
Abstract
Objectives
We sought to evaluate the association between patient sociodemographic status and breast screening volumes (BSVs) during the COVID-19 pandemic in a large, population-based breast screening program that serves a provincial population of over 5 million.
Results
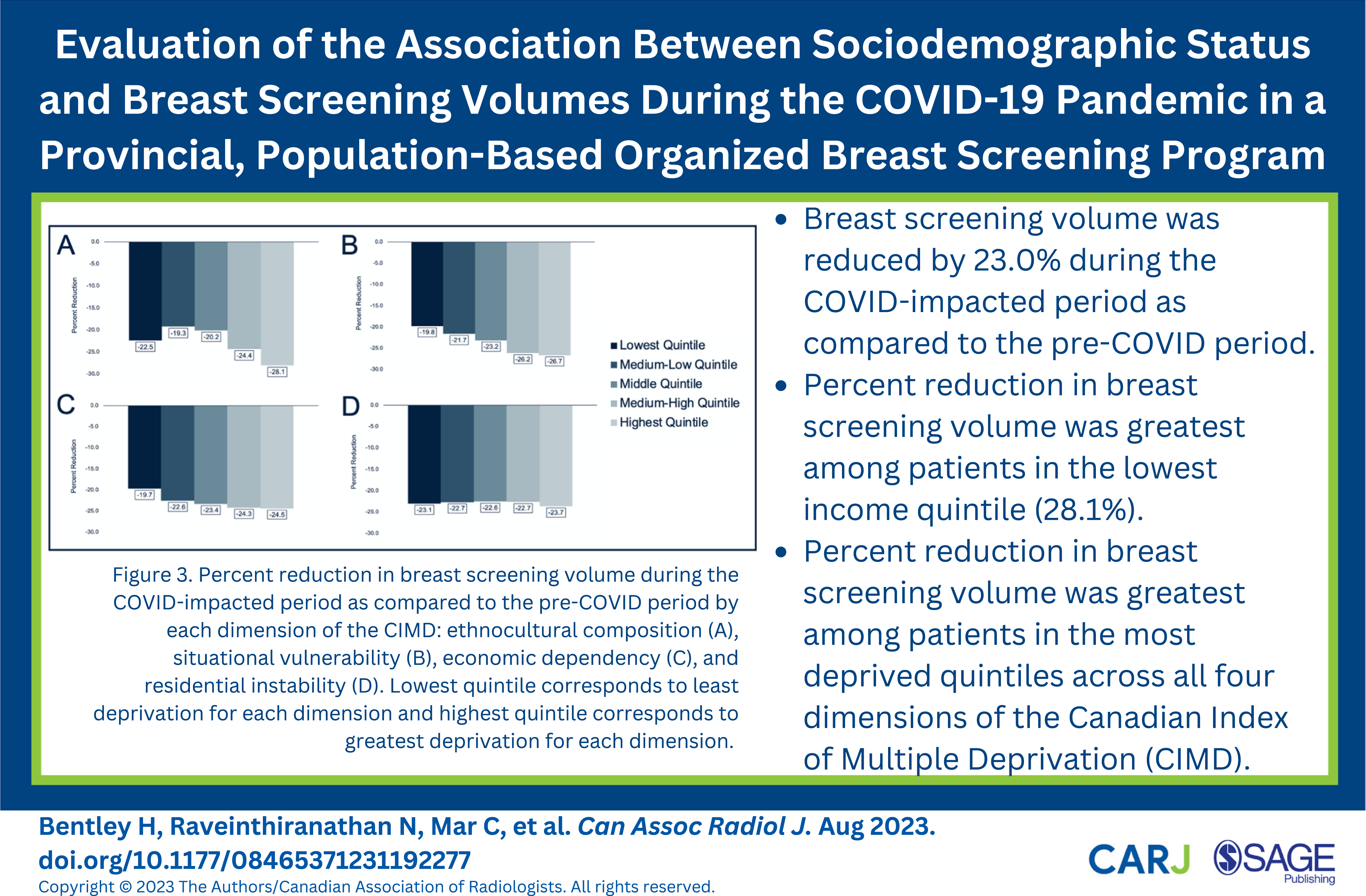
Overall BSV was reduced by 23.0% during the COVID-impacted period as compared to the pre-COVID period. Percent reductions in BSVs were greatest among younger patients aged 40 to 49 years (31.3%) and patients residing in communities with a population of less than 10,000 (27.0%). Percent reduction in BSV was greatest among patients in the lowest income quintile (28.1%). Percent reductions in BSVs were greatest for patients in the most deprived quintiles across all 4 dimensions of the CIMD.
Conclusion
Disproportionate reductions in BSVs were observed during the COVID-19 pandemic among younger patients, patients residing in rural communities, patients in lower income quintiles, and patients in the most deprived quintiles across all 4 dimensions of the CIMD.
Introduction
Throughout the world the COVID-19 pandemic has widely disrupted healthcare systems, including participation in secondary preventative healthcare measures, such as breast screening. At the onset of the COVID-19 pandemic organized breast screening programs were temporarily suspended or were put on hold following recommendations from several national organizations, including the American College of Radiology, 1 the Society of Breast Imaging, 2 and the Canadian Society of Breast Imaging. 3 In the subsequent weeks of an initial phased re-opening, breast screening volumes were limited to allow for the implementation of recommendations to mitigate the spread of COVID-19. 4,5 Consequently, such COVID-19-related disruptions to breast screening limited patients’ ability to participate in this important secondary preventative healthcare measure.
The adverse impacts of the COVID-19 pandemic on breast screening may be disproportionate. Variable participation in breast screening has been previously reported across various sociodemographic groups prior to the onset of the COVID-19 pandemic. 6 –9 Given the variable impact of the COVID-19 pandemic, particularly on vulnerable populations, 10 –13 such inequities in breast screening may be further manifested. Initial reports suggest that the COVID-19 pandemic may have further manifested inequities in breast screening among patients of Black, Hispanic and Asian race, 10,14 –16 and among patients of lower socioeconomic status. 17 Nonetheless, such reports are generally comprised of small, single-institution or insurance claims data.
We sought to evaluate the association between patient sociodemographic status and breast screening volumes during the COVID-19 pandemic in a large, population-based breast screening program that serves a provincial population of over 5 million. As secondary preventative healthcare measures, such as breast screening, remain integral to improved patient outcomes, evaluating the association of sociodemographic status on breast screening volumes during the COVID-19 pandemic is imperative to the development and deployment of targeted interventions to mitigate such identified inequities. 18
Methods
This was an observational historical cohort study. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 19 were followed. The UBC-BC Cancer institutional research ethics board approved this study (REB H20-02086).
Breast Screening Program
In British Columbia, Canada a large, population-based breast screening program, the BC Cancer Breast Screening Program, serves a provincial population of over 5 million and provides breast screening to patients who meet pre-established eligibility criteria. 20 Thirty-nine screening sites, including 3 mobile units, provide screening mammography services across the province, and are operated by local health authorities and community radiology clinics. The BC Cancer Breast Screening Program is publicly funded.
COVID-19-Related Disruptions
As previously described, on March 18th, 2020 all breast screening facilitated through the BC Cancer Breast Screening Program was suspended. 21 After a suspension of approximately 10.5 weeks on May 30th, 2020 breast screening sites throughout the province began a phased re-opening. This phased re-opening incorporated recommendations to mitigate the spread of COVID-19, 5 including social distancing, enhanced equipment cleaning, use of personal protective equipment, and implementation of COVID-19 symptom screening. 21
Data Sources and Cohort Derivation
The primary data source accessed was the population-based BC Cancer Breast Screening database, which contains patient, screen, and outcome information on all screening mammograms completed through the program. The database is regularly linked with the BC Vital Statistics death file to determine the vital status of patients eligible to participate in breast screening.
The study cohort consisted of all patients who completed breast screening between April 1st, 2017 and March 31st, 2021. An average of 3 consecutive annual periods between April 1st, 2017 and March 31st, 2020 was defined as the pre-COVID period to mitigate the effect of annual variation. The period between April 1st, 2020 and March 31st, 2021 was defined as the COVID-impacted period. Patients with missing, invalid, or non-British Columbia residential postal codes were excluded to facilitate geo-coding to area-based sociodemographic variables.
Study Parameters
Summary of Key Dimensions of the Canadian Index of Multiple Deprivation and Contributing Variables.
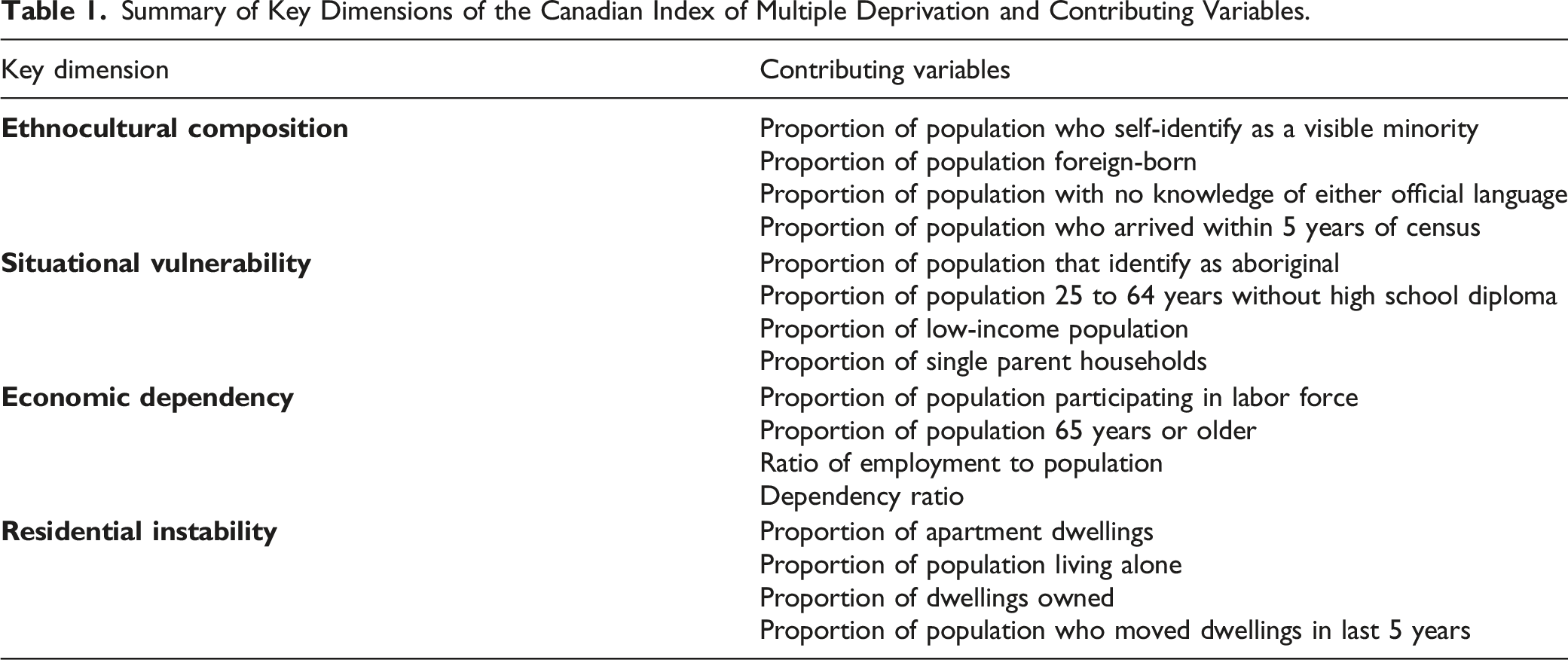
For each key dimension, factor scores for each dissemination area were constructed. Lower factor scores for each dissemination area corresponded to areas that were least marginalized while higher factor scores for each dissemination area corresponded to areas that were most marginalized. Factor scores were ordered from smallest to largest and were divided into quintiles, with quintile 1 being least deprived and quintile 5 being most deprived.
Statistical Analyses
Percent reductions in breast screening volumes during the COVID-impacted period were calculated and were compared to the pre-COVID period overall and for groups defined by sociodemographic variables.
Results
Overall breast screening volume was reduced by 23.0% during the COVID-impacted period with 197,015 breast screens completed during the COVID-impacted period as compared to 255,726 breast screens completed during the pre-COVID period. The percent reduction in breast screening volume during the COVID-impacted period was greatest among younger patients aged 40 to 49 years (31.3%) and least among patients aged 70 to 74 years (7.7%) (Figure 1). Percent reduction in breast screening volume during the COVID-impacted period as compared to the pre-COVID period by patient age.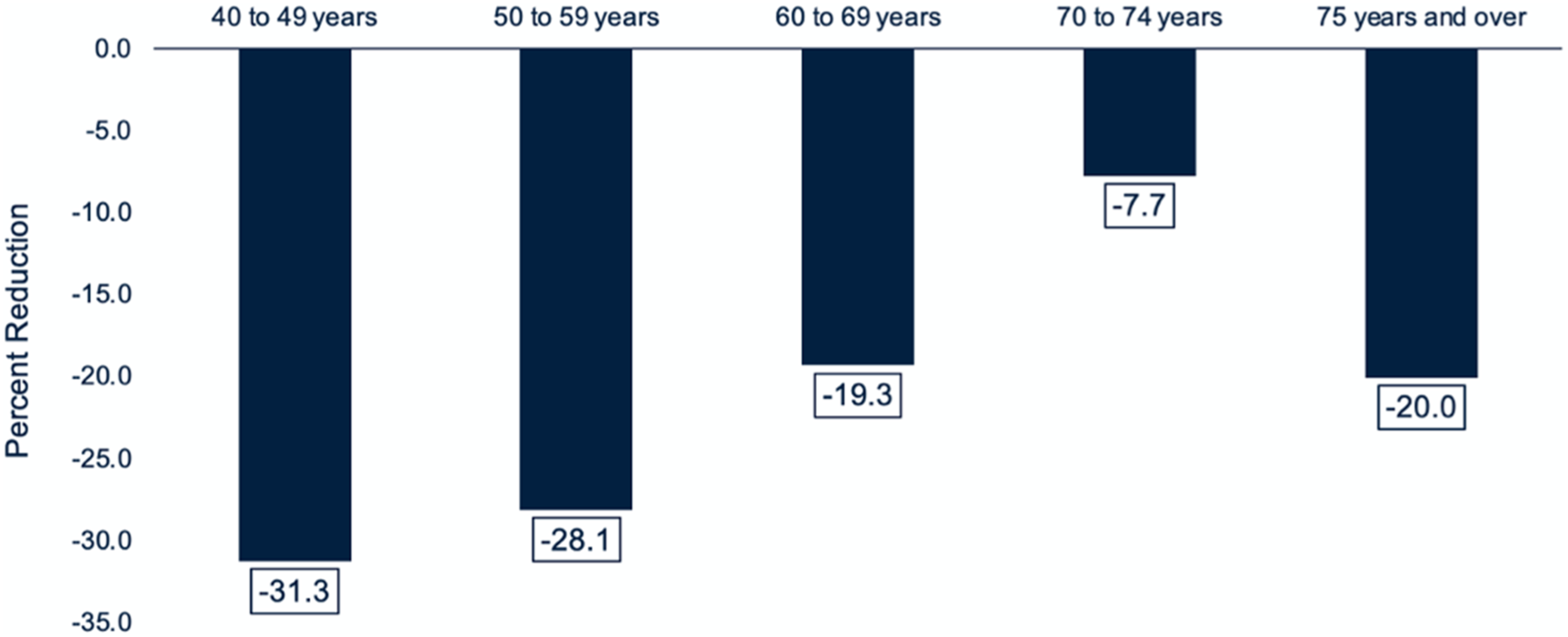
Percent Reduction in Breast Screening Volumes During the COVID-Impacted Period as Compared to the Pre-COVID Period by Screen History, Community Size, and Regional Health Authority.
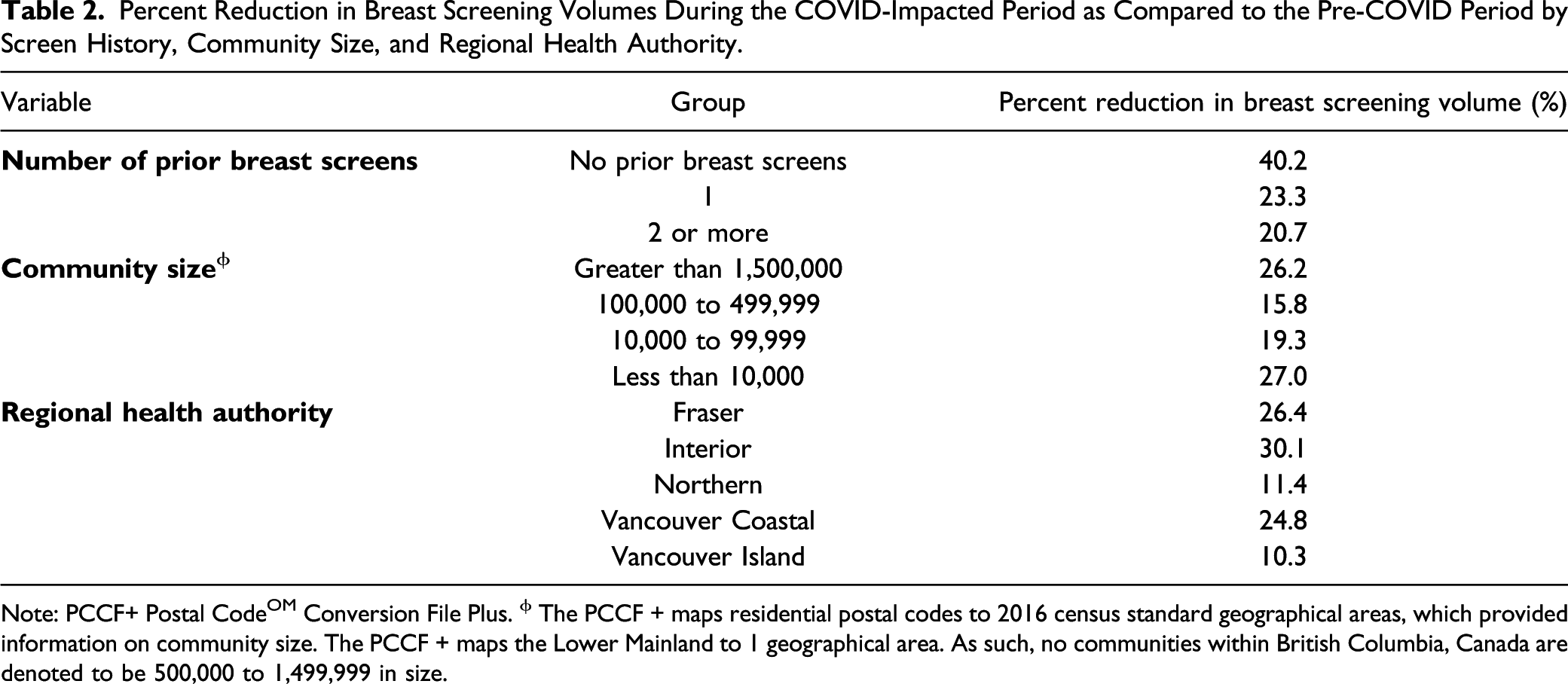
Note: PCCF+ Postal CodeOM Conversion File Plus. ϕ The PCCF + maps residential postal codes to 2016 census standard geographical areas, which provided information on community size. The PCCF + maps the Lower Mainland to 1 geographical area. As such, no communities within British Columbia, Canada are denoted to be 500,000 to 1,499,999 in size.
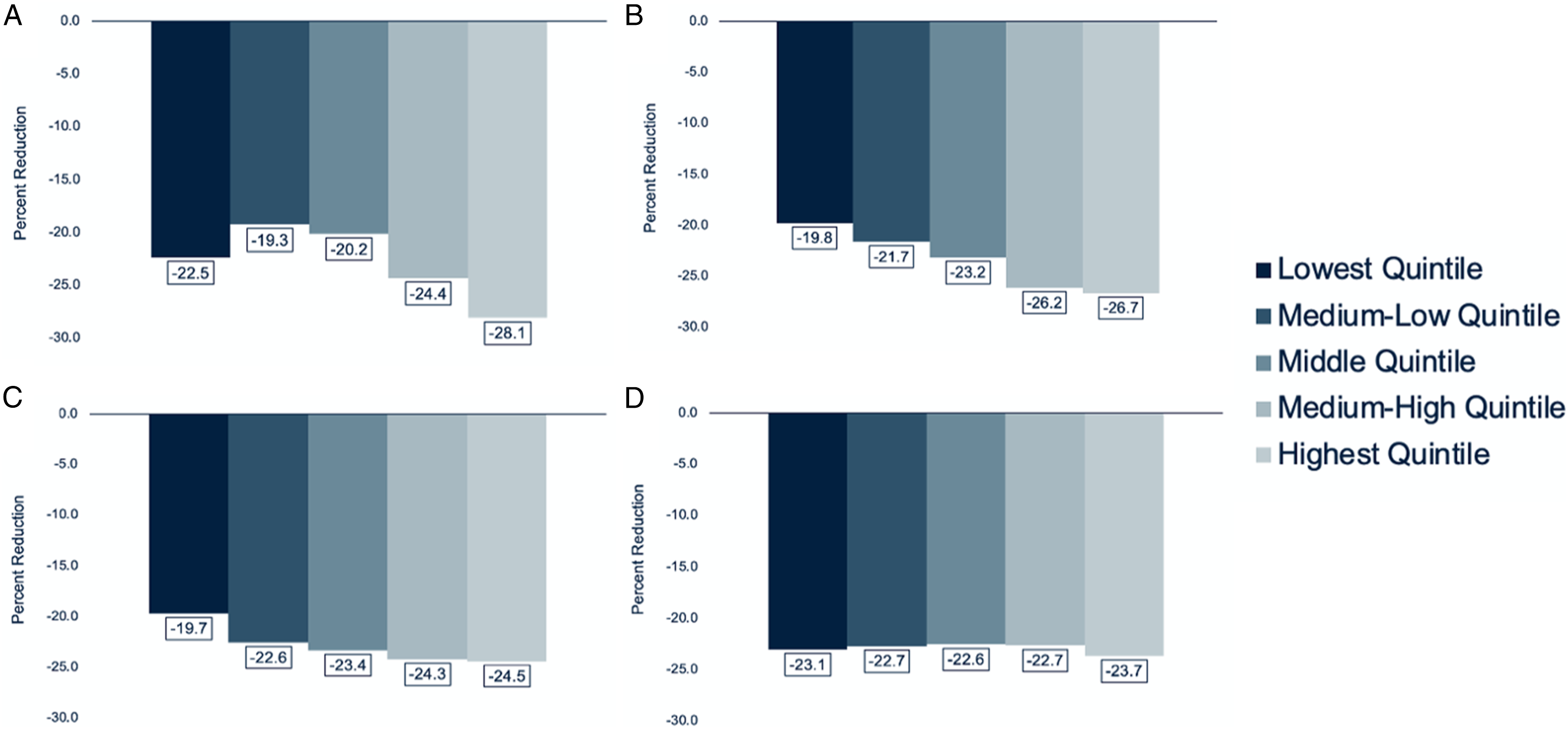
Percent reductions in breast screening volumes during the COVID-impacted period as compared to the pre-COVID period varied with patient income quintile. The largest percent reduction in breast screening volume was among patients in the most deprived income quintile (28.1%). Percent reductions in breast screening volumes were less among patients in less deprived income quintiles (Figure 2). Similarly, percent reductions in breast screening volumes for groups defined by situational vulnerability and economic dependency dimensions of the CIMD increased monotonically with deprivation, with the most deprived quintiles showing the greatest percent reductions in breast screening volumes (Figure 3). A trend towards greater percent reductions in breast screening volumes with increased deprivation of the ethnocultural composition dimension was also observed, with the most deprived quintile experiencing a 28.1% reduction in breast screening volume. A relationship between reduction in breast screening volume and residential instability was not observed. Percent reduction in breast screening volume during the COVID-impacted period as compared to the pre-COVID period by income quintile. Lowest quintile corresponds to the most deprived income quintile and highest quintile corresponds to the least deprived income quintile. Percent reduction in breast screening volume during the COVID-impacted period as compared to the pre-COVID period by each dimension of the CIMD: ethnocultural composition (A), situational vulnerability (B), economic dependency (C), and residential instability (D). Lowest quintile corresponds to least deprivation for each dimension and highest quintile corresponds to greatest deprivation for each dimension.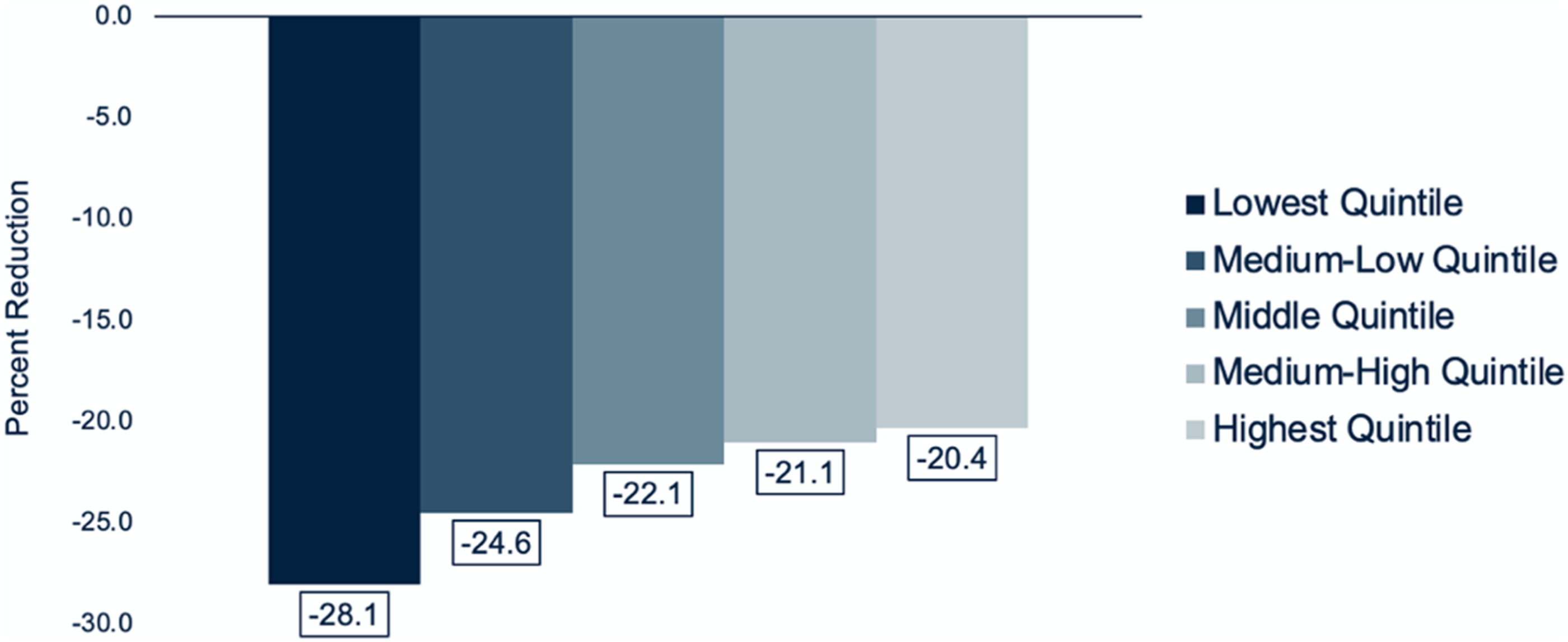
Discussion
Overall breast screening volume was notably reduced during the COVID-impacted period as compared to the pre-COVID period in our large provincial, population-based breast screening program. Reductions in overall breast screening volumes during the COVID-19 pandemic have been previously variably reported. 10,17,24,25 An absolute deficit of approximately 3,900,000 breast screens across the United States has been previously estimated to be arising from reductions in breast screening volumes. 17 Using insurance claims data provided by a large insurance provider, Song et al (2021) estimated an approximately 58% reduction in breast screening volume during the 20 weeks following the onset of the COVID-19 pandemic. 24 Such reductions in overall breast screening volumes have been generally attributed to the suspension of breast screening at the onset of the COVID-19 pandemic, with subsequent recovery of breast screening volumes being variable. 10,17,21,24,25 While this study did not assess temporal variations in breast screening volumes throughout the COVID-impacted period, variations in breast screening volumes in our large provincial, population-based breast screening program throughout this period have been previously reported. 21
We observed the greatest and least percent reductions in breast screening volumes during the COVID-impacted period among younger patients aged 40 to 49 years and older patients aged 70 to 74 years, respectively. In contrast to our observations, Sprague et al (2021) observed a greater reduction in breast screening volume and slower recovery in breast screening volume among patients aged 70 years or older during the COVID-19 pandemic, 10 with similar observations also previously reported. 17 At a single urban safety-net hospital in California, Velazquez et al (2021) observed a greater reduction in breast screening volume among patients aged 40 to 49 years during the period of time corresponding to the first local stay-at-home order and among patients aged 70 years or older during the second local stay-at-home order. 15 The disproportionate impact of the COVID-19 pandemic on younger patients with respect to increased workplace and childcare stressors and on older patients with respect to increased risk of poor health outcomes associated with COVID-19 infection may be potentially associated with these observations.
The least percent reduction in breast screening volume was observed among patients who had previously undergone 2 or more breast screens. The impact of number of prior breast screens on breast screening volumes during the COVID-19 pandemic has not been previously assessed. Appreciation of the importance of breast screening and habituation among patients who have previously undergone multiple breast screens may be suggested to be potentially associated with these observations and is concordant with pre-pandemic observations in the BC Cancer Breast Screening Program. 26 Previously, it has been hypothesized that an increased risk of breast cancer or family history of breast cancer may be associated with smaller reductions in breast screening volumes among patients during the COVID-19 pandemic. Nonetheless, Nyante et al (2021) and Sprague et al (2021) did not observe variations in breast screening volumes among patients with an increased risk of breast cancer during the COVID-19 pandemic. 10,25 While Sprague et al (2021) did observe an increased likelihood of patients with dense breasts to defer breast screening during the COVID-19 pandemic, dense breasts being associated with patients of certain races was thought to underly these observations. 10
Patients in rural communities may have encountered challenges in access to breast screening during the COVID-19 pandemic as we observed that the greatest percent reduction in breast screening volumes was among patients residing in communities with a population of less than 10,000. Using data from a large, state-wide non-profit healthcare system in Washington State, Amran et al (2021) similarly observed greater reductions in breast screening volumes among patients residing in rural communities as compared to urban communities during the COVID-19 pandemic. 16 Variability in breast screening volumes among urban and suburban breast screening sites during the COVID-19 pandemic has also been reported, with an increased proportion of breast screening being completed at suburban breast screening sites as compared to urban breast screening sites. 14 Likewise, we observed geographic regional variability in breast screening volumes among health authorities in British Columbia, Canada. Interestingly, though the Northern Health Authority is primarily comprised of rural communities, patients residing in communities in this health authority were observed to have the second lowest percent reduction in breast screening volumes though poor baseline breast screening volumes may explain in part these observations. Geographic regional variability in breast screening volumes was also observed by Chen et al (2021), who observed that percent reductions in breast screening volumes were variable in geographic regions within the United States. 17 Chen et al (2021) also observed geographic regional variability in recovery of breast screening volumes, with various geographic regions within the United States having variable recovery in breast screening volumes suggested to be attributed to the temporality of COVID-19 infection in various geographic regions. 17
This was the first study to assess the association between patient sociodemographic status and breast screening volumes during the COVID-19 pandemic in a large, population-based breast screening program. We observed the greatest percent reductions in breast screening volumes among patients in the lowest income quintile and among patients in quintiles which were most deprived across all 4 dimensions of the CIMD. These observations are dissimilar to that of Chen et al (2021) who observed that patients in the least deprived socioeconomic status quartiles had the greatest percent reductions in breast screening volumes during the COVID-19 pandemic. 17 As a result of these reductions in breast screening volumes Chen et al (2021) observed comparable breast screening volumes among patients in the least deprived and most deprived socioeconomic status quartiles during the initial months of the COVID-19 pandemic. 17 Nonetheless, the use of data from a Medicare administrative claims database may have underestimated the impact of sociodemographic status on breast screening volumes during the COVID-19 pandemic. 17
The association of patient-reported race, ethnicity, and country of birth on breast screening volumes was not able to be assessed from data collected directly from patients by our breast screening program. Although this information is requested from patients on a comprehensive intake form upon entry into the breast screening program, these sociodemographic variables were found to have a notable proportion of missing data. As such, we were only able to assess some of these sociodemographic dimensions through the CIMD. The impact of race on breast screening volumes during the COVID-19 pandemic has been previously reported in the United States. Disproportionate reductions in breast screening volumes 14 –16 and slower recovery in breast screening volumes 10 among non-White patients during the COVID-19 pandemic have been previously reported. Such inequities during the COVID-19 pandemic were observed to impact not only breast screening volumes but also other radiological imaging. 27 Disproportionate socioeconomic impact associated with the COVID-19 pandemic, increased worry about the risk of COVID-19 infection, and systemic barriers within the healthcare system may potentially contribute to these observations. 10,15 Further research to understand and to develop and to deploy targeted interventions to mitigate such inequities in participation in breast screening are required. 14
Reduced breast screening volumes during the COVID-19 pandemic may negatively impact early detection of breast cancer and may subsequently result in increased breast cancer deaths. A reduction in abnormal breast screens and referrals to tertiary provincial cancer centers arising from breast screening at the onset of the COVID-19 pandemic in our large provincial, population-based breast screening program was previously reported. 21 Approximately 950 excessive breast cancer deaths in the United States between 2020 and 2030 are estimated to be attributed to delayed breast screening during the COVID-19 pandemic. 28 Further work from our group will aim to assess the impact of reduced breast screening volumes during the COVID-19 pandemic on the histopathological breast cancer and patient outcomes in the BC Cancer Breast Screening Program.
Unlike prior reports, which were generally comprised of small, single-institution or insurance claims data, our study included data from a large, population-based breast screening program that serves a provincial population of over 5 million. Moreover, dissimilar to prior reports we utilized an average of 3 annual periods as the baseline breast screening volume to limit the effect of annual variation. Our study was limited by the retrospective nature of our data. Use of residential postal codes to impute sociodemographic variables further did not allow for the use of individual patient-reported sociodemographic data. While our study assessed the impact of community size, we did not evaluate the impact of distance to closest breast screening site on breast screening volumes during the COVID-19 pandemic. As previously described, the impact of race, ethnicity, and country of birth on breast screening volumes during the COVID-19 pandemic could not be assessed. Moreover, our use of breast screening volumes only estimated participation in breast screening. As we calculated percent reductions in breast screening volumes during the COVID-19 pandemic as compared to baseline breast screening volumes, our data may underestimate the disproportionate association of patient sociodemographic status on participation in breast screening.
Conclusion
COVID-19 related disruptions resulted in a notable reduction in the overall breast screening volume in our large provincial, population-based breast screening program during the COVID-19 pandemic. We observed disproportionate reductions in breast screening volumes among younger patients, patients with fewer prior breast screens, and patients residing in rural communities. Moreover, we observed disproportionate reductions in breast screening volumes among patients in lower income quintiles and among patients in quintiles which were most deprived across all 4 dimensions of the CIMD. Identification of inequities in breast screening during the COVID-19 pandemic provides the opportunity to improve equitable participation in breast screening for vulnerable populations. Further research to understand and to develop and to deploy targeted interventions to mitigate disproportionate participation in breast screening are required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Michael Smith Foundation for Health Research Grant (Grant # COV-2020-1048).