
Abstract
The violence against disabled women has its own mechanisms, which differentiates it from the violence suffered by women or the disabled in general. The few Spanish studies on this issue have focused on “double discrimination,” instead we propose intersectionality as a more suitable epistemological framework. The research, carried out in Spain, is based on five life stories of disabled activist women which show us how heteropatriarchal and ableist violence intersect in their lives, and the resistance mechanisms that they develop to deal with it. This research gives important clues to plan and design effective interventions for and with disabled women.
Introduction: Women at the Intersection
The violence suffered by disabled women has its own mechanisms, which differentiates it from the violence suffered by women or the disabled in general, and means that institutional measures to protect women oftentimes do not correspond to their situation. According to the European Parliament (2006), 80% of disabled women will suffer some form of violence during their lives. Furthermore, as reported by the International Network of Women with Disabilities in 2012, violence against disabled women takes many forms including isolation, psychological maltreatment, forced abortion, forced sterilization, economic exploitation, confinement, excessive medicalization, and abandonment. It is a form of violence that is invisible and made invisible that happens mainly in the home and in care facilities and which is perpetrated against people in a highly vulnerable position (Nannini, 2006; Oktay & Tomkins, 2004; Saxton et al., 2001; Young, Nosek, Howland, Chanpong, & Rintala, 1997).
The few studies (such as those by Iglesias, Jonecken, Gil, Mickler, & Knudsen, 1998, and Mun, Conde, & Portillo, 2006, to name the most in-depth ones) carried out on this issue in Spain have focused on the “double discrimination” suffered by these women as a result of their disability and their gender. The problem with this focus is that it portrays these women as passive victims, ignoring their active role and the influence of other variables. We therefore propose intersectionality (Crenshaw, 1989) as a more suitable epistemological framework for tackling this issue. The research was based on five life stories of Spanish women with different types of disability, ages, and social backgrounds. They all shared a common factor, namely, their involvement in political activism for the rights of disabled people.
Firstly, we will present a brief contextualization of the theoretical framework for the discussion. We will then go on to describe the research methodology on which this work is based. And finally, we will set out the results of the analysis of the empirical material.
The Most Forgotten of the Forgotten, Theoretical Notes
Violence arises in certain systems of domination that give such acts meaning and legitimacy. Acts of aggression cannot, therefore, be seen as isolated or individual events but as clear evidence of much wider violence of a symbolic nature. To analyze violence against disabled women from an intersectional perspective, it is therefore vital to identify the systems of domination in which they are immersed. On one hand, we find an ableist system of domination that defines certain bodies as incapable, invalid, unsuitable (Sobsey & Mansell, 1990). While concepts such as gender and race have been dismantled by the social sciences, disability is the last bastion of the reification of biology as a justification for social inequality, due to the persistence of the medical model. Activists and academics in the field of disability studies encourage a social model (Barton, 1996; Shakespeare, 1993; among others) that treats disability as a situation of social oppression. However, although these approaches help to denaturalize the violence experienced by disabled people, they suffer from a certain androcentricity, making it necessary to tackle the subject from the perspective of the specific experience of disabled women (Crow, 1996; Morris, 1993; Wendell, 1996; among others).
The ableist system colludes with a patriarchal system that generates high levels of violence not only against women but also other people who due to reasons of gender or sexuality are dependent on others for their care (Butler, 1990). Although this violence has been widely analyzed and denounced in feminist studies, it has not always taken into account the specific situation of disabled women. With regard to gender roles, feminists struggle against the patriarchal definition assigned them, but these are precisely the roles which are denied to disabled women (Fine & Asch, 1988; Harris & Wideman, 1988). In this respect, theories on feminist disability studies allow for a more complex analysis undertaken from an intersectional perspective. Intersectional theory allows us to analyze, dynamically and in context, how the different variables interact and affect subjects’ symbolic and material positioning. It is important to point out that this process is not independent of the subject, but there is a strategy that means that, in different situations, one variable stands out when determining a person’s identity (Guzmán & Platero, 2014). In this respect, it is crucial to pay attention to the everyday actions, to the personal experiences that allow us to identify the agency of the subject and their acts of “(micro)resistance,” along the lines indicated by Goffman (1963) when he speaks about the strategies for stigma management and by Juliano (1998) when she calls for the agency of women within seemingly conservative structures.
Making History: The Stories of Five Disabled Women
This work is based on five life stories. This technique allows us to understand the experiences of the subjects based on the subjective meanings they themselves give them, as they are not just personal narratives but also unique understandings developed over biographical, historical, and spatial time (Bertaux, 1981). This is an ideal methodological approach for learning about oppressive experiences or about people who are ignored or excluded from official records (Kohler, 2008). We therefore followed the tradition of treating disabled women as speakers generating knowledge in order to overcome the persistent silencing of their narratives (Gilson, Cramer, & DePoy, 2011; Shah, Tsitsou, & Woodin, 2016).
The sample (see table 1) comprised five Spanish women with differing degrees and types of disability (cognitive, sensory, physical, and mental), from different places and social backgrounds, aged from 35 to 59 years old. These women were specifically selected for their involvement in Spanish political activism, as we were interested in learning about the lives of empowered women who have come to be critical of their situation and become leaders of the movement. The approach is based on the recommendations of Plummer and Findley (2012) who, following a review of the literature about violence against disabled women, suggest “the use of the empowerment perspective, strengths perspective, and feminist theory to frame this issue” (p. 26). We were not therefore interested in identifying a particular type of impairment but rather in understanding disability as a situation of social oppression. We based our work on the hypothesis that, although they may not identify it as such, they had suffered some type of violence due to their position as “disabled women.” Our intention was to understand how resistant subjectivities in the face of violence occur, how important they are, and what form they take.
Characteristics of the Women Interviewed.
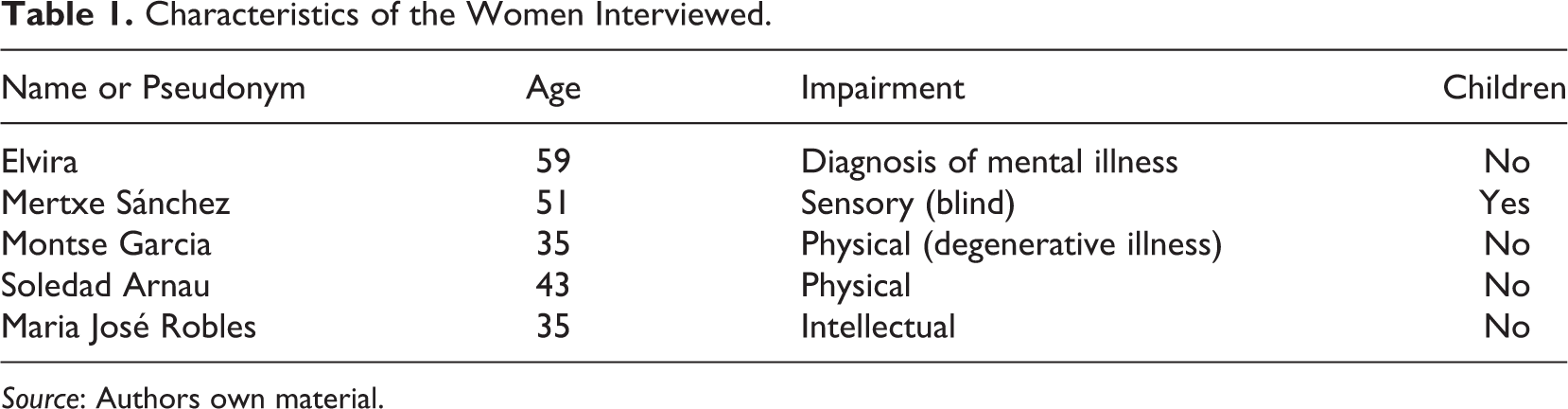
Source: Authors own material.
The women were selected intentionally and contacted individually and personally. This was possible thanks to personal and political relationships between them and us: We are committed researchers involved in the Spanish Independent Living Movement and in feminist activism. This also facilitated an empathetic and friendly atmosphere that gives the study an epistemological advantage, as noted by Shah, Tsitsou, and Woodin (2016). The aims and methodology of the study were explained in detail to all the respondents, and they were asked whether they wished to use their real names. Apart from Elvira, who preferred to remain anonymous, all the women agreed to their names being published and, in fact, several insisted that we also included their surnames, as they wished to raise awareness of their stories and views. Our research was not supervised by an “expert” external ethical committee; rather it was our interlocutors who validated our investigative practices. They wished to make an active and public contribution to the construction of other narratives about themselves and the groups to which they belong. Furthermore, they all gave permission for the results of the study to be widely published.
The life story interviews took an average of 2–3 hr and were carried out using an open script. The interviews were subsequently transcribed literally and then decoded taking into account previously selected fields based on a specialized bibliographical review of the literature on violence, disability, and intersectionality. Once the life stories were decoded and a first draft of the analysis prepared, the participants reviewed the texts and, in some cases, added further details or explanations. They asked for some sections to be removed or amended. The narratives were also expanded using information taken from texts published by the women themselves or in specific cases by third parties referencing their stories. In this work, the analysis is organized under three headings: care and feelings, body (re)perceptions, and the women’s positioning as role models. For this publication, the selected extracts were translated into English by a professional translator.
Storytelling
Feelings, (In)Dependency, and Family Duties
If they love you, shouldn’t they take care of you?
The family is understood as a source of security, love, and unconditional support, which amplifies an aggression when it takes place within it. This is what happened to Elvira, who suffered physical, sexual, and emotional abuse at the hands of her father, until she could not take it anymore and tried to commit suicide. She was subsequently diagnosed with schizophrenia. As shown by O’Hare, Shen, and Sherrer (2015), there is a correlation between childhood sexual abuse, suicide attempts, and diagnoses of schizophrenia.
Given their central role and importance in our lives, families are also potential sources of overprotection and suffocation. Because of this, when a person needs the care of their family to survive, the effort required to maintain some level of autonomy can be gargantuan. In Montse’s case, this meant battling against her mother’s veiled message of “as we have to care for you, you have no right to make any decisions.” The lack of resources and support exacerbates this situation in which the dependent person (Montse) is trapped in a dual, hierarchical relationship with the carer (her mother, who was also caring for her own mother who suffered from Alzheimer’s). The devaluation of the work of carer has a double impact, affecting not only the status of the carer but also that of the person cared for, who is perceived as an object or burden (Hughes, McKie, Hopkins, & Watson, 2005). In this sense, this dual conception of care, restricted to a private, feminized, and devalued sphere, contributes to relationships which are problematic and violent (in both directions).
The vulnerable situation in which the recipients of care find themselves is even greater in total institutions where, as described by Goffman (1961), residents must submit themselves to the anonymity of institutional rules that structure their lives and erase their individuality. Soledad tried to rebel against this dynamic, which led to her being punished by the institution: neglect, abandonment, psychological maltreatment, threats, and so on. If I had to get up at 6 am, they got me up at 4 am, to piss me off. While they were giving me breakfast, they talked about “bloody so-and-so,” I don’t know who, and I was disgusted and they could tell. I didn’t say anything, but they could tell. As they [the carers] saw it, it was an important point […] there was psychological and physical violence.
(Un)caring partners
In all the narratives, love and caring are presented as interlinked in a conflictive relationship. For Soledad, Montse, and Mertxe, who need daily physical support, there is a greater fear of forming partnerships which would put them in a position of dependence and inferiority. This fear is heightened by the environment and intensified when a disabled person enters a romantic relationship with a nondisabled person. In Mertxe’s case, her relationship with a nondisabled man was supported by her family as, in fact, they saw her place as a recipient of care as unchanged. It is taken for granted that disabled people are the receivers of care and not caregivers. This results in a system designed to ensure that they themselves feel incapable and transmit this incapacity. There is certainly a performative aspect to this. What happened was a transfer of care that did not change my status as the receiver of care, wearing down and undermining our loving relationship (…) this helped make me feel undervalued by my partner, but most of all I undervalued myself. I didn’t feel able to tackle day-to-day living, neither as part of a couple nor in my personal life. (Mertxe)
Care is seen from a practical and materialist perspective, in terms of daily physical support in respect of hygiene and feeding which simplifies the symbolic and emotional aspects that support couples’ relationships. Montse explains how she feels “cared” for by her partner in the sense of having company and emotional support. In fact, he is the only person she allows to go with her to the hospital, despite her family’s objections. Montse has found a form of care that allows her to feel loved without feeling suffocated.
Nevertheless, such women are frequently afraid of making their loved ones “suffer” or feel “trapped” (Rich, 2014). It often ends up changing the nature of the relationship: “I am always asking myself: If I really love this person, wouldn’t it be better to let him go?” (Soledad). Feeling that you bring suffering to the people you love, and who love you, and that the price of sharing life with you is “too high,” leads women to make difficult decisions such as breaking off a relationship because by continuing “I would be condemning him for life, the time we are together. I thought that without me he could do many more things than would otherwise be possible…” (Soledad).
The idea that a disabled person’s partner suffers and feels trapped by the need to provide care often features in the collective imagination. The result is that, when people enter into this type of relationship, it is assumed by society that the normal person must have some kind of material motive, a desire for abnegation or sacrifice or even a dark or pathological motive (Shakespeare, 1999). Whatever the motive, the relationship itself is incomprehensible to society, made evident in the symbolic violence of gestures such as looking at the couple judgmentally: “I get disapproving or pitying looks at me and my partner, as if to say ‘poor thing’. Or they assume that we must be related, ‘She must be his mother, or sister’…” (Soledad). These gestures, together with smiles, questions, or paternalistic treatment, may seem minor issues, but they illustrate how disabled people are viewed by society (Keith, 1996, p. 93). This social penalty, the result of ignorance and fear of what is different, is even more painful and common in the person’s immediate circle. Soledad explains that her partners have had to deal with reactions from their families such as, “Is this some kind of act of rebellion? What are you doing with a girl in a wheelchair?” And friends who say: “Look, mate, I wasn’t going to say anything, but someone has to say something, and I’m your friend, so I have to ask: ‘What do you think you’re doing?!’” These types of messages, as described by Keith (1996), constitute a type of violence that affects how a disabled person sees themselves.
When both partners are disabled, as in Montse’s case, this can lead to a conflict, as neither partner is perceived as capable of taking on the role of carer. Nevertheless, it is regarded as more understandable that two people in this situation could meet and get together. And for the couple themselves, it may be more satisfactory to establish a relationship between equals in which they can share their experiences of discrimination and in which there is no imbalance resulting from expectations of gratitude or duty. This is the situation of Maria José and Elvira. Maria José regards this as very positive, compared with her previous partner who did not have any intellectual disability as “before I wasn’t accepted and now I am. He has a disability, the same as me. I understand him better, in every way.” For Elvira, her current relationship represented a key turning point. “From then on the story of my life began again and I never wanted to commit suicide again.” Her partner was also maltreated and sexually abused as a child, and subsequently diagnosed as mentally ill. They found in each other the emotional support they never had from their families, to deal with the present and start looking toward the future.
“She won’t manage alone”: When being a mother is not what you expected
Disabled women suffered from “conflicting roles”: As women they are expected to take on a caring role, but as disabled people they are socialized as and relegated to a position as an object of care (Rohrer, 2005). The maximum expression of this can be found in the most archetypal feminine role: motherhood. For our respondents, it is a problematic topic: Some do not consider themselves capable or don’t even want to contemplate it, and others fear that their children would suffer as they do. Sometimes, the conflict originates on the part of the partner, who rejects them when it is time “to have children.” They can be good girlfriends but they will never be “the mother of his children.” Mertxe is the only one of our respondents with children. Despite the support of her family and friends, she had to endure ableist violence from a society that continually questions her role as a mother. The people who saw me in the street looked at me with surprise and mistrust. They said dreadful things to me. I carried my child in a carrier on my back. (…) and I had to listen to comments such as: How can you put your child at risk? Watch out in case you bump into anything! […] and even worse things said to a child of just 3 or 4 years old like: “You have to take good care of your mummy.” When I split up with my partner and realised I was capable of living in my own home, of maintaining it not just financially but like any other person, keeping it clean and tidy, and looking after my child properly, that was a revelation for me, I was reborn.
The Body Is a Battlefield
In the name of the doctor: Disciplines and knowledge in dispute
If there is one form of institutional violence that is common to the life stories of these women, it is the exercise of biomedical power used to name, categorize, regulate, and discipline their bodies. When the disability is physical, as in the cases of Soledad (arthrogryposis multiplex congenita) and Montse (degenerative autoimmune disorders), there is constant pressure, justified on the grounds of rehabilitation and improving their physical condition, that defines their bodies as deficient and faulty. I remember the devices for sleeping, I believe there are things you forget because they are so painful you don’t know how to deal with them […] The family says, “It was for your own good, we were doing what the doctors told us: so you could walk properly, without your back twisting.” But it really was pretty awful. (Montse) They did the rounds to see if they could “fix me,” to see if anything could be done, and in the end I don’t know how many doctors looked at me! They said there “wasn’t much that could be done with me” and I would have to be in the hands of doctors, traumatologists, “for the rest of my life.” (Soledad)
In the medical sphere, another area where disabled women suffer discrimination is in regard to their sexual and reproductive rights: lack of information; badly designed consultancies, clinics, and equipment; lack of training among health professionals; and so on. It makes these services inaccessible to these women. For Soledad, the lack of adapted equipment led to a wrong diagnosis of early menopause that resulted in life threatening medical complications. Soledad explains: “I said, ‘Look, I’m bleeding’; they didn’t want to and didn’t look properly. ‘We’ll look at you here in the wheelchair and that’s that’, they said.” Even today, getting a gynaecological examination continues to be a battle for her.
As Montse says, the power of the biomedical profession results in “a body that is the property of the doctors, turning you into a lump of meat dissected in the service of science. Your diagnosis and medical history give them a VIP pass to unlimited access to your body, to you” (DV 1 ). Or, as explained by Allué (2003), an alienation of the body that results in it being experienced as “an occupied territory invaded by strange objects and hands” (Allué, 2003, p. 106). Tension is generated when the subjects of this treatment reclaim agency, implementing mechanisms for reappropriating their bodies. This is the experience of peer support groups, as Montse found in the Liga Reumatológica (Rheumatological League, in English), whose members give each other advice on strategies for managing the illness, including the self-regulation of medication, hygiene, and other ways to deal with physical differences that often conflict with medical advice.
Escaping from (being) the ideal woman: Stigma as freedom from normality
Up to now we have referred to the medical diagnosis as the driver or certifier of stigmatization (Goffman, 1963). Nevertheless, it also acts as an identifying label in one sense that may be positive, as it defines one as belonging to a group and assigns a name (and treatment and support) to an experience that may be made more painful if it is out of sight. This was Elvira’s experience: The diagnosis of schizophrenia represented a recognition of the suffering that had led her to attempt suicide. I was destroying myself. The only way out of this situation was through diagnosis […] I had to have a mental illness in order to move forward, otherwise I wouldn’t have had the strength to go on and I wouldn’t have made it to my current age of 58.
It is important to understand the mechanisms of resistance used by the women themselves over their lives because, among other reasons, they can be key variables that some professionals may exploit. But they can also act as visible indicators of situations of violence. Rich (2014) highlights how stigma is used to justify and ramp up violence. Victims internalize stigma so that it becomes another part of the traditional social stereotype (heteropatriarchal) of disabled women. She discusses different strategies for coping with stigma which enable victims to survive by reframing the violence depending on the context, and others which contribute to the violence continuing or escalating. In the same way, the illness that was a source of pain and suffering for Montse was, at the same time, something that freed her from the ties of “normality”: “I wouldn’t have been able to face up to my family, the fear, the risk or being wrong. Perhaps I was so cautious that I wouldn’t have tried so hard to pursue certain goals.”
Her illness came to represent a turning point in which the usual concept of time, the linearity of chronos was questioned by the arrival of kairos: the corner, the profound change, metaphor for the life change experienced (Grunewald, 2009, p. 22). Montse described it as follows: “There is a moment when the illness wrecks everything. Then you have to see it as a chance to rebuild everything, and rebuild yourself.”
Marginalized femininities, reappropriated femininities
This reassessment of one’s life driven by the stigmatization suffered is a determining factor in the (re)construction of one’s gender identity. The “loss” of hegemonic femininity can also represent an opportunity for critical rethinking and the development of alternative femininities. Montse gradually came to accept her new body: There is a moment when you start to love yourself. You start to say, “Who says I am not feminine?” What does being feminine mean? You question the concept of femininity. (…) You start to look at yourself in the mirror more; you look at yourself, not at what you want to be, but really at yourself. Seriously affected by the fact I didn’t want to reveal what was happening. I took advantage of periods, not so much periods when my illness wasn’t flaring up, but just that I was shooting up tons of cortisone and felt a bit better […] all my relationships, which were eminently sexual, took place outside Barcelona, away from my home, as I didn’t want anyone to know I had degenerative illnesses. (Montse) My body is what allows me to exist. I am grateful for existing, and I understand that my non-hegemonic beauty is equally valid. It does not have less aesthetic value just because it is a dissident beauty. Nor does my femininity have less value, although it is not a strictly normative femininity. (Arnau, 2015)
Women Who Are Not Like Others
As reflected in their stories, these women have suffered many acts of violence throughout their lives, violence covered up by a pathologizing dialogue that shackled them to resignation. They have, however, found mechanisms for countering and resisting violence that have allowed them to construct their own alternative narratives. Undoubtedly, certain experiences and personality traits encourage these critical approaches. But above all there are situational variables which can be managed on the basis of their capacity for agency. Soledad and Elvira explain that access to knowledge was a very powerful tool for them. Soledad is currently completing her doctoral thesis, and her studies were for her a mechanism for demonstrating her social and personal worth. Elvira first encountered a critical discourse, describing other possible worlds, through books, which she read in secret. Her subsequent readings of feminist literature helped her to find rebellious and battling female role models with which she could identify.
Montse’s corporeal empowerment came from being in an environment that rejected normative forms of oppression that say which bodies are desirable (and which can and should therefore be publicly displayed) and which are not (and which should therefore be a source of shame and kept hidden). It was summer and I wondered, “Should I wear a skirt or not?” […] because it will be obvious that one of my knees is much bigger than the other. And you reach a point where you say, “So what?”, and this was helped by other friends who had also had operations on their knees and had scars and who had decided they couldn’t care less and they were going to the swimming pool and wherever they liked with their miniskirts and scars on their knees. (Montse)
For Maria José, it has also been fundamental to be able to express herself publicly as a woman with an intellectual disability, defending the rights of the group to which she belongs. She considers it essential that they are represented by spokespeople who share their experiences, as embodied in the slogan of the Independent Living Movement, “Nothing About Us Without Us.” This is because, taking up Spivak’s (1988) argument again, subordinated people are not always able to speak for themselves. Maria José explains, “There are some things my colleagues can’t do, maybe because they are embarrassed, or for some other reason. I can do them, and I can communicate.”
It is also important to note that resistance, rupture, and dissidence come at a cost. These women opened the way; they had no role models and have become role models themselves. They often feel alone and abandoned in their struggles. Other disabled women “are not like them.” Mertxe, for example, tells us that she is the only blind woman she knows who lives alone. Montse says, “They will write you off as selfish for putting yourself at the centre of your own life, accuse you of not being yourself (or what they expect you to be). This is the price of empowerment” (DV). Breaking with the norm frees women, but it also displaces them: “Whenever you try to become a bit more independent, an obstacle appears, you lose something: security, this false sense of refuge that continuity gives you, about what you are” (Mertxe).
Discussion and Implications for Social Work
Our intention was to understand how resistant subjectivities in the face of violence occur, how important they are, and what form they take. The intersectional perspective allows us to analyze how acts of violence are reframed over the course of a life and, in the same way, how mechanisms of resistance are developed. It is important to note that the processes of empowerment are not necessarily linear. They are mediated by a range of structural and individual factors such as the person’s material situation (economic and cultural status, place of residence, and the provision of care), personal factors (physical and psychological health), and emotional factors (loving relationships and support). Structures of domination are not always questioned head on. At other times, it is possible to tackle issues directly, but for this to occur, spaces for support and refuge are necessary, a secure place in a hostile environment. Our respondents have built up these networks and this knowledge based on their own bodies and experiences, through alliances and activism. They have learned how to mix the institutional with the radical, formal, and marginal structures, in order to open up cracks and fissures in the structures that subjugate them. The recognition of these “(micro)resistances” is vital for planning and designing effective social work interventions for and with disabled women.
We were interested in applying this approach to the life stories of disabled women. The respondents’ commitment to the research was essential for this. Not only did they generously share their life stories with us, they also collaborated actively in the construction of their narratives. These narratives provide evidence of acts of violence of different types, levels, and intensity which emerge at distinct points in their stories. It must be noted that these violent acts were not always perceived as such in the past. The respondents told us that the very process of thinking through their life stories, telling them and subsequently reviewing them, led them to identify past situations as violent. This shows the importance for these women of finding spaces in which they can speak and be listened to, in which they can reflect together on key aspects related to their life experiences as “women” and as “disabled.” Within the field of social intervention, these spaces help give rise to political involvement, they foster a raising of awareness, mutual support, and empowerment. They therefore represent spaces both for preventing and stopping and for responding to, the different forms of violence faced by this group.
It is also important to talk about these other forms of violence that place the other in a situation where they are despised, rejected, or undervalued and to detect and tackle them as such. These daily symbolic and linguistic acts of violence are the breeding ground that produces, at the extremes, the most serious and damaging violence. It is therefore important that social workers pay sufficient attention to all aspects of the symbolic mapping of disability. These women have grown up and developed in an environment dominated by a medical model that labels them as deficient, naturalizes the violence they suffer, and tells them that resignation is their only option. Diagnosis gives a situation (generally one of suffering) a name and a response: support, treatment, resources and, most importantly at the symbolic level, a reference group of people who are in the same situation. The antihospitalization movement in mental health and the Independent Living Movement gave them a space for countering and resisting violence without which they would not have been able to weave new narratives about themselves, narratives which formerly they could sense but could not easily structure. Changing how they perceive their differences, encouraging disability awareness: Beginning to understand how a different way of functioning, discriminated against, it is true, but not necessarily worse, has been key to their progress. It is therefore crucial to promote this type of organization, in which people with disabilities are given a voice and can represent themselves. In this way, the role of professionals should be that of support and of placing their technical and personal resources at the service of these initiatives, not to assume leadership.
In this respect, it is of key importance to also apply an intersectional perspective within social work in order to better detect the needs and demands of this group. With respect to gender identity, disability operates in an ambivalent manner: On one hand, there is less pressure to comply with hegemonic expectations, on the other, new mechanisms of subjection come into play. Excluded from traditional femininity, some opt to assume a queer/crip identity that rejects hegemonic roles and normative body types. Others choose to construct their own femininity, playing with conventional standards, rejecting others, and (re)appropriating others. Motherhood or a stable relationship with a partner can be another way for them to break with convention, as they have been told they could not occupy these roles which are reserved for real women. This means we must discard the stereotype of the disabled woman as a subject to be cared for, incapable of caring in turn. As we have seen, these views keep such women away from resources and professional services for fear of being questioned, thereby increasing their isolation.
When loving, caring relationships are strained it can lead to violence. It is especially dangerous in residential care environments where institutionalized individuals are in a very vulnerable situation that normalizes the most subtle forms of violence and makes them less able to combat the more explicit forms. It is important for the field of social work to undertake to ensure that these women have access to the professional resources they need to give them the greatest possible level of independence and to enable them to make their own decisions, such as those related to where and how they live. It is vital to stress the need for control over one’s body to prevent many of the situations of violence experienced by our respondents. Thus, personal assistance is presented as a crucial tool for prevention and protection against violence.
Footnotes
Authors’ Note
Andrea García-Santesmases is currently affiliated to: Internet Interdisciplinary Institute (IN3)-Universitat Oberta de Catalunya (UOC).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: This research has been funded by the Institute of Political and Social Sciences (ICPS), a reserch center affiliated to Universitat Autònoma de Barcelona (UAB).