
Abstract
The Canadian Association of Radiologists (CAR) metabolic dysfunction-associated steatotic liver disease (MASLD) Working Group (WG) is a multidisciplinary working group composed of radiologists, hepatologists, and family physicians. In this 3-part series, we provide Delphi consensus-based guidance on clinical and imaging findings for patients with known or suspected MASLD (formerly termed nonalcoholic fatty liver disease or NAFLD). Part 1 focuses on the detection and grading of hepatic steatosis on imaging; Part 2 on risk stratification of patients with MASLD, including a patient pathway that applies blood-based and imaging-based investigations; and Part 3 on the implementation of practice recommendations for quality assurance using shear wave elastography (SWE) and magnetic resonance elastography (MRE) for disease staging. In the third part of these guidelines, the WG provides 18 recommendations for standardized implementation, remuneration, and quality assurance for SWE and MRE programs. Structured reporting templates for standardized SWE and MRE are provided. Introductory training presentations for technologists and radiologists are also provided. The goal of these guidelines is to enable standardized image-based screening and risk stratification of patients with MASLD across Canada.
Background
The Canadian Association of Radiologists (CAR) metabolic dysfunction-associated steatotic liver disease (MASLD) Working Group (WG) was established in 2024 through the Canadian Society of Abdominal Radiologists (CSAR) and is composed of radiologists, hepatologists, family physicians, a radiology trainee, and an ultrasound technologist from across Canada. The WG was convened to provide unified practice recommendations in patients with MASLD. The WG developed a 3-part comprehensive set of guidance recommendations. Part 1 focuses on the detection and grading of hepatic steatosis on imaging; Part 2 on risk stratification of patients with MASLD, including a patient pathway using serological and imaging investigations; and Part 3 on the implementation of practice recommendations for quality assurance using shear wave elastography (SWE) and magnetic resonance elastography (MRE) programs. Background details and methodology for the CAR MASLD WG in addition to a list of 17 guidance statements for imaging detection and multi-modality grading of hepatic steatosis are described in Part 1. 1 Another 14 recommendations for risk stratifying patients with MASLD using blood-based and image-based investigations including a recommended algorithm for population level screening in Canada are provided in Part 2. 2
Techniques for risk-stratifying MASLD patients with blood-based investigations and vibration-controlled transient elastography (TE) have been used, evaluated and improved upon for more than 2 decades. 3 By contrast, the use of medical imaging techniques such as shear wave elastography (SWE) and magnetic resonance elastography (MRE) are more recent innovations with ongoing adoption across many practices in North America. The accuracy of SWE, including both point SWE (pSWE) and 2-dimensional SWE (2D-SWE) have been primarily compared against TE given the more robust literature available for TE in MASLD patients. 4 The optimal image-based evaluation of liver stiffness as a surrogate for hepatic fibrosis continues to evolve with increased clinical adoption and research.
Recently, both American and European clinical practice guidelines have recommended SWE as a surrogate for TE in their risk stratification pathways.5-7 In these guidelines, unified, modality, and vendor agnostic thresholds have been proposed for SWE and MRE. The indications and thresholds for MRE have been guideline dependent. In Part 2 of our guidelines, the CAR MASLD WG has recognized clear benefits but also potential challenges for a unified threshold across multiple modalities and vendors, particularly as the literature continues to evolve for SWE and MRE. 2 Potential challenges such as variability amongst vendors has been more clearly addressed by the Society of Radiologists in Ultrasound (SRU) which recommend more conservative values for ruling-in and ruling-out disease when using SWE. 8 Nonetheless, optimized imaging quality across modalities and vendors is necessary to ensure reliability and reduced variability of results when using the current unified approach. To achieve high quality and reliability with SWE and MRE, attention to excellent acquisition techniques and standardized reporting practices are needed. Part 3 of these guidelines addresses this need by offering recommendations for standardized program implementation, quality assurance practices, and imaging remuneration for SWE and MRE.
Part 3: SWE and MRE Program Implementation and Quality Assurance
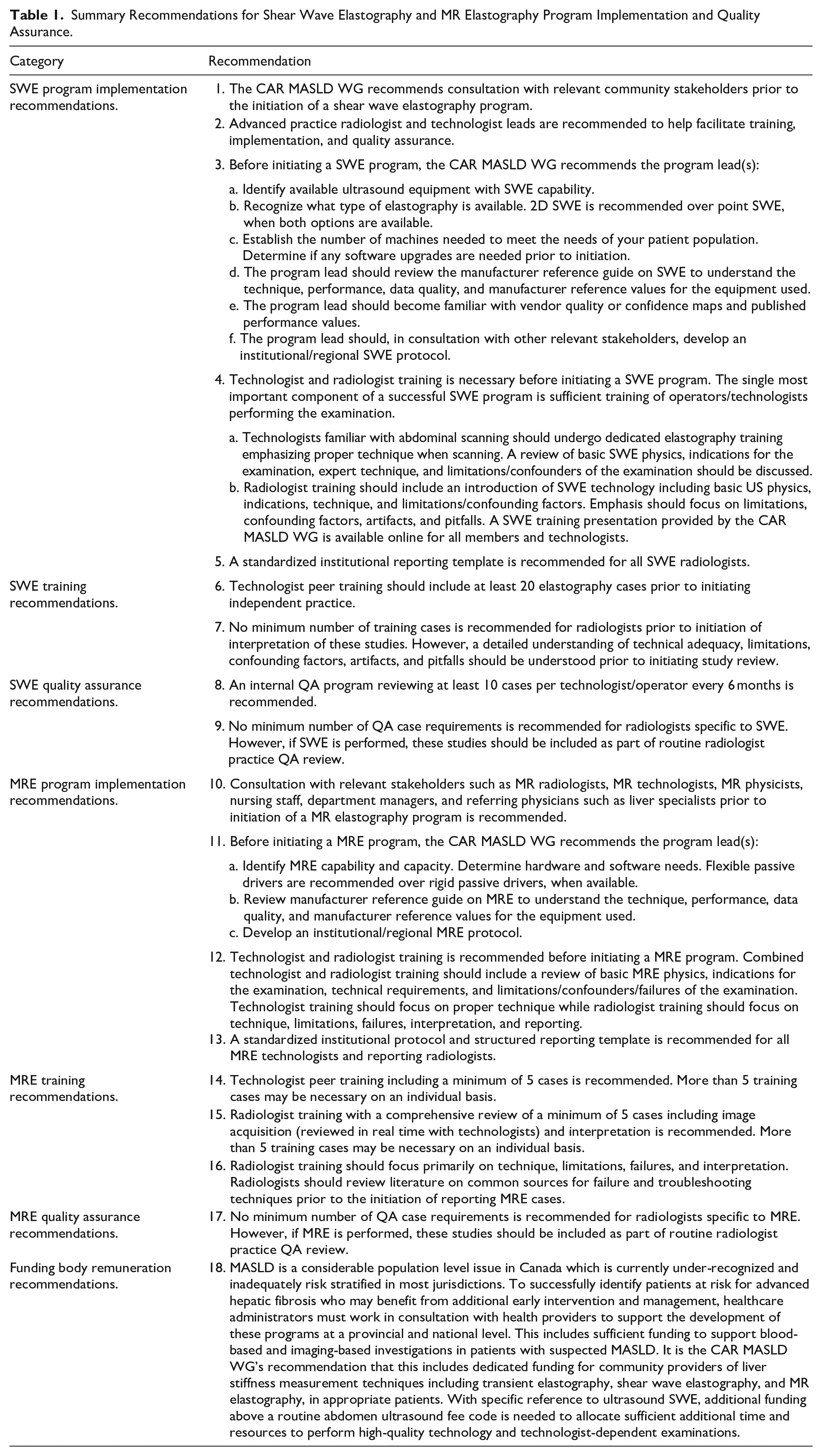
A multi-round Delphi methodology using a 5-point Likert scale with consensus threshold established as a score of ≥4.0 by ≥60% of the WG was used and is explained in further detail in Part 1. 1 Through this process, a list of 18 recommendations for SWE and MRE program implementation and quality assurance are shown in Table 1. Of these, 9 recommendations address SWE (4 for program implementation, 2 for technologist and radiologist training, and 2 for quality assurance), 8 recommendations address MRE (5 for program implementation, 3 for technologist and radiologist training, and 1 for quality assurance), and 1 recommendation addresses funding body remuneration.
Summary Recommendations for Shear Wave Elastography and MR Elastography Program Implementation and Quality Assurance.
While the overarching objective of these guidelines are to provide a comprehensive set of recommendations for imaging-based detection, screening, and risk stratification of patients with MASLD, the WG recognizes that SWE and MRE program implementation may be gradual and stepwise depending on multiple factors. These include physicians and technologists expertise, technology availability, funding models, and more. Most recommendations in Part 3 are aimed at programs which are in the process of or have recently implemented new SWE and/or MRE programs. Additional recommendations on quality assurance and remuneration are aimed at all practices regardless of program maturity.
Part 3A: SWE Program Implementation Recommendations
Rationale: The capacity to develop a SWE program depends not only on equipment availability but also on regional demand, cost, training capacity, technical expertise, and booking availability. To define the internal capacity for implementation, community and hospital providers developing SWE programs are encouraged to consult with their relevant community stakeholders including primary care providers and referral specialists to establish achievable program goals and regional screening pathways before program implementation. Establishing relationships between referral specialists and imaging centers can facilitate connections and improve program feedback as well as quality assurance. As noted, while the CAR MASLD WG endorses a target screening program for all patients with suspected MASLD, institutional program resources should be considered before the development of program-specific approaches. Finally, most ultrasound vendors now offer SWE as an add-on software option with capable machines so it may be prudent to confirm SWE compatibility with new equipment purchases, even if SWE is not initially utilized. This can simplify program implementation and reduce upfront costs with only a one-time SWE software purchase rather than repeat equipment hardware purchases.
Rationale: Nearly 50 recommendations are provided across 3 parts of the CAR MASLD guidelines. These guidelines are specific to MASLD and do not address other potential patient populations for which SWE may be indicated such as chronic viral hepatitis. 8 A lead radiologist, with a detailed understanding of liver disease, SWE, and other imaging-based technologies including technical differences between modalities and individual vendor parameters, and guideline recommendations, is advised. This radiologist can facilitate consultation with relevant stakeholders, discussions with the vendor(s) and guide training, implementation, and quality assurance within a given program or institution.
The acquisition of SWE is technique- and operator-dependent and necessitates detailed standardization across the program.9,10 Having a small group of experienced technologists familiar with abdominal scanning and SWE who can serve to train and evaluate less experienced technologists across the program can also improve overall program quality and address many knowledge gaps often experienced by new operators of the SWE technique.
a. Identify available ultrasound equipment with SWE capability.
b. Recognize what type of elastography is available. 2D SWE is recommended over point SWE, when both options are available.
c. Establish the number of machines needed to meet the needs of your patient population. Determine if any software upgrades are needed prior to initiation.
d. The program lead should review the manufacturer reference guide on SWE to understand the technique, performance, data quality, and manufacturer reference values for the equipment used.
e. The program lead should become familiar with vendor quality or confidence maps and published performance values.
f. The program lead should, in consultation with other relevant stakeholders, develop an institutional/regional SWE protocol.
Rationale: With support of relevant stakeholders including primary care providers and referring specialists, the potential volume demand for SWE is large when considering population-level MASLD screening. Radiologist leads should first define the capacity of their program including the number of ultrasound machines and probes capable of performing SWE, the availability of trainable technologists and determine the available bookings in their practice to reach the program-specific goals and target patient populations/indications. As the program matures, increasing indications may be appropriate depending on regional needs.
When both options are available, the CAR MASLD WG recommends 2D-SWE over pSWE as it can evaluate a larger region of interest and requires a smaller number of repeated measurements. Lead radiologists should have a detailed understanding of their vendor(s) reference guides, performance data, and confidence maps where offered. A standardized institutional/regional SWE protocol is advised to support uniformity across performing technologists and radiologists.
a. Technologists familiar with abdominal scanning should undergo dedicated elastography training emphasizing proper technique when scanning. A review of basic SWE physics, indications for the examination, expert technique, and limitations/confounders of the examination should be discussed.
b. Radiologist training should include an introduction of SWE technology including basic US physics, indications, technique, and limitations/confounding factors. Emphasis should focus on limitations, confounding factors, artifacts, and pitfalls. A SWE training presentation provided by the CAR MASLD WG is available online for all members and technologists (Appendix A).
Rationale: An essential component of a successful SWE program is adequate technique by the performing technologists and radiologists. To achieve this, operators and reporting radiologists should be familiar with abdominal imaging, have a basic understanding of the physical properties underpinning the technology, indications for the examination, technical details of how to perform the exam with high quality and reliability, and limitations and/or confounders which may artificially alter liver stiffness measurement. Some vendors may offer details regarding the quality and reliability of individual measurements, however, the WG supports current SRU recommendations 8 of a combined IQR/median ≤30% for kPa values and ≤15% for m/s, as the single most important measure of reliability. To assist in achieving basic technologist competency in addition to hands-on training, potential sources of education for technologists can include direct training offered by the lead radiologist, education from an on-site applications representative, and/or peer training by experienced SWE technologists. Radiologists should understand how to apply specific reporting patterns detailed in Part 2 of the guidelines, dependent on the presence and scoring of pre-existing FIB-4 results. Radiologists should have a detailed understanding of potential confounders and/or pitfalls which may cause unreliable results.
To supplement the understanding of these underlying principles for technologists and radiologists, an introductory training presentation on SWE provided by the CAR MASLD WG can be accessed online as Appendix A.
Rationale: The CAR MASLD WG recommends standardized template reporting for SWE studies. At a minimum, reports should include a description of pertinent morphological findings in the liver, number of SWE acquisitions, median elasticity/liver stiffness measurement (in kilopascals), IQR/median, and any other potentially significant findings. Additional included template details should be standardized by institutional/regional practice. Interpretation of liver stiffness measurements should be dependent on the provided history and patient population/exam indications outlined in Part 2.
A standardized SWE reporting template developed by the CAR MASLD WG is provided in Figure 1.
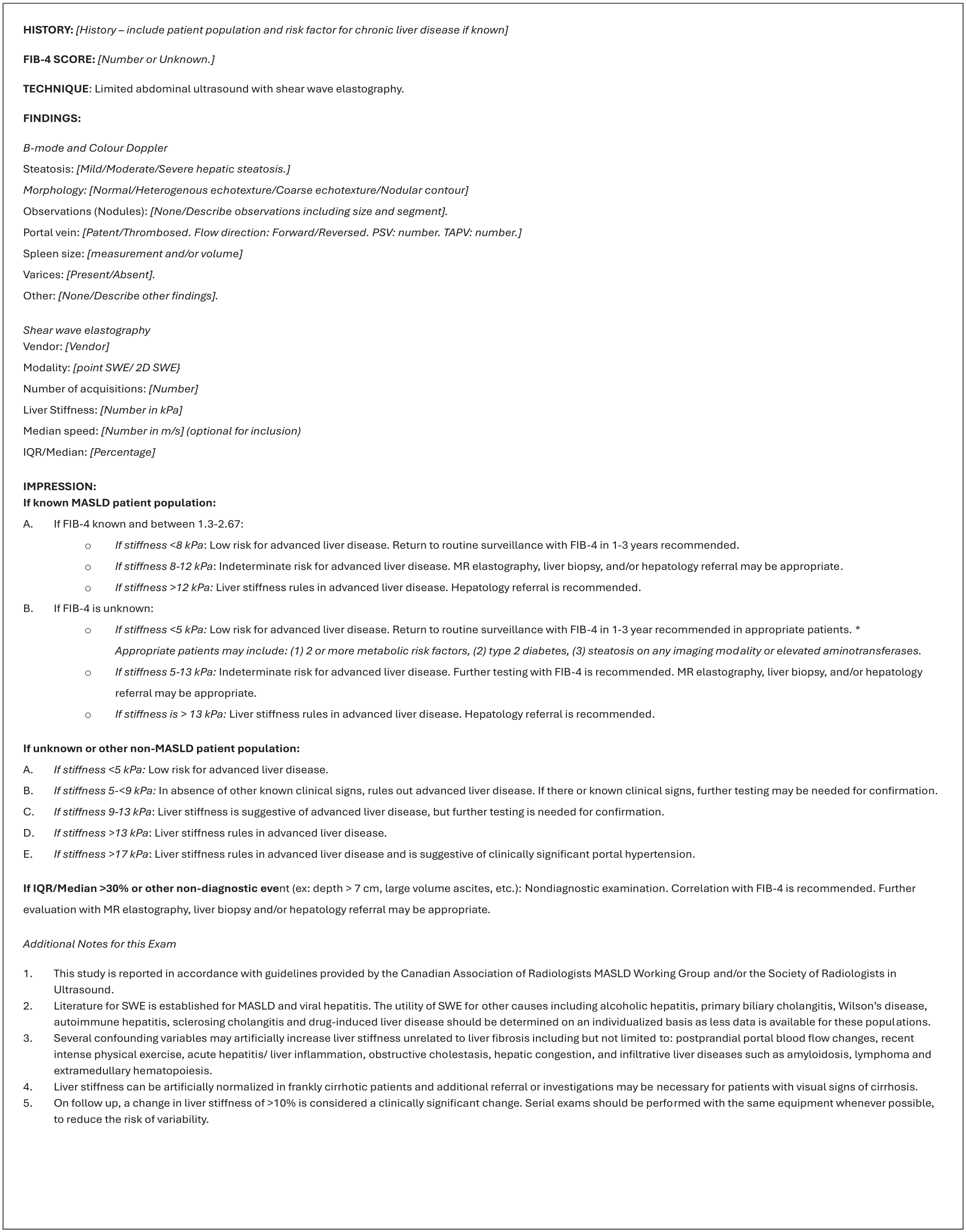
Standardized shear wave elastography structured reporting template example.
Part 3B: SWE Training Recommendations
Rationale: Balancing the need for a practical minimum training requirement at most institutions against the recognition that the single most important component of a successful SWE program is adequate technical training of the technologist/operator, the CAR MASLD WG recommends training with a minimum of 20 elastography cases under direct peer review or supervision prior to independent acquisition.
An initial literature search was performed by 2 authors (EP, SC) to identify existing recommendations for a minimum number of training cases for both technologists and radiologists performing SWE. A single recommendation by the European Federation for Ultrasound in Medicine and Biology (EFUMB) was identified, offering no clear agreement on experience requirements for pSWE or 2D-SWE but referencing proposed definitions for 2D-SWE including performance of >300 abdominal ultrasounds or >50 2D-SWE cases.9-11 These proposed definitions are experience- rather than evidence-based by authors of individual studies. A survey of abdominal radiologists (n = 7) and technologists (n = 35) performing SWE at a single Canadian academic institution was then performed and identified 5 technologist cases and 0 to 5 radiologist cases as the suggested minimum. Most technologists felt a minimum of 2 to 10 studies were needed to develop necessary basic technical skills (mean = 5). Our WG expert SWE technologist favors a minimum of 20 cases to achieve technical competence in their practice. There was variability amongst minimum training requirements currently required across institutions in our WG including a minimum recommendation as high as 50 supervised studies. Based on this variance across programs, a consensus recommendation of 20 training cases for technologists provides a balance between required technical expertise and pragmatic challenges of training.
In addition to a minimum number of training cases, surveyed technologists suggested a minimum of 1 to 2 SWE studies per week to maintain competency. While the CAR MASLD WG does not provide a recommended minimum number of annual cases for technologists, a minimum of 50 cases per year per technologist may be reasonable to maintain volume and confidence in technique and practical skills. This should be determined on an individualized basis and monitored by a lead radiologist within a quality assurance (QA) program.
Rationale: The survey discussed in recommendation #6 identified a recommended minimum of 0 to 5 training cases for reporting radiologists. In the absence of a need for technical skill development, and more important than a minimum number of training cases, a detailed understanding of the underlying technical details and pitfalls of SWE is necessary. These minimum standards of competency are detailed in recommendation #4 and include basic SWE physics, technical adequacy, limitations, confounding factors, artifacts, and potential pitfalls of SWE. Many of these recommendations are further outlined in Part 2. 2 As noted in recommendation #4, a supplemental introductory training presentation on SWE can be accessed online as Appendix A. However, if radiologists are serving as the primary operator for SWE acquisition, a minimum of 20 training cases is recommended in accordance with recommendation #6.
Part 3C: SWE Quality Assurance Recommendations
Rationale: Recognizing that the single most important feature for a successful program is technologist/operator technique and that a minimum number of cases is needed to maintain competency, the CAR MASLD WG advises that a minimum of 10 cases be formally reviewed as part of a QA program for technologists every 6 months to prevent deviation of individual operator standards. Potential barriers to the adoption of a QA program include potential practice specific limitations, particularly time demands of technologists and radiologists. The WG supports a peer-to-peer technologist driven QA program, preferentially led by a small group of experienced technologists, as an alternative to direct review of cases from the lead radiologist.
Rationale: No specific number of cases is identified as necessary for QA review for supervising radiologists although SWE should be included as part of the routine QA program available through the radiologists’ program and/or institution. Particular attention to potential pitfalls or confounders which may result in unreliable reported results is recommended in a radiologist QA program.
Part 3D: MRE Program Implementation Recommendations
Rationale: Engagement from relevant parties such as MR radiologists, MR technologists, MR physicists, nursing staff, department managers, and referring clinicians such as hepatologists is essential in establishing the foundation for a successful and reliable referral program for MRE. Establishing capacity limits, practice specific indications, reporting standards and expected turnaround times should be performed in consultation with referring providers, regional specialists, and department managers. Defining and establishing acceptable standards for image acquisition and reporting can be developed in agreement with practice MR technologists, radiologists, and physicists.
a. Identify MRE capability and capacity. Determine hardware and software needs. Flexible passive drivers are recommended over rigid passive drivers, when available.
b. Review manufacturer reference guide on MRE to understand the technique, performance, data quality, and manufacturer reference values for the equipment used.
c. Develop an institutional/regional MRE protocol.
Rationale: MRE accessibility is dependent on the availability of software, hardware, training, and magnet scan time. Part 2 of these guidelines identifies 4 indications for MRE with the potential for centralized referrals of patients with MASLD and indeterminate risk stratification (FIB-4 between 1.3 and 2.67 and liver stiffness measurement between 8 and 12 kPa). The appropriateness of these indications should be determined on a program/institution specific basis depending on MR availability. When available, newer flexible passive drivers are recommended to reduce the risk of failed MR exams, particularly in thin and small patients, including children, as these malleable drivers optimize skin to driver contact. Program and/or institutional protocols for MRE should be developed and informed by manufacturer specific details amongst other clinical and imaging parameters.
Rationale: Various resources are available to MR technologists and radiologists for onboarding and to develop the necessary knowledge and competence in performing and interpreting MRE.12-15 MR vendors typically provide in-service training sessions during MRE implementation, and MR staff (technologists, radiologists, physicists) involved in the MRE program should have time set aside in the clinical schedule to attend training sessions.
Programs may consider negotiating with high-volume MRE centers to coordinate short secondments for lead MR personnel to gain further experience. This can accelerate the learning process and enhance skill acquisition and comfort levels. In our experience, keeping and maintaining an easy-to-follow procedure manual (a step-by-step scanning guide) is helpful for MR technologists. This can be strategically placed in the MR control room, so staff have easy access to this resource.
Programs should also consider investing in relevant educational materials that their technologists and radiologists can access when needed. This may include relevant literature on MRE, educational videos, and online resources. Professional bodies such as the Radiological Society of North America (RSNA), the Society of Abdominal Radiology (SAR), and International Society for Magnetic Resonance in Medicine (ISMRM) host MRE lectures and workshops run by experts in the field.
To facilitate introductory training on MRE for technologists and radiologists, the CAR MASLD WG has developed an introductory training presentation which can be accessed online as Appendix B.
Rationale: MRE programs should consider the implementation of a standardized institutional protocol and structured reporting template for MRE. This promotes uniformity in form and content of reporting, ensures all relevant information is included, and acceptable standards are maintained. As noted, a readily available easy-to-follow manual (a step-by-step scanning guide) can be particularly helpful for technologists and radiologists with limited experience and/or limited or infrequent patient volumes.
Template reporting can serve as a checklist for radiologists facilitating a more comprehensive assessment of the imaging study and reducing the likelihood of omission errors. These templates are designed to be user-friendly and easy to complete to reduce reporting times, improve efficiency and provide an educational support tool for new radiologists and trainees. By standardizing the terminology and format of the radiology report, structured reporting for MRE can improve the clarity of communication and reliability with referring physicians. Data from structured reports can be further used in data mining for quality improvement initiatives to evaluate the performance of an MRE program.
An example of a structured MRE reporting template developed by the CAR MASLD WG is provided as Figure 2.
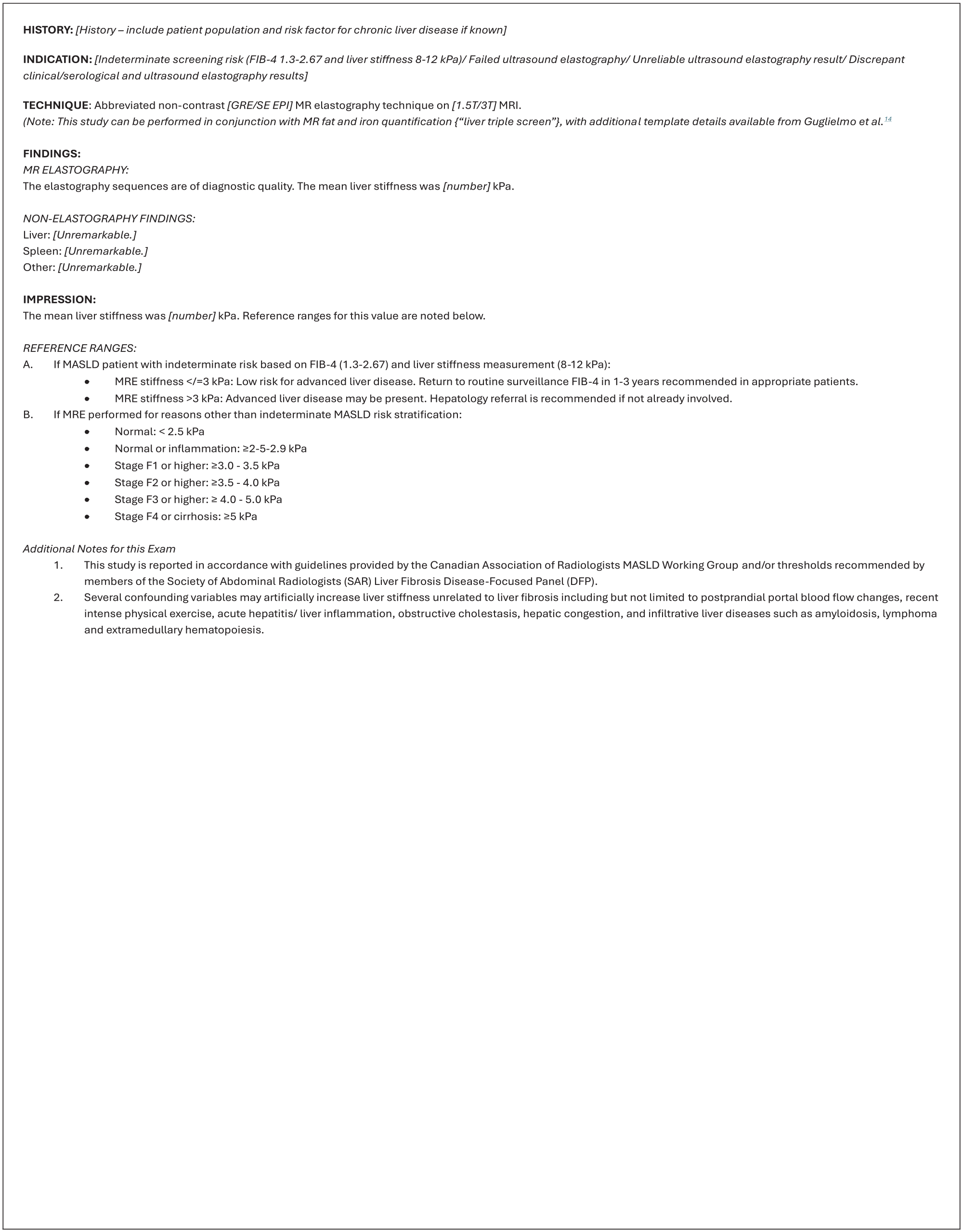
Standardized magnetic resonance elastography structured reporting template example.
Part 3E: MRE Training Recommendations
Rationale: There is no known literature addressing the minimum number of training cases required for technologist competency in performing MRE. The CAR MASLD WG consensus is that in the setting of direct radiologist supervision, a minimum of 5 cases is recommended to develop familiarity with performing MRE in addition to basic pearls and troubleshooting principles. The WG recognizes that MR technologists are often working in a team environment which may aid technologists with limited experience. In addition, as suggested in recommendation #13, an onsite step-by-step scanning guide can be particularly helpful for technologists with limited experience or infrequent patient volumes. The extent of technologist training and skill maintenance should be determined on an individual basis, and may depend on imaging quality and understanding of adequate technique.
Rationale: There is no known literature addressing the minimum number of training cases required for radiologist competency in performing MRE. The CAR MASLD WG consensus is that in addition to information detailed in recommendation #12, radiologists should participate in the acquisition of at least 5 MRE cases to obtain a better understanding of the technical steps involved in image acquisition and the common pitfalls and troubleshooting solutions. Additional radiologist training and skill maintenance should be determined on an individual basis depending on expertise with advanced MR imaging and comfort level.
Rationale: Guglielmo et al described a series of steps for optimizing the MRE technique. 14 This includes patient preparation, correct passive driver placement, selecting the optimal section of the liver to image, performing the MR acquisition during end-expiration, pulse sequence timing, and MR parameter adjustments to fine-tune the image quality. Having all MRE examinations performed with radiologist supervision is recommended to ensure technical quality, assist with troubleshooting, and reduce failure rates. Before a patient is removed from the MR table and the examination is completed, images should be evaluated for adequacy by the MR technologist and radiologist. It is necessary to inspect the MR magnitude, phase, wave, and elastogram images to assess for potential irregularities and errors. For degraded or failed images, the cause should be identified and the MRE sequences repeated once corrections are performed. A detailed understanding of these common pitfalls, troubleshooting and quality control prior to initiating reporting can equip the supervising radiologist with the necessary skills to successfully assist in this capacity.
Moura Cunha et al provide guidance for interpretation and reporting of liver MRE. 12 This includes a summary of confounders and technical pitfalls affecting MRE interpretation, a summary of diagnostic performance of MRE for staging liver fibrosis, and a review of thresholds for staging liver fibrosis according to the Liver Imaging Reporting and Data System (LI-RADS) Quantitative Imaging Working Group and the Society of Abdominal Radiology Liver Disease Focus Panel.
To aid with introductory training of these skills, a training presentation with useful references for supplementary reading can be accessed online as Appendix B.
Part 3F: MRE Quality Assurance Recommendations
Rationale: The CAR MASLD WG advises that MRE QA should be integrated into standard program/institution QA programs including evaluating study success rates, image quality, and reporting standards. Emphasis should be placed in optimizing the technical quality of the MRE acquisition. Additionally, audits of program effectiveness and impact are advised in consultation with other relevant stakeholders to identify areas for system improvement. Regular discussions and feedback between the lead radiologist(s), MR technologists, physicists, and department managers can promote continual MRE program improvement and increased efficiency.
Part 3G: Funding Body Remuneration Recommendations
Rationale: The prevalence of MASLD is rising with approximately 30% of adults in North America believed to have some spectrum of disease severity and approximately 3% of patients at risk for developing liver-related events such as liver failure, complications of portal hypertension, and/or hepatocellular carcinoma.16-19 Combining the growing prevalence and increased awareness of this disease necessitates a move toward population level screening and risk stratification by primary care providers. This approach, with the addition of imaging-based interventions, can be a cost-effective means to prevent and even reverse the severity of liver disease in some MASLD patients, potentially improving outcomes for this population.5,20 In Parts 1 and 2 of these guidelines, the CAR MASLD WG outlined more than 30 recommendations to identify, and risk stratify these patients. To achieve a successful screening program, the WG recognizes the need for collaborative efforts by both regional healthcare administrators and health providers to achieve adequate training, funding, and accessibility necessary to offer these services in patients with suspected MASLD. Funding appropriate to compensate for training, additional technologist and radiologist work hours and to upgrade software and hardware to offer these services in a broadly equitable manner is needed. For example, SWE can be offered as a supplement to routine abdominal and/or liver specific ultrasound imaging but requires additional technologist and radiologist time to obtain reliable results with standardized techniques outlined in Parts 1 and 2 of these guidelines. To successfully achieve broad adoption by health care providers, the CAR MASLD WG recognizes that these services require additional time and corresponding compensation.
Conclusion
The CAR MASLD WG has developed a comprehensive set of nearly 50 recommendations to identify and risk stratify patients with suspected MALSD. In Part 1, 17 recommendations for detecting and grading hepatic steatosis using ultrasound, CT, and MRI are discussed. In Part 2, 14 recommendations for risk stratifying MASLD patients using blood-based and imaging-based techniques are discussed, with specific recommendations surrounding SWE and MRE examinations. In Part 3, an additional 18 recommendations are offered to standardize program implementation, remuneration, and quality assurance across SWE and MRE programs. Training presentations and template examples are provided for SWE and MRE technologists and radiologists to assist with the implementation of these new programs. These guidelines have ultimately been established with the goal of achieving population level screening and risk stratification of MALSD patients across Canada.
Supplemental Material
sj-pdf-1-caj-10.1177_08465371251357446 – Supplemental material for Part 3: CAR Dysfunction-Associated Steatotic Liver Disease Working Group Recommendations for Ultrasound Shear Wave Elastography and MR Elastography Program Implementation, Funding, and Quality Assurance
Supplemental material, sj-pdf-1-caj-10.1177_08465371251357446 for Part 3: CAR Dysfunction-Associated Steatotic Liver Disease Working Group Recommendations for Ultrasound Shear Wave Elastography and MR Elastography Program Implementation, Funding, and Quality Assurance by Mitchell P. Wilson, Gavin Low, Alexandra Medellin, Silvia D. Chang, Emily Pang, Toni Whitaker, Andreu F. Costa, An Tang, Jérémy Dana, Noam Millo, Ania Kielar, Li Xin Zhang, Abdel-Aziz Shaheen, Mark Swain, Victoria Leung, Daisy Fung, Casey Hurrell and Christopher Fung in Canadian Association of Radiologists Journal
Supplemental Material
sj-pdf-2-caj-10.1177_08465371251357446 – Supplemental material for Part 3: CAR Dysfunction-Associated Steatotic Liver Disease Working Group Recommendations for Ultrasound Shear Wave Elastography and MR Elastography Program Implementation, Funding, and Quality Assurance
Supplemental material, sj-pdf-2-caj-10.1177_08465371251357446 for Part 3: CAR Dysfunction-Associated Steatotic Liver Disease Working Group Recommendations for Ultrasound Shear Wave Elastography and MR Elastography Program Implementation, Funding, and Quality Assurance by Mitchell P. Wilson, Gavin Low, Alexandra Medellin, Silvia D. Chang, Emily Pang, Toni Whitaker, Andreu F. Costa, An Tang, Jérémy Dana, Noam Millo, Ania Kielar, Li Xin Zhang, Abdel-Aziz Shaheen, Mark Swain, Victoria Leung, Daisy Fung, Casey Hurrell and Christopher Fung in Canadian Association of Radiologists Journal
Footnotes
Abbreviations
CAR Canadian Association of Radiologists
CSAR Canadian Society of Abdominal Radiologists
CT computed tomography
EFUMB European Federation for Ultrasound in Medicine and Biology
FIB-4 Fibrosis-4 Index
ISMRM International Society for Magnetic Resonance in Medicine
LI-RADS Liver Imaging Reporting and Data System
MASLD metabolic dysfunction-associated steatotic liver disease
MRE magnetic resonance elastography
MRI magnetic resonance imaging
NAFLD nonalcoholic fatty liver disease
pSWE point shear wave elastography
QA quality assurance
RSNA Radiological Society of North America
SAR Society of Abdominal Radiology
SRU Society of Radiologists in Ultrasound
SWE shear wave elastography
TE transient elastography
US ultrasound
WG working group
ORCID iDs
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.