
Abstract
Introduction
The burden of cardiovascular disease (CVD) in Canada and the United States (US) is significant, currently representing one of the leading causes of premature death in men and women 1 and the costliest disease for Canadian and US healthcare systems. 2 Although progress has been made in recent decades to reduce CVD-related mortality in North America, women continue to be underdiagnosed and undertreated for CVD. 3 This may be attributed to the use of current risk stratification tools, such as the Framingham Risk Score (FRS), which does not take sex-specific risk factors into account. 4 Michos et al 5 identified suboptimal risk stratification in women (84% of “low risk” women by FRS had coronary artery calcification [CAC] greater than, or equal to, the 75th percentile for matched age and sex). This highlights the need for more accessible and accurate cardiovascular risk assessment tools. 6
Breast arterial calcifications (BAC) are an incidental finding on breast mammography that have been linked to the presence of coronary artery calcification (CAC) on computed tomography (CT)7-12 and increased risk of incident CVD events including mortality, ischemic stroke, and heart failure.13-17 An association between BAC and sex-specific CVD risk factors, including menopausal status and increased parity, has also been identified. 18
Although extensive research over several decades has identified this link between BAC, CAC, and incident CVD events, BAC is not routinely reported on mammography. 19 The Canadian Society of Breast Imaging (CSBI) 20 released a position statement with reporting guidelines for BAC in January 2023, adapted from McLenachan et al. 21 However, there are no standardized reporting guidelines for BAC in North America. A lack of standardized reporting guidelines impedes the inclusion of BAC in mammography reports. 22 Moreover, uncertainty on optimal management recommendations when BAC is identified may also be a contributing barrier to widespread BAC reporting. One prior study assessed outcomes of BAC reporting on cardiovascular risk assessment. 23 This study identified that informing patients of their BAC status can facilitate downstream cardiovascular risk assessment and that women want to know their BAC status. However, participants in this study did not undergo calcium score CT and therefore, their CAC status was not known.
Our study aimed to assess follow-up after notification of BAC and CAC status in a prospectively recruited cohort undergoing mammography, without known CVD. We collected data on follow-up with primary care providers (PCP), initiation of further cardiovascular screening or tests, specialist referral, and changes in lifestyle at 6 months. We also assessed the association between BAC on mammography and CAC on coronary calcium score CT.
Methods
Our study was a prospective, longitudinal cohort study of participants undergoing mammography at a single hospital centre. Inclusion criteria was any participant undergoing mammography for screening or surveillance; male sex was not an exclusion criterion. Those with established coronary artery disease (CAD) or CVD were excluded, as identified by chart review or survey response. Research ethics approval was obtained from our institutional review board.
Mammogram and CT Imaging
Participants were prospectively recruited over 18 months (August 2022-January 2024) either through referral from a PCP or by volunteering to participate in the study. Research flyers were posted throughout the hospital, including contact information for the research coordinator. Interested subjects reached out via email/phone for further information about the study and/or to sign up. Consented participants underwent a mammogram, if not already done within 6 months. All mammograms were reviewed by 2 fellowship-trained breast radiologists (20+ years’ experience) to report BAC (present/absent), and if present, severity (mild/moderate/severe) according to guidelines by the CSBI, adapted from McLenachan et al (Figure 1).20,21 Vascular calcifications were assessed using standard craniocaudal (CC) and mediolateral oblique (MLO) views from full-field digital mammography (FFDM). Interrater agreement was 96% between radiologists scoring BAC and discrepancies were resolved by consensus. All grade 0 mammograms were classified as “BAC absent,” and all mammograms of grades 1 to 3 were classified as “BAC present.” All participants underwent a coronary calcium score CT scan as part of the study protocol within 6 months of mammography (all CT scans occurred after mammographic imaging). All calcium score CTs were reported by one cardiac imager, and subsequently reviewed by one cardiac radiologist (18 years’ experience), with CAC calculated using the Agatston method (TeraRecon Aquarius INtuition Viewer workstation, v.4.7.0.22-11). There were no clinically significant differences in CAC scoring between imagers.
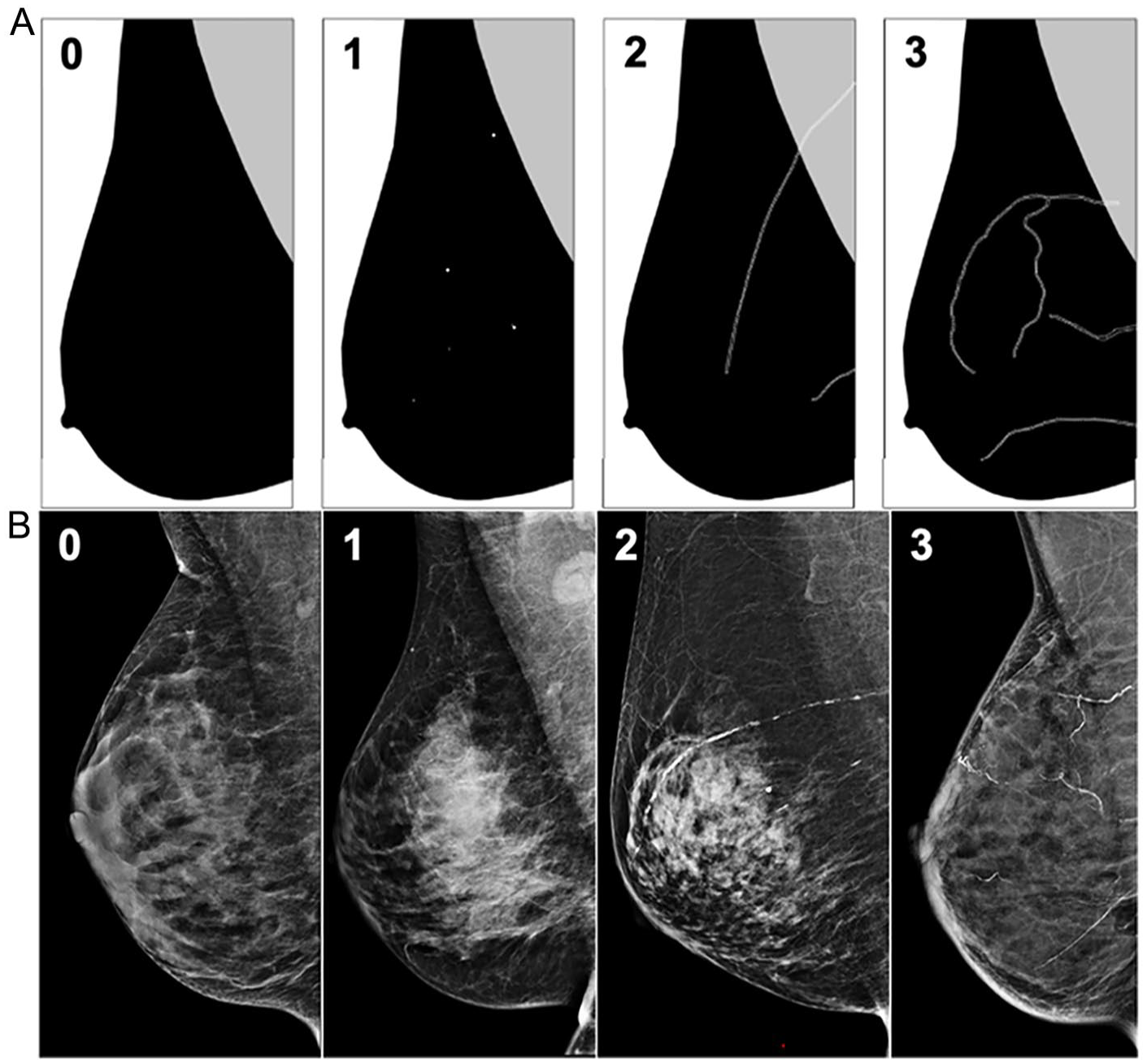
Schematic (A) and mammography (B) images of BAC grading scheme for severity. Grade 0: No breast arterial calcifications. Grade 1: Few punctate breast arterial calcifications without coarse, tram-track, or ring calcifications. Grade 2: Coarse breast arterial calcifications, that may be tram-track in morphology, in fewer than 3 vessels. Grade 3: Severe coarse or tram-track breast arterial calcifications in 3 or more vessels. Schematic courtesy of Dr. Roisin M. Heaney, adapted from McLenachan et al.19,21
Survey Development
Baseline Survey
After providing informed consent, participants completed a baseline questionnaire on demographics (age, sex, body mass index), history of breast cancer (BCa) and treatment, reproductive/gynecologic and obstetrical history (pregnancy, parity, breastfeeding, menarche, polycystic ovarian syndrome [PCOS], gestational diabetes, preterm birth, pre-eclampsia, menopause [status, age]), medications (contraceptives), cardiovascular comorbidities (hypertension, diabetes, dyslipidemia, chronic kidney disease [CKD]), and social history (smoking status, exercise). Participants were asked their perception of their current cardiovascular risk and pre-existing awareness of the correlation between BAC and CVD. Current lipid-lowering therapy was asked of those with BAC and CAC and added to the questionnaire during the study period. Supplemental Appendix 1 details the baseline questionnaire.
Follow-Up Survey
After completion of the calcium score CT, all participants and referring providers were notified of BAC and CAC presence/absence via the research coordinator and electronic patient record. The 3 scenarios requiring notification letters were BAC and CAC negative (scenario 1—no specific follow up recommended), BAC positive and CAC negative (scenario 2—no specific follow-up recommended), and BAC negative or positive and CAC positive (scenario 3—follow-up recommended). Since current medical management is guided by CAC score and no standardized follow-up guidelines exist for BAC, no follow-up recommendations were provided when BAC was positive, and CAC was negative. Supplemental Appendix 2 details follow-up information provided.
Approximately 6 months after mammography, participants completed a follow-up questionnaire to evaluate follow-up with their PCP, implementation of any lifestyle modifications, and/or further cardiovascular investigations (Supplemental Appendix 3). Adverse cardiac events, including myocardial infarction (MI) and stroke, were recorded for all study participants.
Statistical Analysis
The survey responses were recorded on a secure database in REDCap. Descriptive statistics summarized demographics and follow-up data. Categorical variables were reported as frequencies and percentages. Normally distributed continuous variables were described with mean, standard deviation, and range, and non-normally distributed variables with median and interquartile range (IQR). Sensitivity, specificity, positive and negative predictive values (PPV, NPV), and Spearman correlation were calculated for BAC and CAC presence. A true positive was defined as the presence of both BAC on mammography and CAC on CT, and a true negative as the absence of both. False positives had BAC without CAC, while false negatives had CAC without BAC. Weighted Cohen’s Kappa assessed agreement between BAC scores and Fisher exact assessed differences in BAC prevalence with cardiovascular/reproductive risk factors. Statistical significance was P < .05. STATAv.18.5 (StataCorp LLC, TX) was used for analysis.
A sample size calculation was completed before recruitment, a total of 219 participants would be required to achieve 80% power with an α = .05, and a margin of error of ±0.10, given an estimated CAC prevalence of 40%, sensitivity of 65%, and specificity of 85%, based on the literature.11,12,24,25
Results
A total of 314 participants were screened for enrolment. Prior to mammography, 3 were ineligible (all had prior stroke), 12 were lost-to-follow-up, and 5 were no longer interested in participating in the study. Seven participants withdrew before completing their CT, and 1 did not attend the CT appointment. A total of 286 participants completed the primary survey, mammogram and CT. All participants (286/286) completed the follow-up questionnaire (Figure 2).
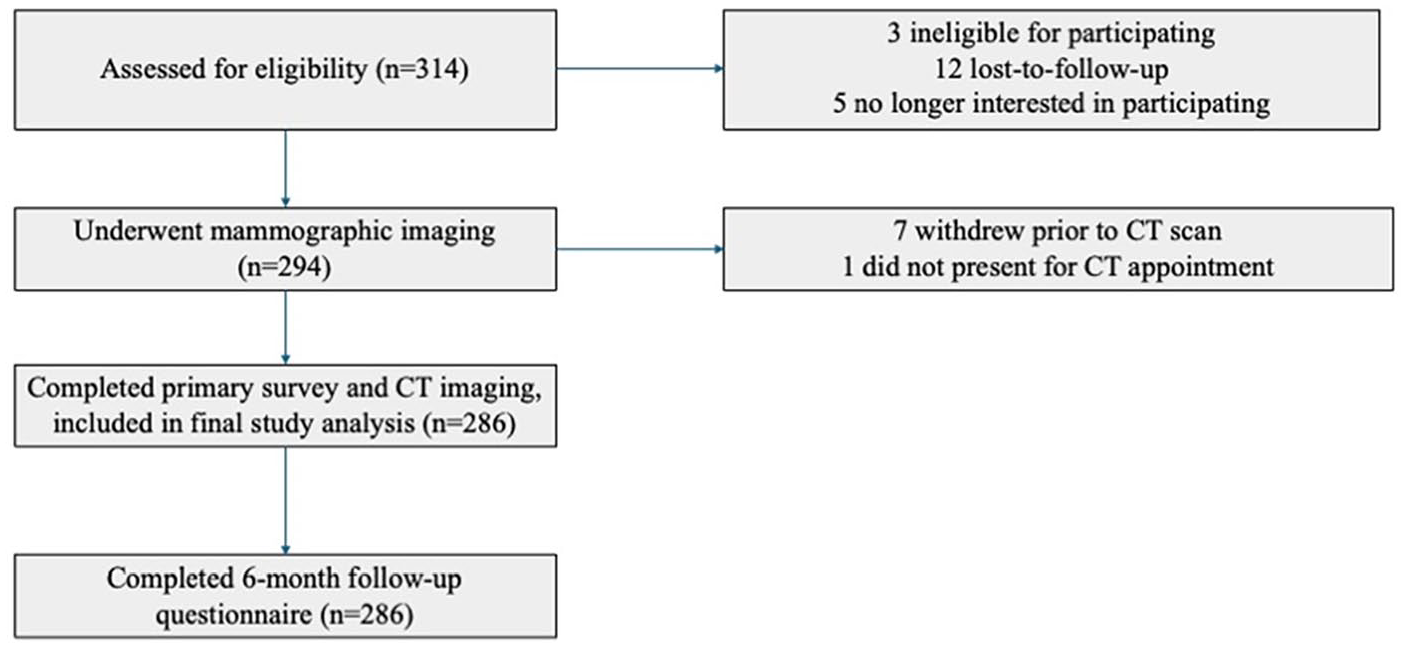
Flow diagram demonstrating study recruitment and participants included in final analysis.
Demographics and Cardiovascular Risk Factors
The mean age of participants was 62 ± 10 years (range 33-87), and 99% female (285/286). Median BMI was 24.5 (IQR: 22.1-27.7). Most participants underwent BCa screening (227/286, 79%), with 59 participants (21%) in surveillance following BCa. Of those with prior BCa, 34 had left-sided, 5 had bilateral, and 20 had right-sided disease. Most participants with prior BCa had radiation therapy (RT; 90%, 53/59), 32 of which had left-sided BCa. Regarding BAC, 9/53 (17%) with prior RT had BAC, compared to 1/6 (17%) not treated with RT. The prevalence of CAC was 50% (16/32) among those with prior RT for left-sided BCa, versus 44% (7/16) for right-sided BCa (P = .77).
Sixty-five percent (186/286) had previously been pregnant and 66% (189/286) had used a form of hormonal contraception. Of those with prior pregnancy, 6% (11/186) had gestational diabetes, 6% (11/186) had pre-eclampsia, and 4% (8/186) had preterm birth. Most (217/286) reached menopause at the time of study (median age 51 years, IQR: 49-54). Regarding cardiovascular risk factors, 11 participants (4%) had diabetes (Type 1, n = 2, Type 2, n = 9). Sixty-eight had dyslipidemia (68/286), 17% (50/286) had hypertension, 14% (39/286) had PCOS, and 1 participant had CKD not on dialysis. Nearly all participants (98%, 281/286) were non-smokers. Most (71%, 17/24) of those with BAC and CAC were not on lipid-lowering therapy at the time of study. All demographic variables are presented in Table 1.
Demographic and Cardiovascular Risk Data of 286 Prospectively Recruited Participants.
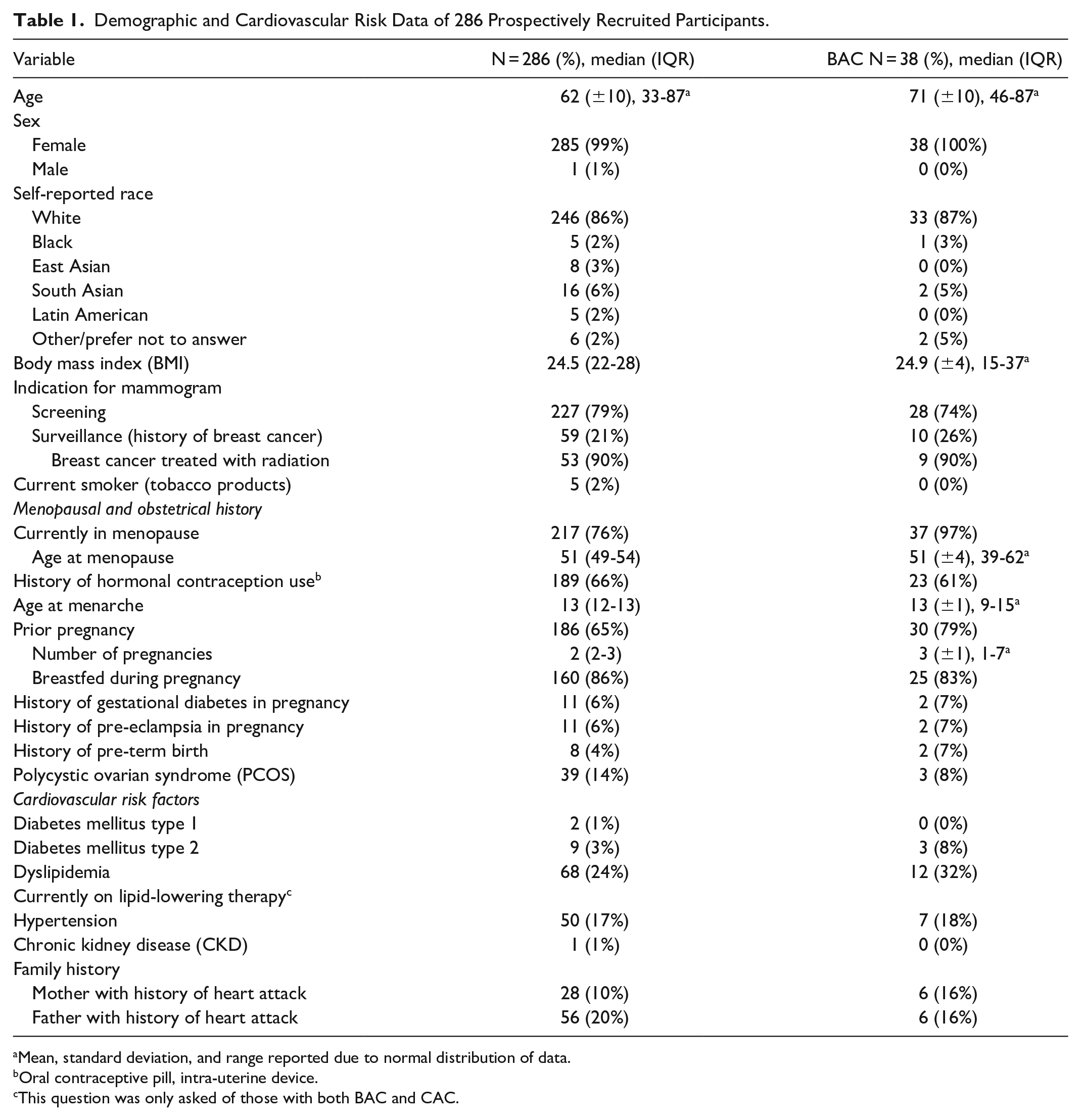
Mean, standard deviation, and range reported due to normal distribution of data.
Oral contraceptive pill, intra-uterine device.
This question was only asked of those with both BAC and CAC.
BAC prevalence was higher in those with prior pregnancy (16%, 30/186 vs 8%, 8/100, P = .04), post-menopausal participants (17% (37/217) vs 1% (1/68), P < .001) and those over the age of 60 (22%, 36/164, vs 2%, 2/122, P < .001). Most (63%, 15/24) participants with BAC and CAC did not believe they were at risk of CVD, and only one (4%, 1/24) was previously aware of the association between BAC and CVD (Table 2).
Participant Perception of Personal Cardiovascular Risk and Predictive Capacity of Breast Arterial Calcification on Mammography for Coronary Artery Calcium on CT.
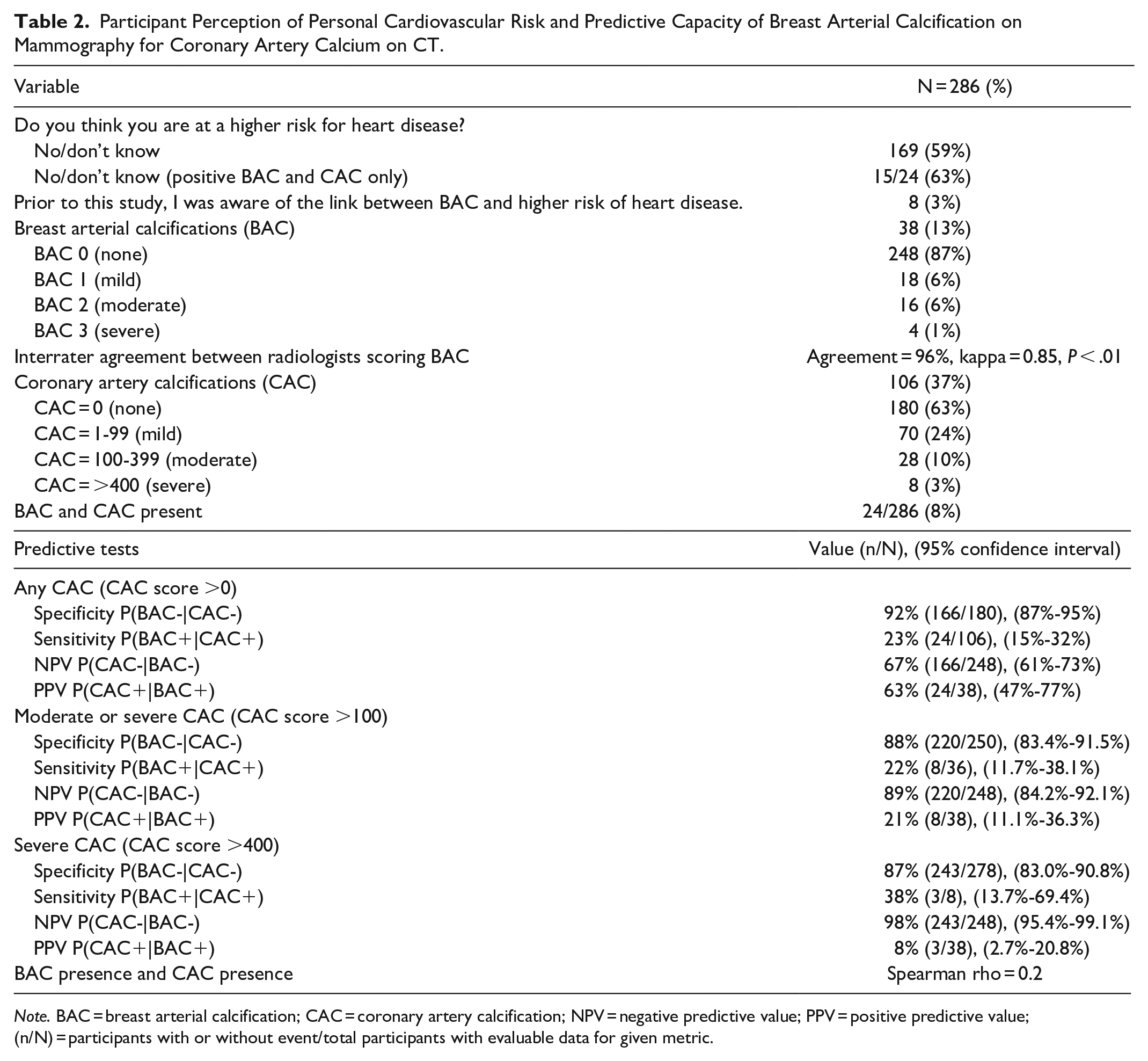
Note. BAC = breast arterial calcification; CAC = coronary artery calcification; NPV = negative predictive value; PPV = positive predictive value; (n/N) = participants with or without event/total participants with evaluable data for given metric.
Breast Arterial Calcifications and Coronary Artery Calcifications
The prevalence of BAC and CAC was 13% (38/286) and 37% (106/286), respectively. For BAC, 248 had none (87%), 18 (6%) mild, 16 (5%) moderate, and 4 (1%) severe. Sixty-three percent of participants had no CAC (180/286), 70 (24%) had CAC 1-99, 28 (10%) CAC 100-399, and 8 (3%) CAC ≥400. The presence of BAC had 92% specificity (166/180), 23% sensitivity (24/106), 63% PPV (24/38), and 67% NPV (166/248) for detecting CAC. The accuracy of BAC for detecting any CAC was 66%, and the accuracy of BAC for detecting moderate or severe CAC was 80%. For CAC >100 and >400, BAC had 89% (220/250) and 98% NPV (243/248), respectively. Interrater agreement was 96% between radiologists scoring BAC, kappa = 0.85 (P < .01; Table 2). Twenty-four participants had both BAC and CAC (8%), 14 (5%) had BAC and no CAC, and 82 (29%) had CAC but no BAC (Figure 3 illustrates BAC and CAC in one participant). Referring providers were notified of all incidental CT findings, detailed in Supplemental Appendix 4.
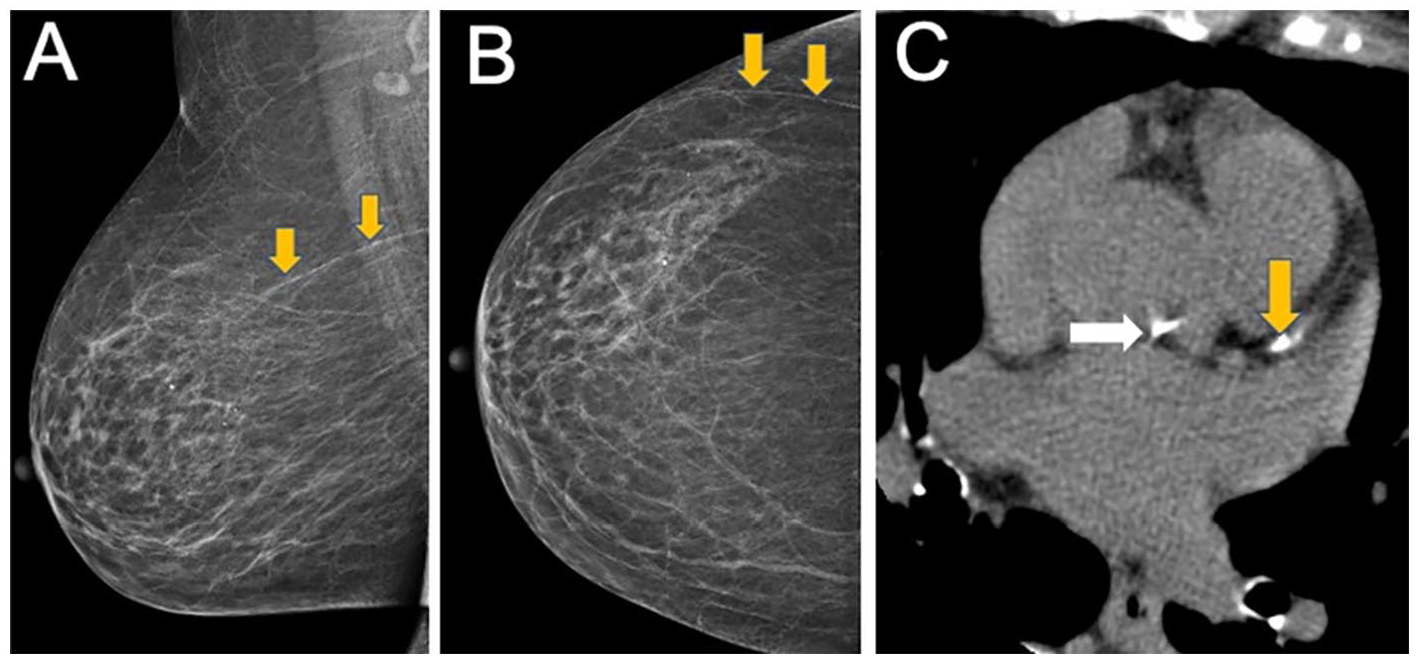
Medial lateral oblique (A) and cranial-caudal view (B) of the right breast in a 70-year-old participant who underwent screening mammography demonstrating Grade 2 BAC (orange arrows) in the upper outer quadrant. Calcium score CT (C) in the same 70-year-old participant. Axial image shows mild CAC in the left anterior descending artery (Agatston score of 64; yellow arrow) and aortic root calcification (white arrow) due to calcified atherosclerotic plaque.
Follow-Up After Imaging
All participants (286/286) completed follow-up questionnaires. Median follow-up time was 202 days since the initial mammogram (IQR 185-237). 92% (22/24) of those with BAC and CAC had an appointment scheduled with their PCP and 46% (11/24) made changes to lifestyle. Of those who completed their appointment (n = 18), 44% had been referred to a cardiologist (8/18) and 17% underwent electrocardiogram (ECG) testing (3/18). One participant with BAC and CAC had a stroke during the follow-up period. No other cardiac events were recorded (Table 3).
Follow-Up After Initial Mammography, Assessing Primary Care Follow-Up and Implementation of Cardiovascular Risk Reduction Strategies Due to Study Findings.
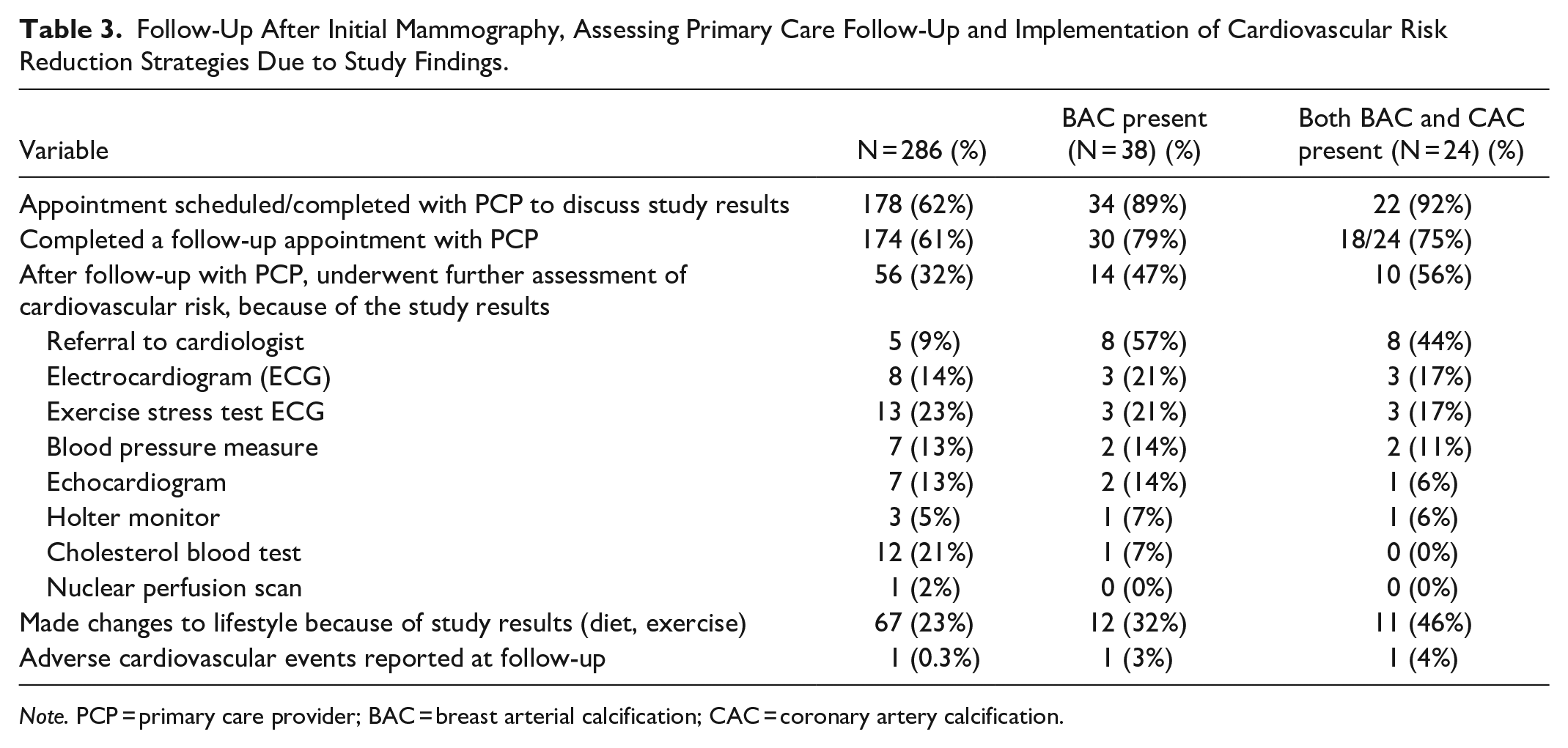
Note. PCP = primary care provider; BAC = breast arterial calcification; CAC = coronary artery calcification.
Discussion
The association between BAC, CAC and CVD events, including mortality and stroke, has been well-documented in the literature.13,15,16,26,27 We sought to build on this literature with the first Canadian prospective cohort assessing follow-up after BAC and CAC reporting in participants without known CVD, undergoing mammography. The prevalence of BAC in our study cohort was 13%, similar to prior research.10,23,28 BAC prevalence was greater in those over age 60, post-menopausal participants and those with prior pregnancy. Most participants with BAC and CAC were unaware of their cardiovascular risk and not on lipid-lowering therapy. Following notification, 92% of participants with BAC and CAC pursued PCP follow-up within 6 months, 56% underwent cardiovascular risk assessment at the time of follow-up assessment, and 46% made changes to lifestyle, based on the study findings.
It is well-documented that the presence of BAC is strongly associated with incident cardiovascular events.26,28 A recent study by Allen et al identified that each 10-point increase in BAC score is associated with higher risk of mortality and composite outcome of MI, heart failure, stroke, and mortality in a cohort of 18 092 women. 26 These associations persisted even in traditionally “low risk” groups, including younger women, nonsmokers, and those without diabetes, hypertension, hyperlipidemia, CKD, or prior CVD. Despite this strong evidence, we found that 71% of participants with both BAC and CAC were not on lipid-lowering therapy, and 63% did not perceive themselves as high risk for CVD. Given that BAC is most predictive of future cardiovascular events in younger women (40-59 years old), 26 similar to the age of those initiating screening mammography and our study cohort, BAC notification may present an opportunity to enhance patient and provider awareness of cardiovascular risk.
Consistent with prior studies, 18 we found BAC to be more prevalent in those over 60 years of age, post-menopausal participants, and those with a history of pregnancy. While BAC demonstrated high specificity, its sensitivity for detecting concurrent CAC in our cohort was low. This finding aligns with a large meta-analysis of 33 583 patients, which identified high specificity of BAC for detecting CAD/atherosclerotic CVD, but low sensitivity (maximum of 50%). 29 The low sensitivity in our study may also be attributable to low BAC prevalence, potentially due to the exclusion of participants with known CVD and our relatively young cohort (mean age 62 years). Due to the low sensitivity, BAC on mammography will not identify all women at risk for CV disease and therefore other CV risk factors need to be considered.
A key objective of our study was to assess follow-up after BAC and CAC reporting. We found that 92% of participants with BAC and CAC scheduled PCP follow-up within 6 months of mammography, compared to 44% of those without BAC or CAC. Our study could not isolate the impact of BAC reporting alone—since all participants were notified of their CAC status and no guidelines on appropriate follow-up based on BAC positivity currently exist. However, 86% of those with BAC and no CAC pursued follow-up, highlighting the potential for BAC notification to independently prompt PCP follow-up. This aligns with prior research, including Vincoff et al, 23 who found that 57% of participants sought PCP or cardiology follow-up within 3 months of BAC notification, and 81% found it helpful to know their BAC status. Similarly, a 2019 study found that 96% of women preferred to be informed about BAC, with 63% favouring direct notification from the radiology department via letter or telephone. 11 Vincoff et al 23 informed participants and providers of their BAC status via e-mail and a postal letter, respectively. We provided participants and referring providers with a letter stating: “Breast arterial calcification has been shown to correlate with coronary artery calcification and increased risk of cardiovascular events. Given positive BAC on this mammogram and CAC on CT, we suggest evaluation of cardiovascular risk factors and consideration of cardiology consultation if needed.” The high follow-up rates in our study and those in the literature emphasize the value of standardized written notification of BAC status to both patients and providers. Calcium score CT was completed in the present study as part of the protocol to assess correlation of BAC and CAC scores. However, we do not recommend routine calcium score CT after a BAC positive finding. Rather, we recommend that BAC notification prompt cardiovascular risk assessment. Collaboration between cardiologists and the breast imaging community will be essential in establishing standardized recommendations for BAC follow-up and clinical management.
The potential clinical impact of BAC notification is further supported by the literature. A 2021 survey of 1085 physicians reported that 80% of respondents would pursue cardiovascular risk assessment if BAC was present on mammography. 30 Similarly, a 2023 study found that within 3 months of BAC notification, 31% of women underwent echocardiography, 14% underwent cardiac stress testing, and 7% underwent coronary angiography. 23 Additionally, a 2018 study of symptomatic women found that, at 21-month follow-up, those with BAC were significantly more likely to be on cardiac medications, have medication adjustments, or undergo functional cardiac imaging, compared to those without BAC. 31 Our findings align with these results; at 6-month follow-up, nearly half of participants with both BAC and CAC had adopted lifestyle changes, 44% had been referred to a cardiologist, and 17% underwent ECG testing. Integrating BAC reporting into routine mammography may therefore prompt cardiovascular risk assessment or lifestyle modifications, addressing a key gap in cardiovascular care.
Despite broad consensus among radiologists and referring providers that a standardized BAC grading system would be beneficial,30,32 the optimal method for grading BAC remains debated. A large systematic review and meta-analysis identified no difference in the association of BAC and CVD based on BAC grading method 33 and we did not identify a correlation between BAC and CAC severity. However, Allen et al 26 identified that more severe BAC is correlated with increased risk of mortality, MI, and stroke in 18 092 women, suggesting a graded scale could improve long-term risk stratification. The present study used a standardized qualitative BAC template with a grading scheme endorsed by the CSBI, adapted from McLenachan et al.20,21 Interrater agreement with this grading scheme was 96%, suggesting that structured templates may improve reporting consistency. AI software tools have also shown value in accurately detecting BAC presence and may help maintain clinical efficiency, minimize workflow disruptions, and streamline BAC implementation. 26 Additional research on AI-driven BAC detection will be important to inform future guidelines.
There is conflicting evidence regarding the association between CAD and left-sided RT for BCa. While earlier studies report increased CAD with left-sided RT, 34 recent research, including our study, do not report significant association.35,36 Similarly, we observed no association with BAC prevalence, consistent with recent literature. 37 Collaboration with breast imagers, cardiologists, and primary care providers will be important to guide appropriate BAC follow-up in this population.
We note several limitations. Most of our participants were recruited by self-referral from flyers/posters within our hospital and imaging department, while a smaller proportion were referred by PCPs, introducing possible selection bias. All potential participants were required to contact our research coordinator to consent to participate and we did not record how a study subject was made aware of our study. Our findings and conclusions are limited by a small sample size of patients with both BAC and CAC, although we were powered sufficiently for the prevalence of CAC in our population. We also could not isolate the impact of BAC reporting alone given there are no standardized clinical follow-up guidelines based solely on BAC positivity. Moreover, we did not gather prior smoking status, which can impact CAC prevalence. We followed participants for approximately 6 months (median 202 days), which does not capture long-term events. However, we plan to assess longer-term outcomes in this cohort, including initiation of medical therapy. Future research should involve large, multi-centre studies with broad recruitment and longer follow-up.
Conclusion
In this prospectively recruited cohort undergoing screening and surveillance mammography without known CVD, notification of BAC and CAC status prompted high follow-up rates with primary care providers and adoption of lifestyle modifications. However, the long-term clinical benefits of BAC reporting remain to be determined.
Supplemental Material
sj-docx-1-caj-10.1177_08465371251337022 – Supplemental material for Joint BrEast CAncer & CardiOvascular ScreeniNg: BEACON Study to Assess Opportunistic Cardiovascular Screening Using Breast Arterial Calcification on Mammography
Supplemental material, sj-docx-1-caj-10.1177_08465371251337022 for Joint BrEast CAncer & CardiOvascular ScreeniNg: BEACON Study to Assess Opportunistic Cardiovascular Screening Using Breast Arterial Calcification on Mammography by Hayley McKee, Teresa Bianco, Kaitlin Zaki-Metias, Vivianne Freitas, Sandeep Ghai, Kate Hanneman, Jean M. Seely, Charlotte Yong-Hing, Husam Abdel-Qadir, Paula J. Harvey and Elsie T. Nguyen in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Sir Thomas Cropo Foundation and the Academic Incentive Fund from the Joint Department of Medical Imaging for providing generous grant funding support for our study.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.