
Abstract
Objective:
To assess the operational and environmental benefits of using an abbreviated protocol for hepatocellular carcinoma (HCC) surveillance.
Methods:
This IRB-approved retrospective single-center quality improvement study evaluated time, energy use, and appointment access. Inclusion criteria were HCC surveillance MRIs with either a full or abbreviated imaging protocol. Exclusion criteria were other abdominopelvic MR protocols or incomplete studies. DICOM time data were extracted via Quantivly and validated with 10 prospective time studies. Exam times from PACS images were cross-referenced with DICOM data to identify and resolve extraction outliers. Power logs from 10 exams per protocol were used to quantify energy and greenhouse gas emissions. Schedule logs assessed appointment volume changes. Mean times (±SD) and energy (±SD) were reported, and Welch’s t-test determined statistical significance (P < .05).
Results:
Exam times for 487 MRIs (318 abbreviated, 169 full protocol) were analyzed, with 67 excluded. The mean duration of exam time for the abbreviated protocol was 12.0 minutes (SD: 4.3), compared with 29.7 minutes (SD: 8.8) for the full protocol (mean difference, 17.7 minutes; P < .0001). The mean energy for the abbreviated protocol was 4.7 kWh (SD: 0.6), compared with 11.7 kWh (SD: 1.3) for the full protocol (mean difference, 7.0 kWh; P < .0001). Across 318 abbreviated exams, estimated savings totaled 2226 kWh and 1494.6 kg CO2eq. Despite time savings, MRI appointment volume and scanner access remained unchanged.
Conclusion:
Abbreviated HCC surveillance MRIs cut scan time, energy use, and carbon emissions by 60%, but scheduling complexities precluded increased MRI appointments.
Introduction
Hepatocellular carcinoma (HCC) stands out as a primary cause of cancer-related deaths, especially in those with cirrhosis and chronic hepatitis B. 1 Surveillance methods targeting HCC have demonstrated their effectiveness in lowering mortality rates by enabling disease detection at early stages.2,3 Based on this, many expert associations have put forth recommendations for semiannual HCC surveillance using stand-alone abdominal ultrasound, or in conjunction with serum alpha-fetoprotein for patients identified as high-risk.4,5
Although abdominal ultrasound remains the primary surveillance approach, its efficacy can be hindered in situations of poor visualization due to factors such as obesity, nonalcoholic fatty liver disease, and advanced cirrhosis.4-8 For these cases, MRI surveillance proves advantageous, delivering high specificity and sensitivity for the early stage HCC detection.9,10 Yet, barriers remain with using MRI for HCC surveillance including long scan duration, cost, and accessibility. 11
To address these barriers, there is growing interest in HCC surveillance using abbreviated MRI protocols.12,13 These condensed imaging techniques reduce exam duration by eliminating certain sequences, while still maintaining similar sensitivity for early-stage HCC detection.12,13 Given their shorter exam times and equivalent HCC detection rate, patients also prefer abbreviated MRIs over full MRIs, which is an important factor for surveillance compliance. 14 However, what remains unexplored are the operational and environmental benefits of implementing abbreviated protocols over full protocols.
This study aimed to quantitatively assess the time, energy consumption, and greenhouse gas (GHG) emissions associated with full and abbreviated MRI protocols for HCC surveillance, while also evaluating whether the shortened protocol increases MRI appointment daily volumes. By providing these insights, we aim to support institutions in making informed decisions about implementing abbreviated MRI protocols for HCC surveillance.
Material and Methods
This is a HIPAA-compliant institutional review board-approved retrospective single-center quality improvement study. The project was undertaken as an initiative to inform operational and environmental differences for abbreviated versus full MRI protocol for HCC surveillance at a single institution.
Study Cohort
Inclusion criteria were hepatocellular carcinoma screening MRIs performed with extracellular contrast administration at the study institution on adult patients between November 2019 and June 2021. Potentially eligible exams were identified through a comprehensive query of the radiology report database, mPower (Nuance, Burlington Massachusetts). The initial search used Boolean search string logic for hepatocellular carcinoma, liver imaging reporting and data system (LI-RADS), hepatitis B, and cirrhosis.
Exclusion criteria were other abdominopelvic MRI protocols (MRI examinations obtained with an additional magnetic resonance cholangiopancreatography, gadoxetate disdodium contrast-enhanced MRI, MRI examinations that include pelvic imaging), pediatric patients (<18 years-old), or incomplete studies.
All potentially eligible exams were manually reviewed by a single study team member to ensure inclusion and exclusion criteria were met. All radiology reports associated with these examinations were manually reviewed for clinical history and examination protocol accuracy by a faculty abdominal radiologist.
Additional Data
For each eligible exam, additional data was obtained through electronic medical record chart abstraction: patient demographics, body mass index, and primary language. These factors have been shown previously to affect MRI scan time. 15
MRI Protocols
Full MRI Protocol
Full MRI examinations included unenhanced T1-weighted, T2-weighted, and diffusion-weighted sequences as well as dynamic contrast-enhanced T1-weighted sequences according to LI-RADS technical recommendations. 16 Dynamic contrast-enhanced imaging used an axial fat-suppressed three-dimensional T1-weighted gradient-recalled-echo sequence performed during the precontrast, late arterial, portal venous, and delayed phases following a power injection of an extracellular gadolinium-based contrast agent (Gadoterate Meglumine, Dotarem®). The full MRI examinations were performed on at-risk patients for HCC undergoing MRI for the first time or with an indication to work up a lesion identified on a prior study.
Abbreviated MRI Protocol
Abbreviated MRI examinations only included the dynamic MRI sequences and were performed on patients that had previously undergone a full protocol on a prior study for HCC surveillance.
Process Map
A process map was generated to define the steps and associated time intervals involved with abbreviated and full MRI protocols. This was done through 10 prospective observations of the full and abbreviated MRI protocols by a biomedical engineer and radiology faculty. The observations were made at different imaging locations, MRI scanners, and with different performing technologists to observe potential variations that might exist in our MR workflow. The observed times were verified with indirect time estimates from focused interviews with MRI technologists.
The episode of imaging care was defined as the time from which the first sequence was initiated to the time when the last sequence was completed. Non-scan related activities such as checking in, patient clothing change, IV placement, scanner positioning, filling the injector with contrast, removing the patient off the MRI table, removing patient’s IV, and cleaning the room between patients were considered identical between the 2 imaging exams, based on prospective observations and interviews, and excluded from this scope of analysis.
Time Analysis
Total imaging time, active gradient time, and inactive gradient time were extracted from digital imaging and communication in medicine (DICOM) header data using Quantivly (Quantivly Inc, Somerville, Massachusetts), a software platform that analyzes, cleans, and harmonizes DICOM metadata across vendors to build a new unified ontology of imaging operations. Timestamps collected for 10 exams of each protocol during the process mapping work described above were used to internally validate the larger retrospective DICOM data set. Total imaging duration extracted by Quantivly were verified by calculating the difference of the time stamp on the first and last images in the picture archiving and communication system.
Energy Analysis
Energy data was extracted from 3 MRI scanners including Siemens 3T MAGNETOM Vida, GE 3T Signa Premier XT, and Siemens 1.5T MAGNETOM Sola. Power meters at the main electrical disconnect captured continuous real-time power data at a 10 second sampling rate to capture detailed fluctuations in power usage. Data logs were segmented into 10 abbreviated and 10 full protocols for HCC screening, to calculate total exam energy consumption. The energy savings were calculated for the abbreviated protocol.
Imaging Appointments
Daily scheduling logs were evaluated for 10 days each during which abbreviated or full MRI protocols were used. Appointment capacity was assessed based on the assigned MRI time block and the number of MRI slots scheduled for the day. Input from lead schedulers and MRI technologists provided insight into operational workflows and scheduling barriers.
GHG Savings
GHG savings were estimated using the 2022 U.S. average emission rate (0.672 kg CO2/kWh). 17
Statistics
Statistical analysis was performed using Stata software (version 18; StataCorp, College Station, TX, USA). Patient characteristics were summarized with means and standard deviation for continuous variables. Categorical variables were presented as percentages and counts. A Welch’s t-test and chi-square tests were used to compare continuous and categorical patient characteristics, respectively. The primary outcomes were scanning time and energy differences between abbreviated and full HCC protocols. Q-Q test and Shapiro-Wilk test were used to determine distribution of data. A Welch’s t-test was used, given unequal sample sizes and assuming unequal variances. It was applied to test the hypothesis that full and abbreviated-MR protocols have equal means. A P-value <.05 was the cutoff for statistical significance.
Results
The study flow diagram is provided in Figure 1. The initial data query returned 554 examinations. The following studies were subsequently excluded: 59 for protocol not meeting study criteria, 4 with incorrect sequences for protocol, and 4 incomplete studies. This resulted in a final study cohort of 487 exams (318 exams with the abbreviated protocol and 169 exams with the full protocol).
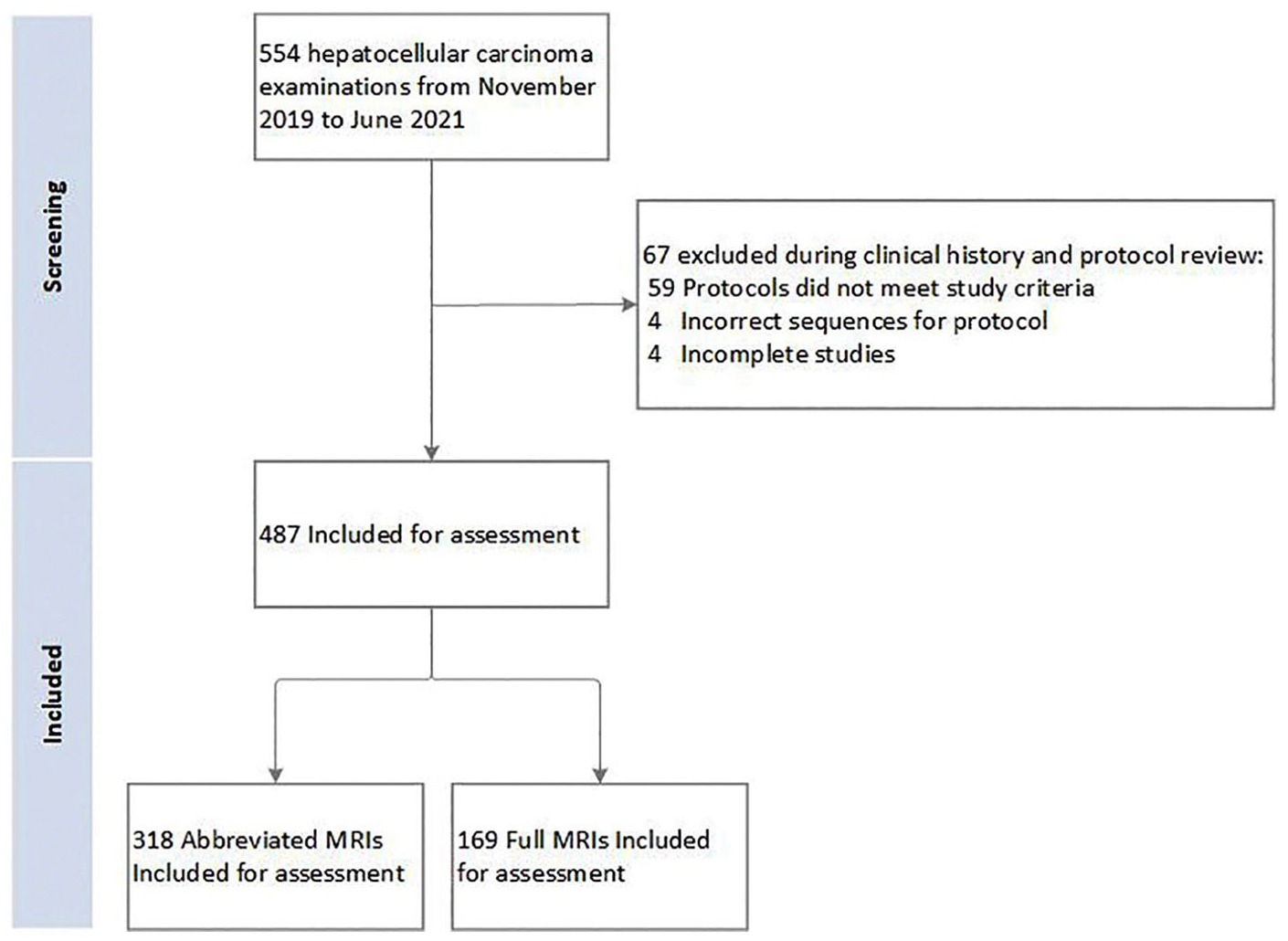
Flow diagram for study inclusion.
Population demographics are summarized in Table 1. The abbreviated protocol had a slightly older population (65 ± 11.4 vs 61 ± 11.5 years; P < .0001) and more males (63% [200/317] vs 52% [86/165]; P = .02) compared to the full protocol. The populations were similar in body mass index (P = .96) and number of patients requiring a translator (P = .97).
Demographics for Patients Undergoing Hepatocellular Carcinoma Surveillance.
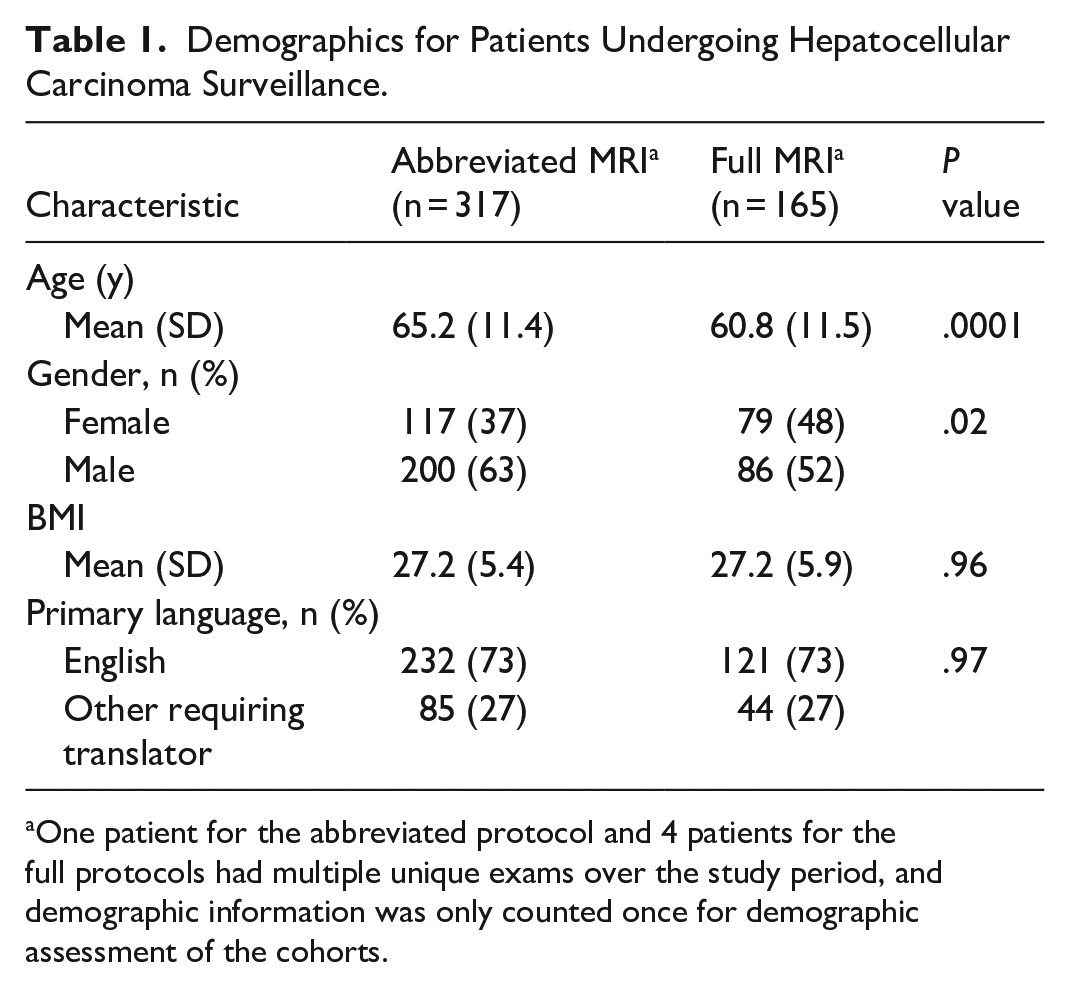
One patient for the abbreviated protocol and 4 patients for the full protocols had multiple unique exams over the study period, and demographic information was only counted once for demographic assessment of the cohorts.
The process map for MRI examinations and protocol times are summarized in Figures 2 and 3. The only difference between the abbreviated and full HCC surveillance MRIs was the scan times. Scan time results are shown in Figure 4 and summarized in Table 2. The data was normally distributed. The total scan time (mean ± SD) for the abbreviated MRI protocol was 12.0 ± 4.3 minutes, compared with 29.7 ± 8.8 minutes for the full protocol (difference, 17.7 minutes; P < .0001). The active gradient time for the abbreviated protocol was 5.4 ± 2.8 minutes, compared with 13.5 ± 5.1 minutes for the full protocol (difference: 8.1 minutes, P < .0001). The inactive gradient times for the abbreviated protocol was 6.6 ± 3.7 minutes, compared with 16.2 ± 6.1 minutes for the full protocol (difference 10.8 minutes, P < .0001).
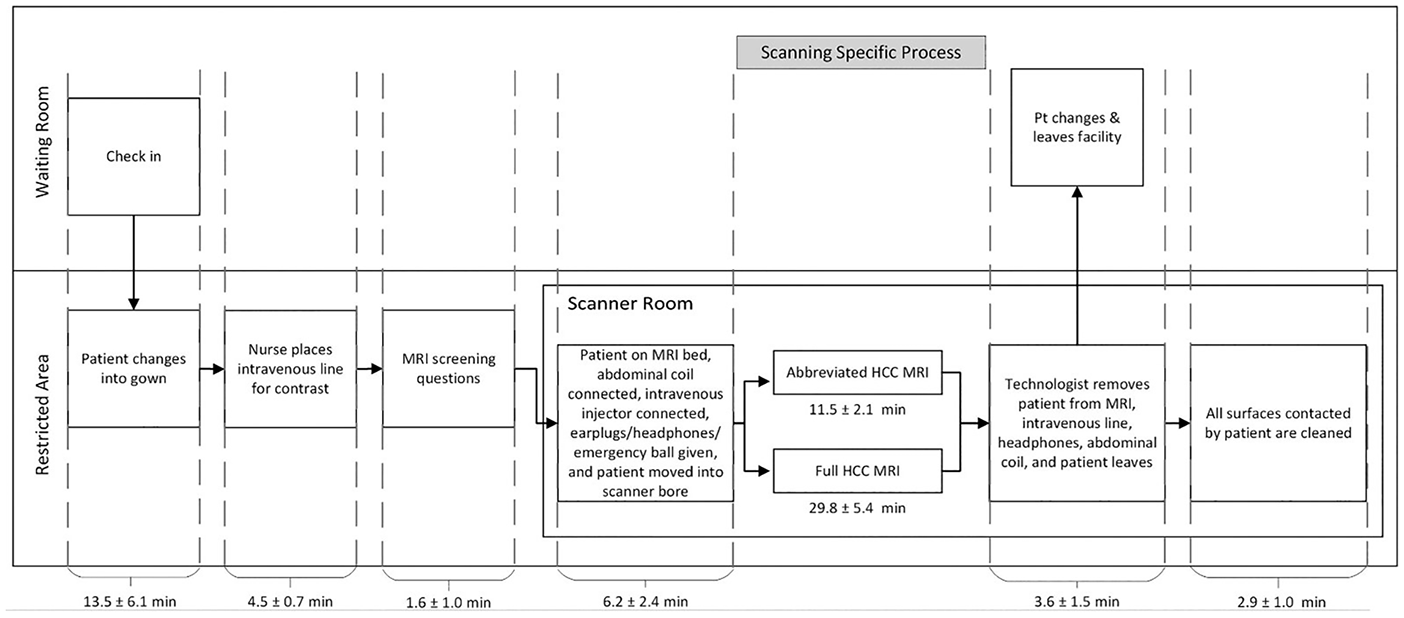
Radiology department MRI process map for full and abbreviated HCC protocols.
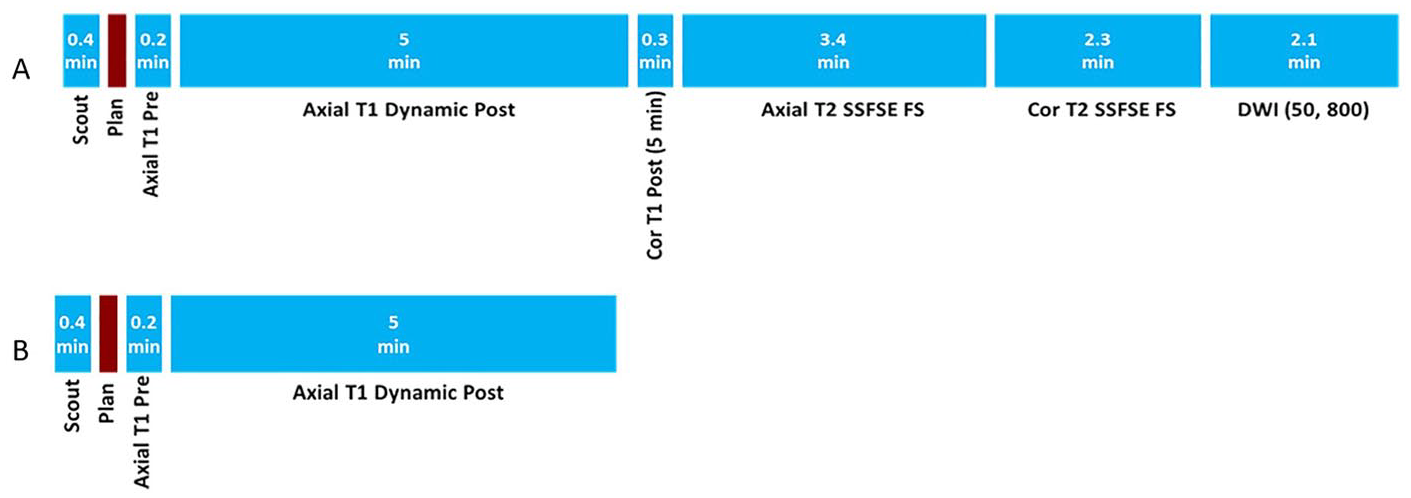
Scan times for each sequence in the full (A) and abbreviated (B) MRI protocols for hepatocellular screening. The expected scan times for sequences were 13.7 and 5.6 minutes. Planned MRI protocols do not include the time in between sequences.
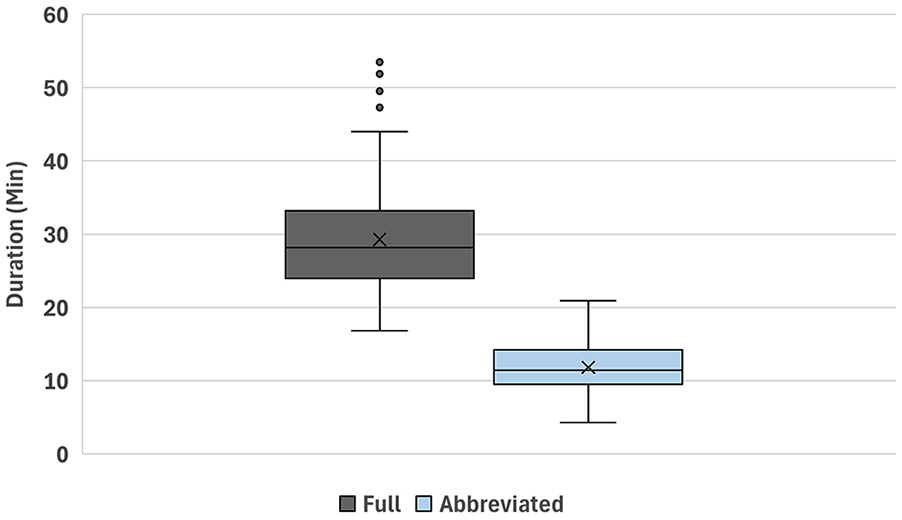
Total scan time for all included full and abbreviated protocols. Box and whisker plot illustrating total scan time for the full protocol (dark gray) and abbreviated protocol (light blue). The boxes represent the interquartile range, the black horizontal line in the box indicates the median value, the x value in the box represents the mean, and the black vertical whisker lines signify the lower and upper 25%. Values outside of the whiskers represent outlier values.
Scan Times for Abbreviated and Full HCC Examinations.

Figure 5 illustrates energy consumption for abbreviated and full-protocol MRI exams and Supplemental Table 1 details the corresponding measurements. The data was normally distributed. The mean energy usage was 4.7 ± 0.6 kWh for the abbreviated protocol and 11.7 ± 1.3 kWh for the full protocol (difference, 7.0 kWh; P < .0001). The estimated carbon emission savings per MRI for the abbreviated protocol was 4.7 kg CO2eq, while the total impact of 318 abbreviated protocols resulted in total estimated savings of 2226 kWh and 1495 kg CO2eq.
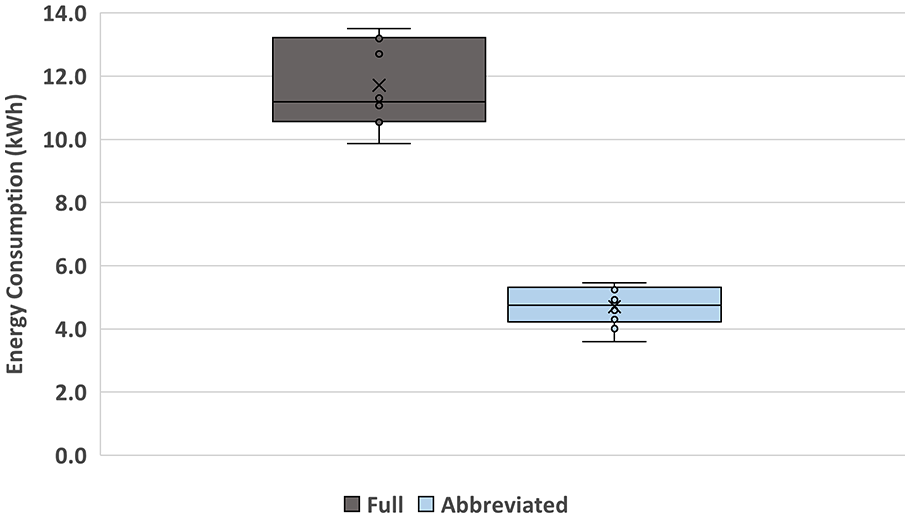
Energy consumption for full and abbreviated protocols. Box and whisker plot illustrating total energy for the full protocol (dark gray) and abbreviated protocol (light blue). The boxes represent the interquartile range, the black horizontal line in the box indicates the median value, the x value in the box represents the mean, and the black vertical whisker lines signify the lower and upper 25%. Values outside of the whiskers represent outlier values.
Analysis of appointment access showed no increase in the number of scheduled appointments on days when abbreviated protocols were used. This was primarily because abbreviated and full exams were assigned the same time blocks on the schedule. Scheduling constraints stemmed from limitations in the ordering and workflow processes: referring providers used a single order for MRI abdomen, and protocol selection—whether abbreviated or full—was typically made by the radiologist after the appointment was already scheduled. Consequently, shorter time slots for abbreviated exams were not utilized, and no gains in throughput were realized.
Discussion
Abbreviated MRI has shown promising results for HCC detection,12,13 yet data on its benefits remain limited. This retrospective, single-center study assessed the time and environmental savings of abbreviated versus full HCC screening protocols, as well as their effect on MRI appointment availability. Abbreviated MRI reduced total scan time by 17.7 minutes, leading to per-exam savings of 7.0 kWh and 4.7 kg CO2eq, with estimated cumulative study-period savings of 2226 kWh and 1495 kg CO2eq. However, these efficiency gains did not translate into increased appointment availability, as MRI slots were booked before protocol selection, and the same order was used for both exam types. While these findings highlight the time and environmental benefits of abbreviated MRIs, they also emphasize the need for optimized scheduling systems to effectively implement protocol modifications that enhance scanner access and patient throughput.
The analysis showed that time saved with abbreviated protocols did not translate into increased scheduled exams. This outcome contrasts with the initial goal of using shorter protocols to expand MRI access. Daily appointment capacity was constrained by operational and system-level barriers: referring providers placed a single MRI abdomen order, and protocol selection—whether abbreviated or full—typically occurred after the appointment had been scheduled. As a result, shorter time slots could not be assigned, and both protocols were booked into the same standard time blocks. These workflow limitations underscore the need for coordinated scheduling strategies that integrate protocol-specific information prior to scheduling.
To fully capitalize on the efficiency gains of abbreviated imaging, strategic scheduling that integrates exams of varying lengths is essential for optimizing scanner utilization. However, such an approach may face challenges in balancing patient scheduling preferences and managing scheduler workload. Future applications of artificial intelligence could streamline these complex scheduling processes, ultimately increasing imaging appointments, accommodating individual patient needs, and reducing the strain on scheduling staff. Prior studies have identified radiology scheduling as a promising area for artificial intelligence-driven interventions, with potential to integrate scanner-specific characteristics, protocol types, risks of delays, no-show likelihood, and safety considerations (eg, contrast use, implants) into scheduling decisions.18,19 These tools may enable protocol-specific time slot allocation and intelligent triage based on clinical indications—ultimately increasing imaging access.
Our study also found that the actual MRI study time considerably exceeded the expected durations derived from the scanner protocols. The activities between sequences constituted over half of the total scan time. Given that abbreviated protocols have reduced intersequence durations, the time saved was more significant than estimates based solely on sequence durations. This unused “dead time” presents a valuable opportunity to enhance both time and energy efficiency and underscores the need for a comprehensive time analysis when determining MRI appointment length and evaluating the benefits of abbreviated protocols.
The energy analysis demonstrated that the 60% reduction in scan time directly corresponded to decreases in energy consumption and GHG emissions. While the primary goal of shorter MRI exams is to enhance scanner availability amid growing healthcare demand, this finding reinforces their additional benefit in reducing environmental impact and electricity per patient. However, any protocol modifications must be carefully coordinated with radiologists to ensure efficiency gains do not compromise diagnostic quality or interpretive confidence.
To our knowledge, no prior studies have performed a time and energy study to assess the benefits of using abbreviated protocols for HCC surveillance. However, several studies have evaluated the time savings of abbreviated protocols.20-23 These studies in general found a time savings between 8 and 20 minutes for abbreviated MRCP, breast MR, and cardiac MR compared to the full protocols.20-24 One study assessed the time and environmental benefits of an abbreviated cardiac MRI protocol, reporting savings of 8 minutes, 3.3 kWh, and 1.4 kg CO2eq. 24 However, unlike previous studies, our research evaluated the time, environmental, and imaging appointment differences of abbreviated versus full HCC screening protocols.
Though not assessed in this study, abbreviated MRI for HCC detection has been extensively evaluated in prior literature, including systematic reviews and multicenter studies.12,13,25,26 A meta-analysis by Kim et al including 7 studies with 1830 patients reported a pooled sensitivity and specificity of 87% (80%-94%) and 94% (90%-98%) for an abbreviated protocol, comparable to full protocols 84% (76%-91%) and 94% (89%-99%). 13 A meta-analysis by Gupta et al including 15 studies with 2807 patients found a pooled sensitivity and specificity of 86% (84%-88%) and 94% (91%-96%) for abbreviated protocols. 12 A more recent meta-analysis by Maung et al reported a pooled sensitivity and specificity of 88% (84%-91%) and 94% (90%-96%) for 15 studies with contrast-enhanced abbreviated MRI. 25 Finally, A well-designed multicenter study by Yokoo et al across 3 institutions evaluated dynamic contrast-enhanced abbreviated MRI in 161 patients with early-stage HCC confirmed by surgical pathology, reporting a sensitivity of 88.2% (83.5-92.5) and a specificity of 89.1% (84.4-93.8). 26
Our study has limitations. This was a single center retrospective study, and time and energy savings could be changed based on differences of MRI protocol. Secondly, the study did not randomize for patient or MRI related factors that can affect imaging times. However, known factors such as BMI and patients requiring a translator were similar between the 2 protocols. Thirdly, our energy estimates isolated MRI native functions, excluding energy for chilled water cooling. Fourth, environmental modeling was based on mean energy data from 3 MRI machines but did not account for the specific energy consumption of each device, which may vary slightly based on technical specifications. Fifth, U.S. energy carbon savings were estimated using national averages, which may not precisely represent local energy mixes, potentially affecting estimates. Sixth, intersequence activities and total scan times could vary by technologist workflow. However, this variability is captured in the total scan time and inactive gradient standard deviations. Lastly, while our environmental findings are broadly applicable, operational outcomes such as scanner throughput and appointment scheduling may differ across institutions based on scanner availability, patient mix, and local workflow practices.
In conclusion, the analysis presented here reveals the time, energy, and GHG savings associated with implementing an abbreviated HCC protocol while highlighting the challenges of increasing MRI appointment availability for shortened protocols. Optimizing scheduling strategies and aligning operational workflows will be essential to fully realize the clinical access goal of shortening protocols.
Supplemental Material
sj-docx-1-caj-10.1177_08465371251371567 – Supplemental material for Hepatocellular Carcinoma Surveillance: Operational and Environmental Impact of Abbreviated MRI Protocols
Supplemental material, sj-docx-1-caj-10.1177_08465371251371567 for Hepatocellular Carcinoma Surveillance: Operational and Environmental Impact of Abbreviated MRI Protocols by Sean A. Woolen, Fayyaz Ahamed, Robert D. MacDougall, Benoit Scherrer, Marc D. Kohli, Alastair Martin, Shuting Dai, Prasad Shankar and Zhen J. Wang in Canadian Association of Radiologists Journal
Footnotes
Abbreviations
DICOM Digital Imaging and Communications in Medicine
GHG Greenhouse Gas
HCC Hepatocellular Carcinoma
LI-RADS Liver Imaging Reporting and Data System
MRI Magnetic Resonance Imaging
Author Contributions
All authors met the ICMJE four criteria for authorship.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SAW supported by funding from RSNA Emerging Issues Grant.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors of this manuscript declare relationships with the following companies: Sean Woolen and Alastair Martin report grants from Siemens Healthineers not related to this study. Robert MacDougall and Benoit Scherrer report employment with Quantively Inc. Marc Kohli reports consultation, advisory, and equity/stocks with Alara. Zhen J Wang reports equity or stocks with Nextrast. Additional authors of this manuscript declare no relationships with any companies.
Data Availability Statement
All data generated or analyzed during the study are included in the published paper.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.