
Abstract
The study presented here examined the gender differences in preferred strategies used by rural Native Hawaiian youths to resist drugs and alcohol. Seventy-four youths (60% of whom were female) in eight middle/intermediate or high schools participated in 15 different focus groups as part of a pilot-feasibility drug prevention study funded by the National Institute on Drug Abuse. Consistent with relational–cultural theory, the qualitative findings indicated that the girls favored drug resistance strategies that maintained relational connectedness with the drug offerer and considered the long-term relational consequences of different drug resistance strategies. Implications of these findings for the indigenous- and gender-specific prevention of drug abuse are discussed.
Compared with other ethnocultural groups, indigenous populations (American Indians, Alaska Natives, and Native Hawaiians) have disproportionally suffered adverse health consequences related to drug and alcohol abuse (Office of Applied Studies, 2009; Ta & Chen, 2008; Tann, Yabiku, Okamoto, & Yanow, 2007; Walters, Simoni, & Evans-Campbell, 2002). Furthermore, substance abuse has disproportionately affected indigenous women (Ta & Chen, 2008; Walters et al., 2002). Indigenous women had the highest drug-induced mortality rate in 2007 (11.5 per 100,000 of all deaths; Centers for Disease Control and Prevention, 2011) and have the highest perinatal risk related to substance use (Fuddy, Prince, & Tang, 2003; Indian Health Service, 1998–1999) compared with women in other major ethnocultural groups. Despite these issues, few studies have described and evaluated culture- and gender-focused substance abuse interventions for indigenous populations (Hawkins, Cummins, & Marlatt, 2008; Mokuau, Garlock-Tuialiì, & Lee, 2008; Ta & Chen, 2008).
The purpose of the study reported here was to examine gender differences in the preferred drug resistance strategies of one population of rural indigenous youths (Native Hawaiians). The study used relational–cultural theory (RCT) as a framework for understanding culture- and gender-specific interactions in the drug-related problem situations of rural Hawaiian youths. The theory was also used to understand the unique relational challenges experienced by Hawaiian girls in these situations. Examining gender differences in drug resistance strategies has implications for promoting developmentally and culturally appropriate, gender-specific drug resistance skills training for indigenous youths, thereby informing ecologically relevant substance abuse prevention programs for these youths.
Dimensions of Indigenous- and Gender-Specific Substance Use
While some studies on gender differences in the rates of substance use among indigenous youths have reported mixed findings (Hawkins et al., 2008), others have indicated significantly higher rates of substance use for indigenous girls than for indigenous boys (Schinke, Tepavac, & Cole, 2000; Wallace et al., 2003). For example, using a large, nationally represented sample across 420 different schools, Wallace et al. examined ethnic and gender differences in illicit substance use for 8th-, 10th-, and 12th-grade students. They found that across all ethnic groups, substance use was the highest among American Indian girls, with approximately 70% of these girls (compared with 54% of American Indian boys) having tried marijuana or hashish, 87% (compared with 81%) having tried alcohol, and 80% (compared with 69%) having tried cigarettes by the 12th grade. Epidemiological studies on Alaska Native and Native Hawaiian girls have similarly found gender disparities in rates of substance use, with these girls indicating a higher use of tobacco (Angstman et al., 2007; Glanz, Maskarinec, & Carlin, 2005; Glanz, Mau, Steffan, Maskarinec, & Arriola, 2007) and alcohol and marijuana (Mayeda, Hishinuma, Nishimura, Garcia-Santiago, & Mark, 2006) than their male counterparts.
Research has also identified gender-specific ecological risk factors for substance abuse for populations of indigenous youths. These studies have examined gender differences in the exposure to offers to use substances for American Indian (Dixon Rayle et al., 2006; Kulis, Okamoto, Dixon Rayle, & Sen, 2006) and Native Hawaiian (Okamoto, Kulis, Helm, Edwards, & Giroux, 2010, in press) youths. These studies also examined the perceived difficulty that these youths have experienced in dealing with these situations. In particular, Dixon Rayle et al. (2006) and Okamoto, Kulis, Helm, Edwards, and Giroux (2010) found that, compared with their male counterparts, American Indian and Native Hawaiian girls were exposed significantly more often to drug offers by peers and family members and found it significantly more difficult to resist these offers. Gender-specific research on indigenous youths has provided limited insights to account for these quantitative findings. Okamoto, Kulis, et al. (2010) indicated several reasons that may have accounted for Hawaiian girls’ higher exposure to offers to use substances (e.g., earlier initiation into substance use than boys). However, the study was limited in elucidating the reasons related to the perceived difficulty that these girls had experienced in dealing with drug offers.
Relational-Cultural Theory (RCT)
RCT evolved from clinical practice in the 1970s, when it was characterized by the centrality of relationships in women’s lives (Comstock et al., 2008). A central tenet of the theory is that women grow “through and toward” connection with others and that significant relationships are central to women’s sense of meaning and well-being (Jordan, 2001, 2008). West (2005) expanded on Jordan’s early theoretical principles by linking them directly to feminist theory building, while Comstock et al. elucidated the implications of RCT to counseling and direct practice. According to RCT, relational development occurs across the life span and is linked to individuals’ racial, cultural, and social identities (Comstock et al., 2008). In effect, psychological “disorders” become less about the individual and more about the relational and cultural context (Comstock et al., 2008; West, 2005). Disorders evolve more from culture-based relational disconnections between individuals than from problems or issues within the individual. West suggested that RCT had strong implications for the development of preventive interventions, including gender-specific interventions for youths in school settings.
To apply RCT to the lives of indigenous girls, it is important to understand their unique relational and cultural contexts. Some research has described these unique contexts for American Indian and Native Hawaiian youths and how these contexts may function to intensify both the risk of and protection from substance use for these youths (Hurdle, Okamoto, & Miles, 2003; Okamoto, Helm, Po‘a-Kekuawela, Chin, & Nebre 2009; Waller, Okamoto, Miles, & Hurdle, 2003). Specifically, these studies have described these youths’ close-knit networks of biological and ascribed family members within the home, school, and community and how these networks functioned as strong influences for or against the use of illicit substances. In other words, research has emphasized that indigenous youths live within a cultural context that both values and is characterized by close, interconnected relational networks and that these networks function as both ecological risk and protection. For indigenous girls, RCT would suggest that the demand to stay relationally “connected” is particularly strong, in that both gender and culture intersect to provide these girls with a sense of meaning and well-being through their significant relationships.
RCT can be used to understand indigenous girls’ perceived difficulty in refusing offers to use illicit substances from peers and family members that has been found in recent empirical research (Dixon Rayle et al., 2006; Okamoto, Kulis, et al., 2010). The theory suggests that indigenous girls’ perceived difficulty in dealing with drug offers may be an outgrowth of balancing harmony within significant relationships and the goal of abstaining in the use of illicit substances. This difficulty may place these girls at an increased risk of substance use, particularly when the ability to effectively refuse substances threatens the harmony within a significant relationship. RCT suggests that indigenous girls may feel increased social pressure to accept drugs and/or alcohol to mitigate discord or conflict in the relationship with the drug offerer, particularly since relational disconnection is incongruent with their culture- and gender-based norms and values.
In the study presented here, qualitative methods were used to examine the gender-specific considerations and preferences in drug resistance strategies for rural Native Hawaiian youths. Research has indicated that rural youths have higher rates of alcohol use than their urban counterparts (Swaim & Stanley, 2011), with rural minority youths having particularly elevated risks of substance use (Curtis, Waters, & Brindis, 2010). The analysis in this study elucidated the ways in which Hawaiian girls balanced relational and health-related demands or expectations within various ecological settings (the home, school, or community). Using RCT as a framework for understanding the narratives of the participants, the findings also helped to elucidate the reasons behind indigenous girls’ perceived difficulty in refusing offers to use substances that were found in earlier studies (Dixon Rayle et al., 2006; Okamoto, Kulis, et al., 2010).
Method
Data from the study came from a multiyear pilot-feasibility study on drug prevention funded by the National Institute on Drug Abuse, in which youths were asked to adapt and/or validate narrative scripts to be used to create culturally grounded drug prevention videos. All research procedures were approved by the Institutional Review Boards at Hawai‘i Pacific University, the University of Hawai‘i at Mānoa, and the State of Hawai‘i Department of Education.
Sampling and Participants
Six middle or intermediate schools and two high schools within two of the three public school complexes on the Island of Hawai‘i participated in the study. The participating schools were located in low-income, rural communities. These communities had populations of less than 50,000 and had a higher percentage of families receiving public assistance compared to the state (Accountability Resource Center Hawai‘i, 2010). The recruitment of participants for the study was conducted in collaboration with school-based research liaisons, who were typically school staff members, such as teachers or school counselors, who had long-standing professional relationships with the university-based research team from a prior multiyear preprevention study. The liaisons assisted in the recruitment of Hawaiian students and responded to the students’ and parents’ questions about the study. They also helped to distribute and collect parental consent forms from the students and secured space within their respective schools for the focus group discussions.
Of the 74 youths who participated, 67% were female, with a mean age of 13.21 years (SD = 2.17). The mean number of youths participating per school was 9.25 (SD = 2.76). The majority of these youths were in the 7th grade (38%), followed by the 8th grade (22%), 12th grade (18%), 6th grade (11%), 11th grade (7%), and the 9th and 10th grades (1% each). In terms of ethnicity, approximately 88% of the youths indicated they were Hawaiian or part-Hawaiian; however, the majority also identified as being of additional ethnocultural groups, such as Chinese (42%), Filipino (54%), Portuguese (49%), and white (41%). Of the youths who indicated they were Hawaiian or part-Hawaiian, 80% indicated that they primarily identified with their Hawaiian background over their other ethnic backgrounds.
Procedures
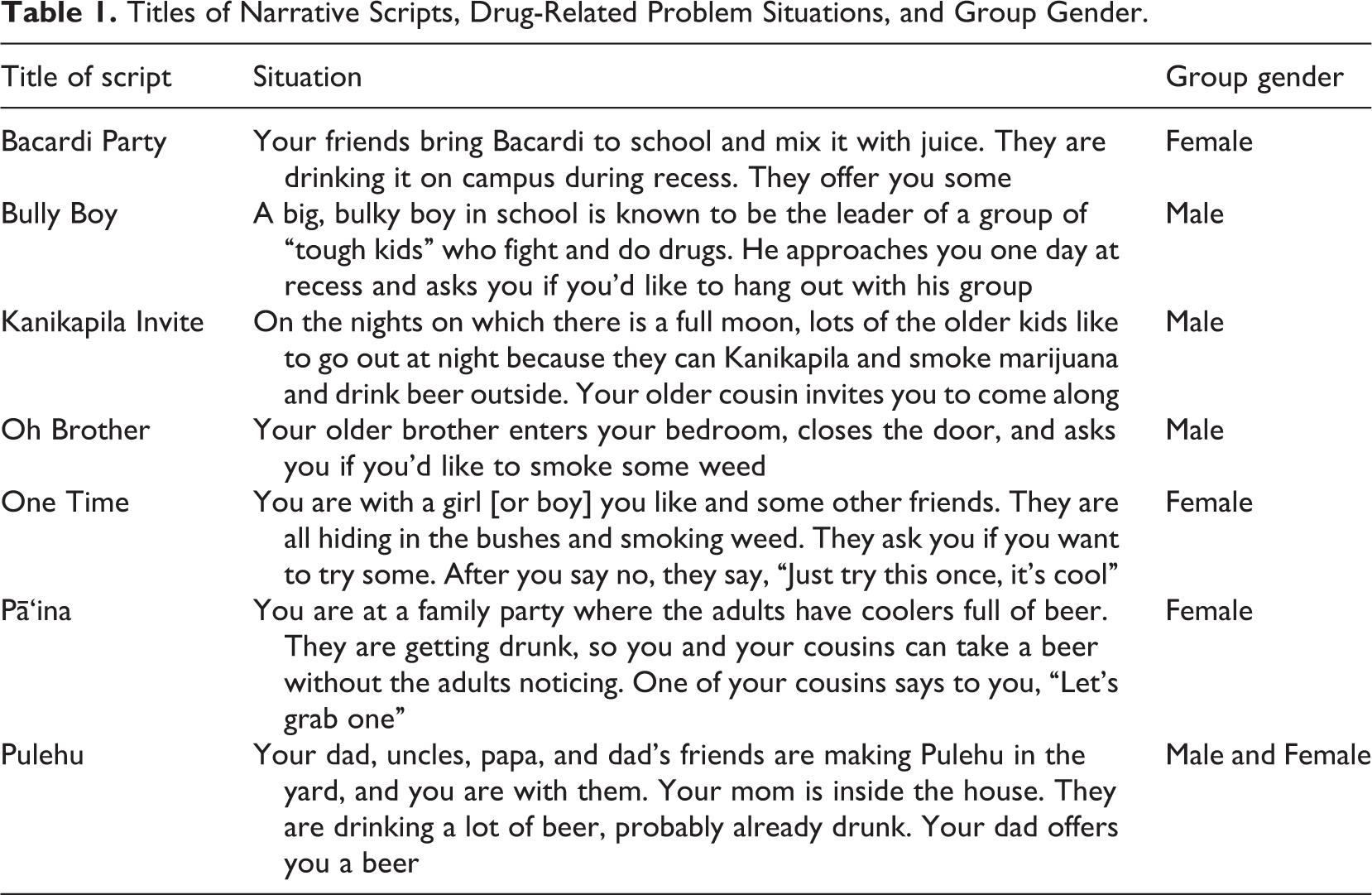
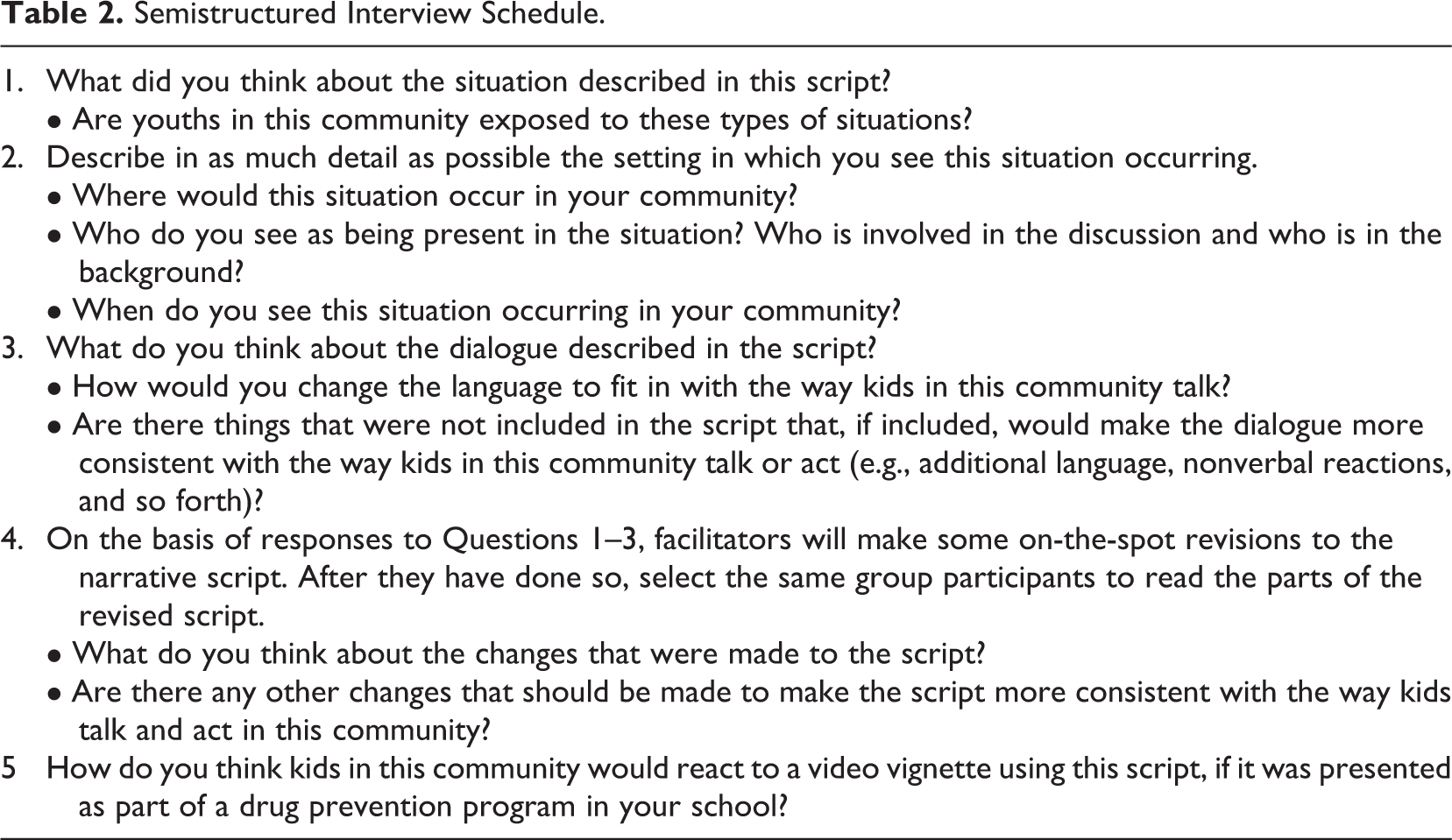
Each youth participated in 1 of the 15 gender-specific focus groups (2–10 youths per group; M = 4.63, SD = 2.33), and the gender of the group facilitators matched that of the participants. The goal of these groups was to adapt and/or validate seven narrative scripts to be used to film culturally grounded drug prevention videos focused on rural Hawaiian youths. Each script outlined a brief vignette based on a drug-related problem situation that was developed and validated in prior research (Okamoto, Helm, Giroux, Edwards, & Kulis, 2010). Table 1 presents the names of the scripts, the associated drug-related problem situations, and the gender composition of the groups that adapted and/or validated each script. Following each situation, each script outlined three different types of responses for refusing drugs, such as avoiding the situation or saying no. The drug-refusal responses corresponding to each scripted situation also had been developed and validated in prior research (Okamoto, Helm, Giroux, & Kaliades, 2011; Okamoto, Helm, Giroux, Kaliades, et al., 2010). The semistructured interview schedule that was used for the focus groups is presented in Table 2. The participants were informed to keep all disclosures in the group setting confidential. Because we audiorecorded the interviews, the youths were asked to use preselected pseudonyms to refer to themselves and others who participated in the group discussions, as well as individuals in their stories.
Titles of Narrative Scripts, Drug-Related Problem Situations, and Group Gender.
Semistructured Interview Schedule.
Data Analysis
All the interviews were audiorecorded and transcribed verbatim by a member of the research team. As an added layer of research protection, the participants’ self-selected pseudonyms were replaced by researcher-selected pseudonyms in the analyzed transcript and disseminated data. To ensure the quality of the data, each transcript was reviewed for accuracy by at least two members of the research team. Following this process, a comprehensive set of open codes (Strauss & Corbin, 1990) was identified by the principal and coprincipal investigators (Okamoto and Helm) and was imported into a qualitative research data analysis program (NVivo, 2010). NVivo is one of several code-based theory-building programs that allow researchers to represent relationships among codes or build higher-order classifications (Weitzman, 2000). To establish intercoder reliability and validity, all members of the research team collectively coded one transcript to clarify the definition and parameters of each of the codes. Then, all subsequent transcripts were separately coded and cross-checked by at least two members of the research team. Narrative segments that were not identically coded by the team members were identified, discussed, and justified for inclusion or exclusion in the data set. As an additional validation check, after all the transcripts were coded and entered into NVivo, the content of conceptually complex codes was again reviewed and validated by the research team, which allowed for further clarification and verification of the content of the codes. Upon establishing intercoder reliability and validity, we conducted an analysis of the changes to the narrative scripts suggested by the participants. Gender differences were systematically examined within each code, including differences in content and the manner in which the male and female participants discussed the drug-related problem situations and their associated responses depicted in each script.
Results
Across all the focus groups, 54% of the narrative content came from the boys’ groups, and 46% came from the girls’ groups. The primary gender differences for the participants were evident in the discussion and/or modification of proposed responses to drug offers described in each script. The boys were more inclined to endorse and/or describe responses that “disconnected” the protagonist in the script from the drug offerer more abruptly (e.g., “[S]he would leave the situation”), while the girls were more inclined to endorse and/or describe methods to stay relationally “connected” in the situation, despite the drug offer (e.g., “Next time,” “not now, maybe later”). As an example of a disconnected response to a drug offer, several boys described how the female youth protagonist in “Pulehu” should react to her father’s offer to drink beer with him. In this script, a 13-year-old girl (Ku‘u) is offered a beer by her father in front of several uncles and a grandfather. The boys compared her actions with how they would behave in this type of situation.
So how would you feel [if your father offered you beer]? Awkward. Uncomfortable. Awkward, uncomfortable. How do you act when you feel uncomfortable? If somebody makes you feel uncomfortable and they ask you to do something, how do you act? I[’d] go in the house. I[’d] walk away. You’d walk away? I[’d] go to my room and play games. How would you react immediately? Would you just look at them and then just turn and walk away? Or, would you. [Interrupts] I just look at somebody else. No, my dad’s really strict, so I would just sit down, but not too close to [him]. And it sounds like you would kinda look away, too; you just said, so you would sit down kind of close to him and look away. So would you say anything, right at that moment? I[’d] say “Dad, I go play games. I go play game[s].”
In contrast to the refusal strategy endorsed by the boys, the girls who validated “Pulehu” felt differently about how Ku‘u should respond to her father’s offer of alcohol. Their suggested responses illustrated concern for the father’s well-being and an attempt to stay relationally connected with him.
OK, so it sounds like all of you guys would be [feeling] some level of discomfort [and] fear [if your father offered you a beer], or I think you said feel[ing] scared, confused, [and] pressured. Empathy. Empathy. OK, so then what do you think Ku‘u should do in this situation? How would she behave in this situation? She would like, tell her dad [uncles, and grandfather] that she doesn’t wanna drink. And that she wanna just listen, like, talk with them instead.
The theme of relational connectedness was also evident in other scripts validated by the girls’ focus groups. For example, in “Pā‘ina,” several girls discussed the merits of two different responses to a drug offer from a cousin—diverting the topic away from drug use by suggesting to the offerer that they go play a game with other cousins (Response 2) or leaving the situation and going inside to watch television (Response 3). “Candy” described how Response 2 would allow her to help her cousin who is offering her alcohol, supporting the importance of staying relationally connected with him as a potential intervention strategy.
So what’s the difference between the second response and the third response? ‘Cause the second response, she[‘s] going to try and [get] them not [to] drink. And, the third response, she’s just going to let them go, and she[’s] not going to know what’s going to happen. Oh, OK. So, [do] you guys follow what Candy’s saying? Explain it [again]. I want to make sure I understand. The second response is better than the third because [in] the third [response], she[’s] just going to leave them outside and she[‘s] not going to know what’s going to happen. And, [in] the second [response], she’s going to help them in not making them drink, and she’s going to help them have fun.
The importance for girls of staying relationally connected in drug resistance also extended to scripts with peers as drug offerers. In “One Time,” a group of older adolescents described how the female youth protagonist (Kiana) should refuse a marijuana offer from a boy whom she just had met and shared a mutual attraction (Eric). The group participants debated whether Kiana should refuse the offer by saying “no thanks, I’m cool.” They debated various responses that conveyed refusal, but also suggested the potential for drug use in the future, so as not to “cut off” the relationship.
I like the “No thanks, I’m cool.” Like, she’s trying to flirt with him at the same time ‘cause she does like him, you know. Like, or “no thanks,” not “I’m cool” but something else. Not “No thanks.” “I’m good.” “I’m fine.” I think what you’re picking up on, Sherrie, is that she does like this boy. So she wants to keep him [around her]. Yeah, keep him there but not like push him away on the side like “No thanks, I’m cool.” So you’re thinking that way is OK. But then the suggestion that you made, you don’t want totally to like kick the guy off the [curb]. But what you said can work if you say it. Yeah, in a different way. You could do something, too, in your voice, if you want. She could be like “Noooo, next time.” Yeah “next time.” ‘Cause then he’ll, he would be like [asking] again. And the next time would be like again, “No, no, next time.” Yeah. She’ll be like “No, no, not right now, next time.” ‘Cause there’s other people there, too. So like. [Interrupts] She doesn’t want, she doesn’t want his friends to be like, “Brah, drop her, man.” [Referring to an extracurricular activity] She could be like “Nah, I gotta practice, you know.”
The data further suggested that the female participants were more aware of and/or concerned about the long-term ramifications of their interactions to their relational networks when they refused drugs. This concern was exemplified by “Pearl’s” statement that Kiana in “One Time” should choose a refusal strategy that would minimize Eric’s friends from pressuring him away from dating her in the future (i.e., “Brah, drop her, man.”). Also demonstrating insight related to the long-term relational impact of drug refusal strategies, the female participants who validated “Bacardi Party” described how responses to drug offers that involved telling an adult authority figure at school about the offer might be construed as “tattletailing” and could eventually lead to a fight among peers. Overall, the girls expressed insights into the impact that specific drug resistance strategies could have on their relationship with the drug offerer, as well as with their relationships with individuals who are in the offerer’s social network.
Some of the more serious and insightful responses in relation to this theme came from the female participants who validated “Pulehu.” These participants expressed an overall concern with how adult family members might perceive Ku‘u’s refusal to drink alcohol with her father.
I would feel pressured because that’s your family, and you don’t want to like [does not finish statement], and it’s with your uncle guys and stuff. [Repeats a little bit louder] I would feel pressured because it’s your dad and your uncle guys. What do you mean by “pressured”? Like maybe, just ‘cause they might find it offensive that you don’t want to drink beer, but they do. And that they think bad about it and stuff.
Later in the group discussion, these participants expressed concern specifically about the impact of one of Ku‘u’s responses to her father’s alcohol offer, in which she yelled to her mother “Look what dad gave me!” The girls in this focus group described how this response might affect her father’s relationship with her mother and subsequently her relationship with her father (Kana).
[Reading the script] So Kana hands her the beer he just cracked open. Ku‘u looks down hesitantly at the beer in her hand, then she looks back toward the house and yells out. Mom, look what dad gave me! And Ku‘u holds up the beer and her [mother walks out and stands] out the door with her hands on her hips. Alright, what do you think about that one? Her dad’s in trouble. Dad’s in trouble. OK. Go ahead Dakota. I was just gonna say that, like, that decision she made could start problems between her mom and her dad, and then she could start getting abused by her dad because we still don’t know what kind of person he is.
Conversely, several of the boys who validated “Pulehu” did not seem to express as much concern about Ku‘u’s response to her father’s alcohol offer. On the surface, they seemed to minimize the impact or extent of the problems that this response might have caused Ku‘u’s family.
OK, so in Response 2, Kana says, “E Ku‘u, relax and have a beer with us.” And then, Kana hands her the beer he just cracked open. Ku‘u looks down hesitantly at the beer in her hand, then she looks back toward the house and yells out, “Mom, look what dad gave me!” Ku‘u holds up the beer. Her Mom steps out the door with her hands on her hips. What do you think about that response? [Laughs] I think that’s very realistic. Oh, you think that is realistic, that it could happen? Yeah. ‘Cause then, you know, mother[‘s] gonna get like mad. Would this cause more problems within the family? No. Yeah. Only with the dad, mom and dad.
Discussion
To elucidate recent findings related to the ecological risk of drug use for indigenous girls (Dixon Rayle et al., 2006; Okamoto, Kulis, et al., 2010), this article examined gender differences in preferred drug resistance strategies for rural Hawaiian youths who participated in a culturally grounded drug prevention pilot-feasibility study. An analysis of the modifications to the narrative scripts described by the participants indicated distinct gender differences and supported the theoretical principles of RCT. Compared with the female participants, the male participants were more likely to endorse drug resistance strategies that relationally disconnected the youth protagonist from the drug offerer in the script. These strategies allowed the protagonist to eliminate the personal risk of substance use in the short term, but eventually might result in adverse relational consequences. Conversely, the female participants appeared to favor resistance strategies that maintained a connection to the drug offerer. They considered the long-term relational consequences of their actions and behaviors and appeared to balance the need to maintain relational and social harmony with the goal of abstinence from drugs.
Although the need for Hawaiian girls to stay relationally connected in the midst of drug-related problem situations is consistent with RCT, it also may account for the perceived difficulty that indigenous girls have expressed in dealing with these situations found in prior research (Dixon Rayle et al., 2006; Okamoto, Kulis, et al., 2010). Developmentally, indigenous preadolescent girls may be more aware of the social and relational consequences of different drug refusal strategies than their male counterparts. Because of this awareness, these girls may not see relational disconnection as an option in drug-related problem situations, since they may perceive it as culturally disrespectful or as leading to problems within their close-knit social network. In some cases, the female participants described how relational connectedness in drug resistance with family members could even function as an intervention strategy, emphasizing the social responsibility that some of these girls felt in preventing the substance use of family members. In any case, the qualitative findings strongly suggested that indigenous girls are compelled to engage in interactions with significant individuals who are offering them drugs, while simultaneously meeting the conflicting goals of maintaining social and relational harmony with these individuals and personally abstaining from drugs. Balancing all these considerations represented an enormous challenge for these girls.
Implications for Indigenous- and Gender-Specific Practices
Examining gender differences in preferred drug resistance strategies has implications for promoting developmentally and culturally appropriate, gender-specific resistance skills training for rural Hawaiian youths. Historically, drug prevention interventions have focused on instrumental means to meet individualistic goals related to abstinence (e.g., “just say no”). Although research on prevention has largely identified these skills as overly simplistic and ineffective (Tobler & Stratton, 1997), they are particularly inappropriate for girls (indigenous or nonindigenous) because they fail to consider the culture- and gender-based relational consequences of these types of responses. The findings of this study suggest that resistance skills that focus solely on meeting individualistic goals to resist drugs (e.g., walking away) may not be appropriate for indigenous girls.
As RCT suggests, drug resistance skills must equally balance the goals of relational connectedness and drug abstinence, particularly for indigenous girls in close-knit rural communities. Furthermore, gender- and indigenous-specific drug prevention strategies may need to be much more contextual and relational in nature and thereby will most likely be highly complex. This is particularly the case for drug offers from adult family members (e.g., parents). For example, an emerging video-based, culturally grounded drug prevention program for rural Hawaiian youths demonstrates how the female protagonist in “Pulehu” (Ku‘u) used a series of verbal and nonverbal interactions with her father and other protective adults to maintain her positive relationship with her father, while simultaneously protecting herself from drinking beer with him (Okamoto, Helm, McClain, & Dinson, 2012). The intent of this approach is to demonstrate how Ku‘u was able to use her culture-based relational networks as protection against substance use. Training in balancing drug abstinence with relational consequences is being developed for a school-based prevention curriculum to be delivered by teachers, but these types of skills have been adapted to other settings (e.g., social service agencies) in prior research (Holleran Steiker, 2008). Drug prevention programs for other populations of indigenous youths may need similarly to reflect realistic gender-specific problem situations and unique ways in which indigenous girls deal effectively with them.
Limitations of the Study
There were several limitations to this study. Because the data came from a pilot-feasibility drug prevention study focused on Native Hawaiian youths on the Island of Hawai‘i, the results may not be transferable to Hawaiian girls on other islands or to indigenous girls on the U.S. Mainland. Furthermore, the topic of drug use can be sensitive, affecting the level of comfort or amount of disclosure in a focus group setting. However, because the focus of these groups was on validating scripts based on hypothetical drug-related problem situations, not on intrusive topics such as past personal substance use, the lack of comfort or disclosure in the group setting for these youths did not appear to be an issue. Finally, because active parental consent was required for all youths who participated in the study, the sample may have been influenced by a selection bias. Youths with more extensive personal or familial histories of substance abuse may not have been granted permission to participate because of their parents’ concern that these histories might be disclosed in the focus groups. As a result, the preferred drug resistance strategies of Hawaiian girls with more extensive histories of drug use may not have been reflected in the youths’ narratives.
Conclusion
Despite these limitations, the study built on prior gender-specific theory and practice by examining the preferred ways in which Hawaiian girls manage offers to use substances by peers and family members. Coupled with the framework of RCT, the findings suggest that drug prevention interventions for Hawaiian youths should target the relational and cultural context (rather than the individual) as a primary focus of the intervention (West, 2005). Future research should examine the relational connectedness of Native Hawaiian girls in drug-related problem situations more closely, including subthemes that may provide more insights into the aspects or nature of relational connectedness with these youths. The findings from this study may have implications for the development of gender-specific drug prevention programs for other populations of indigenous youths, particularly those in rural or reservation communities.
Footnotes
Acknowledgments
The authors acknowledge the support of Matt Yamashita in the development of the video scripts and Ay-Laina Dinson, Jessica Mabanag, and Nicholas Maez in the data collection for the study. A version of this study was presented at the 17th Annual Society for Social Work and Research Conference in San Diego, CA, January 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant R34 DA031306 from the National Institutes of Health, National Institute on Drug Abuse, with supplemental funding from the Trustees’ Scholarly Endeavors Program, Hawai‘i Pacific University.