
Abstract
Introduction
Marfan Syndrome (MFS) is a genetically determined connective tissue disorder with multisystem involvement, predominantly of the skeletal, cardiovascular and ocular systems.1,2 MFS is caused by pathogenic variants in the gene encoding extracellular matrix protein fibrillin-1 (FBN1) and is associated with an excessive release of transforming growth factor-beta (TGF-β). Pectus excavatum (PEX) is a common skeletal abnormality, occurring in two-thirds of MFS patients 3 with an unclear etiopathogenesis. Based on familial studies, it is possible that PEX may be partly due to defects in connective tissue genes such as FBN, collagen and TGF-β. 4 The well-known cardiovascular manifestations in MFS are aortic aneurysm, mitral valve prolapse (MVP) and regurgitation (MR). In animal models, increased TGF-β activity and signalling has been shown to correlate temporally and spatially with mitral valve pathology. 5 There is growing evidence of primary myocardial dysfunction and findings to support the existence of Marfan cardiomyopathy.6-12 Since TGF-β mediates tissue fibrosis associated with inflammation and injury, diffuse myocardial fibrosis in MFS is plausible. 13
Numerous studies have demonstrated right ventricular (RV) distortion and dysfunction in non-syndromic individuals with PEX14-16 and some suggest improvement in RV function following surgical treatment of the deformity.17,18 A small paediatric study demonstrated mild RV dysfunction in MFS patients with PEX. 19 However, in patients with MFS and PEX, it is unclear if the mechanism of RV dysfunction is due to compromised RV filling due to compression, cardiomyopathy related to the genotype that is more evident or a combination. Despite the frequent association in MFS, the relationship of PEX with cardiac function and MFS-related cardiovascular abnormalities has not been systematically evaluated. Since the spectrum of cardiothoracic abnormalities of MFS are related to abnormal TGF-β signalling, we hypothesized that PEX is a marker of cardiovascular manifestations in MFS. Therefore, the objectives of our study were to compare the frequency of mitral valve abnormalities and cardiac MRI derived biventricular volumes, function and aortic dimensions in MFS PEX+ and PEX− patients.
Methods
Study Population
This single-centre retrospective cross-sectional study was approved by the institutional research and ethics board. The requirement for written informed consent was waived. Patient inclusion and exclusion is detailed in Figure 1. Inclusion criteria were adult patients (≥18 years of age) referred for cardiac MRI between 2010 and 2020 with a confirmed diagnosis of MFS based on revised Ghent nosology.
20
Exclusion criteria were incomplete cardiac MRI, artifacts degrading image quality and co-existent ischaemic or congenital heart disease. For ventricular volumetry, additional exclusion criteria were prior cardiovascular surgery and any valvular regurgitation characterized as moderate or severe by Doppler echocardiography. Demographic and clinical data including blood pressure, medications, ECG and echocardiography findings were obtained from electronic patient records where assessments were performed per established guidelines.21,22 Flowchart demonstrating number of patients with MFS included for mitral valve assessment and ventricular volumetry. MFS: Marfan syndrome; PEX: pectus excavatum. *Additional exclusion criteria for ventricular volumetry, numbers not mutually exclusive.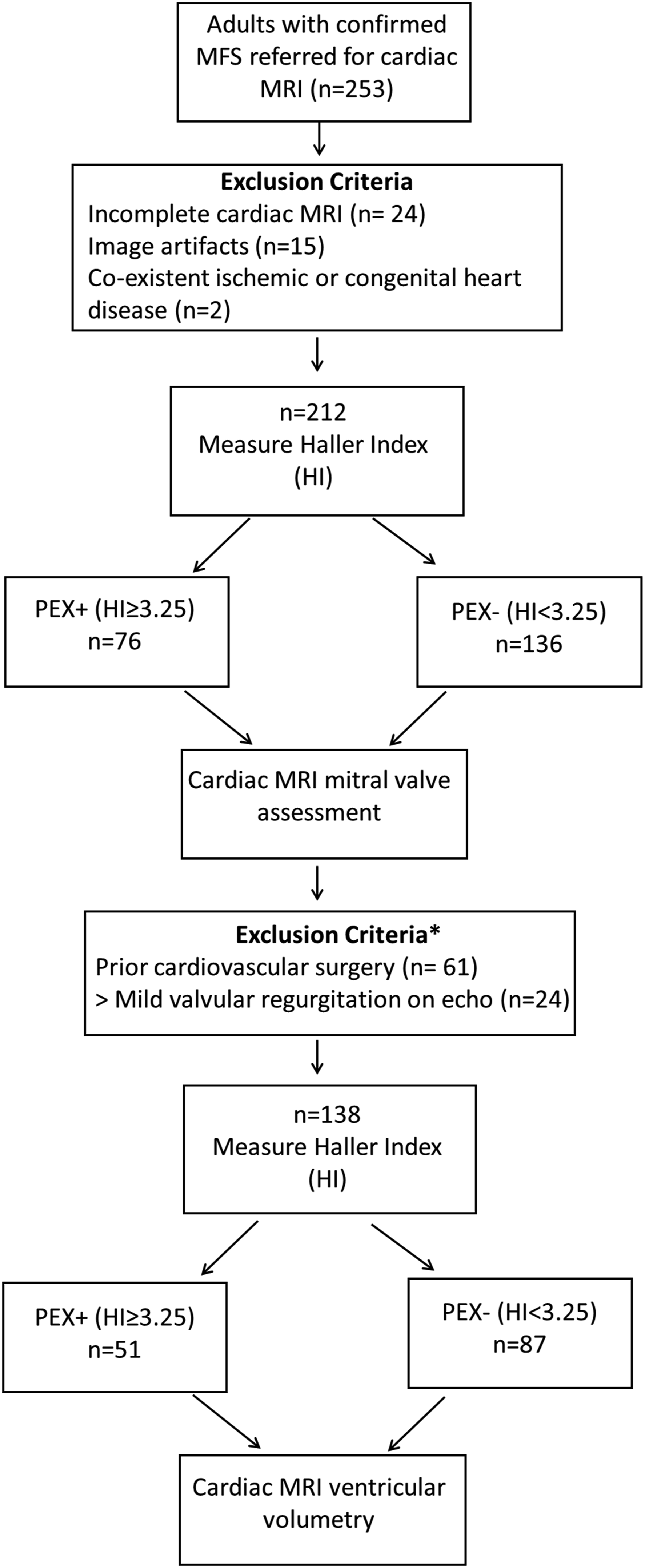
Cardiac MRI Acquisition
Cardiac MRI was performed using 1.5T (Magnetom Avanto fit; Siemens Healthcare, Erlangen, Germany) or 3T (Magnetom Skyra fit; Siemens Healthcare, Erlangen, Germany) scanners using commercially available cardiac surface coils. Retrospectively gated cine steady-state free precession images (SSFP) were obtained in multiple planes including two, three and four chamber views, left ventricular (LV) outflow tract coronal oblique and oblique aortic valve plane. A stack of short-axis SSFP images with coverage from base to apex (slice thickness 8 mm, 2 mm gap, temporal resolution 30-40 ms and other parameters as previously described) were acquired for ventricular volumetry. 23 Axial single-shot SSFP images of the chest, abdomen and pelvis were acquired. Non-ECG gated contrast-enhanced MR angiography was completed in the sagittal plane following intravenous administration of gadobutrol (Gadovist, Bayer Healthcare, Berlin, Germany) with optimization for maximal aortic enhancement during the arterial-phase acquisition.
Cardiac MRI Analysis
Cardiac MRI analyses were performed by a fellowship trained reader with 1 year experience in cardiac imaging, blinded to all identifying information using commercially available software (cmr42, version 5.6.3; Circle Cardiovascular Imaging, Calgary, Canada). PEX was quantified using Haller Index (HI) as the ratio between the lateral distance of the chest wall (inner margins) and the narrowest anteroposterior distance between the vertebrae and sternum, both measured on the same level on an axial single-shot SSFP image.
24
Since HI ≥3.25 is considered moderate or severe PEX and significant to warrant surgical correction,
25
patients were classified as PEX+ or PEX− based on this cut-point. MVP was defined as ≥2 mm excursion of any mitral leaflet segment(s) beyond the mitral annular plane into the left atrium as measured on the end-systolic LV 3-chamber cine SSFP image, Figure 2.
26
Mitral annular disjunction (MAD) was defined as a separation between the left atrium-posterior mitral leaflet junction and the atrial margin of the LV myocardium. The length of MAD was measured from the left atrium-posterior mitral leaflet junction to the atrial margin of the LV basal inferolateral wall on the end-systolic LV 3-chamber cine SSFP image, Figure 2.
27
Valves were assessed qualitatively for the presence and severity of regurgitation on long- and short-axis cine SSFP images. If only one valve was regurgitant, the difference in biventricular stroke volumes was used for quantification. Maximum sinus to sinus aortic root dimensions were measured on the aortic valve oblique cine SSFP images in end-diastole and maximum aortic diameters were measured on double oblique MR angiography images perpendicular to the aortic centreline using commercially available software (Aquarius iNtuition Viewer, TeraRecon, Durham NC, USA).
28
Ventricular volumes, function and mass were measured using semi-automated contour detection with manual adjustment when required.
28
In men, the thresholds for ventricular dilatation were LV indexed end-diastolic volume (LVEDVi) >105 mL/m2 in men, RVEDVi >121 mL/m2 and for reduced ejection fraction (EF) were LVEF <57% and RVEF <52%.
29
In women, the thresholds for ventricular dilatation were LVEDVi>96 mL/m2, RVEDVi >112mL/m2 and for reduced EF were LVEF<57% and RVEF<51%.
29
Twenty-nine-year-old female with Marfan syndrome and severe pectus excavatum: (A) Haller Index of 8.8 measured as internal transverse diameter (red)/anteroposterior diameter (green), (B) Normal RV size (RVEDVi 96 mL/m2) with impaired RV function (RVEF 43%); dilated LV (LVEDVi 144 mL/m2) with impaired LV function (LVEF 51%). (C) Prominent aortic root dimensions (black) 41 mm, (D) Mitral valve prolapse (blue)10 mm, (E) Mitral annular disjunction (orange) 3 mm. RV: right ventricle; LV: left ventricle; EDV: end-diastolic volume; ESV: end-systolic volume; I: indexed to body surface area.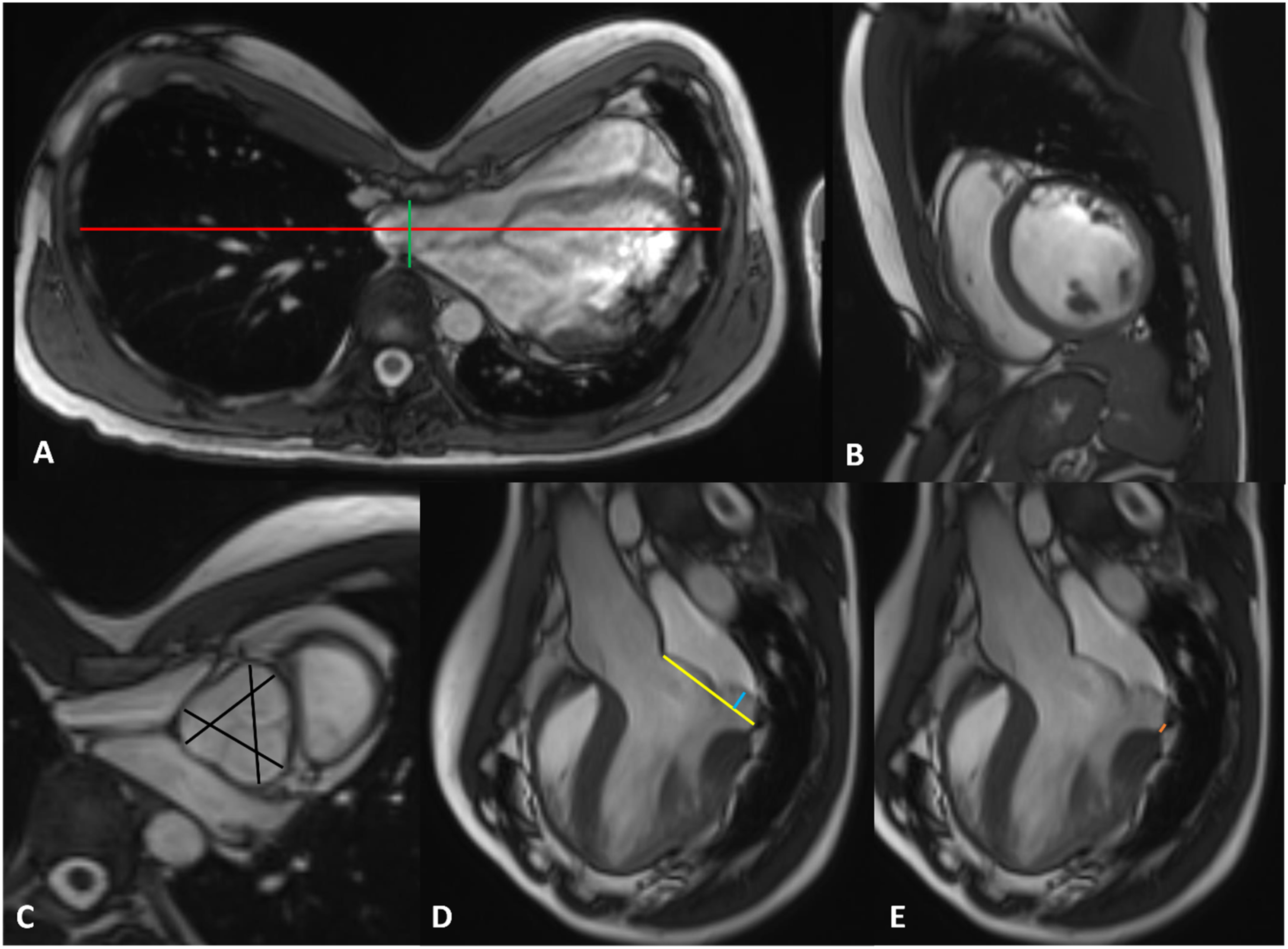
Intra-observer and Inter-observer Agreement
A random subset of 30 studies were selected and reanalysed by the same reader following a minimum 2-month interval after the initial analysis to assess intraobserver agreement. The same subset was analysed by an experienced fellowship trained observer with 7 years of cardiovascular imaging experience to assess inter-observer agreement. The studies were evaluated for presence or absence of MVP, MAD and calculation of HI. Both readers were blinded to all identifying information and results of the first analysis.
Statistical Analysis
Categorical data are presented as counts (percentage) and continuous variables as means (standard deviation). The normality of continuous data was tested using the Kolmogorov–Smirnov test. We estimated that 88 patients (44 in each group) will provide 80% power at two-sided alpha error of 5%, to detect a difference in RVEF as low as 3% with a standard deviation of 5%. For comparison of continuous variables between groups, two-tailed independent samples t-test or non-parametric Mann–Whitney test was used and for comparison of categorial variables, Chi-square test or Fisher exact test were used as appropriate. Pearson or Spearman correlation coefficients were used to evaluate associations between continuous variables. Cohen’s kappa was used to assess intra-observer and inter-observer agreement for determining MVP and MAP. Intraclass correlation coefficient (ICC) with one-way random-effects model and two-way random-effects model were used for assessment of intraobserver and interobserver agreement, respectively, for the calculation of HI. Statistical analysis was performed using a professional statistical software package GraphPad Prism 9.0.2 (GraphPad Software, Inc., La Jolla, CA, USA). P-value <.05 (two-sided) was considered statistically significant.
Results
Clinical and Cardiac Valve Characteristics.
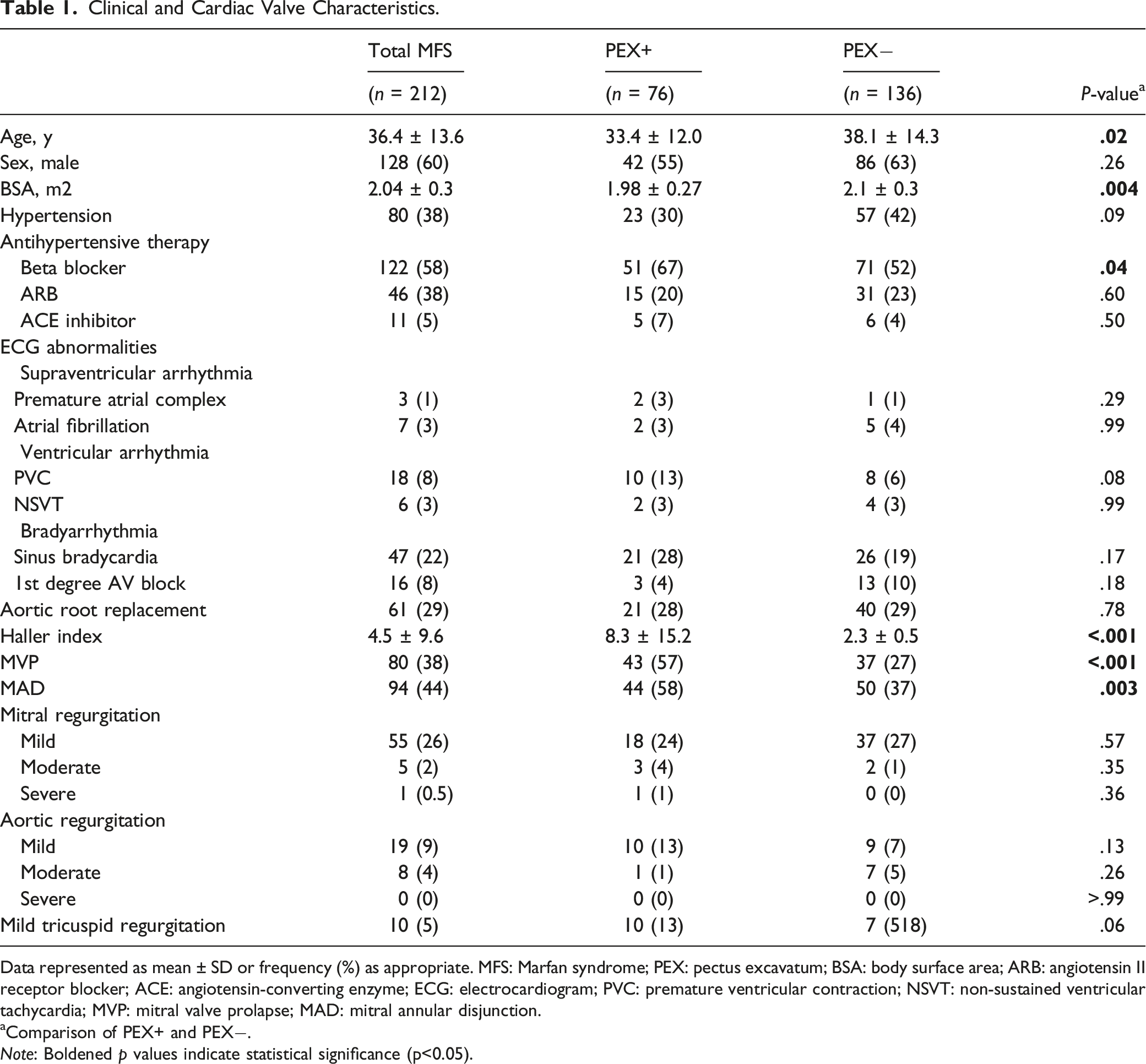
Data represented as mean ± SD or frequency (%) as appropriate. MFS: Marfan syndrome; PEX: pectus excavatum; BSA: body surface area; ARB: angiotensin II receptor blocker; ACE: angiotensin-converting enzyme; ECG: electrocardiogram; PVC: premature ventricular contraction; NSVT: non-sustained ventricular tachycardia; MVP: mitral valve prolapse; MAD: mitral annular disjunction.
aComparison of PEX+ and PEX−. Note: Boldened p values indicate statistical significance (p<0.05).
The overall prevalence of MVP was 80/212 (38%) and of MAD was 94/212 (44%). The prevalence of MVP and MAD was significantly higher in the PEX+ group [43/76 (57%) vs 37/136 (27%), P < .001 and 44/76 (58%) vs 50/136 (37%), P = .003]. A total of 61/212 (29%) of the MFS patients had MR, of which 55/212 (26%) had mild MR, 5/212 (2%) had moderate MR and 1/212 (0.5%) had severe MR. This was similar among PEX+ and PEX−. All six patients with moderate or severe MR had both MVP and MAD.
Assessment for MVP had excellent intra-observer and inter-observer agreement (κ 0.92, 0.86, respectively). Assessment for MAD had substantial intra-observer agreement (κ 0.80) and excellent inter-observer agreement (κ 0.92). Quantification of HI had excellent intra-observer [ICC 0.99, 95% CI (0.98, 0.995)] and inter-observer agreement [ICC 0.99, 95% CI (0.98, 0.995)].
Ventricular Volumetry and Aortic Dimensions.
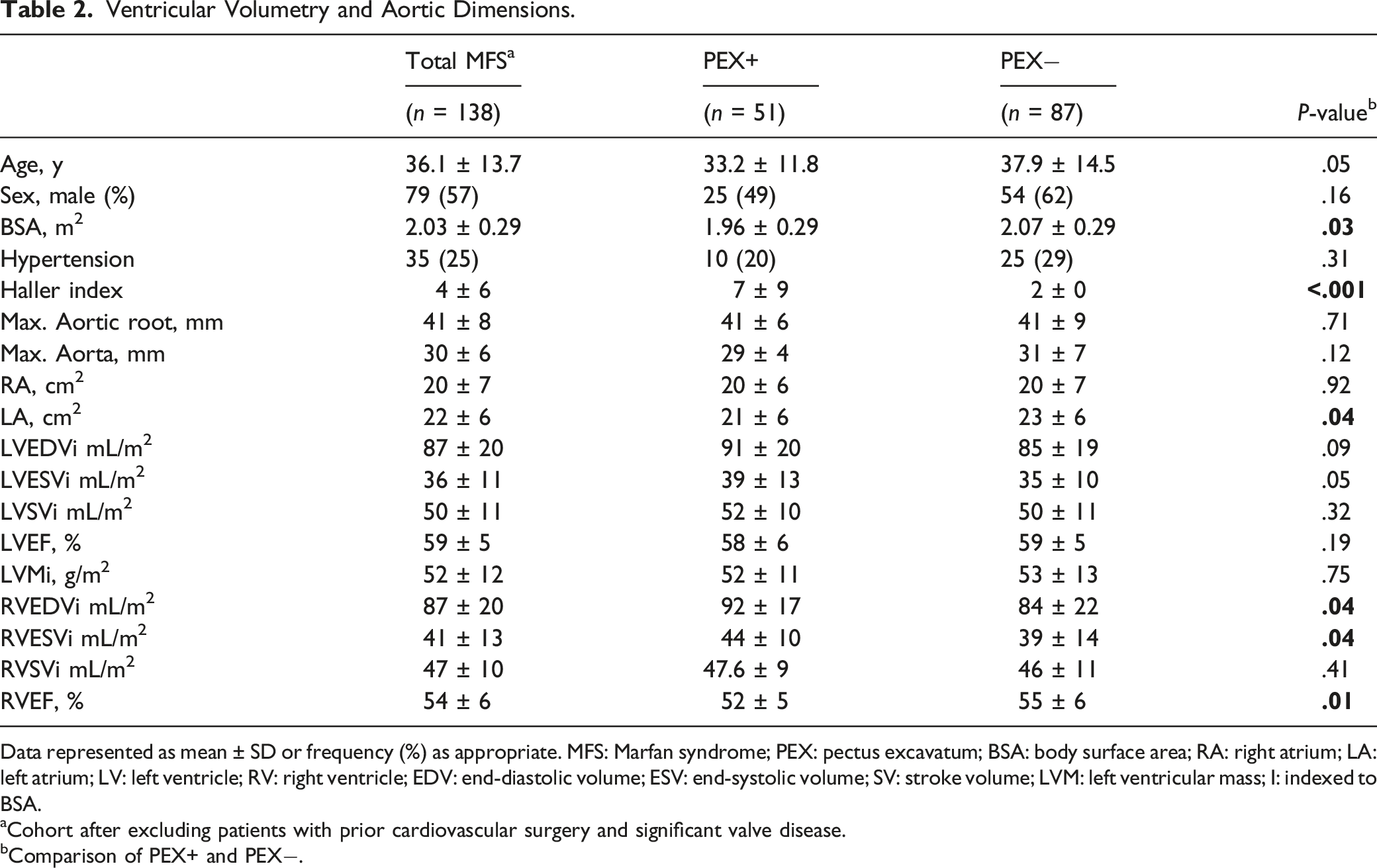
Data represented as mean ± SD or frequency (%) as appropriate. MFS: Marfan syndrome; PEX: pectus excavatum; BSA: body surface area; RA: right atrium; LA: left atrium; LV: left ventricle; RV: right ventricle; EDV: end-diastolic volume; ESV: end-systolic volume; SV: stroke volume; LVM: left ventricular mass; I: indexed to BSA.
aCohort after excluding patients with prior cardiovascular surgery and significant valve disease.
bComparison of PEX+ and PEX−.
PEX+ patients had higher RV end-diastolic and end-systolic volumes (RVEDVi 92 ± 17 mL/m2 vs 84 ± 22 mL/m2; RVESVi 44±10 mL/m2 vs 39±14 mL/m2, both P = .04) and lower RVEF (52 ± 5% vs 55 ± 6%, P = .01). There was no significant difference in LV volumes or LVEF in PEX+. The maximum aortic dimensions were also similar.
Discussion
PEX is a key feature of MFS. Despite the frequent association of PEX with MFS, the relationship of PEX with MFS-related cardiovascular abnormalities, cardiac size and function has not been systematically evaluated. If PEX in MFS is related to abnormal TGF-β signalling, its presence may indicate other cardiovascular manifestations of MFS. Furthermore, in the context of genotype-related intrinsic myocardial dysfunction in MFS, any further PEX-associated ventricular remodelling as shown in non-syndromic patients, can be an additional burden in these patients and have potential clinical implications. To the best of our knowledge, this is the first adult study and the largest study to evaluate the association of PEX with valvular abnormalities, cardiac structure and function in MFS. Our study adds the following information to the understanding of cardiac health in MFS patients with PEX: 1. The prevalence of MVP and MAD is significantly higher in MFS patients with pectus excavatum compared to those without. 2. MFS PEX+ patients have higher RV volumes and lower RVEF compared to those without.
HI is a simple, quick and reliable measure to grade the severity of PEX and can be easily calculated on axial MRI or CT. According to current imaging guidelines, CT is an alternative modality for aortic evaluation in MFS when MRI is unavailable or when patients have contraindications to undergo MRI. 30 Often, general or non-cardiac radiologists interpret thoracic aortic CTs. Therefore, the awareness of association of higher frequency of cardiac manifestations in those with MFS and pectus is important.
Mitral Valve Abnormalities
MVP is a well-known finding in MFS. 31 MAD is a separation between the posterior mitral valve leaflet insertion and the left ventricular myocardium. MAD has received significant interest recently given its potential clinical significance based on the association with ventricular tachycardia and sudden cardiac death. 32 MAD appears to be common in myxomatous mitral valve disease and MVP, and the prevalence of MAD is high in MFS. In an animal model with MFS, the increased TGF-β activity and signalling has been shown to correlate temporally and spatially with mitral valve pathology. 5 Demolder et al 33 described a 34% prevalence of MAD in MFS patients which was associated with the occurrence of arrhythmic events, a higher need for mitral valve intervention and increased aortic events in the form of dissection and prophylactic aortic surgery for dilatation. Chivulescu et al 34 reported a 41% prevalence of MAD in a combined cohort of MFS and Loeys-Dietz syndrome patients, associated with a more severe disease phenotype characterized by aortic surgery at younger age and frequent need for mitral surgery. 34 The overall prevalence of MAD in both groups in our study is similar to what is reported in prior studies.
Specifically, we found a significantly higher prevalence of MAD and MVP in the PEX+ group. Therefore, we propose that there is an increased association of cardiac-valvular abnormalities of MFS in those with PEX. While we did not examine the association of ocular or other skeletal abnormalities with MVP and MAD, it is possible that patients with MFS with more syndromic manifestations may also have a higher frequency of mitral valve pathology. MFS patients with PEX may have different outcomes compared with PEX – which requires further study. Given the evidence of adverse clinical outcomes in those with MVP and MAD and the increased association of these valvular abnormalities in MFS PEX+, careful screening for mitral valve abnormalities and close monitoring is warranted.
Ventricular Volumes and Function
There is data to support the existence of intrinsic myocardial dysfunction in the absence of significant valvular disease and cardiovascular surgery in MFS.9,10 Ventricular dilation in MFS has been shown and genotype-phenotype relationships in the myocardium have been indicated.13,35 Similar to prior data, we found a proportion of MFS patients with LV and RV dilatation and impaired global function compared to established reference standards.
A single study evaluated the impact of PEX in paediatric MFS patients and found lower RVEF compared to healthy controls. 19 Since Marfan cardiomyopathy is an effect modifier, the RVEF reduction cannot be attributed to PEX alone. However, this finding persisted on subgroup analysis of MFS patients when classified based on the presence or absence of a significant PEX as evidenced by HI >3.25. Lam et al 19 did not find significant differences in the LV or RV volumes among paediatric MFS PEX+, PEX− and healthy controls. 19 Given the higher RV volumes among PEX+ adults in our study, it is plausible that RV dilation and cardiomyopathy may be slowly progressive. Although we are unable to establish causality, we observed significantly lower RVEF among PEX+ patients.
In the non-syndromic population, the cardiac dysfunction is thought to be secondary to depression of the sternum and resultant mechanical compression and geometric distortion of the RV. Based on our findings of increased RV volumes and reduced RVEF in PEX, we suggest an alternative explanation for RV dysfunction. While the role of mechanical compression cannot be excluded, as in non-syndromic patients, this alone cannot explain the altered volumetry since the RV volumes are higher and not lower as would be expected with a posteriorly displaced sternum abutting the RV and compromising its filling. Therefore, the second proposed mechanism is that the higher ventricular volumes and lower ejection fraction are a reflection of the primary Marfan cardiomyopathy, which is more evident in those with PEX, another manifestation of MFS. Furthermore, this is supported by the association of increased mitral valve abnormalities which are also syndromic manifestations. It is important for all radiologists interpreting aortic MRI or CT in patients with MFS to be aware of this association. Highlighting significant pectus as measured by HI can facilitate screening for mitral valve and other cardiac abnormalities.
Arrhythmia
Increased risk of arrhythmia in MFS patients has been documented compared to healthy controls. 10 Similar to published data, we found that a minority of patients had ECG abnormalities including sinus bradycardia and premature ventricular contractions (PVCs). There is limited data on the prevalence of rhythm disturbances specifically in those with PEX. While sinus bradycardia and PVCs typically have a favourable prognosis in the absence of structural heart disease, the long-term impact in patients with Marfan cardiomyopathy and PEX remains to be determined.
Our study has a number of limitations. Since it is a retrospective study, changes to the cardiac MRI protocol such as addition of phase contrast imaging for quantification of valvular regurgitation and parametric mapping techniques to assess fibrotic remodelling could not be performed. Additionally, a single slice of LV 3-chamber cine SSFP images was acquired and not a stack. Therefore, the MVP and MAD assessment can be potentially impacted by the slice selection and plane of acquisition. Lastly, since this is a quaternary-care single centre study, the findings may not be generalizable to all MFS patients.
The results of our study offer pathomechanistic insights into ventricular remodelling in MFS with PEX. In summary, MFS adults with significant PEX have increased prevalence of mitral valve abnormalities, larger RV volumes and lower RV systolic function. These findings suggest that the PEX may be a disease marker, reflecting increased cardiac manifestations of MFS and thereby severe disease phenotype. Given the increased associations of MFS-related cardiac abnormalities in patients with PEX, MFS PEX+ may have different outcomes compared with PEX− which requires further larger prospective longitudinal studies. The detection and systematic confirmation of this phenomenon would impact patient management, necessitate careful screening for mitral valve abnormalities and imaging and outcomes surveillance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.