
Abstract
Introduction
Cardiovascular disease (CVD) is the leading cause of premature death in Canadian women, 1 and the majority of Canadian women are unaware of their personal cardiovascular risk status. 2 Cardiovascular disease in women is underappreciated, underdiagnosed, undertreated, and poorly researched, 3 and there is growing need for a gender-focused approach to cardiovascular care. 4 Traditional cardiovascular risk assessment tools such as the Framingham Risk Score, typically underestimate cardiovascular risk in women.5,6 In addition to the traditional risk factors, an assessment of a woman’s cardiovascular risk status should include sex-specific risk factors including: early menarche, premature menopause, hypertension in pregnancy, gestational diabetes, pre-term labor, and infertility.3,7,8
Coronary arterial calcium (CAC) score on computed tomography (CT) scans has emerged as a valuable tool for cardiovascular risk stratification, especially in asymptomatic and intermediate risk populations.9,10 Recent literature demonstrates a correlation between breast arterial calcification (BAC) on mammography and CAC, and identifies BAC as an independent cardiovascular risk factor.11-16 Breast arterial calcification is a common incidental finding on mammography, identified in at least 12% of women undergoing mammography as part of breast cancer screening programs, 12 but can range up to 42.5% depending on the population studied. 17 However, BAC is not typically documented in mammogram reports nor is it part of current reporting standards. Given that approximately 54% of eligible patients between the ages of 50–69 years undergo screening mammography in Canada, the detection of BAC on mammography could be used to identify women at higher cardiovascular risk, thereby facilitating lifestyle modification and/or medical intervention at an earlier stage, helping to prevent adverse cardiovascular events and outcomes.3,18 This is particularly important in communities where mammography is available, but more advanced cardiac imaging such as CAC scoring CT may not be accessible.
Recent studies from Europe and the United States (USA) analyzed the practice and perceptions of breast radiologists with regard to the reporting and implications of BAC.19,20 These studies reported a high rate of awareness of BAC as a cardiovascular risk factor (66–81%), with routine documentation of BAC in mammogram reports performed by 41–62% of breast radiologists. There was no consensus as to whether radiologists should inform patients and referring physicians, or provide cardiac follow-up recommendations. Another USA study surveying referring physicians demonstrated that most physicians indicated a preference for BAC reporting and subjective quantification on mammograms, and that such reporting would prompt further workup for coronary artery disease. 21 Furthermore, a 2020 USA survey of patients suggests that most patients prefer routine reporting of BAC on screening mammography and direct correspondence from the radiology department with notification of their result. 22
We hypothesize that most Canadian radiologists who report mammography are unaware of the clinical implications of BAC on mammography as well as the importance of reporting it, from a cardiovascular risk stratification standpoint.
Our study aims to evaluate the awareness of Canadian radiologists who report mammography of the clinical significance of BAC and their attitudes towards reporting BAC on mammography compared to their European and American counterparts.
Methods
This study was a survey of Canadian radiologists who report mammography.
Survey Development
A 25 question non-randomized survey was created in both English and French using the secure online survey software platform SurveyMonkey. In completing the survey, respondents provided consent to collect data on their responses and represent them in aggregate. No personal identifying information was collected about each individual study participant. However, the internet protocol addresses were recorded by SurveyMonkey so that duplicate responses would be detected and rejected. The survey (Supplementary Appendix 1) consists of three parts. The first part assessed the respondent’s demographic information including age and gender identification as well as their current role and subspecialty, practice setting and location, and their annual mammogram reporting volumes. The second part of the survey addressed the respondent’s awareness of the association of BAC and cardiovascular risk, their attitudes and experience in reporting BAC, and opinions on local and national policy on BAC reporting. Lastly, survey respondents were asked if the survey had increased the likelihood of them reporting BAC on mammography in the future and a comment box was provided for any further remarks.
Survey Distribution
The survey was distributed via email to mailing lists of the Canadian Society of Breast Imaging (CSBI), the Canadian Association of Radiologists, Ontario Association of Radiologists, British Columbia Radiological Society, Société de Radiologie du Québec, Alberta Society of Radiologists, and Canadian Radiology Women. The initial email included a brief description of the study and participation was both voluntary and anonymous. Informed consent was obtained prior to completion of the survey. Survey responses were collected during the 5-week period from April 27th 2022 to June 1st 2022. A reminder email was sent 10 days prior to closure of the survey, on May 21st 2022.
Statistical Analysis
The survey responses were recorded on a secure database. Descriptive statistics were used to summarize respondent demographics and responses to the questionnaire. Categorical variables were reported using frequency distributions and percentages.
STATA v.16 software (StataCorp LLC, College Station, TX) was used for statistical analyses. Multinomial logistic regression models were created to assess four specific BAC questions with the following independent variables, determined a priori; community vs academic radiologists, proportion of diagnostic work in mammography (<25% vs >25%), and number of mammograms read annually (<2000 vs > 2000). All independent variables were examined for collinearity using Pearson’s rank coefficient (defined as >|.8|), evaluated for confounding (defined as a 30% change in coefficients on removal of the variable), and tested for significance of pairwise interactions (defined as P < .05). No independent variables met these criteria.
Ethical Approval
This study was approved by the University Health Network Research Ethics Board (REB# 21-5810).
Results
There were 198 responses to the survey over the 5 week period. The total number of radiologists who received the survey is unknown, as any one radiologist could be a member of more than one society, and we did not have access to the member emails to cross reference the various email distribution lists for duplicate emails. Of the 198 responses, 12 were excluded; 6 of these had incomplete responses, 5 respondents did not actually report mammography, and 1 respondent had both an incomplete response and did not report mammography. A total of 186 complete responses were included in the analysis.
Demographics and Breast Imaging Experience
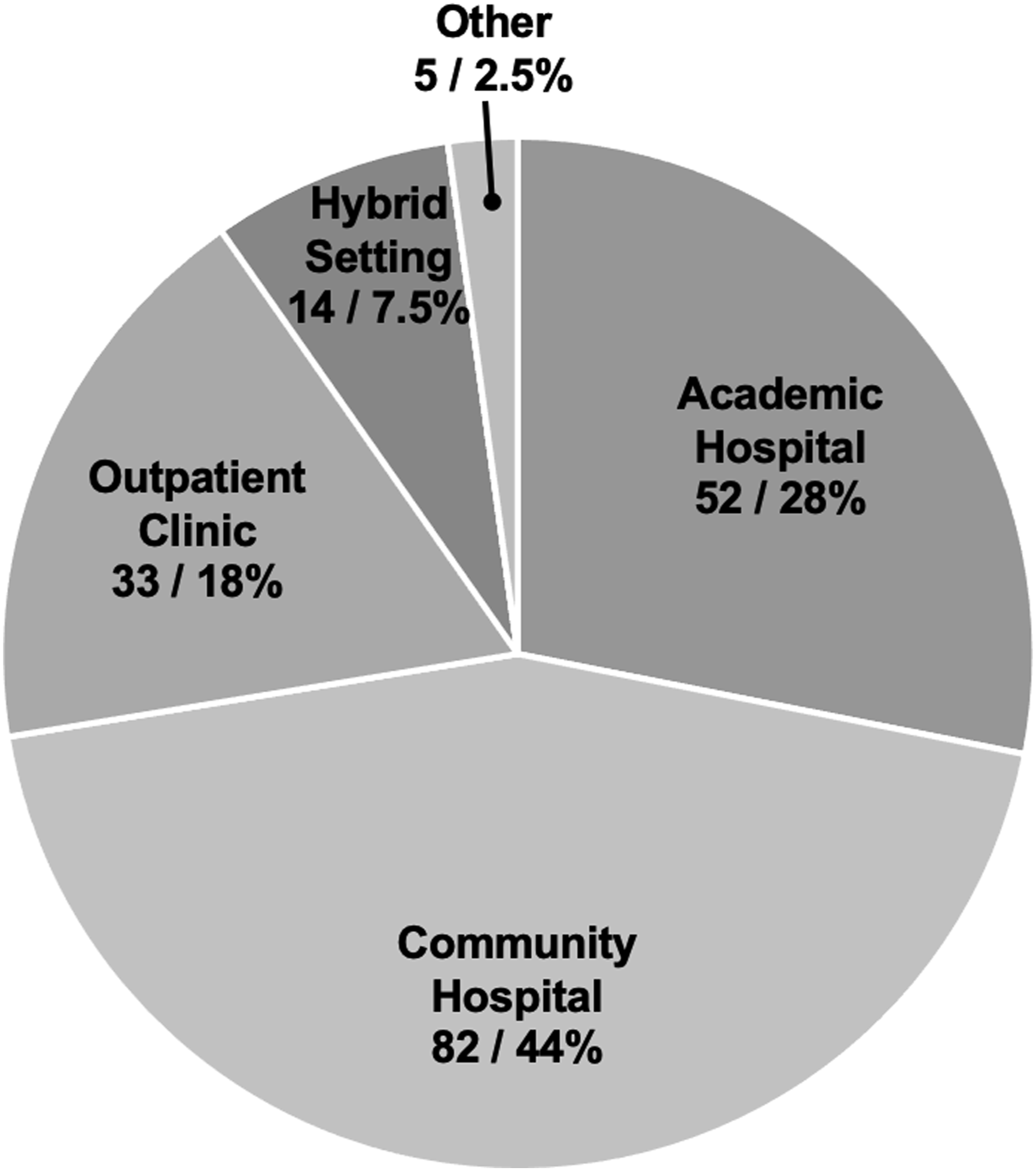
Fifty-five percent (102/186) of respondents identified as female, 44% (82/186) as male, and 1% (2/186) preferred not to say. The most common age range of respondents was 40–49 years (33%, 62/186). Board-certified radiologists comprised the majority (95%, 177/186), with 2% (3/186) radiology residents, and 3% (6/186) radiology fellows also participating. Ontario-based radiologists had the highest rate of participation (53%, 99/186) (Figure 1). Community-based practice was the predominant practice setting (44%, 82/186) (Figure 2), with the majority of radiologists reporting both screening and diagnostic mammograms (96%, 179/186). Breakdown of the location of the survey respondents by Canadian provinces and territories. *Nunavut imaging is interpreted by The Ottawa Hospital and responses are therefore included in the Ontario group. Practice settings of survey respondents.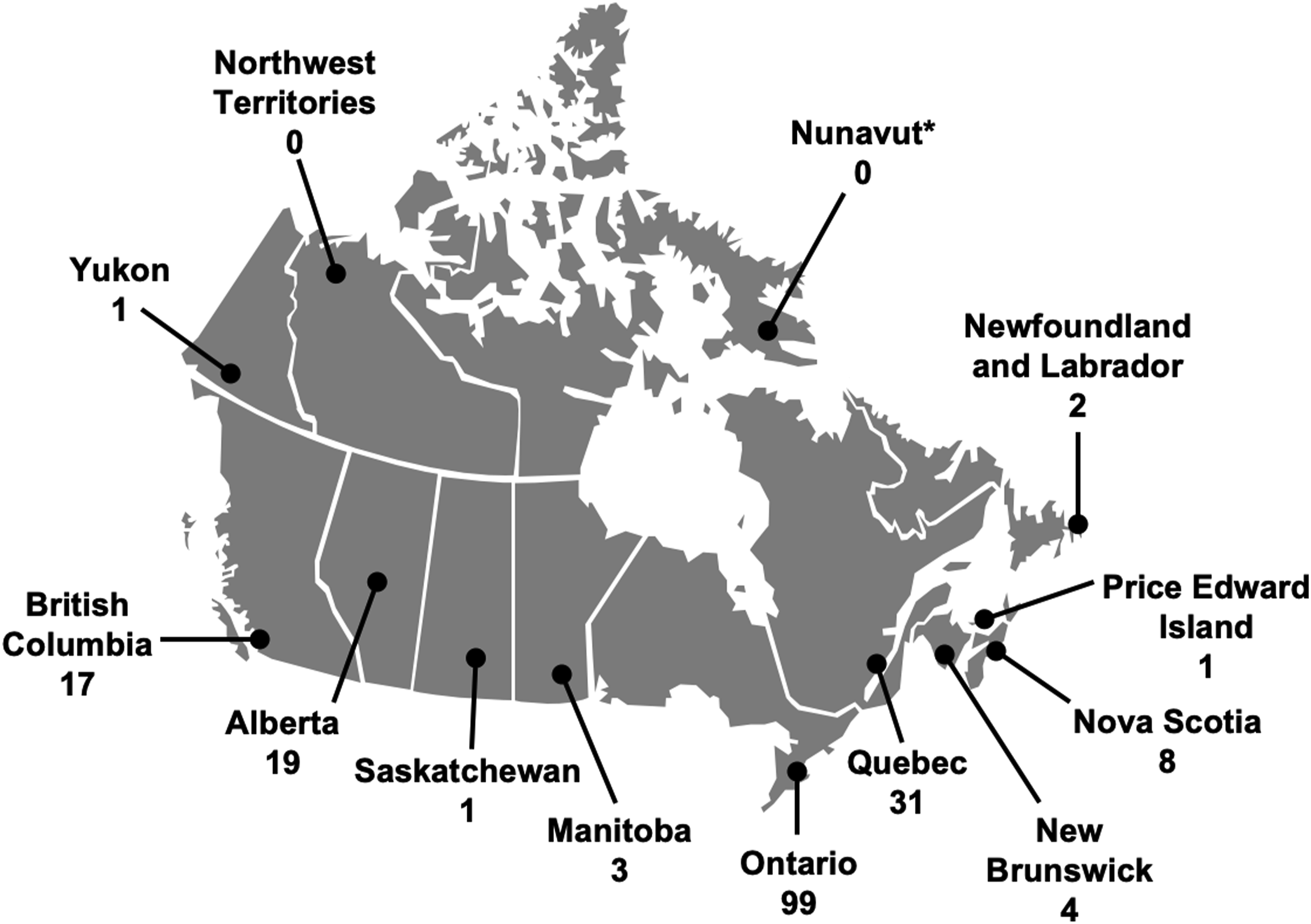
Most respondents reported spending <25% of their clinical time reporting mammography (41%, 77/186), with one third of respondents (62/186) having >20 years of experience reporting mammography, and 42% (78/186) reporting between 1000 and 1999 mammograms per year.
Demographics and Experience of Survey Respondents.
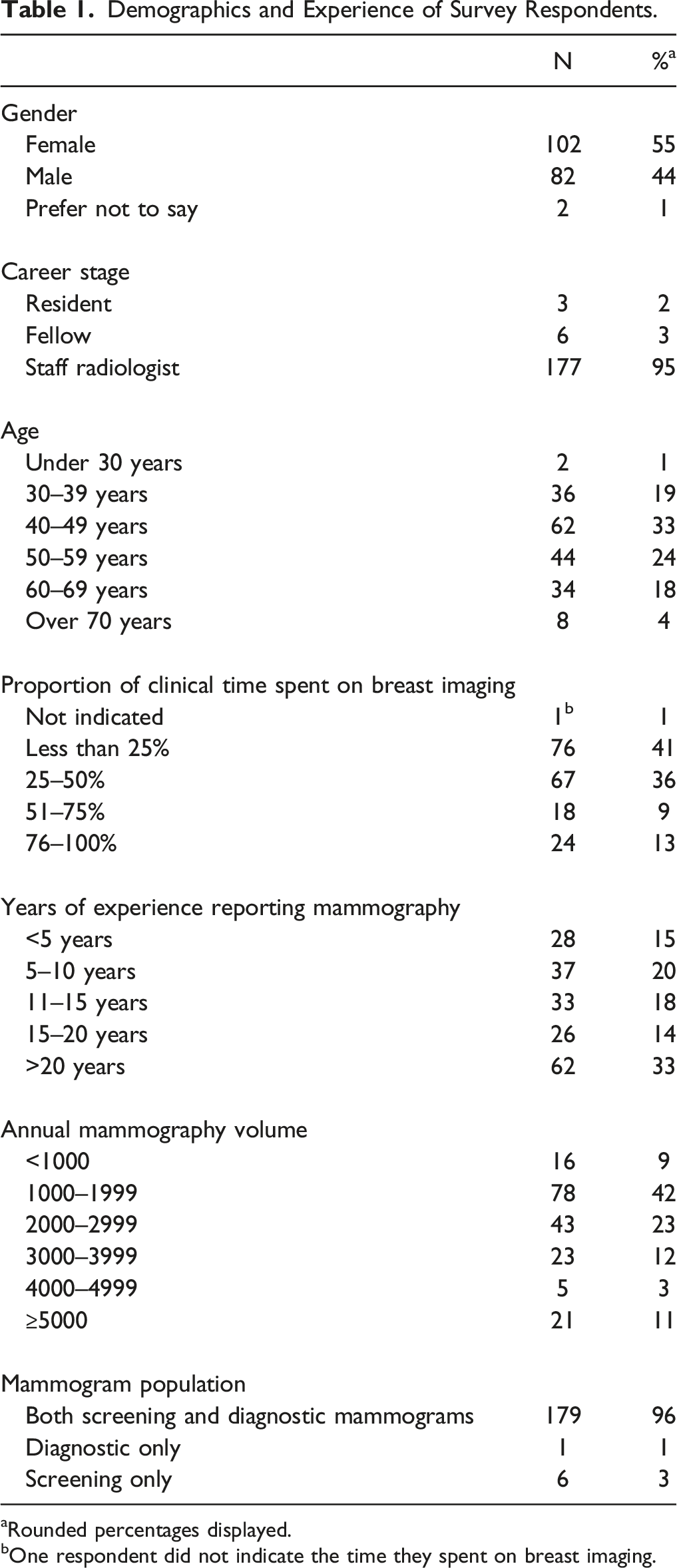
aRounded percentages displayed.
bOne respondent did not indicate the time they spent on breast imaging.
BAC Awareness and Reporting
Sixty percent (112/186) of those surveyed were already aware of the association between BAC on mammography and cardiovascular risk, while 34% (64/186) reported that they were not aware. All of the participating radiology residents (n = 3) and fellows (n = 6) reported that they were aware of the association. Most respondents (46%, 85/186) do not routinely document BAC in their reports, with 30% (56/186) sometimes documenting BAC if severe, and 9% (16/186) selecting the “other” option. Of those that selected “other,” 9 respondents reported BAC if they deemed the patient to be young and 3 declared that they do not report BAC as it is not a permitted function of their reporting program. There is a lack of consensus on whether in principle, BAC should be included in reports, with 22% (41/186) believing it should, 15% (28/186) that it shouldn’t, and 45% (84/186) that it should only if severe or if the patient is young.
Breast Arterial Calcification Awareness and Experience Among Respondents.
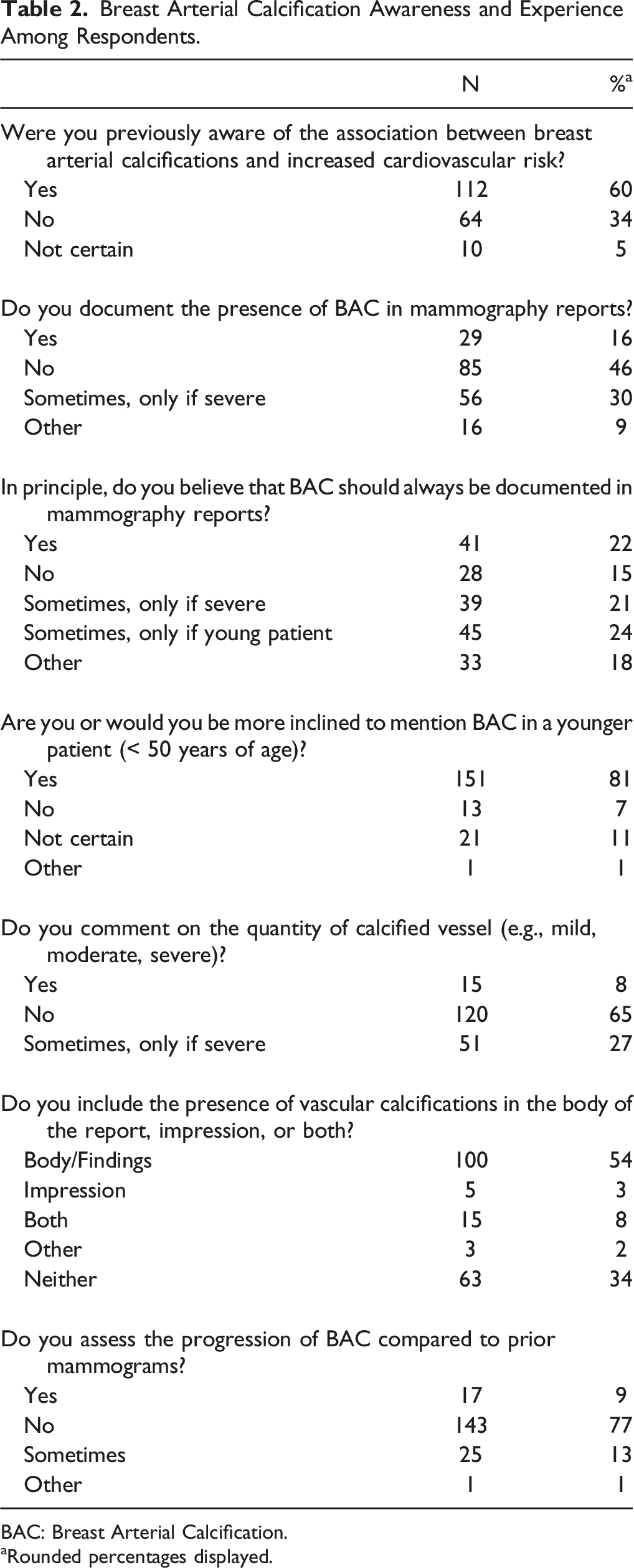
BAC: Breast Arterial Calcification.
aRounded percentages displayed.
Management and Implications of BAC Reporting
The majority of Canadian radiologists who report mammography (96%, 178/186) do not inform the patient about the presence of BAC or investigate the patient’s personal or family cardiovascular risk history (85%, 158/186). Similarly, 81% (151/186) of respondents do not include a recommendation to the referring physician regarding the presence of BAC. Of the surveyed radiologists, only 4% (7/186) work in radiology departments that have standard BAC reporting guidelines, the majority of which are in academic hospitals in Ontario (n = 6).
Clinical Implications of Breast Arterial Calcification Reporting.
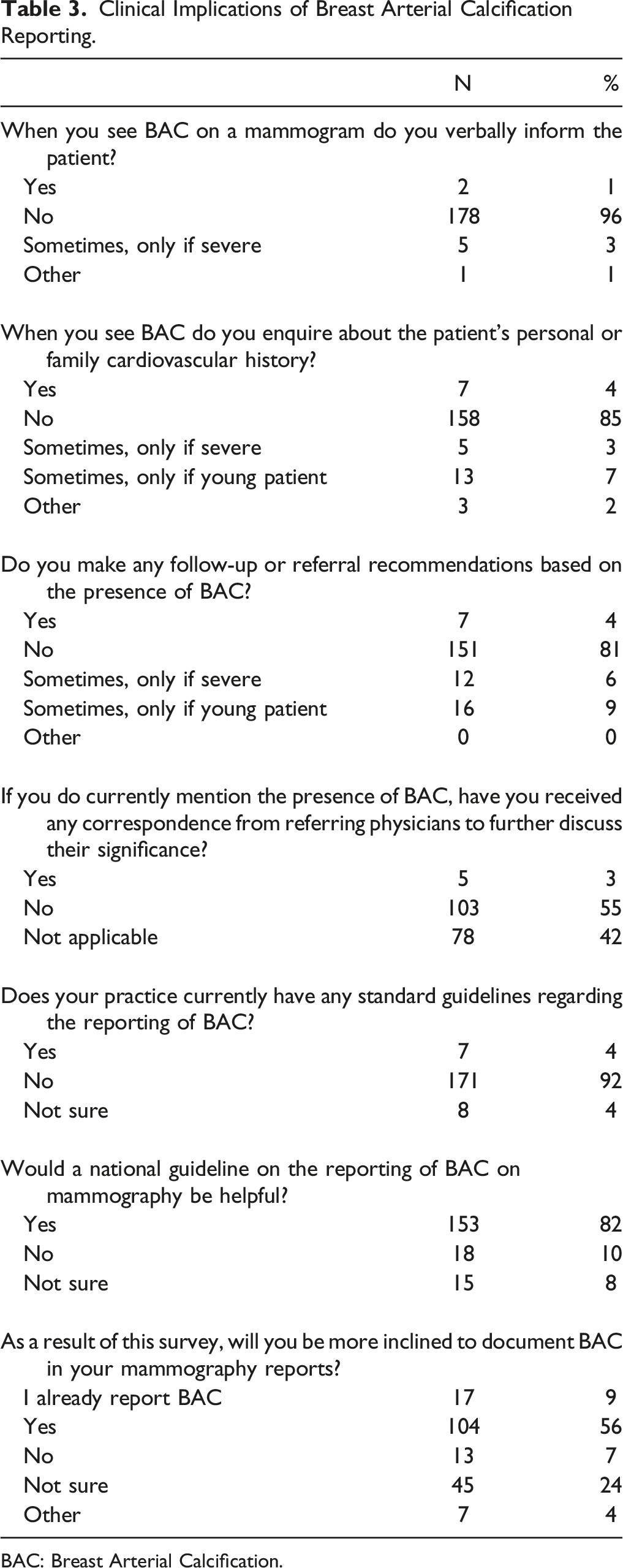
BAC: Breast Arterial Calcification.
Academic radiologists were more likely than community radiologists to be aware of the association between BAC and increased cardiovascular risk (OR 4.56, 95% CI 1.76–11.78, P < .002). There were no other significant trends in survey responses when respondents were categorized according to academic vs community radiologists, proportion of work in mammography, or annual mammographic volume, based on a multinomial regression analysis.
Comparison With European and American Radiologists
BAC: Breast Arterial Calcification.
aDNA = Did not ask.
Discussion
Our survey of Canadian radiologists who report mammography found that while 60% were aware of the association between BAC and cardiovascular risk, only 16% document its presence on mammographic reports with a further 39% who do so if there is a severe burden of BAC or in a young patient. Additionally, the majority of radiologists include this finding in the body of the report and not the conclusion, and little or no correlation with personal or family cardiovascular history or management recommendations are provided. There is a general lack of consensus amongst radiologists on whether, in principle, BAC on mammography should be reported. The majority of radiology departments have no local guidelines on BAC reporting. Eighty two percent of respondents are in favor of a national guideline on BAC reporting and, after completing our survey, 56% of radiologists are now more likely to report the presence of BAC in their mammogram reports.
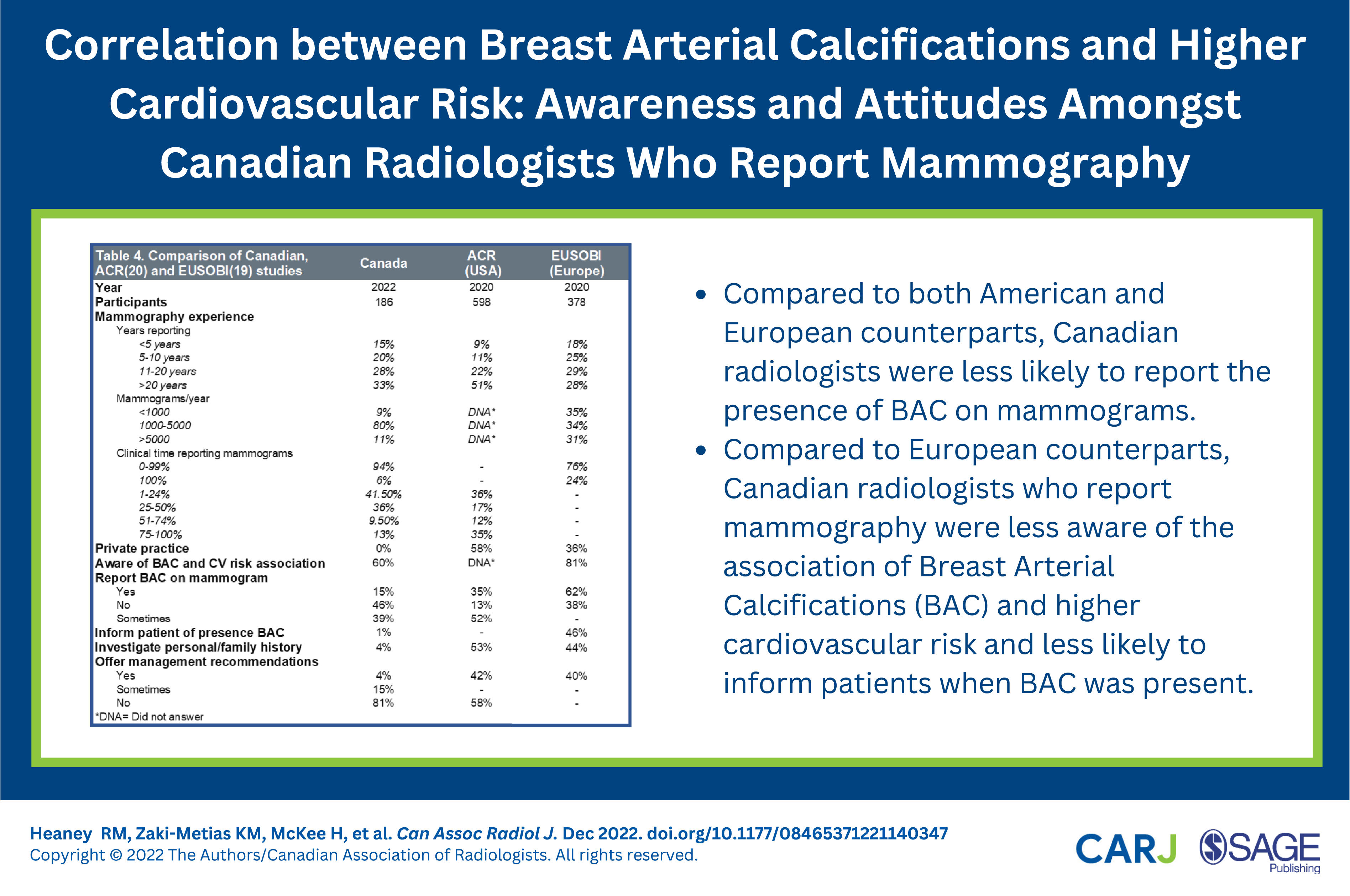
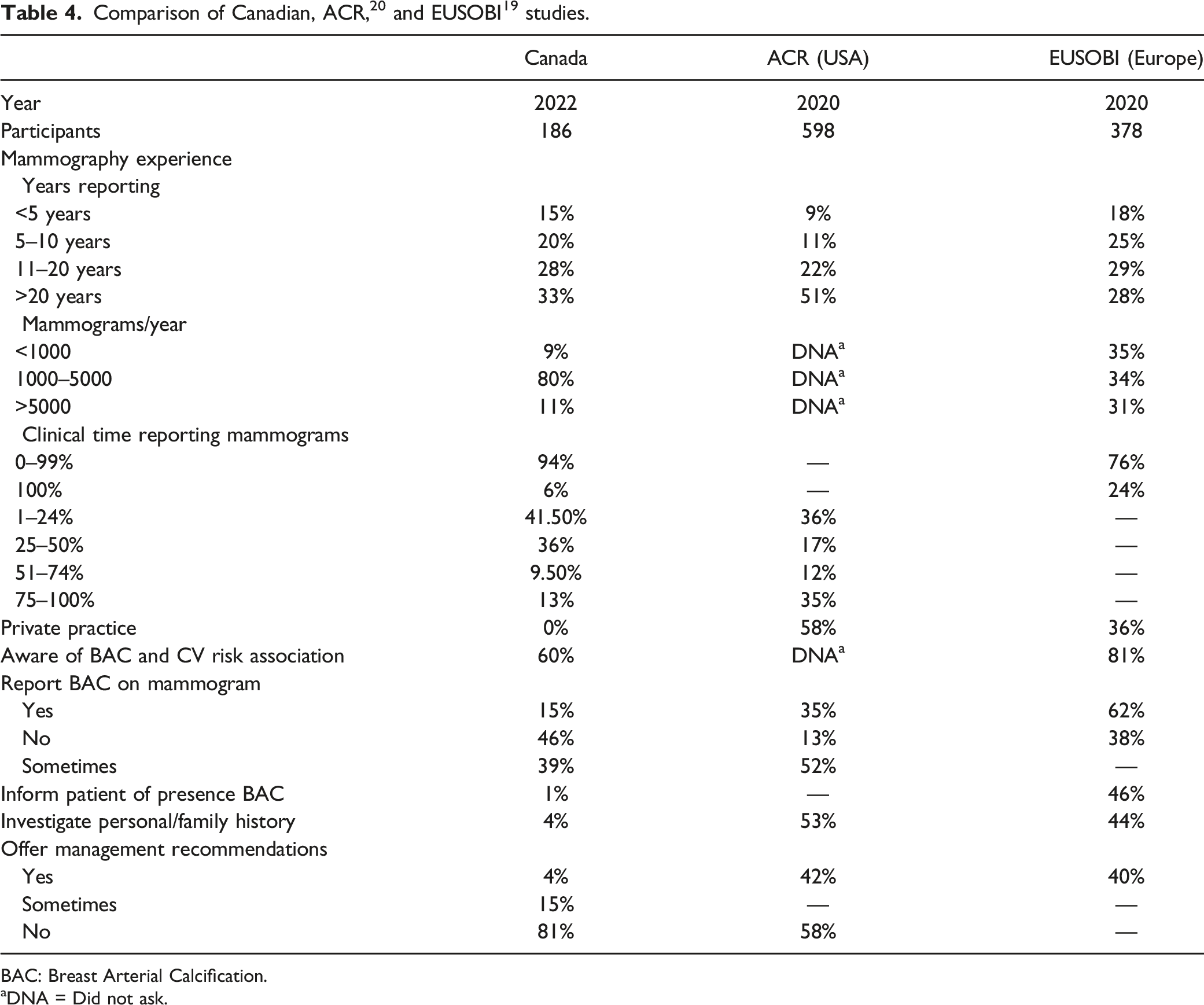
There have been two recent similar studies published in the literature that assessed the experience and perceptions of the members of the European Society of Breast Imaging (EUSOBI) 19 and American College of Radiology (ACR) 20 with regards to BAC reporting (Table 4). Our results demonstrate that Canadian radiologists who report mammography are less aware of the association between BAC and cardiovascular risk compared to European radiologists, less likely to report the presence of BAC compared to both European and American radiologists, and less likely to inform the patient of the presence of BAC on mammography compared to European radiologists. They are also less likely to provide management recommendations for the referring physicians compared to European and American radiologists.
One of the main reasons for not reporting BAC cited by Canadian radiologists in our study is the lack of clarity and data on the strength of the predictive link between the presence of BAC and adverse cardiovascular outcomes. Much of the published research to date details the relationship between BAC and CAC on non-cardiac chest CT 17 with varying strength of correlation with cardiovascular events and outcomes. However, recent results from the MINERVA study (Multiethnic Study of Breast Arterial Calcium Gradation and Cardiovascular Disease) involving 5,059 women in Northern California, demonstrated that the presence of BAC on mammography is associated with increased risk of atherosclerotic cardiovascular disease (ASCVD) events (such as acute myocardial infarction, ischemic stroke and CVD death), and global CVD. 23 This study, however, included women in the 60–79 age range only and not the younger population in whom Canadian radiologists are more likely to report the presence of BAC, based on our study results. Additionally, mean follow-up duration in this MINERVA study was relatively short at 6.5 years. It is clear that studies involving younger patient cohorts and longer follow-up periods are needed to establish the outcome benefit of reporting BAC. A prospective study using CAC scoring on cardiac gated CT would also likely be of benefit.
Similar to our American counterparts, there is no consensus on whether BAC reporting should be standard practice among Canadian radiologists who report mammography. 20 As evidence linking the presence of BAC and increased likelihood of incident ASCVD continues to emerge, we feel that reporting of BAC should become a requirement, comparable to the manner in which breast density notification has been introduced across Canada since 2018, 24 with some variation in implementation between the provinces. Similar to concerns about the public effect of breast density notification reported in the Canadian Medical Association Journal in 2020, 25 the impact of mandatory reporting of BAC should also be considered. Without involvement of primary care physicians and cardiologists, as well as standardized management recommendations, BAC reporting could potentially increase the burden on an already stretched healthcare system, as well as cause unnecessary patient anxiety.
The standard reporting template of many provincial breast screening programs does not facilitate reporting of BAC and several of the radiologists in our study considered this to be a barrier. Modification of the provincial screening forms would be a relatively easy and realistic first step in promoting BAC reporting. Our study showed that over 80% of participating Canadian radiologists seek national guidelines on the topic. As part of these guidelines, our study respondents indicated that they want to know what age qualifies as a “young” patient and what is “significant” or appropriate grading of BAC. In the literature, “younger” screening populations are often defined as 39–59 years of age.
17
Another barrier to introducing standardized BAC reporting is how it should be reported or described. Does a description of the presence vs absence of BAC suffice, or should attempts be made to grade severity or quantify BAC? A semiquantitative visual scale of mild, moderate, and severe has been recommended by cardiologists,
26
but the incremental benefit of BAC quantification is not clear. The MINERVA group has adopted a densitometry method to calculate a continuous BAC mass in milligrams using locally developed software.
27
It is imperative that the chosen descriptor or quantification method be feasible for use in both the screening and diagnostic environments to prevent workflow disruption. By way of example, we include a qualitative BAC grading system that has been published in the literature
13
with suggested wording for mammogram reports, recently endorsed by the CSBI (Figure 3). Grading of breast arterial calcifications
13
: Grade 0: No vascular calcification. Grade 1: Few punctate vascular calcifications, without coarse, tram-track, or ring calcifications. Grade 2: Coarse vascular calcification or tram-track calcification in fewer than three vessels. Grade 3: Severe, coarse, or tram track calcifications affecting three or more vessels. Suggested script: There are severe coarse vascular or tram track calcifications affecting three or more vessels in the breasts (Grade 3). A strong association between breast arterial calcifications and cardiovascular disease has been identified in multiple studies. Consider correlation with cardiovascular risk factors as clinically indicated.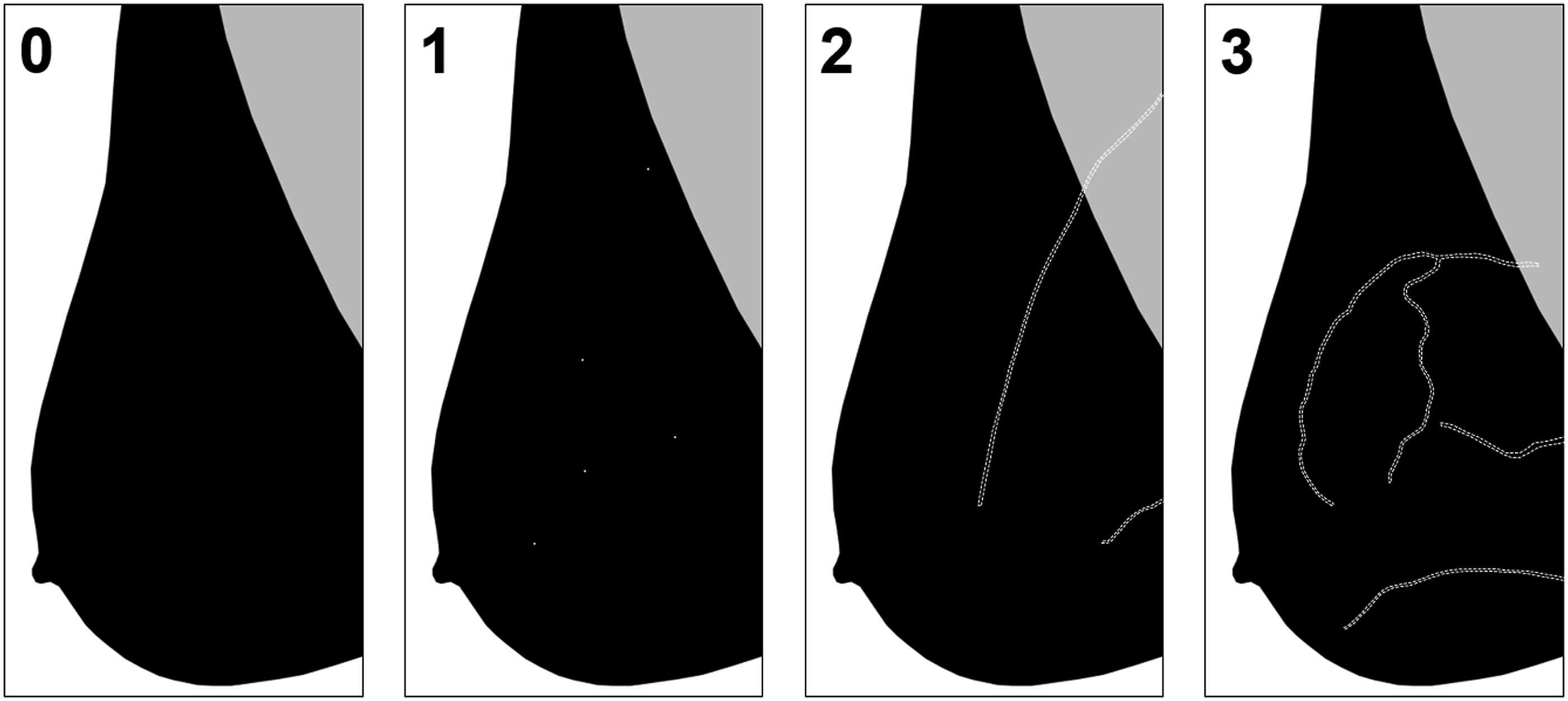
Guidelines on management recommendations directed towards the referring physician was another unmet need indicated by participating radiologists in our survey. Polonsky et al. recommended that the presence of BAC should prompt a comprehensive assessment of the patient’s lifestyle and cardiovascular risk factors by the referring clinicians, with initiation of medication as indicated in existing guidelines. 26 In addition, they recommend that if the threshold to commence statin therapy is not met, then a formal CAC score could be performed. 26 The recent publication from the MINERVA group also suggests that BAC should be interpreted in conjunction with the patient’s traditional cardiovascular risk factors, that those at borderline or intermediate risk of ASCVD may benefit from aggressive treatment, and that treatment escalation should be considered in women already deemed to be high risk. 23 Furthermore, it has been suggested that mammogram reports should include a statement in fine print noting the association between BAC and CAC, and detailing the aforementioned management advice. 11 In general, detection of BAC on mammography should prompt cardiovascular risk assessment, lifestyle modification to reduce CVD risk, possibly a calcium score CT to calculate CAC, and optimal medical management with lipid lowering agents guided by the CAC score.14,17 Breast arterial calcification as a CVD screening tool should be used to identify apparently healthy women with subclinical disease and higher CVD risk but not to rule it out. Absence of BAC on mammograms does not necessarily confer low risk, especially among older women, as the CVD prevalence increases and negative predictive value decreases. 14
Lastly, one must consider the patient’s perspective. Margolies et al. surveyed consecutive patients undergoing mammography of which 96% wanted to be informed of the presence of BAC directly, and not simply mentioned in the report to their providers. 22 Seventy-five percent of those surveyed reported that they would act on this information including: diet and lifestyle modification, commencing prescription medication, and undergoing coronary artery CT. In ambulatory patients, incidental but important findings may be overlooked by referring clinicians if not specifically flagged. 28 Patient notification of BAC, in a similar fashion to standardized reporting of breast density in many provinces, would mitigate this potential problem and empower patients to modify their lifestyle and other cardiovascular risk factors.
We acknowledge several limitations. Our study is subject to selection and response bias, as with any survey study. Attempts were made to reduce selection bias by the wide distribution of the survey via provincial and national radiology associations in order to include non-dedicated breast imagers. The survey was anonymized to minimize the effect of response bias. Due to the method of distribution, we are unable to accurately ascertain how many radiologists received the survey and what the response rate was. We estimate a response rate of 46% (186/402) based on a population of 3000 radiologists in Canada, 402 of whom are known to report mammography in a previous survey. 29
In conclusion, Canadian radiologists reporting mammography are less aware of the association between BAC and increased cardiovascular risk than their European and American counterparts, and are less likely to document the presence of BAC or provide management recommendations. Given the correlation of BAC with increased cardiovascular event risk, there is need for increased awareness as well as national BAC reporting guidelines.
Supplemental Material
Supplemental Material - Correlation Between Breast Arterial Calcifications and Higher Cardiovascular Risk: Awareness and Attitudes Amongst Canadian Radiologists Who Report Mammography
Supplementary Material for Correlation Between Breast Arterial Calcifications and Higher Cardiovascular Risk: Awareness and Attitudes Amongst Canadian Radiologists Who Report Mammography by Roisin M. Heaney, Kaitlin M. Zaki-Metias, Hayley McKee, Huijuan Wang, Barakat Ogunde, Charlotte J. Yong-Hing, Vivianne Freitas, Sandeep Ghai, Jean M. Seely, and Elsie T. Nguyen in Canadian Association of Radiologists Journal.
Footnotes
Acknowledgments
We thank the Canadian Society of Breast Imaging for their collaboration and endorsement of the survey. We would like to recognize the Canadian Association of Radiologists, Ontario Association of Radiologists, British Columbia Radiological Society, Société de Radiologie du Québec, Alberta Society of Radiologists, and Canadian Radiology Women for distribution and promotion of the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.