016. Information on subsequent contacts with the youth justice system were available for the cohort until June 30, 2016. Youth justice data included sex, age, Indigenous status, dates (i.e., dates of charges; admission and discharge dates), and nature of the contact (i.e., charged, community-based order, or detention).
Death records were provided by the National Death Index (June 30, 1993–January 31, 2017), a national database of all deaths occurring across Australia. Coroner records were provided by the National Coronial Information System (NCIS; July 1, 2000–January 31, 2017), a database containing records from coroner’s investigations in Australia and New Zealand. Within Australia and New Zealand, coroners investigate preventable deaths, including those related to violence, suicide, motor vehicles accidents, and other situations in which there is a public health interest. They are not necessarily a medical doctor, but often a magistrate who completes a thorough investigation into the circumstances that led to a death. A coroner’s investigation often includes police, toxicology, and autopsy reports that accompany a major fact-finding report, or the coroner’s report. Death and coroner records provided information on the cause, date and location of death, and Indigenous status.
Linkage of the youth justice records with the death and coroner records was conducted by the AIHW and the NCIS, respectively, using best-practice data linkage methodology, which has been shown to accurately and reliably identify deaths among justice-involved people in Australia (Kariminia et al., 2005; Tibble et al., 2018). Data linkage was conducted using participants’ name, sex, date of birth, and all known aliases. Including aliases has been shown to improve sensitivity in data linkage, without adversely affecting specificity (Tibble et al., 2018).
Adult correctional records were provided by Queensland Corrective Services (January 1, 1994–December 31, 2016) and contained information on the dates and nature of contact (i.e., community-based order or incarceration) with the adult correctional system, and Indigenous status. The linkage was conducted by the Queensland Government Statistician’s Office using participants’ name, sex, date of birth, residential postcode, a unique individual identifier created by the police and all known aliases. Data were right censored at June 30, 2016 to ensure complete coverage of all data sources.
Ethics
The study was approved by the Griffith University (2016/376), AIHW (EO2016/3/280), and Victorian Department of Justice and Community Safety (CF/16/17318) Human Research Ethics Committees, and by the Department of Youth Justice (Queensland), Queensland Corrective Services, and the Western Australian Coronial Ethics Committees.
Role of the Funding Source
This work was funded by the National Health and Medical Research Council (GNT1151103, GNT1171981). The funding source had no involvement in the study design, the collection, analysis, and interpretation of data, the writing of the report, or the decision to submit the paper for publication.
Outcomes
The primary outcome was violence-related death occurring in the community following contact with the youth justice system. This was a categorical variable coded as: 1 = violence-related death, 2 = death from other cause (used for the competing risk analysis) and was coded as missing for people who did not die over the study period. As the rate and risk factors for violence-related death are likely different during incarceration compared to the community, deaths and person-time occurring during a period of youth detention or adult incarceration were excluded from analyses. Deaths were considered to be violence-related if the underlying cause was coded as assault, sequelae of assault, legal intervention, or maltreatment syndromes using the following International Classification of Disease (ICD) codes in either death or coroner records: E960 to E978, 995.50 to 995.54, 995.59, 995.80 to 995.85, T74, X85 to Y09, Y87.1, Y35, and Y89.0 (Supplemental Appendix 1). Additional deaths coded as violence-related in the coroner records were included because, for deaths investigated by a coroner, there may be a lag in updating the cause of death in the national death records after a coroner has made a finding (e.g., on notification of death, the cause could be coded as undetermined intent, which may be changed to assault after a coroner’s investigation) (Australian Bureau of Statistics, 2020). We also included deaths in the coroner records where the “intent” of death was precoded in the database as either “assault,” or “legal intervention” (i.e., the killing of a person by a police officer acting in the course of duty [Doherty & Bricknell, 2020]) where the officer was in close contact with the deceased. As this study focused on interpersonal violence, deaths from suicide (i.e., self-directed violence) were not included in the outcome.
To examine the effect of including additional violence-related deaths identified in coroner records that were not coded as violence-related in the death records, we conducted a sensitivity analysis wherein only deaths coded as violence-related in the death records were included in the analysis.
Measures
The cohort was divided into three mutually exclusive groups according to the most serious type of youth justice system contact experienced over the study period. The groups were: (a) receiving one or more youth justice charges without being sentenced to a community-based order or experiencing youth detention (charged), (b) being charged and receiving at least one community-based order without experiencing youth detention (community-based order), or (c) being charged and experiencing youth detention (including pre-trial detention) at least once (detention).
The following factors were examined: sex (1 = female, 2 = male), Indigenous status (1 = non-Indigenous, 2 = Indigenous), age at first youth justice contact in the study period (1 = 10–13, 2 = 14–18 years), most serious youth justice contact during the study period (1 = charge, 2 = community-based order, 3 = detention), charged in the youth justice system for a violent offense during follow-up (0 = no, 1 = yes), and contact with adult corrections during follow-up (i.e., community-based order and/or incarceration; 0 = no, 1 = yes). These variables were ascertained from the linked administrative records (described above). To minimize under-ascertainment, a person was considered Indigenous if they were coded as such in any available data source.
Data Analyses
Descriptive statistics were calculated for the cohort overall and stratified by cause of death. We calculated violence-related crude mortality rates (CMRs) per 100,000 person-years. Time at risk was calculated as time spent in the community from the date of first contact with the youth justice system until death or the end of the study period, excluding any time spent in youth detention or adult incarceration.
Standardized mortality ratios (SMRs) were calculated to compare the risk of violence-related death in the cohort to that of the general population in Australia. Mortality rates in the cohort were standardized by age and sex to the 2005 (the mid-point of the study period) population. Australian population mortality rates were obtained from the AIHW’s publicly available data on mortality (AIHW, 2018). These data are reported by ICD chapters and, therefore, the mortality rates for deaths related to violence reported by the AIHW contain only deaths where the underlying cause was assault (ICD-9: E960–E968; ICD-10: X85–Y09), a narrower definition of violence than considered in this study (Supplemental Appendix 1). As such, only deaths in the cohort, which met this narrower definition (referred to as deaths from assault), were included in the calculation of SMRs.
We constructed univariable and multivariable, cause-specific Cox regression models to identify predictors of violence-related death (Dignam & Kocherginsky, 2008). Cause-specific Cox regression models are an extension of the standard Cox model, where a Cox regression model is applied to both the outcome of interest and any competing risks (i.e., any cause of death that was not violence-related) simultaneously (Dignam & Kocherginsky, 2008). All factors except for sex, Indigenous status, and age at first contact were included as time-varying covariates, where the values represented the person’s status at the time of each most recent contact with the youth or adult justice system during the study period. All analyses were performed using Stata/SE Release 15.
Results
Cohort Characteristics
Over the study period, 49,011 young people had contact with the youth justice system in Queensland. Of these, 321 were excluded from the analysis due to data linkage errors, 20 were excluded as their age was missing in all records, and 19 were excluded as they died during a period of youth detention or adult incarceration (none from violence-related causes). The remaining 48,647 (99.3%) people were included in analyses.
Across the cohort, there was a total of 625,607 person-years of follow-up; 597,490 in the community and 28,117 during incarceration (the latter of which were removed from analyses). Each young person was followed for a median of 13.0 years (interquartile range [IQR] 7.9–17.8). The median age at first youth justice contact during the study period was 15.3 years (IQR 14.0–16.0; range 10–18). The median age at the end of the study period was 28.7 years (IQR 23.7–33.7) for those who were alive, and the median age at death from any cause was 23.9 years (IQR 19.4–29.0). More than half of the cohort only received a charge over the study period (n = 28,248, 58.1%). The remainder were sentenced to a community-based order without experiencing detention (n = 12,874, 26.5%), or were sentenced to youth detention at least once (n = 7,525, 15.5%). During follow-up (i.e., from first contact with the youth justice system until death or the end of the study period, excluding time in youth detention or adult incarceration), there were 1,328 deaths from any cause in the community. We identified 57 (4%) deaths that were from violence-related causes. Of these, 53 were identified through death records and an additional four deaths were identified from coroner records. The most frequent other cause of death was suicide (n = 461, 35%; Supplemental Appendix 2).
Nature of Violence-Related Death
The majority of the 57 young people who died from violence-related causes were male (n = 46, 81%; Table 1). The median age at death of those who died from violence was 24 years (IQR 19–28). Despite Indigenous people comprising 27% of the cohort, just under half (n = 26, 46%) of the young people who died from violence-related causes were Indigenous. Of justice-involved young people who died from violence, 46% of them (n = 26) only received a charge over the study period, 30% of them (n = 17) were sentenced to a community-based order without experiencing detention, and 25% of them (n = 14) were sentenced to youth detention at least once. Just under one-third (n = 17, 30%) of those who died from violence had any contact with the adult criminal justice system (i.e., community order or incarceration); all of whom were incarcerated in the adult system at least once over the study period. The majority of violence-related deaths involved the use of a weapon (n = 40, 70%), which was most frequently a sharp object (n = 30, 75%), followed by a firearm (n = 5, 13%) and a blunt object (n < 5). Eleven (19%) young people who died from violence-related causes had contributing causes of death (i.e., secondary causes) that were not directly related to violence or injuries sustained during the fatal event; these were commonly substance-related (e.g., mental and behavioral disorders due to use of alcohol; n = 7, 64%).
Rate of Violence-Related Death
The CMR for violence-related death in the community was 9.5 per 100,000 person-years (95% confidence interval [95% CI] 7.4, 12.4; Table 2). The CMR was 17.2 per 100,000 person-years [11.7, 25.3] for young Indigenous people and 6.9 per 100,000 person-years [4.9, 9.9] for young non-Indigenous people. When stratified by most serious youth justice contact, the violence-related CMR was 18.4 per 100,000 person-years [10.9, 31.0] among those who experienced youth detention, 10.2 per 100,000 person-years [6.3, 16.4] among those who experienced a community-based order, and 7.3 per 100,000 person-years [5.0, 10.8] among those who were charged only.
CMRs and Cause-Specific Cox Regression Models for Predictors of Violence-Related Deaths Among Young People who have had Contact With the Youth Justice System.
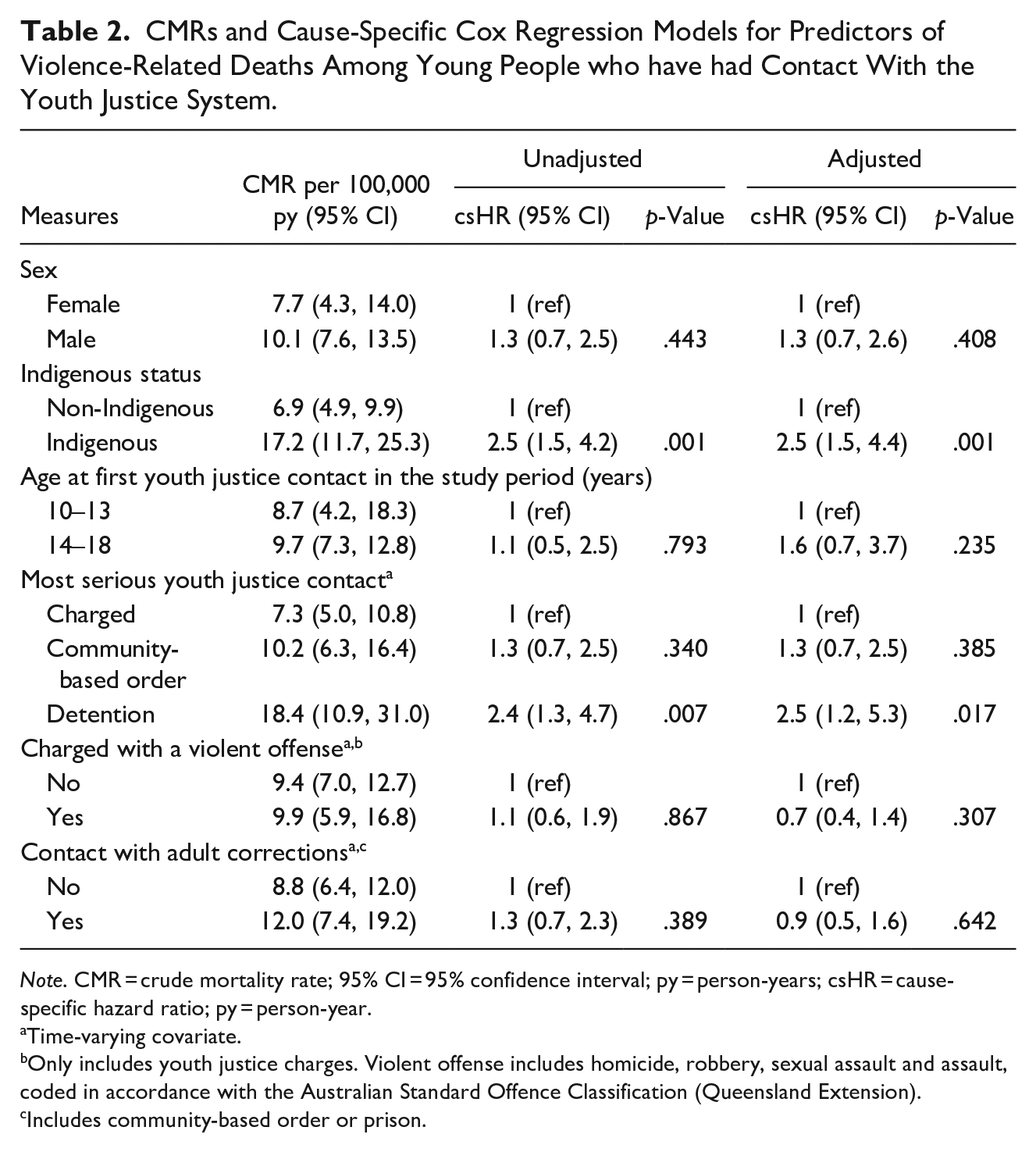
Note. CMR = crude mortality rate; 95% CI = 95% confidence interval; py = person-years; csHR = cause-specific hazard ratio; py = person-year.
Time-varying covariate.
Only includes youth justice charges. Violent offense includes homicide, robbery, sexual assault and assault, coded in accordance with the Australian Standard Offence Classification (Queensland Extension).
Includes community-based order or prison.
Of the 57 violence-related deaths, 56 (98%) were consistent with the definition of assault in publicly available general population data. The SMR for deaths from assault was 6.8 (95% CI 5.3, 8.9; Table 3). For young women, the SMR was 13.7 [7.6, 24.7], and for young men the SMR was 6.1 [4.6, 8.2]. The SMR for those whose most serious youth justice contact was detention was 11.7 [6.8, 20.2], 7.0 [4.4, 11.3] for those whose most serious contact was a community-based order, and 5.6 [3.8, 8.2] for those who were charged.
SMRs for Deaths From Assault Among Young People Who Have Had Contact With the Youth Justice System.
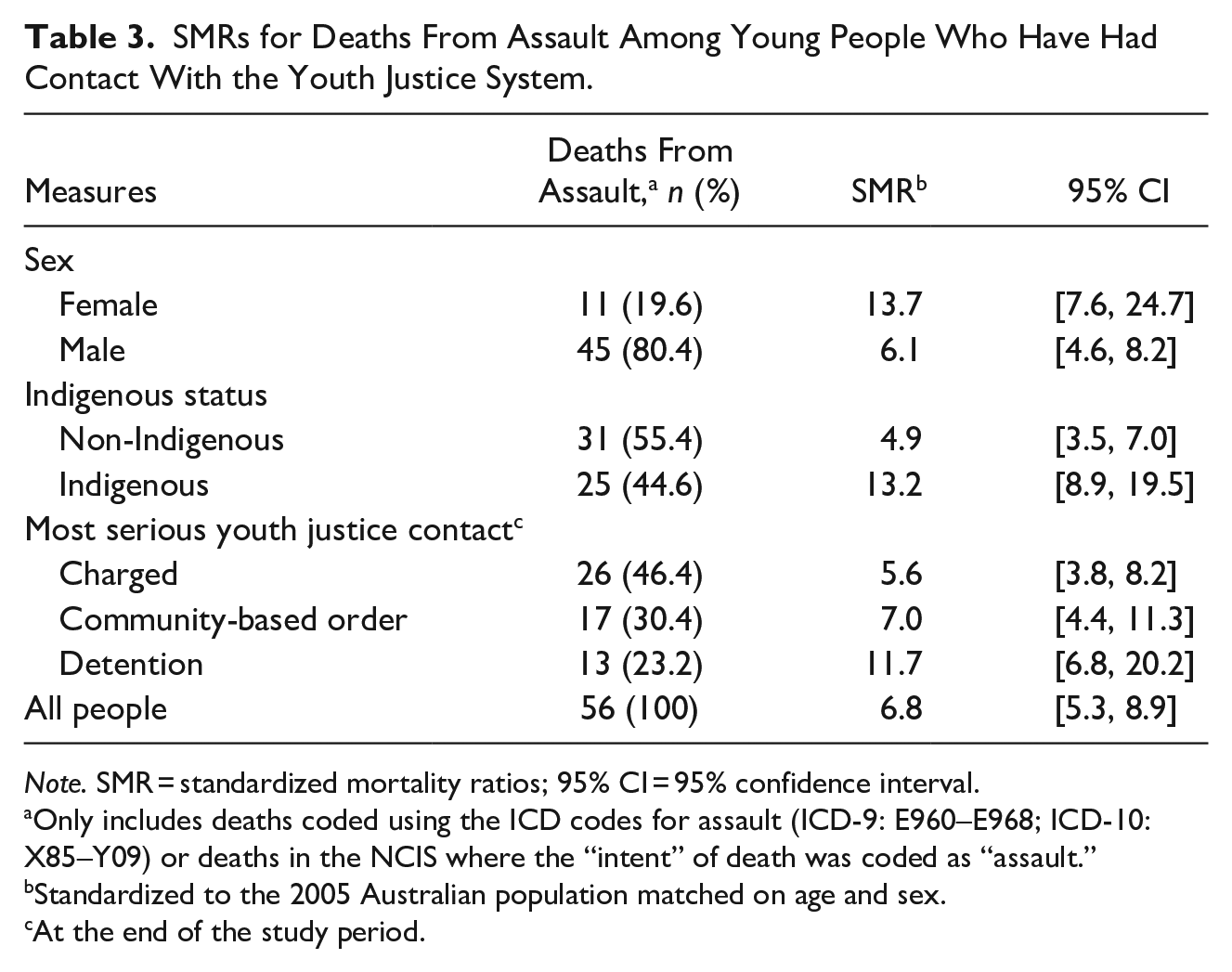
Note. SMR = standardized mortality ratios; 95% CI = 95% confidence interval.
Only includes deaths coded using the ICD codes for assault (ICD-9: E960–E968; ICD-10: X85–Y09) or deaths in the NCIS where the “intent” of death was coded as “assault.”
Standardized to the 2005 Australian population matched on age and sex.
At the end of the study period.
Predictors of Violence-Related Death
In the multivariable model, young Indigenous people had a greater risk of dying from violence-related causes than non-Indigenous people (cause-specific hazard ratio [csHR] 2.5; 95% CI 1.5, 4.4; p = .001; Table 2). Young people who experienced youth detention had 2.5 times ([1.2, 5.3]; p = .017) the risk of dying from violence-related causes compared to young people whose most serious youth justice contact was a charge. The risk of dying from violence did not differ by sex or whether the young person was charged with a violent offense during the study period (p > .05).
Sensitivity Analysis
The results of the sensitivity analysis that included 53 violence-related deaths that were identified through the death records only were consistent with our primary analysis (Supplemental Appendices 3–4).
Discussion
This study examined violence-related death in a large, whole-population cohort of young people who were followed for up to 23 years after contact with the youth justice system in Queensland, Australia. Our findings show that justice-involved young people in Australia, like their peers in the United States (Teplin et al., 2014), have an elevated risk of dying from violence. Justice-involved young people in Australia are almost seven times more likely than the age- and sex-matched general population to die from violence-related causes (SMR = 6.8). The risk compared to the general population is elevated for all justice-involved young people, regardless of the type of youth justice contact experienced.
Although the rate of violence-related death found in this study is lower than that found in previous studies on young people released from detention in the United States (Aalsma et al., 2016; Ezell & Tanner-Smith, 2009; Teplin et al., 2014), it is consistent with a previous smaller study that examined mortality in young people released from youth detention in Victoria, Australia over 15 years ago (Coffey et al., 2004). In the United States, firearm violence is a key driver of violence-related death in the general population (Grinshteyn & Hemenway, 2016) and among justice-involved young people (Aalsma et al., 2016; Teplin et al., 2014). The difference in access to firearms between the United States and Australia likely contributes to the lower rate of violence-related death in Australia (Chapman et al., 2016). Additionally, increased access to social welfare (Tuttle, 2018) and healthcare services (Chon, 2010), such as is available in Australia, has been associated with a decreased risk of violence-related death in the general population. The findings of this study are likely to be more generalizable than previous U.S.-based studies to other high-income countries with similar population level rates of violence as Australia (e.g., the United Kingdom, Canada, France, and Germany). Our findings also provide some possible policy directions for countries aiming to reduce deaths from violence either at the population level, or among justice-involved young people.
We found that young justice-involved Indigenous people are more likely than non-Indigenous people to die from violence-related causes. Violence prevention requires countries with colonial histories, such as Australia, New Zealand, United States, and Canada, to consider the unique cultural needs of young justice-involved Indigenous people. In these countries, Indigenous people have higher rates of violence-related death and are overrepresented in the criminal justice system (Cunneen & Tauri, 2019). Due to historical and ongoing racist and discriminatory practices and policies, many Indigenous people in Australia experience multiple economic, health, and social inequities (Walter, 2016), which are in turn associated with an increased risk of violence victimization (Armstead et al., 2019) and criminal justice involvement (Cunneen & Tauri, 2019). Connecting young Indigenous people who have had contact with the youth justice system with culturally appropriate and trauma-informed services (Campbell et al., 2018) that focus on their health and well-being, including their connection to culture and community, may assist in reducing these violence-related deaths.
In contrast to previous studies of justice-involved young people in the United States (Teplin et al., 2014) and young people in the general population (United Nations Office on Drugs and Crime, 2019), the risk of violence-related death did not differ between young men and women in the cohort. As young men in the general population are more likely to die from violence (United Nations Office on Drugs and Crime, 2019), our findings suggest that justice-involved young women have a risk of dying from violence that is elevated such that it is approximately equal to the risk of violence-related death among justice-involved men. Thus, justice-involved young women may be a group that is particularly vulnerable to experiencing violence. Although both young men and women in our study had an elevated risk of dying from violence compared to men and women in the general population, respectively, the elevation in risk compared to the general population was greater for young women than men. Young women, both in the general population (United Nations Office on Drugs and Crime, 2019) and those who have had contact with the youth justice system (Willoughby et al., 2021), are more likely to be victims of intimate partner violence, whereas young men are more likely to experience violence perpetrated by a friend or an acquaintance. As such, prevention programs should address the sex-specific drivers of violence victimization in each group.
We found that young people who experience detention have an increased risk of violence-related death compared to those whose most serious contact was a charge. This may be suggestive of a dose–response relationship wherein increasing seriousness of youth justice contact is associated with an increased risk of dying from violence. However, we are not able to determine from our study whether this association is causative. Previous U.S.-based research has also found that young people who were incarcerated were more likely to die from any cause than young people whose most serious contact was a charge (Aalsma et al., 2016). It is possible that being released from youth detention may present new risks or exacerbate existing risks for violence-related death (e.g., homelessness and substance use issues (Decker et al., 2018)). Young people who experience detention may also differ from those who have not been incarcerated in ways which are associated with an increased risk of violence-related death. Rather than the experience of detention influencing a person’s risk of dying from violence, it may be that those who experience detention have pre-existing risk factors for violence-related death that are less common among those who are only charged with an offense. Given the evidence that incarceration is largely ineffective at addressing the reasons for committing offenses as a young person (Lambie & Randell, 2013), our findings provide further support to reduce the use of detention as a criminal sanction for young people.
The use of detention is an international human rights issue for young people (United Nations Committee on the Rights of the Child, 2019). The United Nations mandates that detention should be a sanction of last resort, only to be used in exceptional cases, for the minimum necessary time period (United Nations, 1990), and never applied to young people under 16 years (United Nations Committee on the Rights of the Child, 2019). However, youth justice practices in many countries, including Australia, are inconsistent with these international standards (Cunneen et al., 2016). In Australia, children as young as 10 years of age can be charged with an offense and incarcerated (Cunneen et al., 2016). Australia has recently been criticized internationally for this policy, and campaigns to “raise the age” in Australia are underway (Gordon, 2021). Efforts to reduce the use of incarceration for young people should be paired with efforts to ensure that the treatment of young people in the criminal justice system is consistent with their needs and human rights (United Nations, 2019).
This study cannot establish whether youth justice system contact increases a person’s risk of dying from violence. It is possible that health and social factors may predispose some people to both youth justice system contact and experiencing violence. Health and social inequities, such as homelessness, low socioeconomic status, poor mental health, and substance-use issues, are common among people who have contact with the youth justice system (Borschmann et al., 2020; Hughes et al., 2020) and are also associated with an increased risk of violence victimization in the general population (Armstead et al., 2019). Young people who experience these types of disadvantage in the community may be more likely to have contact with the youth justice system and also have a greater risk of dying from violence. Addressing these health and social disadvantages may help to reduce the risk of violence-related death and future criminal justice system contact among justice-involved young people. Despite the whole-population cohort design and extended follow-up period (up to 23 years), our study was limited by the relatively small number of violence-related deaths occurring during the study period. Efforts to improve the ascertainment of these often underreported deaths (Andreev et al., 2015) was enhanced by using two national death databases. However, as coroner records were only available from July 2000, we may still have under-ascertained violence-related death in the cohort. Although our study was restricted to one state in Australia, due to the large whole-population cohort, our findings are likely to be generalizable to justice-involved young people nationally and are similarly likely to be internationally relevant, particularly for other high-income countries with similar criminal justice systems and patterns of violence at the population level. Future studies could explore whether patterns of offending (e.g., repeat compared to “once-off/sporadic” offending) are associated with the risk of dying from violence.
Our findings on the rates of violence-related death among justice-involved young people in Australia differ from previous research based on U.S. samples. This likely reflects community and structural factors, such as the underlying rates of violence at the population level, access to firearms, and availability of social and health services in each country. Our findings question the generalizability of studies of justice-involved young people in the United States for other high-income countries with lower rates of violence-related death. To be effective, violence prevention strategies should be informed by evidence that is specific to the targeted population and setting. In Australia, the elevated risk of violence-related death among justice-involved young people represents an important public health issue. Young Indigenous people and those released from detention are at high risk of dying from violence and are therefore likely key groups to target for prevention efforts in this setting.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605231169490 – Supplemental material for Violence-Related Death in Young Australians After Contact With the Youth Justice System: A Data Linkage Study
Supplemental material, sj-docx-1-jiv-10.1177_08862605231169490 for Violence-Related Death in Young Australians After Contact With the Youth Justice System: A Data Linkage Study by Melissa Willoughby, Jesse T. Young, Rohan Borschmann, Matthew J. Spittal, Claire Keen, Katie Hail-Jares, George Patton, Susan M. Sawyer and Stuart A. Kinner in Journal of Interpersonal Violence
Footnotes
Acknowledgements
The views expressed here are solely those of the authors and in no way reflect the view or policies of Queensland Corrective Services, the Department of Children, Youth Justice and Multicultural Affairs (Queensland), or the National Coronial Information System (NCIS). The NCIS is a database source of data and is managed by the Victorian Department of Justice and Community Safety. JY receives salary and research support from the National Health and Medical Research Council (NHMRC) Investigator Grant (GNT1178027). RB receives salary and research support from the NHMRC Emerging Leader-2 Investigator Grant (GNT2008073). MS is a recipient of an Australian Research Council Future Fellowship (project number FT180100075) funded by the Australian Government. MW, JY, RB, GP, SS, and SK are researchers in the NHMRC-funded Centre of Research Excellence in Driving Global Investment in Adolescent Health (GNT1171981).
Author Note
The authors would like to acknowledge the passing of Professor George Patton and thank him for his invaluable guidance and critical feedback on this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was funded by the National Health and Medical Research Council (GNT1151103 and GNT1171981). The funding source had no involvement in the study design, the collection, analysis, and interpretation of data, the writing of the report, or the decision to submit the paper for publication.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.