
Abstract
This is a visual representation of the abstract.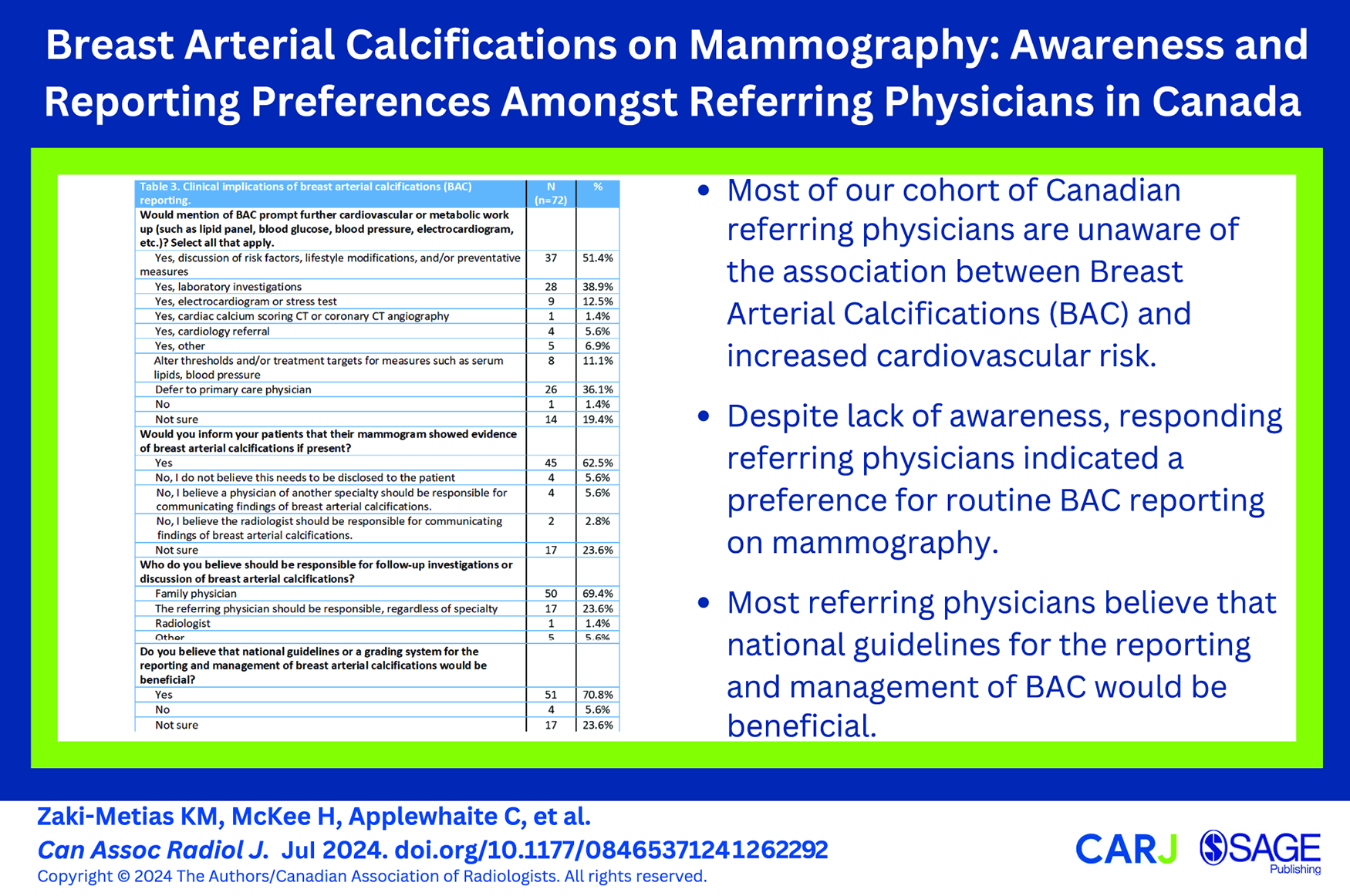
Introduction
Breast arterial calcifications (BAC) on mammography have been a topic of increasing discussion pertaining to opportunistic screening for atherosclerotic cardiovascular disease (ASCVD) in asymptomatic patients using mammography. BAC are commonly encountered on both screening and diagnostic mammograms and are identified in 12% to 42.5% of patients undergoing mammography; incidence of BAC increases with age.1,2 Several studies have demonstrated an independent association between BAC, increased cardiovascular risk, and ASCVD.1,3-7 BAC have also been positively correlated with coronary artery calcium (CAC) scores on non-contrast computed tomography (CT), angiographic coronary arterial stenosis, metabolic syndrome, and the progression of coronary atherosclerotic disease, among other related cardiovascular risk factors.1,8-12 However, despite their prevalence, reporting of BAC is not standard practice nor recommended by any guideline.
The utility of BAC as cardiovascular risk marker is most relevant in women under the age of 60. 13 Reporting of BAC on mammography may prove a useful opportunistic screening tool to identify those at increased cardiovascular risk, given that just over half of eligible Canadians aged 50 to 69 undergo regular screening mammography.14,15 This presents a unique opportunity for radiologists to provide additional insight into an individual’s cardiovascular risk, which may aid in prevention of adverse cardiovascular events by facilitating lifestyle modification, further investigation, or initiation or escalation of care.
Recent studies surveying radiologists have found that awareness of BAC is heterogeneous, and most radiologists do not directly inform patients of the presence or significance of BAC.16-19 Furthermore, patient surveys show that patients prefer to be informed of BAC, and that BAC reporting encourages active participation in cardiovascular risk mitigation strategies.20,21 While several studies have investigated the awareness and preferences of radiologists and patients pertaining to the reporting of BAC, only one such American study has been conducted to assess referring physicians’ perception and awareness of BAC. 22
We hypothesize that most referring physicians in Canada are currently unaware of the correlation and clinical implications of BAC and cardiovascular risk. The purpose of this study is to evaluate the awareness of the clinical significance of BAC amongst referring physicians in Canada. We also sought to identify preferences of BAC reporting on mammography, if such reporting is perceived to result in any further investigations or intervention, and the potential utility of BAC reporting and management guidelines.
Methods
This study was a survey of non-radiologist physicians who request or review the results of mammography in Canada. The target audience included family physicians, medical oncologists, surgical oncologists, radiation oncologists, internal medicine physicians, and general surgeons. Because in Canada gynaecologists do not typically order breast imaging, they were not included in the survey. Ethical approval was obtained from a Canadian academic institution.
Survey Development
A 15-question non-randomized survey was created and distributed in English and French using the secure online survey software platform SurveyMonkey. A consent form to participate in the survey and collect anonymous responses preceded the survey. No personal or identifying information was collected. The survey (Appendix) consisted of 2 parts: the first part gathered demographic information including the respondent’s specialty, current role, province of practice, practice setting, years in practice, and if they requested or reviewed the results of mammography in their practice. Physicians who indicated they did not request mammograms or review mammography results were taken to the end of the survey and were excluded from further analysis. Likewise, radiologists who inadvertently received and completed the survey were excluded given the focus on referring physician preferences.
The second part of the survey assessed respondents’ prior awareness of the association between BAC and increased cardiovascular risk, their preferences on BAC reporting in mammography, and whether quantification or a BAC grading system would be of benefit. Subsequent questions assessed physicians’ inclination to further assess and inform patients with reported BAC on mammography, who should be responsible for disclosing and discussing the presence of BAC with patients, and opinions on the utility of national BAC reporting and management guidelines. A comment box was provided for any further remarks.
Survey Distribution
The survey was distributed via several methods in both English and French. An email containing the survey link was sent to the mailing lists of the Canadian Society of Breast Imaging, BC Women’s Hospital and Health Centre, Doctors of British Columbia, Breast Health Centre (Manitoba), and CancerCare Manitoba. The survey was also distributed via newsletters sent to members of the Canadian Association of General Surgeons, Canadian Society of Surgical Oncology, Canadian Society of Internal Medicine, and Manitoba College of Family Physicians. The initial email or newsletter posting included a brief description of the study and the target audience with a link to access the survey. The survey was further shared via social media. Survey responses were collected over a 10-week period from February 14th, 2023 to April 30th, 2023. Reminder emails, newsletters, and social media posts were distributed at 4-week intervals prior to closure of the survey.
Statistical Analysis
The survey responses were recorded on a secure database. Descriptive statistics were used to summarize demographics and responses. Categorical variables were reported using frequency distributions and percentages. STATA v.16 software (StataCorp LLC, College Station, TX) was used for statistical analyses. Univariate logistic regression models were created to assess 5 specific BAC questions for each of the following independent variables, determined a priori; community versus academic physicians, number of years in practice (<5, 5-10, 11-15, 16-20, ≥20 years), specialty (family medicine, medical oncology, radiation oncology), surgical specialties (general surgery and surgical oncology), and other medical specialties (internal medicine and cardiology). Multivariate logistic regression models were created to assess 2 specific BAC questions, controlling for the same independent variables; academic versus non-academic physicians, number of years in practice (≤10, >10 years), specialty (family medicine), surgical specialties (general surgery, surgical oncology), and other medical specialties (internal medicine, cardiology, medical oncology, radiation oncology). All independent variables were examined for collinearity using Pearson’s rank coefficient (defined as >|0.8|), evaluated for confounding (defined as a 30% change in coefficients on removal of the variable), and tested for significance of pairwise interactions (defined as P < .05). No independent variables met these criteria.
Results
Over the 10-week period, 103 survey responses were received. Given the nature of distribution of the survey link via physician organizations and social media, the total number of physicians who received the survey is not known. Of the 103 responses, 31 were excluded; 20 of these respondents were radiologists, 8 respondents did not request mammography or review mammogram results, and 3 had incomplete responses. Seventy-two complete responses were included in the analysis.
Demographics
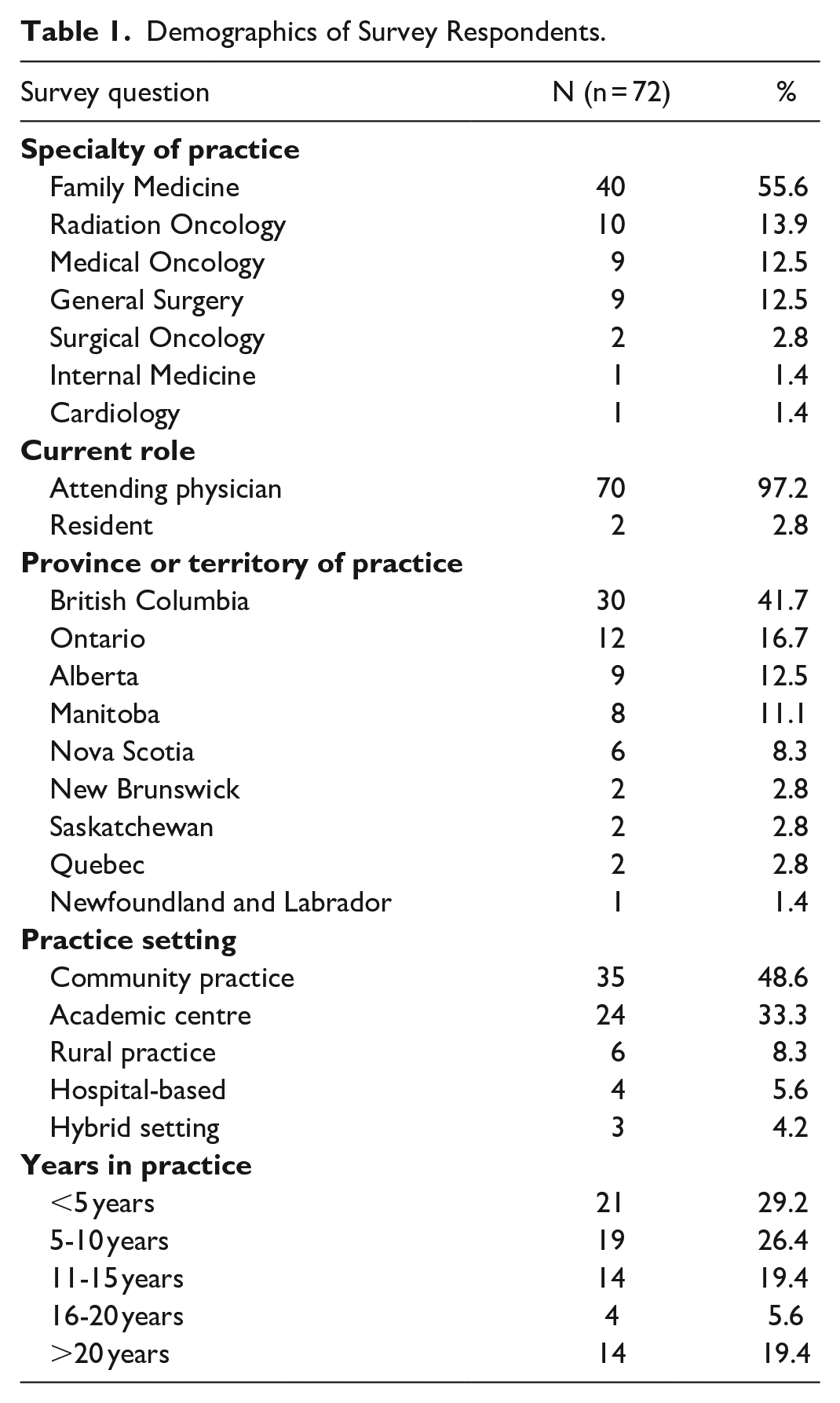
A total of 55.6% (40/72) of respondents were family physicians, 13.9% (10/72) radiation oncologists, 12.5% (9/72) medical oncologists, 12.5% (9/72) general surgeons, 2.7% (2/72) surgical oncologists, 1.4% (1/72) internal medicine physicians, and 1.4% (1/72) cardiologists (Figure 1). Most respondents were attending physicians (70/72; 97.2%). Physicians from British Columbia made up the largest number of participants (30/72; 41.7%), followed by Ontario (12/72; 16.7%; Figure 2). Community practice was the predominant practice setting amongst participating physicians, accounting for nearly half of responses (33/72; 48.6%; Figure 3), although there was a relatively widespread distribution of physician experience as indicated by years in practice. A detailed breakdown of demographic responses is presented in Table 1.
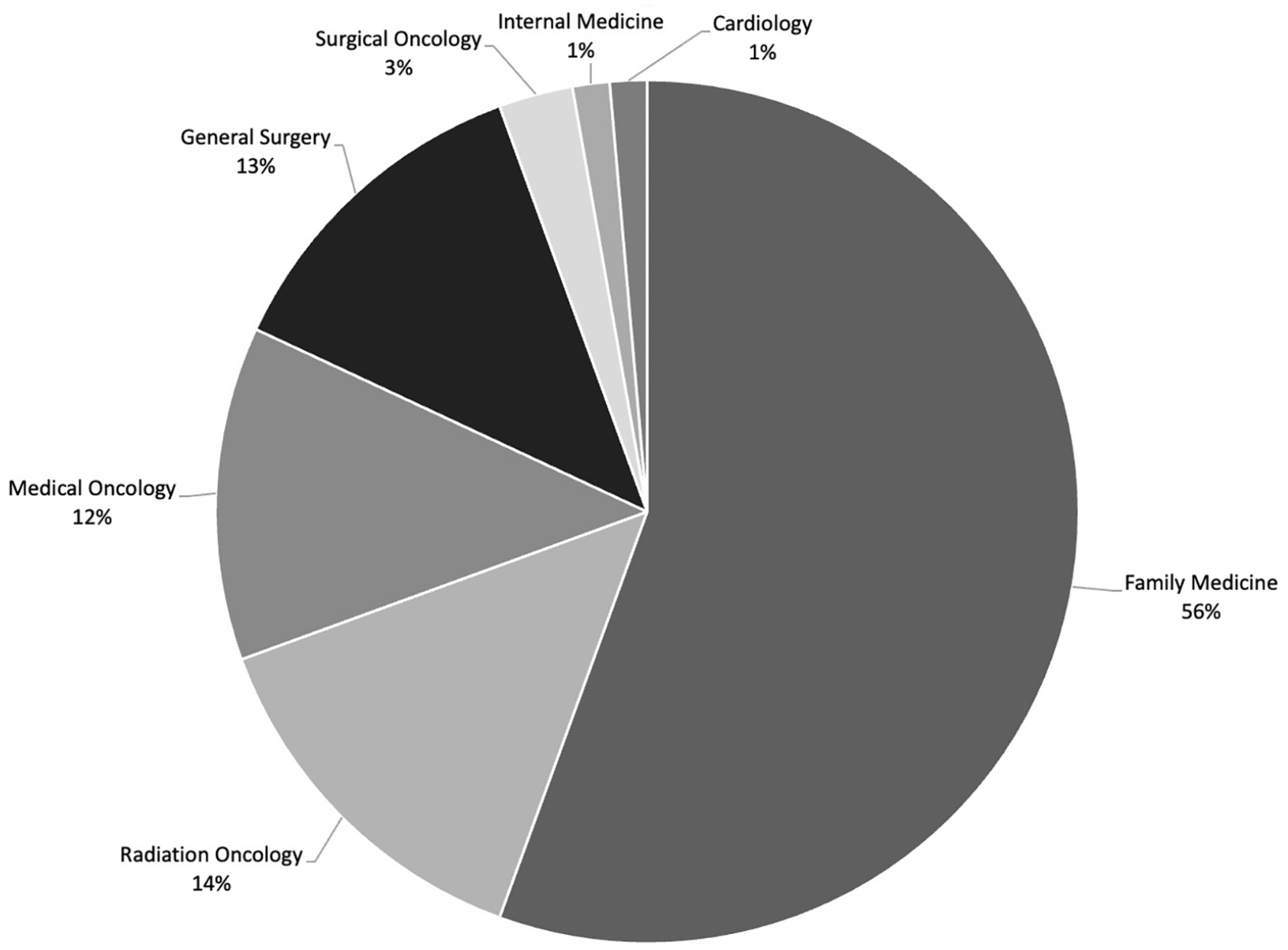
Breakdown of survey respondents’ specialty of practice.
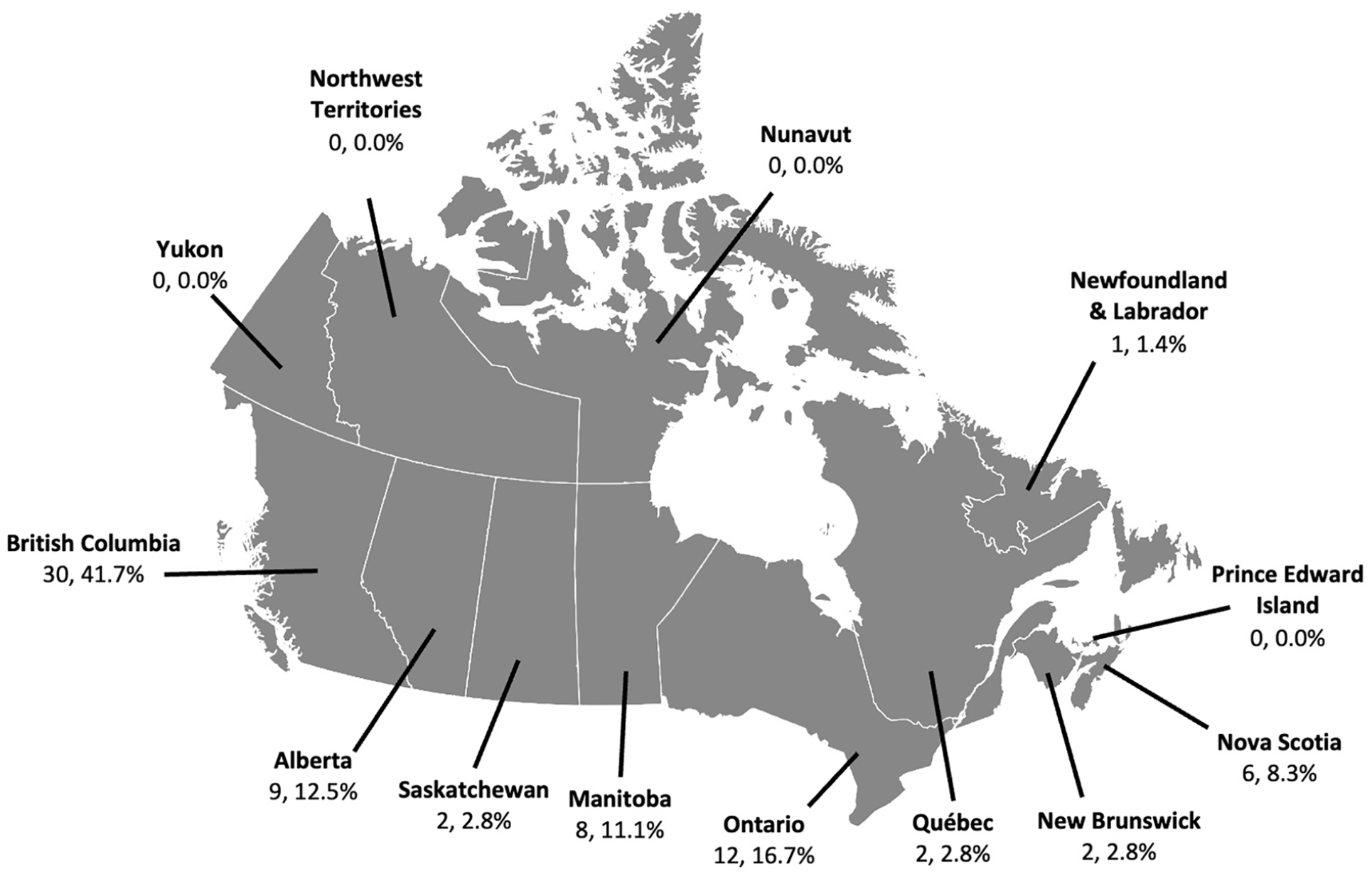
Location of survey respondents per Canadian province.
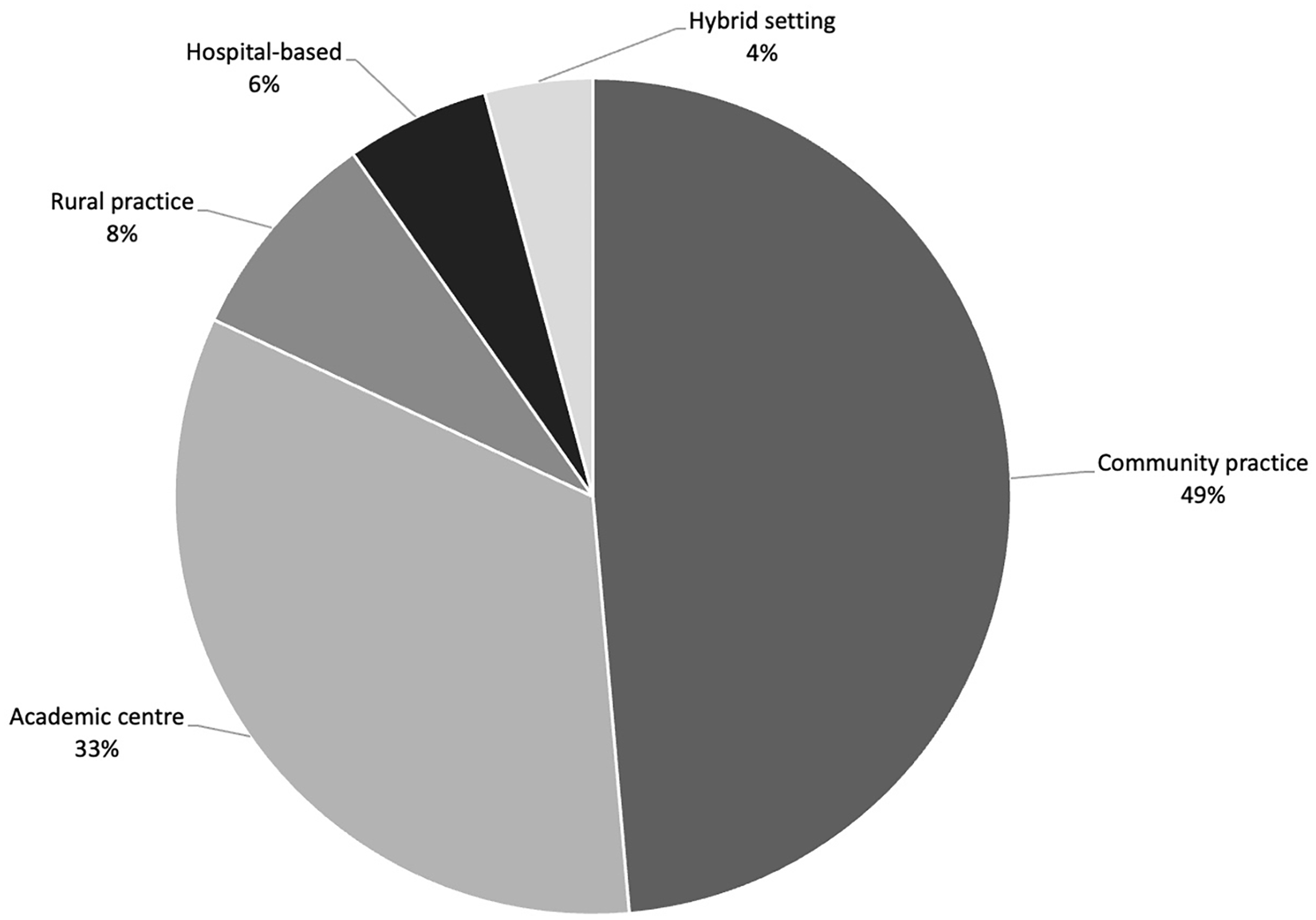
Breakdown of survey respondents’ practice setting.
Demographics of Survey Respondents.
Awareness and Reporting Preferences of BAC
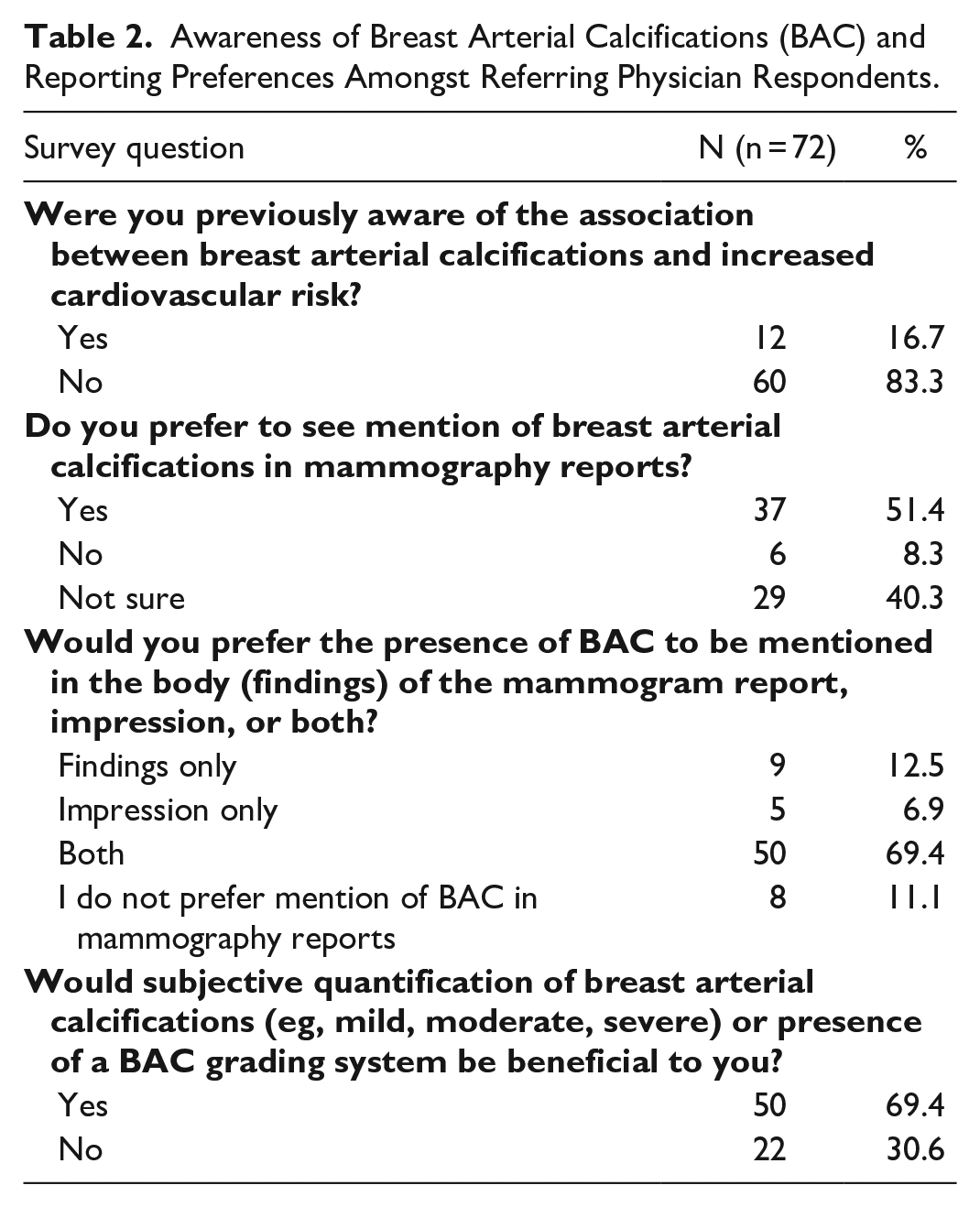
Twelve referring physician respondents (12/72; 12.6%) were previously aware of the association between BAC and increased cardiovascular risk. All responding physicians with 11 to 20 years of practice experience were unaware of the association between BAC and increased cardiovascular risk (18/72; 25%). Respondents in surgical specialties were more likely to be aware of the association between BAC and increased cardiovascular risk compared to family physicians on univariate analysis (OR 7.05, CI 1.29-38.62, P = .024) and on multivariate analysis after controlling for specialty, number of years in practice, and practice setting (OR 9.3, CI 1.57-55.6, P = .01).
Just over half (37/72; 51.4%) of respondents indicated that they would prefer to see BAC reported on mammography, with the majority (50/72; 69.4%) indicating that subjective quantification (eg, mild, moderate, severe) or a BAC grading system would be beneficial to them. Respondents in academic centres (24/72; 33.3%) were less likely to report that subjective quantification or a BAC grading system would be beneficial, compared to those in community settings 35/72; 48.6%) on univariate analysis (OR 0.175, CI 0.05-0.58, P = .004). Compared to family physicians (40/72; 55.6%), radiation oncologists (10/72; 13.9%; OR 0.12, CI 0.03-0.55, P = .006) and surgical specialists (11/72; 15.3%; OR 0.10, CI 0.02-0.45, P = .003) were also less likely to find subjective quantification of BAC beneficial on univariate analysis. The cardiologist and internist (2/72; 2.8%) responded that such quantification would be useful. A detailed breakdown of survey responses pertaining to awareness and reporting preferences of BAC on mammography is presented in Table 2.
Awareness of Breast Arterial Calcifications (BAC) and Reporting Preferences Amongst Referring Physician Respondents.
Clinical Implications of BAC Reporting
Thirty-one of the 72 participating physicians (43.1%) indicated that the mention of BAC in a mammogram report would prompt further action, ranging from a discussion of risk factors and lifestyle modification to laboratory investigations and cardiovascular assessment to cardiology referral. Medical oncologists (OR 0.13, CI 0.03-0.61, P = .010), radiation oncologists (OR 0.11, CI 0.02-0.51, P = .005), and surgeons (OR 0.06, CI 0.01-0.31, P = .001) were less likely to respond that mention of BAC would prompt further assessment, compared to family physicians on univariate analysis. Furthermore, respondents from academic centres were also less likely to respond that mention of BAC would prompt further workup, compared to physicians in the community setting on univariate analysis (OR 0.12, CI 0.03-0.38, P < .001). Table 3 displays detailed survey responses pertaining to the clinical implications of BAC reporting on mammography.
Clinical Implications of Breast Arterial Calcifications (BAC) Reporting.
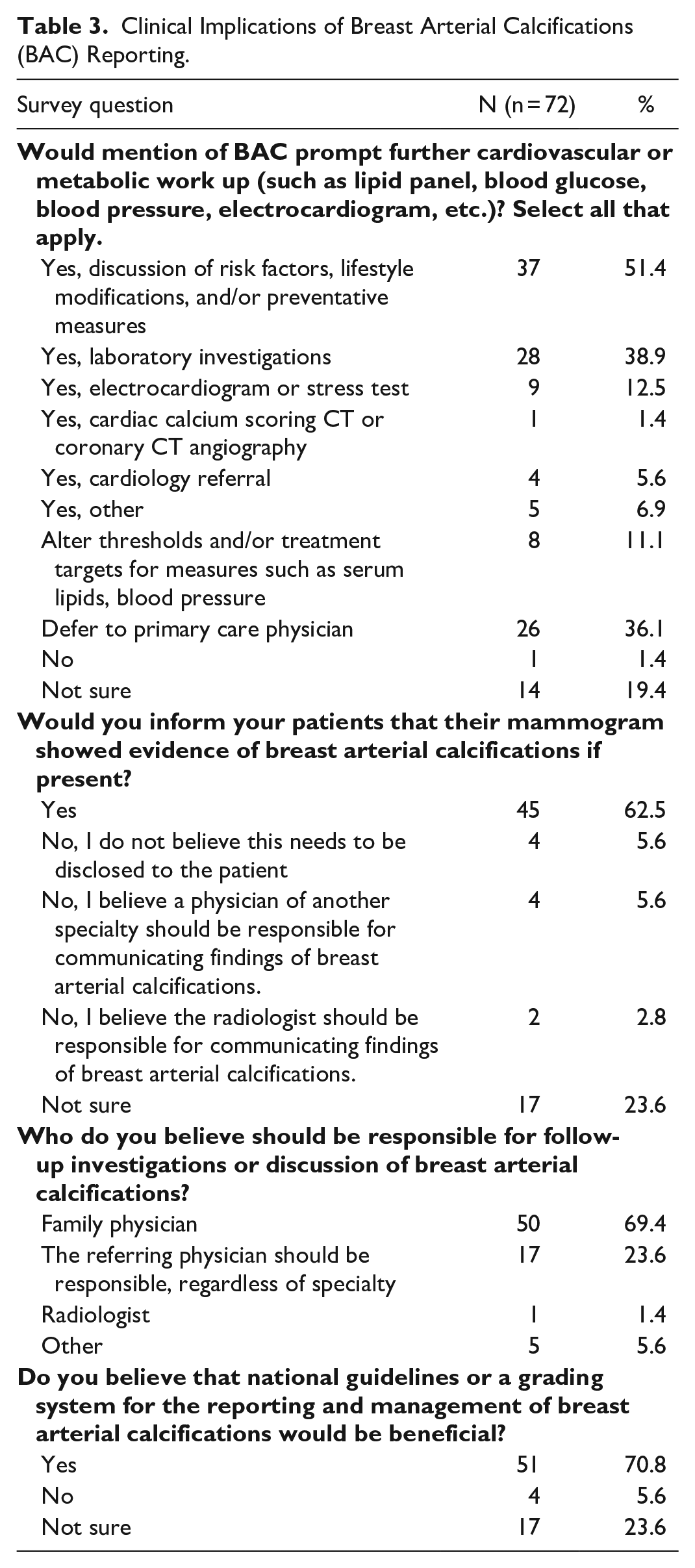
Greater than half of responding physicians (45/72, 62.5%) stated that they would inform their patients if their mammogram showed evidence of BAC. The majority of respondents (50/72, 69.4%) stated that a patient’s family physician should be responsible for disclosing and discussing the presence and implications of BAC with patients, although, 23.6% (17/72) of respondents believe that this duty should fall to the physician who referred the patient for mammography. Univariate analysis revealed that physicians at academic centres were less likely to respond that they would inform their patients that their mammogram showed evidence of BAC compared to respondents in community settings (OR 0.25, CI 0.08-0.75, P = .014). Several respondents left comments in the provided free-text box suggesting a multidisciplinary approach, with the referring physician disclosing the presence of BAC, and follow-up investigations contributed by all members of the patient’s healthcare team.
Over two-thirds (51/72, 70.8%) of responding physicians stated that national guidelines on the reporting and management of BAC would be useful. Family physicians were most likely to agree with this statement. Surgeons were less likely to concur, compared to family physicians, on univariate analysis (OR 0.08, CI 0.02-0.38, P = .001) and multivariate analysis, after controlling for specialty, number of years in practice and practice setting (OR 0.10, CI 0.02-0.49, P = .005). The cardiologist (n = 1) and internist (n = 1) both believed that such guidelines would be beneficial.
Qualitative Survey Responses
Free-text comments demonstrated an overall interest in the topic of BAC and cardiovascular risk. One respondent remarked that risk factors for cardiovascular disease overlap significantly with those for breast cancer and other common malignancies, and that an emphasis on and prioritization of prevention would benefit not only those at cardiovascular risk but also those at risk for breast and other malignancies. However, clear communication and differentiation between BAC and breast microcalcifications suspicious for malignancy is critical to ensure that there is no confusion or undue concern for calcifications resulting from breast cancer. One medical oncologist indicated that BAC reporting would spur more thorough investigation into cardiovascular history and risk stratification for patients on certain chemotherapeutic agents.
Discussion
Cardiovascular disease is the second leading cause of premature death in Canadian women, second to breast cancer in women under the age of 55 and lung cancer in women over the age of 55. 23 Despite this, most Canadian women are unaware of their personal cardiovascular risk, and there are currently no recommendations for routine cardiovascular screening, unlike for breast and lung cancer.14,24 Traditional measures of cardiovascular risk such as the Framingham Risk Score often underestimate cardiovascular risk in women, and there is a demonstrated need for improved risk assessment and management, with inclusion of sex-specific factors. 25
The results of our survey of Canadian referring physicians found that most are unaware of the association between BAC and increased cardiovascular risk. Despite an overall lack of awareness, most participating referring physicians indicated a preference for BAC reporting and quantification. These results echo those of a 2021 Michigan-based survey study of referring physicians regarding the impact of BAC reporting on patient care, which demonstrated an overall preference for routine BAC reporting. 22 However, the surveyed cohort of Canadian physicians in academic settings were less likely to find BAC reporting useful relative to physicians in community practice, although this may represent a potential source of bias as only one family physician indicated an academic practice setting. Most surveyed physicians would discuss lifestyle modification, obtain laboratory investigations (such as serum lipid profile and haemoglobin A1c), and alter treatment thresholds or targets. This underscores the potential value in reporting of BAC on mammography, given the relatively cost-effective and non-invasive measures that physicians would likely pursue.
Most respondents specified that national guidelines would be beneficial, mirroring the opinions of Canadian radiologists. 17 Previous studies have suggested radiologists include a footnote on mammogram reports briefly outlining the association between BAC and cardiovascular risk with general advice on management. 26 The Canadian Society of Breast Imaging (CSBI) published the first BAC reporting guideline for radiologists in Canada in January 2023 (Figure 4). 27 The creation of reference guides for referring physicians and patient-facing brochures on BAC and cardiovascular risk may also provide additional support and aid in informed decision-making.
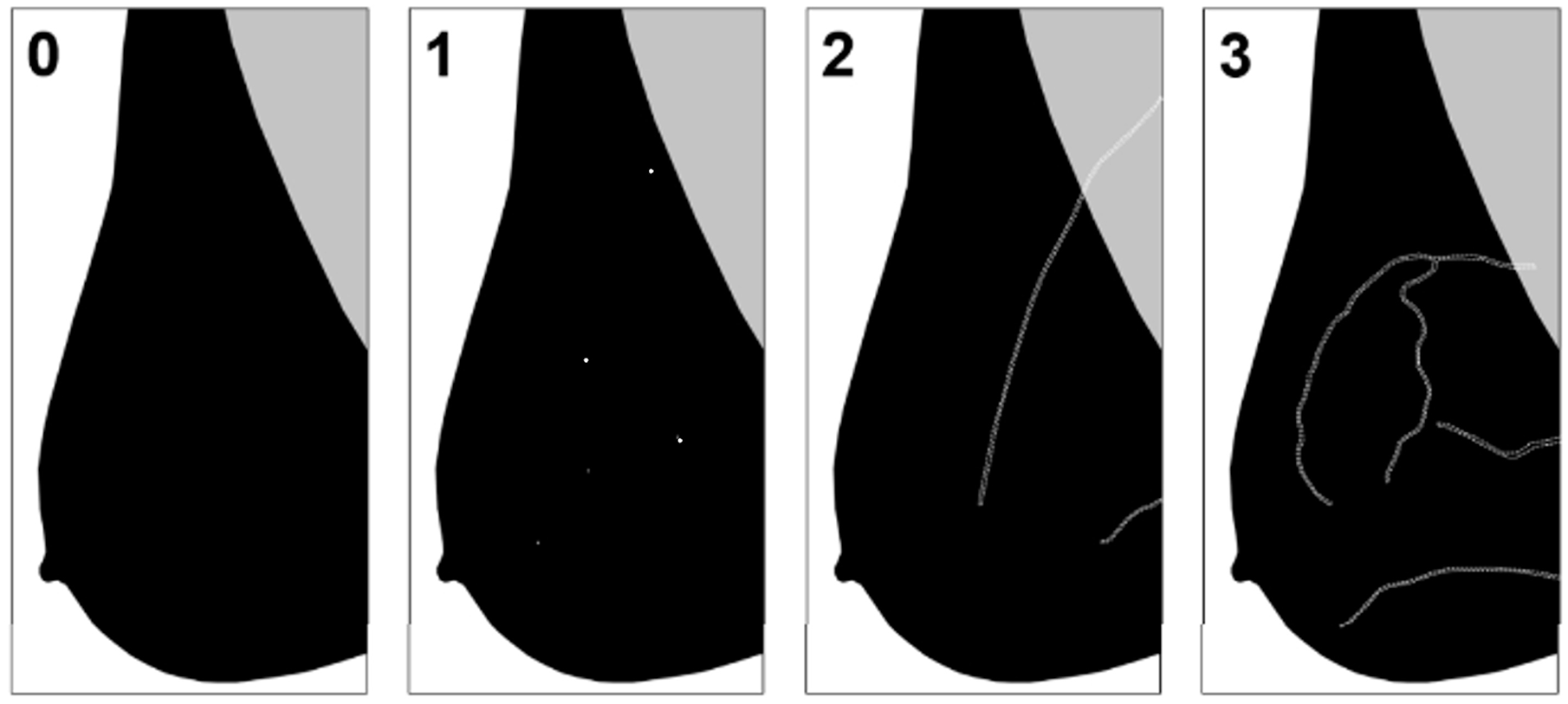
Grading of breast arterial calcifications17,27: Grade 0: No vascular calcification. Grade 1: Few punctate vascular calcifications, without coarse, tram-track, or ring calcifications. Grade 2: Coarse vascular calcification or tram-track calcification in fewer than 3 vessels. Grade 3: Severe, coarse, or tram track calcifications affecting 3 or more vessels.
Similar to their American counterparts, the majority of responding physicians would inform their patients of the presence of BAC, with most attributing this responsibility to either the patient’s family physician or the referring physician. This may cause further undue burden on family physicians, who will likely be expected to notify patients and guide subsequent management. This also has the potential to increase cardiology referrals and contribute to capacity issues. Given these factors, it is critical that BAC reporting and clinical management guidelines are created in collaboration with referring physicians, including family medicine and cardiology.
Another logistical barrier to BAC reporting pertains to patients who undergo screening mammography either by entering the provincial breast screening programmes or via self-referral without direct referral from a physician. In these cases, a lay letter conveying mammography results is sent directly to the patient. Incidental findings such as BAC may not be included in these letters, and, if they are, patients may present to their family physician for further guidance. While this may cause an added strain on family physicians and the healthcare system at large, up to 4.6 million Canadians are without a family doctor and may fall through the cracks. 28 Furthermore, incidental but potentially actionable findings are easily overlooked by referring physicians in the outpatient setting, which may present another obstacle to meaningful integration of BAC reporting on mammography. 29 Standardized reporting and direct patient notification, similar to practices in place for breast density, may circumvent these issues and promote patients to take ownership of their cardiovascular health. 17
Participating physicians expressed concerns that reporting of BAC would cause undue patient anxiety and an increased burden of administrative work on family physicians. Some physicians felt that they would still feel obligated to always notify patients with BAC (eg, if observed on an otherwise negative or benign mammogram who were already on primary or secondary preventative therapy for cardiovascular risk factors), even if they were not making meaningful changes to the care plan. Several additional comments highlighted the need for shared decision-making with patients, including a conversation on cardiovascular risk factors and risk mitigation. One physician also questioned if a patient’s age would be considered when reporting BAC on mammography, and if the degree of calcification would be expected for their age, as this would impact the physician’s decision to proceed with further investigation or risk management strategies.
The patient perspective must also be considered when determining the utility and feasibility of BAC reporting. Despite national campaigns, overall awareness of cardiovascular risk status in women remains low. Patient notification of BAC can allow for patient autonomy and empower women to become more actively involved in preventative measures and their overall cardiovascular health. 18 Patient surveys conducted in the United States suggest that an overwhelming majority of patients want to be notified of BAC and prompt more active participation in their preventative cardiovascular health.20,21 Educational materials such as brochures and online tools should be compiled to help patients better understand potential cardiovascular risk and prompt risk management discussions with their physician.
We acknowledge several limitations in our study. The significantly low response rate represents a small fraction of practicing physicians in Canada. We are unable to determine the true response rate, given the means of distribution and inability to ascertain how many referring physicians received the survey. Furthermore, not all physicians are members of the various associations who aided in survey distribution, and thus a proportion of our target audience may have been inadvertently excluded. Generalizability across various jurisdictions and practice settings is also a concern, given the larger proportion of respondents from British Columbia. However, despite these limitations, our results suggest that referring physicians prefer BAC reporting on mammography and would find value in national guidelines.
Future directions may include a more comprehensive analysis of the preferences of a focused group of physicians, for example, in a single provincial or territorial breast cancer screening programme, to determine the feasibility and repercussions of BAC reporting. Given the variability in eligibility for women aged 40 to 49 to participate in provincial and territorial screening programmes, BAC reporting presents an opportunity for earlier cardiovascular risk assessment in this age group in jurisdictions which encourage or allow screening mammography to begin at 40. Furthermore, the patient perspective of BAC reporting and implications has not yet been assessed in Canada and would provide valuable information on the utility of BAC reporting in the Canadian context.
Conclusion
Our cohort of Canadian referring physicians were largely unaware of the association between BAC and increased cardiovascular risk but prefer routine BAC reporting on mammography. Within the limitation of the number of responses, this suggests that the clinical importance is recognized and supports the need for education and BAC reporting and management guideline development. This may present the opportunity to capture a larger proportion of individuals with asymptomatic ASCVD through routine mammographic screening and introduce earlier intervention and preventative measures.
Footnotes
Appendix: Survey
Acknowledgements
We thank the Canadian Society of Breast Imaging for their collaboration and endorsement of the survey. We would like to recognize the Canadian Association of General Surgeons, Canadian Society of Surgical Oncology, Canadian Society of Internal Medicine, BC Women’s Hospital and Health Centre, Doctors of British Columbia, Breast Health Centre of Manitoba, CancerCare Manitoba, Doctors Manitoba, Manitoba College of Family Physicians, New Brunswick Medical Society, Newfoundland & Labrador Medical Association, Medical Society of Prince Edward Island, Rossy Cancer Network, Saskatchewan Medical Association, British Columbia College of Family Physicians, Women’s Health Research Institute for distribution and promotion of the survey.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kaitlin Zaki-Metias, Jean Seely, and Charlotte Yong-Hing served on the Canadian Society of Breast Imaging Board of Directors throughout the course of this study. Elsie Nguyen serves on the Canadian Society of Thoracic Radiology Executive Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.